Spatiotemporal Clustering Analysis of Malaria Infection in Pakistan

 ,
,  ,
, 
 and
and
Abstract
:1. Introduction
2. Methods
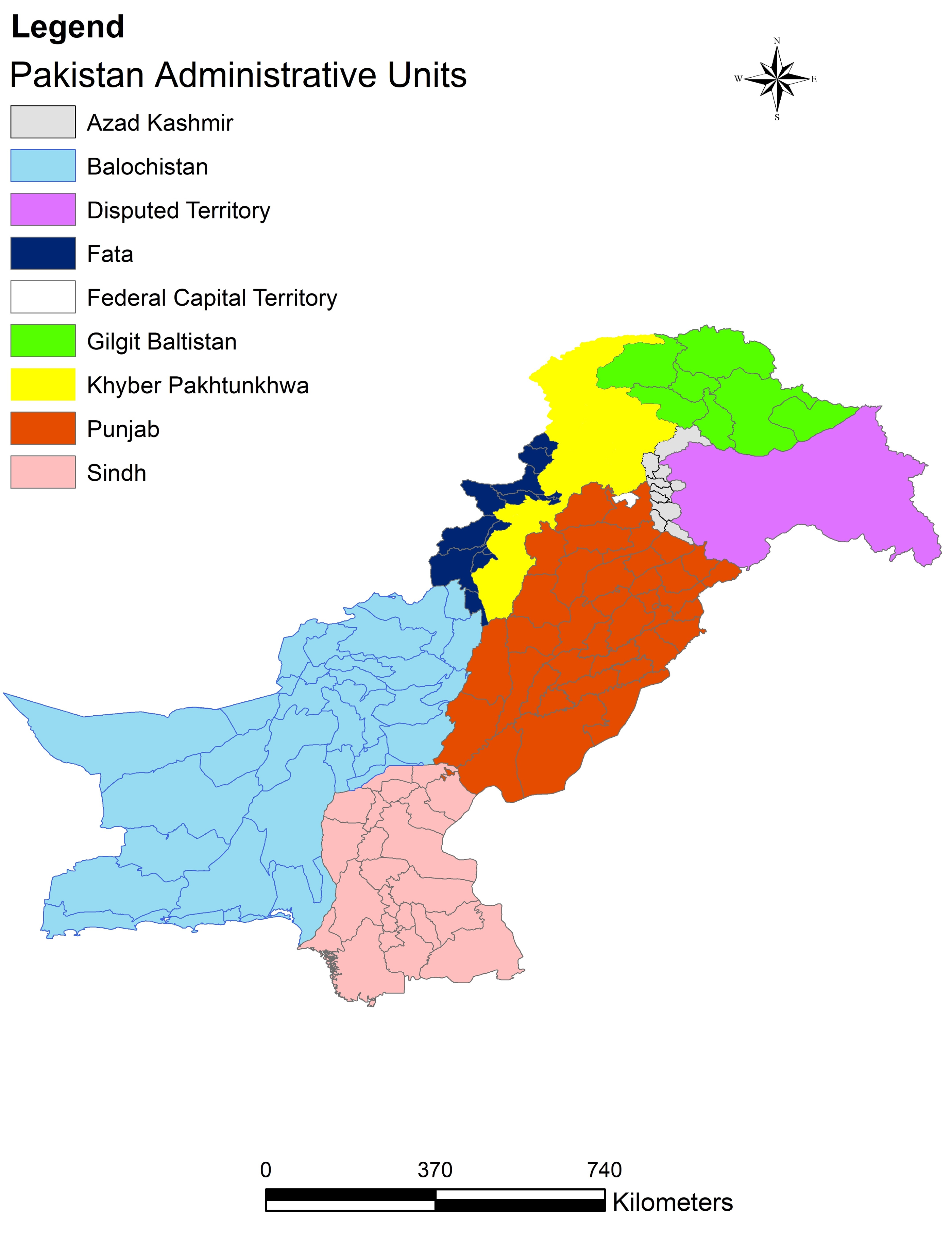
2.1. Study Area
2.2. Data Collection
2.3. Data Analyses
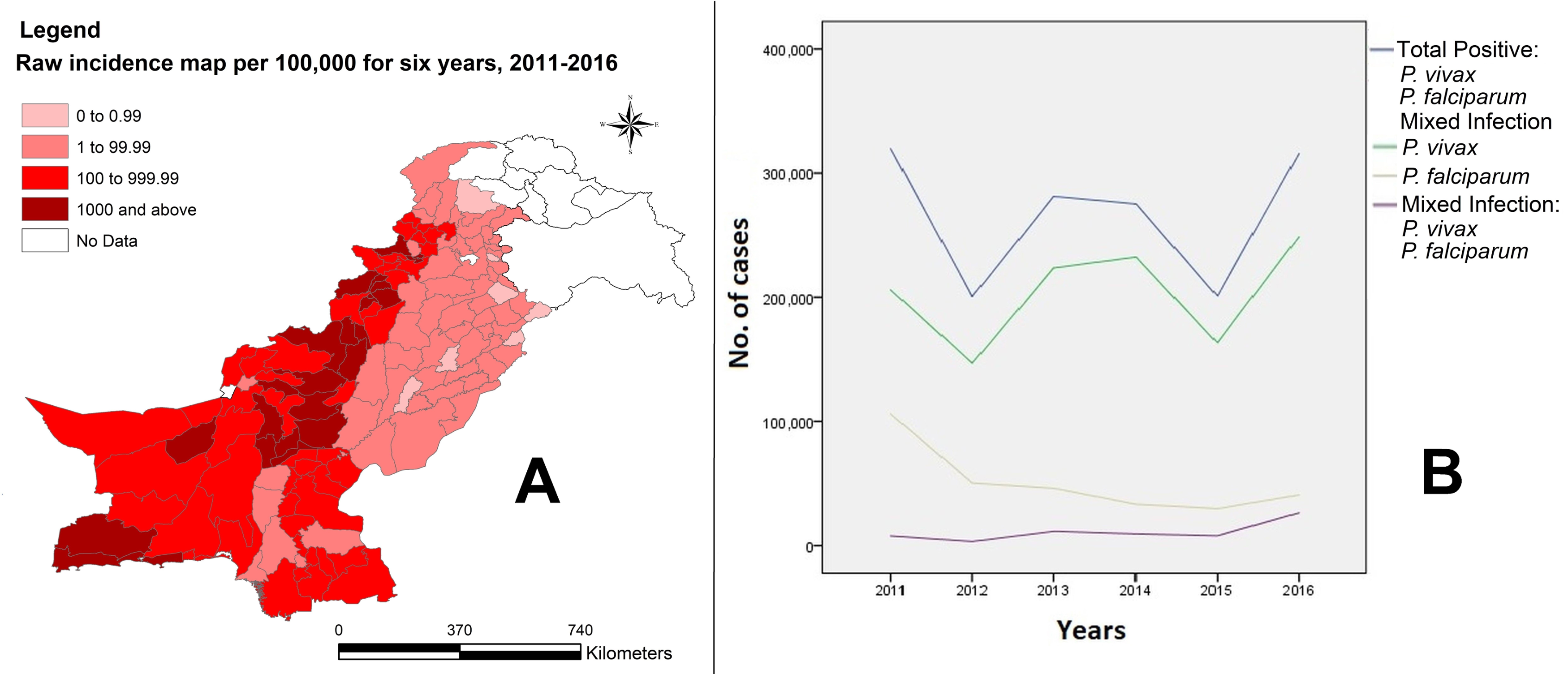
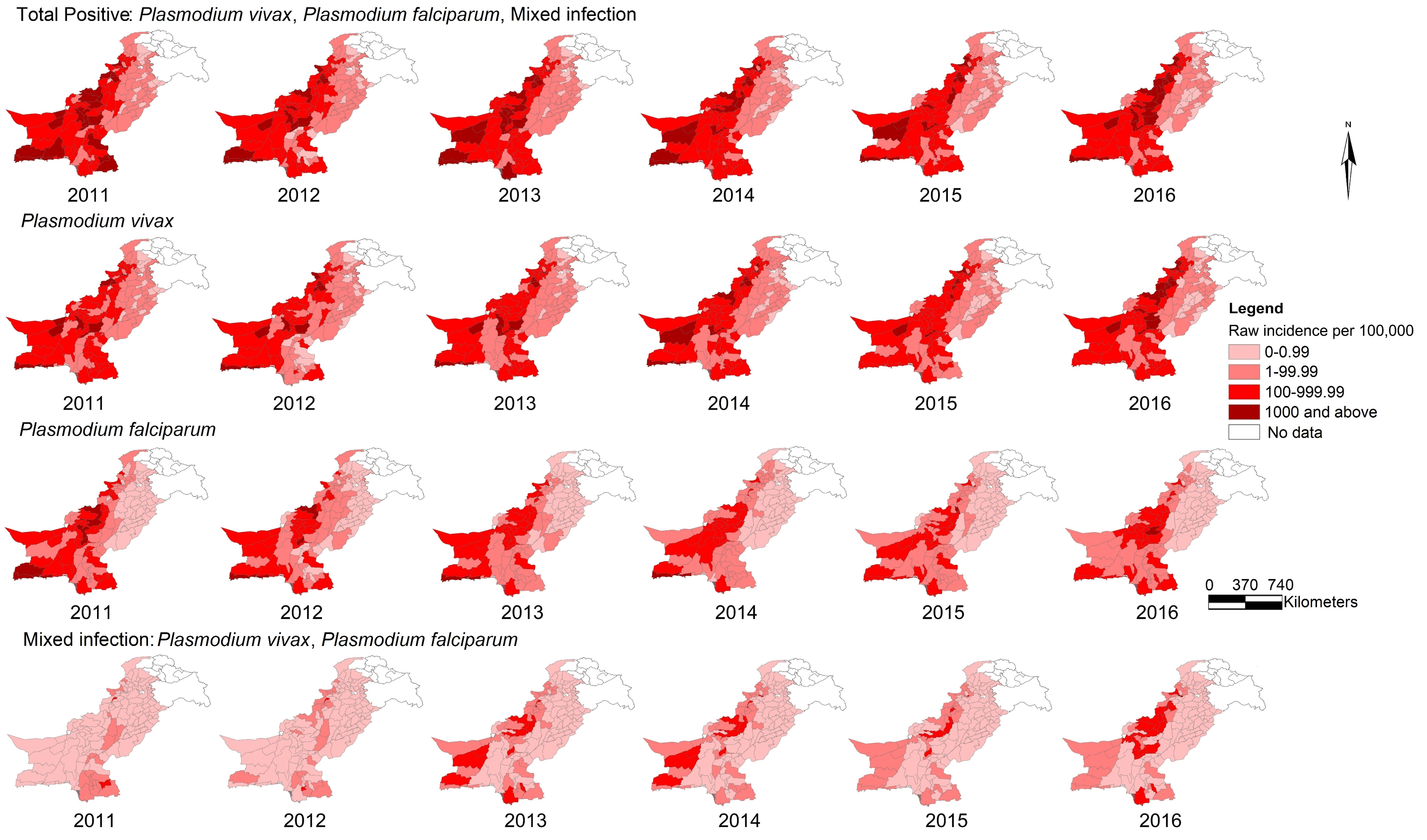
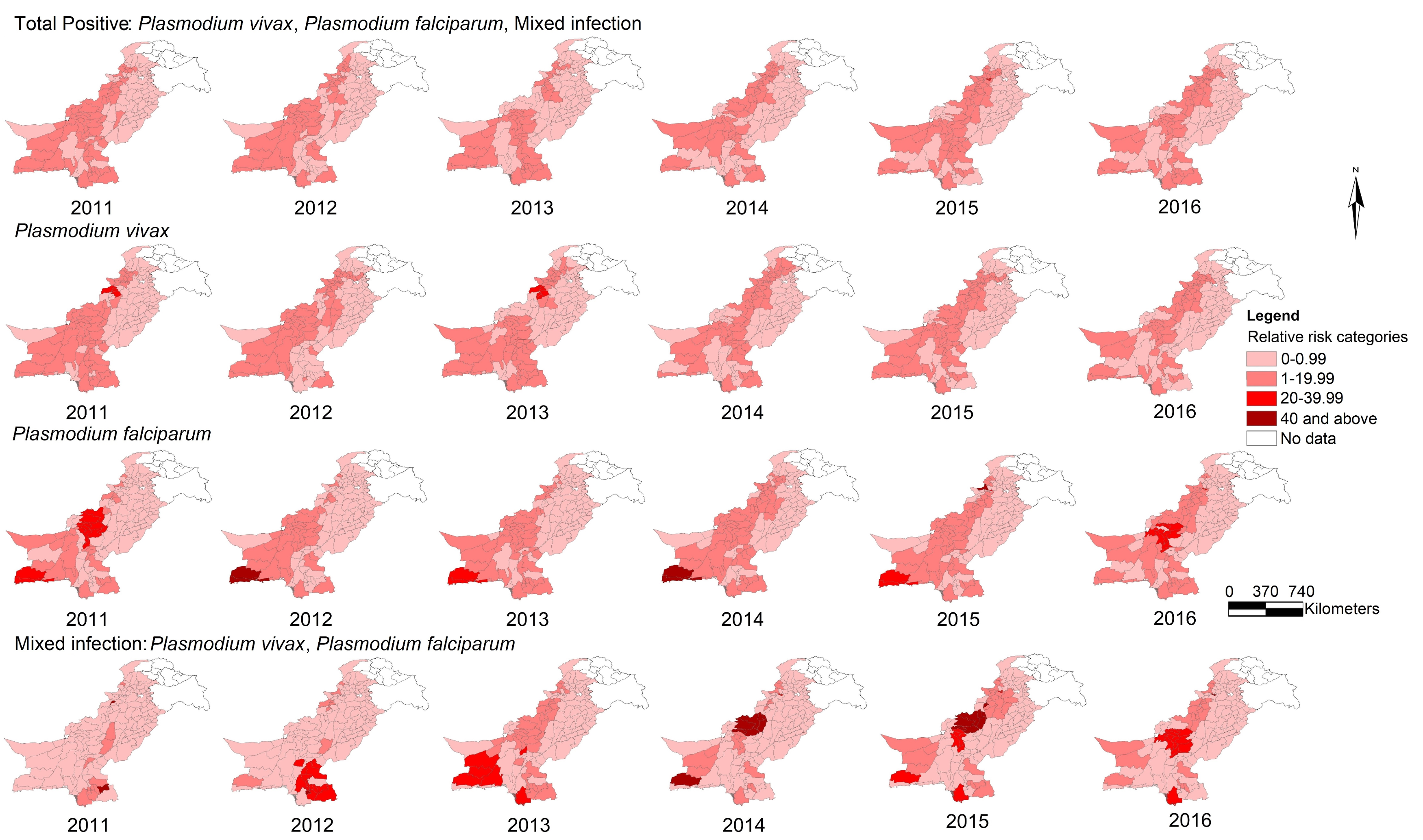
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| P | Plasmodium |
| EMRO | Eastern Mediterranean Regional Office |
| WHO | World Health Organization |
| GIS | Geographical Information System |
| KPK | Khyber Pakhtunkhwa |
| FATA | Federally Administered Tribal Areas |
| DoMC | Directorate of Malaria Control Program |
| DHIS | District Health Information System |
| MIS | Malaria Information System |
| DEWS | Disease Early Warning System |
| IR | Incidence Rate |
| RR | Relative Risk |
| PCR | Polymerase Chain Reaction |
References
- Faburay, B. The case for a “one health” approach to combating vector-borne diseases. Infect. Ecol. Epidemiol. 2015, 5, 28132. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). World Malaria Report 2017; WHO Press: Geneva, Switzerland, 2017; pp. 33–41. [Google Scholar]
- Hundessa, S.H.; Williams, G.; Li, S.; Guo, J.; Chen, L.; Zhang, W.; Guo, Y. Spatial and space–time distribution of Plasmodium vivax and Plasmodium falciparum malaria in China, 2005–2014. Malar. J. 2016, 15, 595. [Google Scholar] [CrossRef] [PubMed]
- Gunda, R.; Chimbari, M.J.; Shamu, S.; Sartorius, B.; Mukaratirwa, S. Malaria incidence trends and their association with climatic variables in rural Gwanda, Zimbabwe, 2005–2015. Malar. J. 2017, 16, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Gething, P.W.; Elyazar, I.R.F.; Moyes, C.L.; Smith, D.L.; Battle, K.E.; Guerra, C.A.; Patil, A.P.; Tatem, A.J.; Howes, R.E.; Myers, M.F.; et al. A long neglected world malaria map: Plasmodium vivax endemicity in 2010. PLoS Negl. Trop. Dis. 2012, 6, e1814. [Google Scholar] [CrossRef] [PubMed]
- Cotter, C.; Sturrock, H.J.W.; Hsiang, M.S.; Liu, J.; Phillips, A.A.; Hwang, J.; Gueye, C.S.; Fullman, N.; Gosling, R.D.; Feachem, R.G.A. The changing epidemiology of malaria elimination: New strategies for new challenges. Lancet 2013, 382, 900–911. [Google Scholar] [CrossRef]
- Feachem, R.G.A.; Phillips, A.A.; Hwang, J.; Cotter, C.; Wielgosz, B.; Greenwood, B.M.; Sabot, O.; Rodriguez, M.H.; Abeyasinghe, R.R.; Ghebreyesus, T.A.; et al. Shrinking the malaria map: Progress and prospects. Lancet 2010, 376, 1566–1578. [Google Scholar] [CrossRef]
- Imwong, M.; Nakeesathit, S.; Day, N.P.J.; White, N.J. A review of mixed malaria species infections in anopheline mosquitoes. Malar. J. 2011, 10, 253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ginouves, M.; Veron, V.; Musset, L.; Legrand, E.; Stefani, A.; Prevot, G.; Demar, M.; Djossou, F.; Brousse, P.; Nacher, M.; et al. Frequency and distribution of mixed Plasmodium falciparum-vivax infections in French Guiana between 2000 and 2008. Malar. J. 2015, 14, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Directorate of Malaria Control Program Pakistan. National Malaria-Strategic Plan-Pakistan (2015–2020), 2014. Available online: http://www.dmc.gov.pk/documents/pdfs/1National Malaria-Strategic Plan-Pakistan.pdf (accessed on 10 November 2017).
- Program Management Unit DoMC. Malaria Annual Report 2016, 2017. Available online: http://dmc.gov.pk/documents/pdfs/Malaria%20Annual%20Report%202016.pdf (accessed on 15 November 2017).
- Rahman, S.; Jalil, F.; Khan, H.; Jadoon, M.A.; Ullah, I.; Rehman, M.; Khan, A.M.; Khan, A.; Hayat, A.; Iqbal, Z. Prevalence of malaria in district Shangla, Khyber Pakhtunkhwa, Pakistan. J. Entomol. Zool. Stud. 2017, 5, 678–682. [Google Scholar]
- Owens, S. Malaria and the millennium development goals. Arch. Dis. Child. 2015, 100, S53–S56. [Google Scholar] [CrossRef] [PubMed]
- Gupta, B.; Gupta, P.; Sharma, A.; Singh, V.; Dash, A.P.; Das, A. High proportion of mixed-species Plasmodium infections in India revealed by PCR diagnostic assay. Trop. Med. Int. Health 2010, 15, 819–824. [Google Scholar] [CrossRef] [PubMed]
- Khatoon, L.; Khan, I.U.; Shah, S.A.; Jan, M.I.; Ullah, F.; Malik, S.A. Genetic diversity of Plasmodium vivax and Plasmodium falciparum in Kohat District, Pakistan. Braz. J. Infect. Dis. 2012, 16, 184–187. [Google Scholar] [CrossRef]
- Fareed, N.; Ghaffar, A.; Malik, T.S. Spatio-temporal extension and spatial analyses of dengue from Rawalpindi, Islamabad and Swat during 2010–2014. Climate 2016, 4, 23. [Google Scholar] [CrossRef]
- Shahzadi, S.; Akhtar, T.; Hanif, A.; Sahar, S.; Niaz, S.; Bilal, H. Molecular detection of malaria in South Punjab with higher proportion of mixed infections. Iran. J. Parasitol. 2014, 9, 37–43. [Google Scholar] [PubMed]
- Oneeb, M.; Maqbool, A.; Lateef, M.; Babar, M.E. Detection of Plasmodium falciparum infection in Anopheles stephensi in Punjab, Pakistan. Pak. J. Zool. 2015, 47, 1192–1195. [Google Scholar]
- Dash, A.P.; Valecha, N.; Anvikar, A.R.; Kumar, A. Malaria in India: Challenges and opportunities. J. Biosci. 2008, 33, 583–592. [Google Scholar] [CrossRef] [PubMed]
- Rana, M.S.; Tanveer, A.; Latif, A.A.; Tahir, A.H. Significant reduction of malaria in the Punjab, Pakistan after introduction of roll back malaria strategy in 2003. Med. Forum Mon. 2011, 22, 54–59. [Google Scholar]
- Weiss, D.J.; Mappin, B.; Dalrymple, U.; Bhatt, S.; Cameron, E.; Hay, S.I.; Gething, P.W. Re-examining environmental correlates of Plasmodium falciparum malaria endemicity: A data-intensive variable selection approach. Malar. J. 2015, 14, 68. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Global Malaria Programme. Global Technical Strategy for Malaria 2016–2030; WHO Press: Geneva, Switzerland, 2015; pp. 1–15. [Google Scholar]
- Ikeda, T.; Behera, S.K.; Morioka, Y.; Minakawa, N.; Hashizume, M.; Tsuzuki, A.; Maharaj, R.; Kruger, P. Seasonally lagged effects of climatic factors on malaria incidence in South Africa. Sci. Rep. 2017, 7, 2458. [Google Scholar] [CrossRef] [PubMed]
- Hay, S.I.; Snow, R.W. The malaria atlas project: Developing global maps of malaria risk. PLoS Med. 2006, 3, 2204–2208. [Google Scholar] [CrossRef] [PubMed]
- Directorate of Malaria Control Program, Pakistan Medical Research Council (PMRC). Malaria Indicator Survey in 38 High Risk Districts of Pakistan—2013–14; PMRC: Islamabad, Pakistan, 2014. Available online: http://dmc.gov.pk/documents/pdfs/3Final%20MIS%20Report-From%20Printe-30%20April%202015%20(2).pdf (accessed on 5 October 2017).
- Hay, S.I.; Guerra, C.A.; Gething, P.W.; Patil, A.P.; Tatem, A.J.; Noor, A.M.; Kabaria, C.W.; Manh, B.H.; Elyazar, I.R.F.; Brooker, S.; et al. A world malaria map: Plasmodium falciparum endemicity in 2007. PLoS Med. 2009, 6, 286–302. [Google Scholar] [CrossRef]
- Cohen, J.M.; Le Menach, A.; Pothin, E.; Eisele, T.P.; Gething, P.W.; Eckhoff, P.A.; Moonen, B.; Schapira, A.; Smith, D.L. Mapping multiple components of malaria risk for improved targeting of elimination interventions. Malar. J. 2017, 16, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Pakistan Bureau of Statistics (PBS). Press Release on Provisional Summary Results of the 6th Population and Housing Census–2017. PBS: Islamabad, Pakistan, 2017; Government of Pakistan, Ministry of Statistics website. Available online: http://www.statistics.gov.pk/assets/publications/Population_Results.pdf (accessed on 3 October 2017).
- Ali, H.; Qamer, F.M.; Ahmed, M.S.; Khan, U.; Habib, A.H.; Chaudhry, A.A.; Ashraf, S.; Khan, B.A. Ecological ranking of districts of Pakistan: A geospatial approach. Pak. J. Bot. 2012, 44, 263–268. [Google Scholar]
- Meghani, S.T.; Sehar, S.; Punjani, N.S. Comparison and analysis of healthcare delivery system: Pakistan versus China. Int. J. Endorsing Health Sci. Res. 2014, 2, 46–49. [Google Scholar]
- Directorate of Malaria Control Program. Pakistan Malaria Program Review (MPR), 2014. Available online: dmc.gov.pk/documents/pdfs/4MPR%20Pakistan.pdf (accessed on 20 November 2017).
- Rowland, M.; Rab, M.A.; Freeman, T.; Durrani, N.; Rehman, N. Afghan refugees and the temporal and spatial distribution of malaria in Pakistan. Soc. Sci. Med. 2002, 55, 2061–2072. [Google Scholar] [CrossRef]
- SPSS Inc. SPSS for Windows, version 13.0; SPSS Inc.: Chicago, IL, USA, 2005. [Google Scholar]
- Kulldorff, B.M. SaTScanTM User Guide V9.4, 2015. Available online: https://www.satscan.org/cgi-bin/satscan/register.pl/SaTScan_Users_Guide.pdf?todo=process_userguide_download (accessed on 9 September 2017).
- Kulldorff, M. A spatial scan statistic. Commun. Stat. Theory Methods 1997, 26, 1481–1496. [Google Scholar] [CrossRef]
- Qi, X.; Hu, W.; Page, A.; Tong, S. Spatial clusters of suicide in Australia. BMC Psychiatry 2012, 12, 86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Environmental Systems Research Institute (ESRI). ArcGIS Desktop, version 10.2; ESRI: Redlands, CA, USA, 2014. [Google Scholar]
- Ullah, Z.; Khattak, A.A.; Bano, R.; Hussain, J.; Awan, U.A.; Rahman, S.U.; Mahsud, M.A.J. High incidence of malaria along the Pak-Afghan bordering area. J. Pak. Med. Assoc. 2018, 68, 42–45. [Google Scholar] [PubMed]
- Kakar, Q.; Khan, M.A.; Bile, K.M. Malaria control in Pakistan: New tools at hand but challenging epidemiological realities. East Mediterr Health J. 2010, 16, S54–S60. [Google Scholar] [CrossRef] [PubMed]
- Mengal, M.H.; Mengal, M.A.; Mengal, M.A.; Rautio, A.; Rehman, F.; Mengal, M.A. Prevalence of drug resistance malaria in Pakistan (Plasmodium vivax and P. falciparum). J. Appl. Emerg. Sci. 2016, 5, 12–19. [Google Scholar]
- Khattak, A.A.; Venkatesan, M.; Nadeem, M.F.; Satti, H.S.; Yaqoob, A.; Strauss, K.; Khatoon, L.; Malik, S.A.; Plowe, C.V. Prevalence and distribution of human Plasmodium infection in Pakistan. Malar. J. 2013, 12, 297. [Google Scholar] [CrossRef] [PubMed]
- Gov Pakistan Stat Div, Pakistan Bureau of Statistics (PBS). Pakistan Social and Living Standards Measurement Survey (2014–15); PBS: Islamabad, Pakistan, 2016. Available online: http://www.pbs.gov.pk/content/pakistan-social-and-living-standards-measurement (accessed on 2 December 2017).
- Karim, A.M.; Hussain, I.; Malik, S.K.; Lee, J.H.; Cho, I.H.; Kim, Y.B.; Lee, S.H. Epidemiology and clinical burden of malaria in the war-torn area, Orakzai Agency in Pakistan. PLoS Negl. Trop. Dis. 2016, 10, e0004399. [Google Scholar] [CrossRef] [PubMed]
- Malik Tareen, A.; Tareen, A.M.; Rafique, M.; Wadood, A.; Qasim, M.; Rahman, H.; Shah, S.H.; Khan, K.; Pirkani, G.S. Malaria burden in human population of Quetta, Pakistan. Eur. J. Microbiol. Immunol. 2012, 2, 201–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yasinzai, M.I.; Kakarsulemankhel, J.K. Prevalence of human malaria infection in district Jhal Magsi of Balochistan. Rawal Med. J. 2012, 37, 9–12. [Google Scholar]
- Yasinzai, M.I.; Kakarsulemankhel, J.K. Frequency of human malaria infection in south-eastern areas of Balochistan: District Lasbella. Pak. J. Med. Sci. 2012, 28, 167–170. [Google Scholar]
- Farooq, M.A.; Salamat, A.; Iqbal, M.A. Malaria—An experience at CMH Khuzdar (Balochistan). J. Coll. Phys. Surg. Pak. 2008, 18, 257–258. [Google Scholar]
- Yasinzai, M.I.; Kakarsulemankhel, J.K. Incidence of human malaria infection in northern hilly region of Balochistan, adjoining with NWFP, Pakistan: District Zhob. Pak. J. Biol. Sci. 2008, 11, 1620–1624. [Google Scholar] [PubMed]
- Awan, Z.U.R.; Shah, H.T.A.; Shah, A.H.; Khan, M.A.; Suleman, M. Malaria among the students of religious schools of Bannu district, Khyber Pakhtunkhwa, Pakistan. Pak. J. Zool. 2012, 44, 959–962. [Google Scholar]
- Majid, A.; Rehman, M.U.; Ahmad, T.; Ali, A.; Ali, S. Prevalence of malaria in human population of district Mardan, Pakistan. World J. Zool. 2016, 11, 63–66. [Google Scholar]
- Nizamani, M.A.; Kalar, N.A.; Khushk, I.A. Burden of malaria in Sindh, Pakistan: A two years surveillance report. J. Liaquat Univ. Med. Health Sci. 2006, 5, 76–83. [Google Scholar]
- Khan, S.Y.; Khan, A.; Arshad, M.; Tahir, H.M.; Mukhtar, M.K.; Ahmad, K.R.; Arshad, N. Irrational use of antimalarial drugs in rural areas of eastern Pakistan: A random field study. BMC Public Health 2012, 12, 941. [Google Scholar] [CrossRef] [PubMed]
- Herrel, N.; Amerasinghe, F.P.; Ensink, J.; Mukhtar, M.; van der Hoek, W.; Konradsen, F. Adult anopheline ecology and malaria transmission in irrigated areas of south Punjab, Pakistan. Med. Vet. Entomol. 2004, 18, 141–152. [Google Scholar] [CrossRef] [PubMed]
- Zubairi, A.B.; Nizami, S.; Raza, A.; Mehraj, V.; Rasheed, A.F.; Ghanchi, N.K.; Khaled, Z.N.; Beg, M.A. Severe Plasmodium vivax malaria in Pakistan. Emerg. Infect. Dis. 2013, 19, 1851–1854. [Google Scholar] [CrossRef] [PubMed]
- Price, R.N.; Douglas, N.M.; Anstey, N.M. New developments in Plasmodium vivax malaria: Severe disease and the rise of chloroquine resistance. Curr. Opin. Infect. Dis. 2009, 22, 430–435. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.P.; Ahmad, F.; Ashfaq, A.; Danish, S.H.; Warsi, S.M.A.; Khan, A.I. Malaria and dengue: Assessment of knowledge among households in rural Sindh, Pakistan. J. Dow Univ. Health Sci. 2015, 9, 106–111. [Google Scholar]
- Imtiaz, F.; Nisar, N.; Shafi, K.; Nawab, F. Knowledge and practices regarding malaria control and its treatment among patients visiting outpatient clinics of civil hospital Khairpur. Ann. Abbasi Shaheed Hosp. Karachi Med. Dent. Coll. 2015, 21, 221–227. [Google Scholar]
- Jamil, S.; Khan, M. Seasonal variations of vivax and falciparum malaria: An observation at a tertiary care hospital. J. Ayub Med. Coll. Abbottabad 2012, 24, 93–95. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Plasmodium vivax | Plasmodium falciparum | Mixed Plasmodium | Total Positive | ||||
|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Min–Max | Mean ± SD | Min–Max | Mean ± SD | Min–Max | Mean ± SD | Min–Max | |
| 2011 | 264.43 ± 523.15 | 0–3745.63 | 181.17 ± 560.99 | 0–5322.22 | 7.26 ± 47.13 | 0–523.01 | 452.85 ± 866.79 | 0–5903.79 |
| 2012 | 259.12 ± 629.89 | 0–4913.11 | 109.42 ± 265.42 | 0–1811.71 | 4.25 ± 19.66 | 0–189.07 | 372.79 ± 786.09 | 0–5805.01 |
| 2013 | 439.90 ± 1528.29 | 0–15,615.63 | 99.04 ± 251.98 | 0–2289.91 | 28.75 ± 105.69 | 0–1112.85 | 568.09 ± 1826.10 | 0–19,018.40 |
| 2014 | 430.25 ± 1202.55 | 0–11,509.69 | 70.54 ± 169.64 | 0–1198.92 | 26.18 ± 80.30 | 0–525.08 | 526.98 ± 1338.77 | 0–12,442.91 |
| 2015 | 278.85 ± 584.71 | 0–3813.32 | 63.42 ± 155.33 | 0–1085.41 | 21.47 ± 74.44 | 0–505.52 | 363.76 ± 733.58 | 0–4335.27 |
| 2016 | 617.27 ± 2096.72 | 0–19,935.05 | 98.61 ± 245.61 | 0–1914.28 | 70.93 ± 215.63 | 0–1687.26 | 786.18 ± 2434.84 | 0–22,071.55 |
| Type of Malaria | Year | Number of Districts in Primary Cluster | Coordinates of Primary Cluster Centroid | Primary Cluster Radius (km) | Primary Cluster Population | Number of Cases in Primary Cluster | Incidence Rate/100,000 | RR | p Value |
|---|---|---|---|---|---|---|---|---|---|
| Plasmodium vivax | 2011 | 5 | 33°00′ N, 70°44′ E | 59.53 | 2,175,181 | 43,211 | 1987.9 | 22.61 | <0.0001 |
| 2012 | 17 | 33°69′ N, 70°31′ E | 142.42 | 11,009,128 | 63,356 | 574.3 | 11.29 | <0.0001 | |
| 2013 | 8 | 32°65’N, 70°39′ E | 49.46 | 2,725,805 | 59,438 | 2182.0 | 23.45 | <0.0001 | |
| 2014 | 25 | 33°00′ N, 70°44′ E | 181.76 | 18,172,987 | 113,900 | 627.2 | 8.76 | <0.0001 | |
| 2015 | 25 | 33°00′ N, 70°44′ E | 181.76 | 18,705,115 | 76,566 | 409.6 | 7.98 | <0.0001 | |
| 2016 | 25 | 33°00′ N, 70°44′ E | 181.76 | 19,253,991 | 136,436 | 707.1 | 10.96 | <0.0001 | |
| Plasmodium falciparum | 2011 | 8 | 30°30′ N, 68°72′ E | 118.93 | 1,293,463 | 21,447 | 1659.2 | 33.96 | <0.0001 |
| 2012 | 19 | 30°04′ N, 67°82′ E | 195.57 | 5,220,346 | 18,683 | 357.1 | 19.17 | <0.0001 | |
| 2013 | 19 | 30°04′ N, 67°82′ E | 195.57 | 5,412,261 | 11,211 | 207.3 | 10.33 | <0.0001 | |
| 2014 | 2 | 25°40′ N, 63°43′ E | 75.41 | 646,999 | 4947 | 765.1 | 49.20 | <0.0001 | |
| 2015 | 1 | 34°04′ N, 71°20′ E | 0 | 854,777 | 4978 | 582.8 | 44.10 | <0.0001 | |
| 2016 | 19 | 30°04′ N, 67°82′ E | 195.57 | 6,039,018 | 13,472 | 222.6 | 15.31 | <0.0001 | |
| Mixed Plasmodium | 2011 | 8 | 29°98′ N, 69°54′ E | 153.44 | 7,719,217 | 13,752 | 178.3 | 22.21 | <0.0001 |
| 2012 | 13 | 25°98′ N, 69°31′ E | 174.87 | 14,988,376 | 2474 | 16.5 | 33.96 | <0.0001 | |
| 2013 | 12 | 25°34′ N, 69°75′ E | 190.84 | 12,975,991 | 4289 | 33.1 | 7.63 | <0.0001 | |
| 2014 | 7 | 31°22′ N, 68°78′ E | 137.22 | 1,173,936 | 3008 | 256.4 | 72.87 | <0.0001 | |
| 2015 | 7 | 31°22′ N, 68°78′ E | 137.22 | 1,205,587 | 1658 | 137.6 | 40.95 | <0.0001 | |
| 2016 | 14 | 32°29′ N, 69°81′ E | 154.61 | 6,303,983 | 9941 | 157.4 | 17.96 | <0.0001 | |
| Total positive | 2011 | 13 | 32°29′ N, 69°81′ E | 153.66 | 5,289,934 | 76,418 | 1445.6 | 9.96 | <0.0001 |
| 2012 | 9 | 33°00′ N, 70°44′ E | 77.62 | 3,986,266 | 49,846 | 1247.9 | 14.19 | <0.0001 | |
| 2013 | 7 | 32°65′ N, 70°39′ E | 49.46 | 2,725,805 | 66,089 | 2426.2 | 19.85 | <0.0001 | |
| 2014 | 15 | 32°29‘ N, 69°81′ E | 158.42 | 6,447,603 | 81,991 | 1272.5 | 11.67 | <0.0001 | |
| 2015 | 25 | 33°00′ N, 70°44′ E | 181.76 | 18,705,115 | 88,869 | 475.4 | 7.17 | <0.0001 | |
| 2016 | 25 | 33°00′ N, 70°44′ E | 181.76 | 19,253,991 | 157,613 | 816.9 | 9.00 | <0.0001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Umer, M.F.; Zofeen, S.; Majeed, A.; Hu, W.; Qi, X.; Zhuang, G. Spatiotemporal Clustering Analysis of Malaria Infection in Pakistan. Int. J. Environ. Res. Public Health 2018, 15, 1202. https://doi.org/10.3390/ijerph15061202
Umer MF, Zofeen S, Majeed A, Hu W, Qi X, Zhuang G. Spatiotemporal Clustering Analysis of Malaria Infection in Pakistan. International Journal of Environmental Research and Public Health. 2018; 15(6):1202. https://doi.org/10.3390/ijerph15061202
Chicago/Turabian StyleUmer, Muhammad Farooq, Shumaila Zofeen, Abdul Majeed, Wenbiao Hu, Xin Qi, and Guihua Zhuang. 2018. "Spatiotemporal Clustering Analysis of Malaria Infection in Pakistan" International Journal of Environmental Research and Public Health 15, no. 6: 1202. https://doi.org/10.3390/ijerph15061202
APA StyleUmer, M. F., Zofeen, S., Majeed, A., Hu, W., Qi, X., & Zhuang, G. (2018). Spatiotemporal Clustering Analysis of Malaria Infection in Pakistan. International Journal of Environmental Research and Public Health, 15(6), 1202. https://doi.org/10.3390/ijerph15061202