The Effect of Methylphenidate and Atomoxetine on Heart Rate and Systolic Blood Pressure in Young People and Adults with Attention-Deficit Hyperactivity Disorder (ADHD): Systematic Review, Meta-Analysis, and Meta-Regression

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
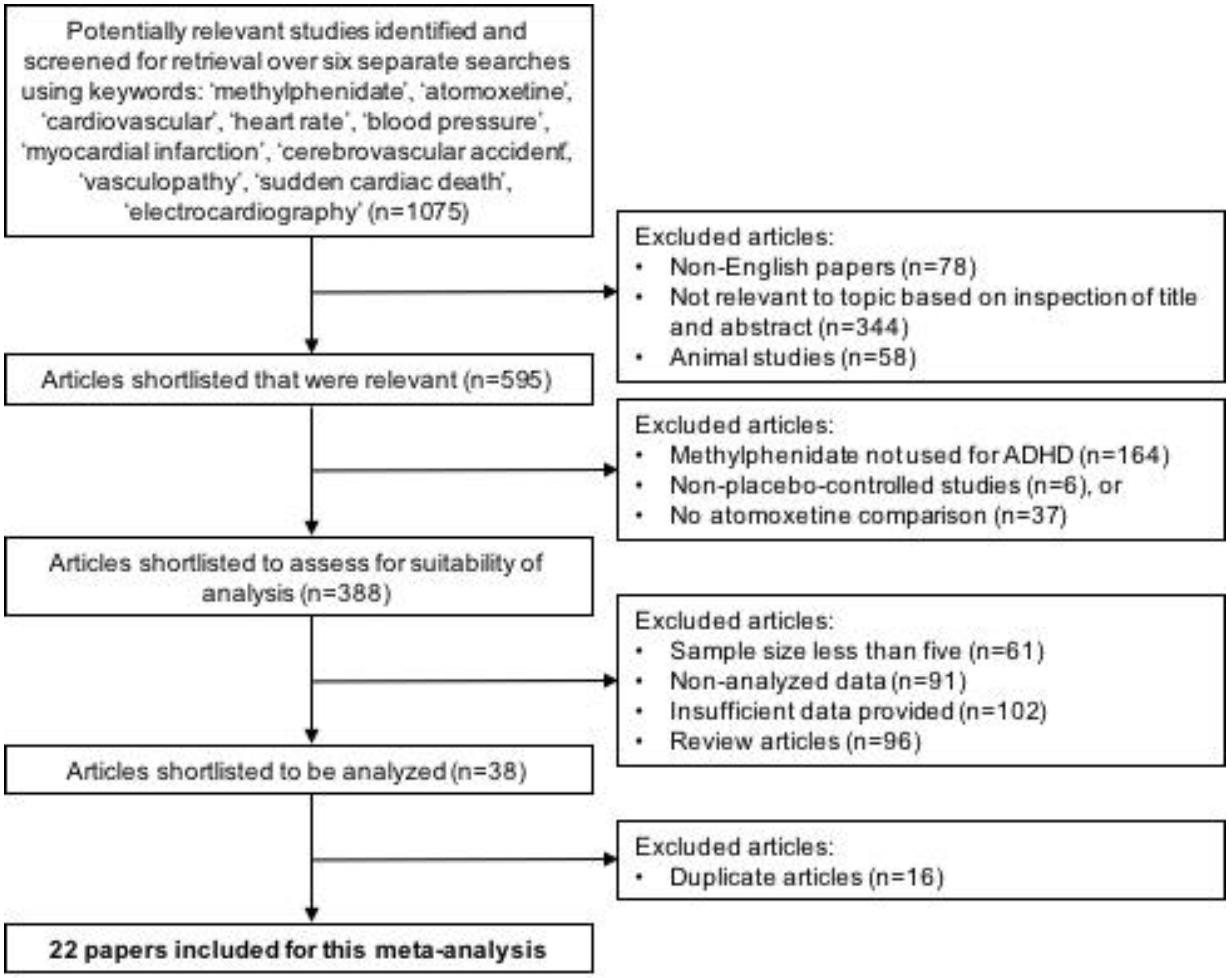
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Outcome Measures of This Meta-Analysis
2.4. Assessment of Quality of Trial
2.5. Statistical Analysis
3. Results
3.1. Articles Included in Data Analyses
3.2. Heart Rate
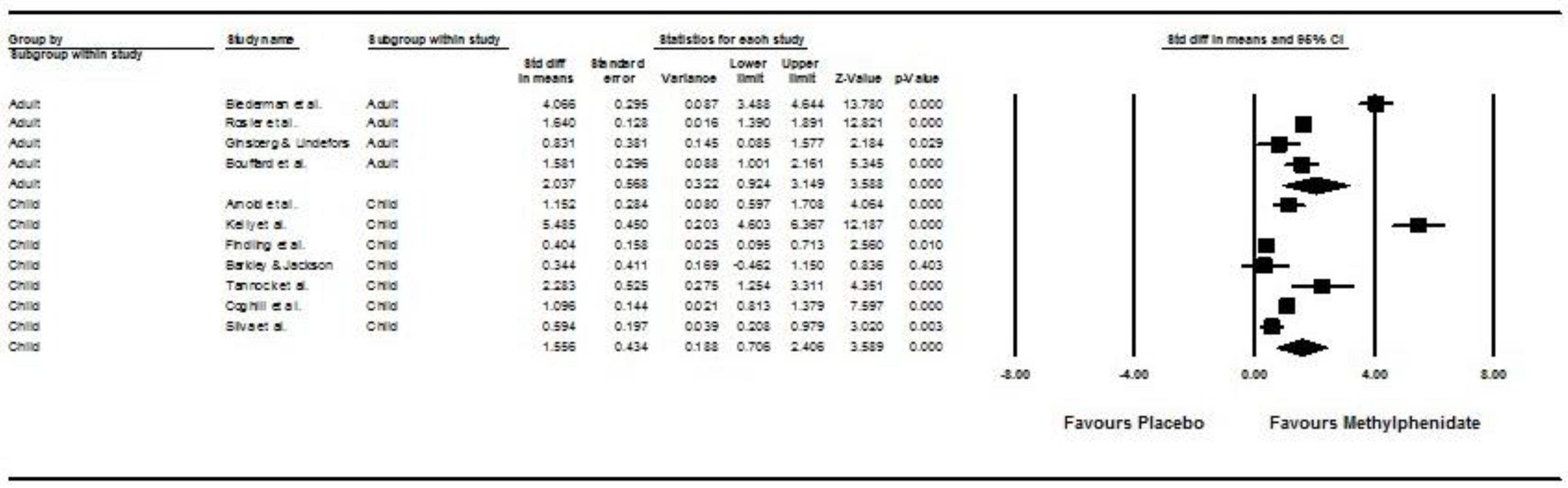
3.2.1. Comparing Post- vs. Pre-Treatment HR between the Methylphenidate and Placebo Groups (Children/Adolescents and Adults)
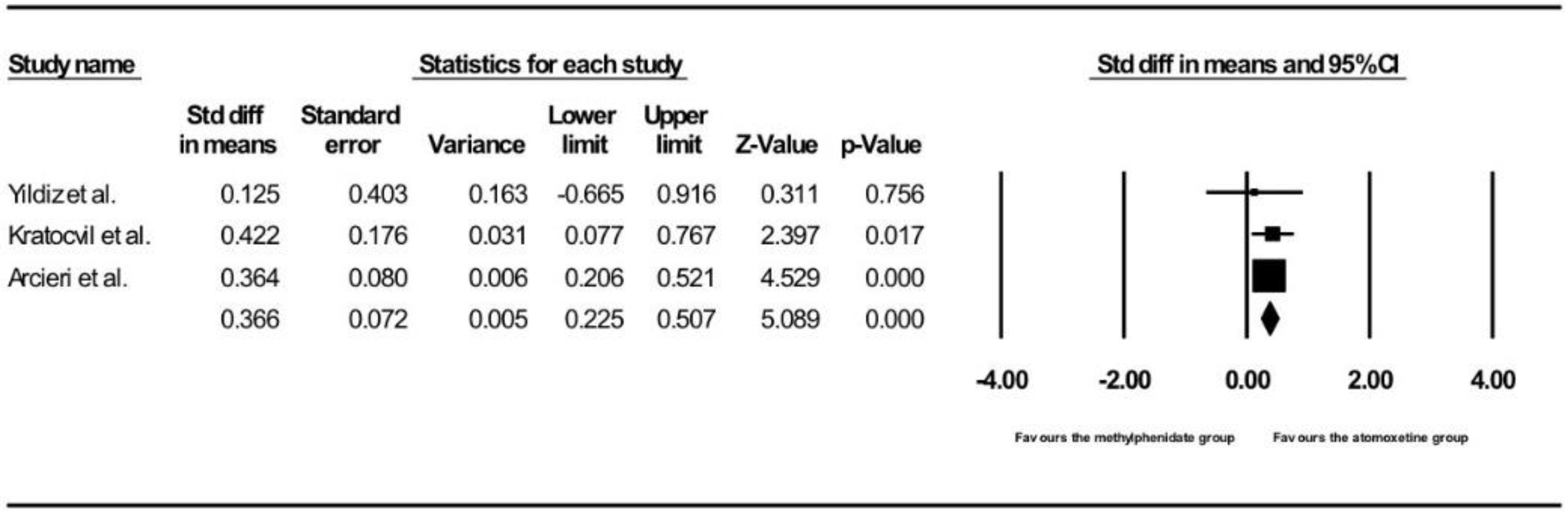
3.2.2. Comparing Post- vs. Pre-Treatment HR between the Methylphenidate and Atomoxetine Groups (Children/Adolescents Only)
3.3. Systolic Blood Pressure
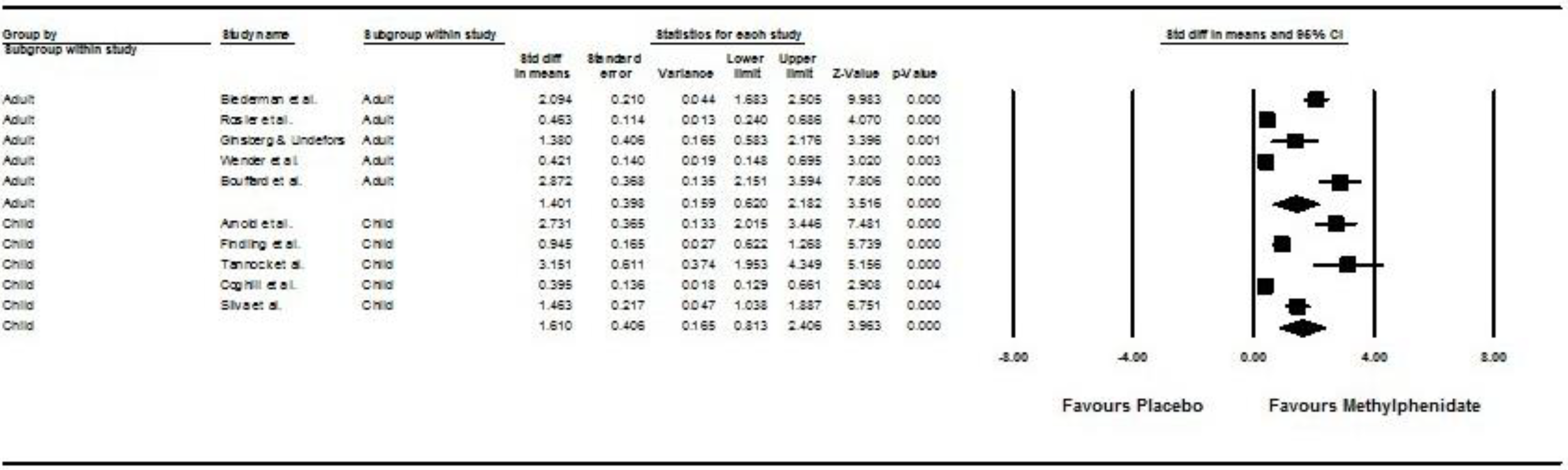
3.3.1. Comparing Post- vs. Pre-Treatment SBP between the Methylphenidate and Placebo Groups (Children/Adolescents/Adults)
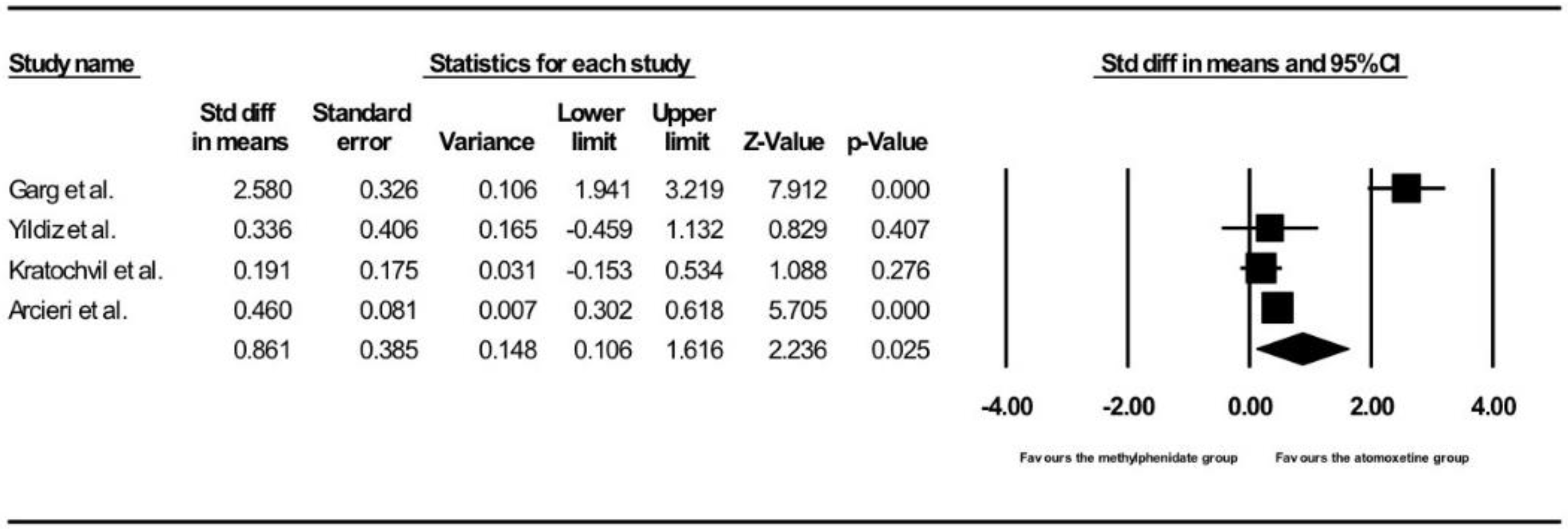
3.3.2. Comparing Post- vs. Pre-Treatment SBP between the Methylphenidate and Atomoxetine Groups (Children/Adolescents Only)
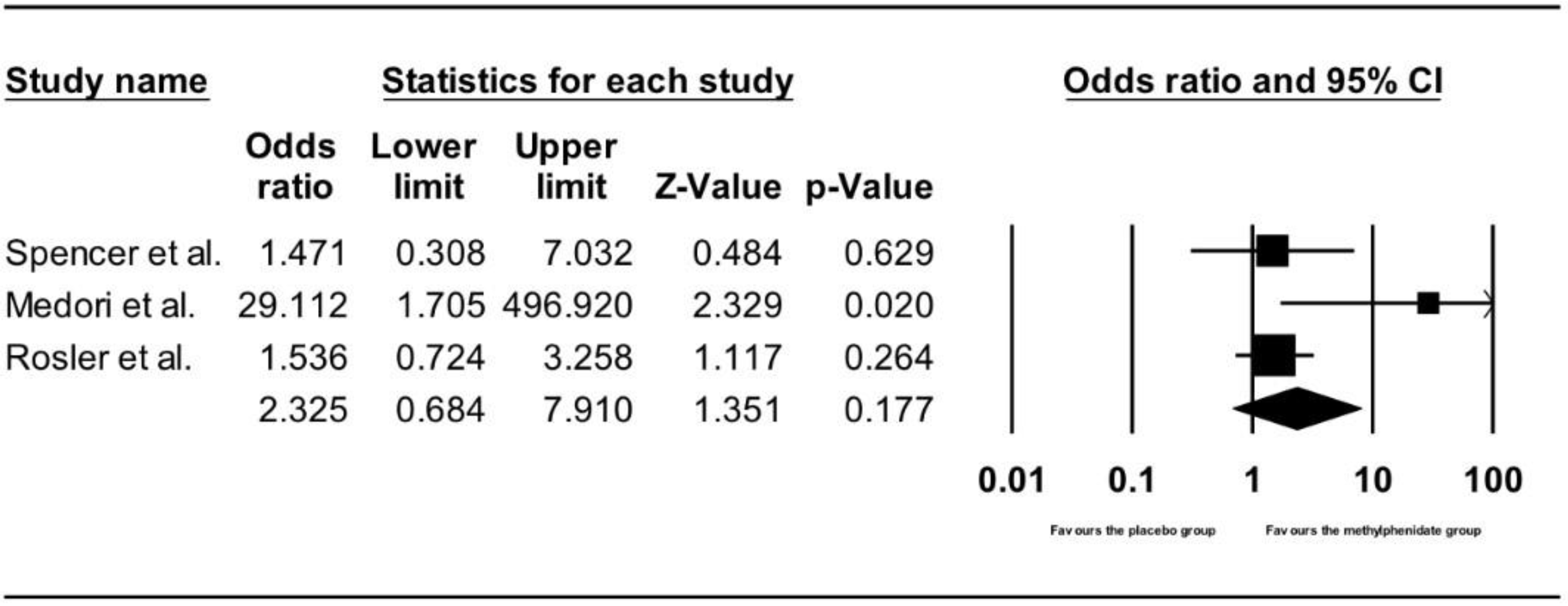
3.3.3. Comparing Number of Adverse Cardiac Events between the Methylphenidate and Placebo Groups in Adults
3.3.4. Comparing Number of Adverse Cardiac Events between the Methylphenidate and Atomoxetine Groups in Children and Adolescents
4. Discussion
4.1. Principal Findings
4.2. Comparison with Other Studies
4.3. Mechanisms Leading to Increase in HR and SBP
4.4. Clinical Implications
4.5. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Willcutt, E.G. The prevalence of DSM-IV attention-deficit/hyperactivity disorder: A meta-analytic review. Neurotherapeutics 2012, 3, 490–499. [Google Scholar] [CrossRef] [PubMed]
- Visser, S.N.; Danielson, M.L.; Bitsko, R.H.; Perou, R.; Blumberg, S.J. Convergent validity of parent-reported attention-deficit/hyperactivity disorder diagnosis: A cross-study comparison. JAMA Pediatr. 2013, 167, 674–675. [Google Scholar] [CrossRef] [PubMed]
- Singh, I. Beyond polemics: Science and ethics of ADHD. Nat. Rev. Neurosci. 2008, 12, 957–964. [Google Scholar] [CrossRef] [PubMed]
- Kooij, S.J.; Bejerot, S.; Blackwell, A.; Caci, H.; Casas-BruguÃ, M.; Carpentier, P.J.; Edvinsson, D.; Fayyad, J.; Foeken, K.; Fitzgerald, M.; et al. European consensus statement on diagnosis and treatment of adult ADHD: The European Network Adult ADHD. BMC Psychiatry 2010, 10, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, P.S. A 14-month randomized clinical trial of treatment strategies for attention-deficit/hyperactivity disorder. Arch. Gen. Psychiatry 1999, 56, 1073–1086. [Google Scholar]
- National Institute of Clinical Excellence (NICE). Attention Deficit Hyperactivity Disorder. Evidence Update July 2013. Available online: https://www.nice.org.uk/guidance/cg72/evidence/evidence-update-241959277 (accessed on 1 May 2018).[Green Version]
- Lamberti, M.; Italiano, D.; Guerriero, L.; D’Amico, G.; Siracusano, R.; Ingrassia, M.; Germanò, E.; Calabrò, M.P.; Spina, E.; Gagliano, A. Evaluation of acute cardiovascular effects of immediate-release methylphenidate in children and adolescents with attention-deficit hyperactivity disorder. Neuropsychiatr. Dis. Treat. 2015, 11, 1169–1174. [Google Scholar] [CrossRef] [PubMed]
- Puri, B.; Hall, A.; Ho, R.C. (Eds.) Revision Notes in Psychiatry, 3rd ed.; CRC Press: New York, NY, USA, 2014. [Google Scholar]
- Kratochvil, C.J. ADHD pharmacotherapy: Rates of stimulant use and cardiovascular risk. Am. J. Psychiatry 2012, 169, 112–114. [Google Scholar] [CrossRef] [PubMed]
- Maxwell, R.A.; Plummer, A.J.; Ross, S.D.; Daniel, A.L. Studies concerning the cardiovascular actions of the central nervous stimulant, methylphenidate. J. Pharmacol. Exp. Ther. 1958, 123, 22–27. [Google Scholar] [PubMed]
- Ballard, J.E.; Boileau, R.A.; Sleator, E.K.; Massey, B.H.; Sprague, R.L. Cardiovascular responses of hyperactive children to methylphenidate. JAMA 1976, 236, 2870–2874. [Google Scholar] [CrossRef] [PubMed]
- Buchhorn, R.; Müller, C.; Willaschek, C.; Norozi, K. How to predict the impact of methylphenidate on cardiovascular risk in children with attention deficit disorder: Methylphenidate improves autonomic dysfunction in children with ADHD. ISRN Pharmacol. 2012, 2012, 170935. [Google Scholar] [CrossRef] [PubMed]
- Arcieri, R.; Germinario, E.; Bonati, M.; Masi, G.; Zuddas, A.; Vella SChiarotti, F.; Panei, P. Italian Attention-Deficit/Hyperactivity Disorder Regional Reference Centers. Cardiovascular Measures in Children and Adolescents with Attention-Deficit/Hyperactivity Disorder Who Are New Users of Methylphenidate and Atomoxetine. J. Child Adolesc. Psychopharmacol. 2012, 22, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Westover, A.N.; Halm, E.A. Do prescription stimulants increase the risk of adverse cardiovascular events?: A systematic review. BMC Cardiovasc. Disord. 2012, 12, 41. [Google Scholar] [CrossRef] [PubMed]
- Awudu, G.A.; Besag, F.M. Cardiovascular effects of methylphenidate, amphetamines and atomoxetine in the treatment of attention-deficit hyperactivity disorder: An update. Drug Saf. 2014, 37, 661–676. [Google Scholar] [CrossRef] [PubMed]
- Mick, E.; McManus, D.D.; Goldberg, R.J. Meta-analysis of increased heart rate and blood pressure associated with CNS stimulant treatment of ADHD in adults. Eur. Neuropsychopharmacol. 2013, 23, 534–541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hennissen, L.; Bakker, M.J.; Banaschewski, T.; Carucci, S.; Coghill, D.; Danckaerts, M.; Dittmann, R.W.; Hollis, C.; Kovshoff, H.; McCarthy, S.; et al. Cardiovascular Effects of Stimulant and Non-Stimulant Medication for Children and Adolescents with ADHD: A Systematic Review and Meta-Analysis of Trials of Methylphenidate, Amphetamines and Atomoxetine. CNS Drugs 2017, 31, 199–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montastruc, F.; Montastruc, G.; Montastruc, J.L.; Revet, A. Cardiovascular safety of methylphenidate should also be considered in adults. BMJ 2016, 353, i3418. [Google Scholar] [CrossRef] [PubMed]
- Schelleman, H.; Bilker, W.B.; Kimmel, S.E.; Daniel, G.W.; Newcomb, C.; Guevara, J.P.; Cziraky, M.J.; Strom, B.L.; Hennessy, S. Methylphenidate and risk of serious cardiovascular events in adults. Am. J. Psychiatry 2012, 169, 178–185. [Google Scholar] [CrossRef] [PubMed]
- Cortese, S.; Adamo, N.; Del Giovane, C.; Mohr-Jensen, C.; Hayes, A.J.; Carucci, S.; Atkinson, L.Z.; Tessari, L.; Banaschewski, T.; Coghill, D.; et al. Comparative efficacy and tolerability of medications for attention deficit hyperactivity disorder in children, adolescents, and adults: A systematic review and network meta-analysis. Lancet Psychiatry 2018, in press. [Google Scholar] [CrossRef]
- Shin, J.Y.; Roughead, E.E.; Park, B.J.; Pratt, N.L. Cardiovascular safety of methylphenidate among children and young people with attention-deficit/hyperactivity disorder (ADHD): Nationwide self controlled case series study. BMJ 2016, 353, i2550. [Google Scholar] [CrossRef] [PubMed]
- Olfson, M.; Huang, C.; Gerhard, T.; Winterstein, A.G.; Crystal, S.; Allison, P.D.; Marcus, S.C. Stimulants and cardiovascular events in youth with attention-deficit/hyperactivity disorder. J. Am. Acad. Child Adolesc. Psychiatry 2012, 51, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Strandberg, T.E.; Pitkala, K. What is the most important component of blood pressure: Systolic, diastolic or pulse pressure? Curr. Opin. Nephrol. Hypertens. 2003, 12, 293–297. [Google Scholar] [CrossRef] [PubMed]
- Jadad, A.; Moore, A.; Carroll, D.; Jenkinson, C.; Reynolds, J.; Gavaghan, D.; McQuay, H. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Reprint—Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Phys. Ther. 2009, 89, 873–880. [Google Scholar] [PubMed]
- Ho, R.C.; Ong, H.S.; Kudva, K.G.; Cheung, M.W.; Mak, A. How to critically appraise and apply meta-analyses in clinical practice. Int. J. Rheum. Dis. 2010, 13, 294–299. [Google Scholar] [CrossRef] [PubMed]
- Cheung, M.W.; Ho, R.C.; Lim, Y.; Mak, A. Conducting a meta-analysis: Basics and good practices. Int. J. Rheum. Dis. 2012, 15, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Loh, A.Z.; Tan, J.S.; Zhang, M.W.; Ho, R.C. The Global Prevalence of Anxiety and Depressive Symptoms Among Caregivers of Stroke Survivors. J. Am. Med. Dir. Assoc. 2017, 18, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Ho, R.C.; Thiaghu, C.; Ong, H.; Lu, Y.; Ho, C.S.; Tam, W.W.; Zhang, M.W. A meta-analysis of serum and cerebrospinal fluid autoantibodies in neuropsychiatric systemic lupus erythematosus. Autoimmun. Rev. 2016, 15, 124–138. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Mak, K.K.; van Bever, H.P.; Ng, T.P.; Mak, A.; Ho, R.C. Prevalence of anxiety and depressive symptoms in adolescents with asthma: A meta-analysis and meta-regression. Pediatr. Allergy Immunol. 2012, 23, 707–715. [Google Scholar] [CrossRef] [PubMed]
- Puthran, R.; Zhang, M.W.; Tam, W.W.; Ho, R.C. Prevalence of depression amongst medical students: A meta-analysis. Med. Educ. 2016, 50, 456–468. [Google Scholar] [CrossRef] [PubMed]
- Arnold, L. Methylphenidate vs. Dextroamphetamine vs. Caffeine in Minimal Brain Dysfunction. Arch. Gen. Psychiatry 1978, 35, 463–473. [Google Scholar] [CrossRef] [PubMed]
- Kelly, K.; Rapport, M.; DuPaul, G. Attention Deficit Disorder and Methylphenidate: A Multi-step Analysis of Dose-response Effects on Children’s Cardiovascular Functioning. Int. Clin. Psychopharmacol. 1988, 3, 167–181. [Google Scholar] [CrossRef] [PubMed]
- Findling, R.; Short, E.; Manos, M. Short-Term Cardiovascular Effects of Methylphenidate and Adderall. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 525–529. [Google Scholar] [CrossRef] [PubMed]
- Biederman, J.; Mick, E.; Surman, C.; Doyle, R.; Hammerness, P.; Harpold, T.; Dunkel, S.; Dougherty, M.; Aleardi, M.; Spencer, T. A Randomized, Placebo-Controlled Trial of OROS Methylphenidate in Adults with Attention-Deficit/Hyperactivity Disorder. Biol. Psychiatry 2006, 59, 829–835. [Google Scholar] [CrossRef] [PubMed]
- Barkley, R.; Jackson, T. Hyperkinesis, autonomic nervous system activity and stimulant drug effects. J. Child Psychol. Psychiatry 1977, 18, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Tannock, R.; Schachar, R.; Carr, R.; Logan, G. Dose-Response Effects of Methylphenidate on Academic Performance and Overt Behavior in Hyperactive Children. Am. Acad. Pediatr. 1989, 84, 648–657. [Google Scholar]
- Rösler, M.; Fischer, R.; Ammer, R.; Ose, C.; Retz, W. A randomised, placebo-controlled, 24-week, study of low-dose extended-release methylphenidate in adults with attention-deficit/hyperactivity disorder. Eur. Arch. Psychiatry Clin. Neurosci. 2009, 259, 120–129. [Google Scholar] [CrossRef]
- Ginsberg, Y.; Lindefors, N. Methylphenidate treatment of adult male prison inmates with attention-deficit hyperactivity disorder: Randomised double-blind placebo-controlled trial with open-label extension. Br. J. Psychiatry 2012, 200, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Bouffard, R.; Hechtman, L.; Minde, K.; Iaboni-Kassab, F. The Efficacy of 2 Different Dosages of Methylphenidate in Treating Adults with Attention-Deficit Hyperactive Disorder. Can. J. Psychiatry 2003, 48, 546–554. [Google Scholar] [CrossRef] [PubMed]
- Coghill, D.; Banaschewski, T.; Lecendreux, M.; Soutullo, C.; Johnson, M.; Zuddas, A.; Anderson, C.; Civil, R.; Higgins, N.; Lyne, A.; et al. European, randomized, phase 3 study of lisdexamfetamine dimesylate in children and adolescents with attention-deficit/hyperactivity disorder. Eur. Neuropsychopharmacol. 2013, 23, 1208–1218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, R.; Muniz, R.; Pestreich, L.; Brams, M.; Childress, A.; Lopez, F. Efficacy of Two Long-Acting Methylphenidate Formulations in Children with Attention- Deficit/Hyperactivity Disorder in a Laboratory Classroom Setting. J. Child Adolesc. Psychopharmacol. 2005, 15, 637–654. [Google Scholar] [CrossRef] [PubMed]
- Garg, J.; Arun, P.; Chavan, B. Comparative short term efficacy and tolerability of methylphenidate and atomoxetine in attention deficit hyperactivity disorder. Indian Pediatr. 2014, 51, 550–554. [Google Scholar] [CrossRef] [PubMed]
- Yildiz, O.; Sismanlar, S.; Memik, N.; Karakaya, I.; Agaoglu, B. Atomoxetine and Methylphenidate Treatment in Children with ADHD: The Efficacy, Tolerability and Effects on Executive Functions. Child Psychiatry Hum. Dev. 2010, 42, 257–269. [Google Scholar] [CrossRef] [PubMed]
- Kratochvil, C.J.; Heiligenstein, J.H.; Dittmann, R.; Spencer, T.J.; Biederman, J.; Wernicke, J.; Newcorn, J.H.; Casat, C.; Milton, D.; Michelson, D. Atomoxetine and Methylphenidate Treatment in Children with ADHD: A Prospective, Randomized, Open-Label Trial. J. Am. Acad. Child Adolesc. Psychiatry 2002, 41, 776–784. [Google Scholar] [CrossRef] [PubMed]
- Wender, P.; Reimherr, F.; Marchant, B.; Sanford, M.; Czajkowski, L.; Tomb, D. A One Year Trial of Methylphenidate in the Treatment of ADHD. J. Atten. Disord. 2010, 15, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Spencer, T.; Adler, L.; McGough, J.; Muniz, R.; Jiang, H.; Pestreich, L. Efficacy and Safety of Dexmethylphenidate Extended-Release Capsules in Adults with Attention-Deficit/Hyperactivity Disorder. Biol. Psychiatry 2007, 61, 1380–1387. [Google Scholar] [CrossRef] [PubMed]
- Medori, R.; Ramos-Quiroga, J.; Casas, M.; Kooij, J.; Niemelä, A.; Trott GLee, E.; Buitelaar, J.K. A Randomized, Placebo-Controlled Trial of Three Fixed Dosages of Prolonged-Release OROS Methylphenidate in Adults with Attention-Deficit/Hyperactivity Disorder. Biol. Psychiatry 2008, 63, 981–989. [Google Scholar] [CrossRef] [PubMed]
- Guertin, J.; LeLorier, J.; Durand, M.; Gow, R.; Holbrook, A.; Levine, M. Impact of a Restrictive Drug Access Program on the Risk of Cardiovascular Encounters in Children Exposed to ADHD Medications. J. Popul. Ther. Clin. Pharmacol. 2014, 21, e357–e369. [Google Scholar] [PubMed]
- Cortese, S.; Panei, P.; Arcieri, R.; Germinario, E.; Capuano, A.; Margari LChiarotti, F.; Curatolo, P. Safety of Methylphenidate and Atomoxetine in Children with Attention-Deficit/Hyperactivity Disorder (ADHD): Data from the Italian National ADHD Registry. CNS Drugs 2015, 29, 865–877. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, S.; Rafaniello, C.; Bravaccio, C.; Grimaldi, G.; Granato, R.; Pascotto, A.; Sportiello, L.; Parretta, E.; Rinaldi, B.; Panei, P.; et al. Safety of Attention-Deficit/Hyperactivity Disorder Medications in Children: An Intensive Pharmacosurveillance Monitoring Study. J. Child Adolesc. Psychopharmacol. 2012, 22, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Shang, C.; Pan, Y.; Lin, H.; Huang, L.; Gau, S. An Open-Label, Randomized Trial of Methylphenidate and Atomoxetine Treatment in Children with Attention-Deficit/Hyperactivity Disorder. J. Child Adolesc. Psychopharmacol. 2015, 25, 566–573. [Google Scholar] [CrossRef] [PubMed]
- Joyce, P.R.; Nicholls, M.G.; Donald, R.A. Methylphenidate increases heart rate, blood pressure and plasma epinephrine in normal subjects. Life Sci. 1984, 34, 1707–1711. [Google Scholar] [CrossRef]
- Volkow, N.D.; Wang, G.J.; Fowler, J.S.; Molina, P.E.; Logan, J.; Gatley, S.J.; Gifford, A.; Ding, Y.S.; Wong, C.; Pappas, N.R.; et al. Cardiovascular effects of methylphenidate in humans are associated with increases of dopamine in brain and of epinephrine in plasma. Psychopharmacology 2003, 166, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Wakamatsu, A.; Nomura, S.; Tate, Y.; Shimizu, S.; Harada, Y. Effects of methylphenidate hydrochloride on the cardiovascular system In Vivo and In Vitro: A safety pharmacology study. J. Pharmacol. Toxicol. Methods 2009, 59, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Michelson, D.; Read, H.A.; Ruff, D.D.; Witcher, J.; Zhang, S.; McCracken, J. CYP2D6 and clinical response to atomoxetine in children and adolescents with ADHD. J. Am. Acad. Child Adolesc. Psychiatry 2007, 46, 242–251. [Google Scholar] [CrossRef] [PubMed]
- Kelly, R.P.; Yeo, K.P.; Teng, C.H.; Smith, B.P.; Lowe, S.; Soon, D.; Read, H.A.; Wise, S.D. Hemodynamic effects of acute administration of atomoxetine and methylphenidate. J. Clin. Pharmacol. 2005, 45, 851–855. [Google Scholar] [CrossRef] [PubMed]
- Ho, R.C.; Neo, L.F.; Chua, A.N.; Cheak, A.A.; Mak, A. Research on psychoneuroimmunology: Does stress influence immunity and cause coronary artery disease? Ann. Acad. Med. Singap. 2010, 39, 191–196. [Google Scholar] [PubMed]
- Medicines & Healthcare Products and Regulatory Agency (UK). Available online: https://www.gov.uk/drug-safety-update/atomoxetine-strattera-increases-in-blood-pressure-and-heart-rate (accessed on 1 May 2018).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Design * | Comparison * | Dose | n | Age (Mean) | % Male | Study Population | Study Duration (Weeks) | Jadad Score |
|---|---|---|---|---|---|---|---|---|---|
| Arnold et al. (1978) [32] | RCT (CO) | MPH (n = 29) vs. placebo (n = 29) | MPH: 3.6 mg/day | 58 | 8.0 | 0.759 | Children | 3 | 4 |
| Kelly et al. (1988) [33] | RCT (CO) | MPH (n = 47) vs. placebo (n = 47) | MPH: 20 mg/week | 94 | 8.3 | 0.936 | Children | 5 | 3 |
| Findling et al. (2001) [34] | RCT | MPH (n = 82) vs. placebo (n = 82) | MPH: 5–15 mg/day | 164 | 10.0 | 0.805 | Children and adolescents | 1 | 1 |
| Biederman et al. (2006) [35] | RCT | MPH (n = 67) vs. placebo (n = 74) | MPH: 1.3 mg/kg/day | 141 | 40.5 | 0.518 | Adults | 6 | 4 |
| Barkley & Jackson (1977) [36] | RCT (CO) | MPH (n = 12) vs. placebo (n = 12) | MPH: 10–25 mg/day | 24 | 8.2 | 1.000 | Children | 2 | 4 |
| Tannock et al. (1989) [37] | RCT (CO) | MPH (n = 12) vs. placebo (n = 12) | MPH: 1 mg/kg/day | 24 | 8.4 | 0.830 | Children | 0.86 | 4 |
| Rosler et al. (2009) [38] | RCT | MPH (n = 241) vs. placebo (n = 118) | MPH: 10–60 mg/day | 359 | 34.7 | 0.496 | Adults | 24 | 3 |
| Ginsberg & Lindefors (2011) [39] | RCT | MPH (n = 15) vs. placebo (n = 15) | MPH: 36–72 mg/day | 30 | 34.4 | 1.000 | Adults | 47 | 5 |
| Bouffard et al. (2003) [40] | RCT (CO) | MPH (n = 30) vs. placebo (n = 30) | MPH: 30–45 mg/day | 60 | 34.0 | 0.800 | Adults | 4 | 5 |
| Coghill et al. (2013) [41] | RCT | MPH (n = 111) vs. placebo (n = 110) | MPH: 18–54 mg/day | 221 | 10.9 | 0.819 | Children and adolescents | 7 | 5 |
| Silva et al. (2005) [42] | RCT (CO) | MPH (n = 54) vs. placebo (n = 54) | MPH: 18–40 mg/day | 108 | 9.4 | 0.630 | Children | 6 | 3 |
| Garg et al. (2014) [43] | RCT | MPH (n = 33) vs. ATX (n = 36) | MPH: 0.2–1 mg/kg/day ATX: 0.5 mg/kg/day | 69 | 8.6 | 0.812 | Children | 8 | 3 |
| Yildiz et al. (2011) [44] | RCT | MPH (n = 11) vs. ATX (n = 14) | MPH: 18–54 mg/day ATX: 0.5–1.2 mg/kg/day | 25 | 9.9 | 0.880 | Children | 12 | 2 |
| Kratochvil et al. (2002) [45] | RCT | MPH (n = 40) vs. ATX (n = 180) | MPH: 15–60 mg/day ATX: 0.2–1 mg/kg/day | 220 | 10.4 | 0.925 | Children and adolescents | 10 | 3 |
| Wender et al. (2011) [46] | RCT (CO) | MPH (n = 105) vs. placebo (n = 105) | MPH: 30–60 mg/day | 210 | 36.9 | 0.724 | Adults | 52 | 5 |
| Spencer et al. (2007) [47] | RCT | MPH (n = 165) vs. placebo (n = 53) | MPH: 20–40 mg/day | 218 | 38.6 | 0.574 | Adults | 5 | 3 |
| Medori et al. (2008) [48] | RCT | MPH (n = 102) vs. placebo (n = 96) | MPH: 18–72 mg/day | 198 | 34.0 | 0.576 | Adults | 5 | 4 |
| Arcieri et al. (2012) [13] | CS | MPH (n = 315) vs. ATX (n = 316) | MPH: 0.3–0.6 mg/kg/day ATX: 0.5–1.2 mg/kg/day | 631 | 10.6 | 0.883 | Children and adolescents | 52 | NA |
| Guertin et al. (2014) [49] | CS | MPH (n = 37011) vs. ATX (n = 3595) | Variable doses | 40606 | 9.1 | 0.703 | Children | 13 | NA |
| Cortese et al. (2015) [50] | Retrospective CS | MPH (n = 1426) vs. ATX (n = 985) | MPH: 0.3–0.6 mg/kg/day ATX: 0.5–1.2 mg/kg/day | 2411 | 10.7 | 0.881 | Children and adolescents | 240 | NA |
| Ruggiero et al. (2012) [51] | Retrospective CS | MPH (n = 8) vs. ATX (n = 68) | Variable doses | 76 | 9.6 | 0.868 | Children | Variable duration | NA |
| Shang et al. (2015) [52] | RCT | MPH (n = 80) vs. ATX (n = 80) | MPH: 18–54 mg/day ATX: 0.5–1.2 mg/kg/day | 160 | 9.8 | 0.875 | Children and adolescents | 24 | 3 |
| Moderators | No. of Studies Used | Slope | Standard Error | Lower Limit (95% CI) | Upper Limit (95% CI) | Z-Value | p-Value |
|---|---|---|---|---|---|---|---|
| Mean age of all participants | 11 | 0.0032 | 0.00044 | 0.0023 | 0.0041 | 7.31 | <0.001 |
| Proportion of male gender in all participants | 11 | −1.88 | 0.41 | −2.70 | −1.06 | −4.50 | <0.001 |
| Duration of treatment of the methylphenidate and placebo groups | 11 | 0.011 | 0.0055 | 0.00057 | 0.022 | 2.06 | 0.04 |
| Mean dose of methylphenidate | 10 | 0.032 | 0.0049 | 0.022 | 0.042 | 6.53 | <0.001 |
| Moderators | No. of Studies Used | Slope | Standard Error | Lower Limit (95% CI) | Upper Limit (95% CI) | Z-Value | p-Value |
|---|---|---|---|---|---|---|---|
| Mean age of all participants | 4 | −0.079 | 0.013 | −0.10 | −0.05 | −5.90 | p < 0.001 |
| Proportion of male gender in all participants | 4 | −17.7 | 3.12 | −23.82 | −11.59 | −5.67 | p < 0.001 |
| Duration of treatment of the methylphenidate and atomoxetine groups | 4 | −0.02 | 0.01 | −0.04 | 0.002 | −1.77 | 0.08 |
| Mean dose of methylphenidate | 4 | −0.082 | 0.02 | −0.11 | −0.05 | −5.12 | p < 0.001 |
| Mean dose of atomoxetine | 4 | −0.047 | 0.009 | −0.065 | −0.03 | −5.27 | p < 0.001 |
| Moderators | No. of Studies Used | Slope | Standard Error | Lower Limit (95% CI) | Upper Limit (95% CI) | Z-Value | p-Value |
|---|---|---|---|---|---|---|---|
| Mean age of all participants | 10 | −0.00037 | 0.00038 | −0.0011 | 0.00037 | −0.98 | 0.33 |
| Proportion of male gender in all participants | 10 | 0.19 | 0.42 | −0.63 | 1.00 | 0.44 | 0.65 |
| Duration of treatment of the methylphenidate and placebo | 10 | −0.016 | 0.0053 | −0.026 | −0.0058 | −3.07 | 0.0022 * |
| Mean dose of methylphenidate | 9 | 0.013 | 0.0050 | 0.0035 | 0.0023 | 2.66 | 0.0079 * |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liang, E.F.; Lim, S.Z.; Tam, W.W.; Ho, C.S.; Zhang, M.W.; McIntyre, R.S.; Ho, R.C. The Effect of Methylphenidate and Atomoxetine on Heart Rate and Systolic Blood Pressure in Young People and Adults with Attention-Deficit Hyperactivity Disorder (ADHD): Systematic Review, Meta-Analysis, and Meta-Regression. Int. J. Environ. Res. Public Health 2018, 15, 1789. https://doi.org/10.3390/ijerph15081789
Liang EF, Lim SZ, Tam WW, Ho CS, Zhang MW, McIntyre RS, Ho RC. The Effect of Methylphenidate and Atomoxetine on Heart Rate and Systolic Blood Pressure in Young People and Adults with Attention-Deficit Hyperactivity Disorder (ADHD): Systematic Review, Meta-Analysis, and Meta-Regression. International Journal of Environmental Research and Public Health. 2018; 15(8):1789. https://doi.org/10.3390/ijerph15081789
Chicago/Turabian StyleLiang, Edwin F., Samuel Z. Lim, Wilson W. Tam, Cyrus S. Ho, Melvyn W. Zhang, Roger S. McIntyre, and Roger C. Ho. 2018. "The Effect of Methylphenidate and Atomoxetine on Heart Rate and Systolic Blood Pressure in Young People and Adults with Attention-Deficit Hyperactivity Disorder (ADHD): Systematic Review, Meta-Analysis, and Meta-Regression" International Journal of Environmental Research and Public Health 15, no. 8: 1789. https://doi.org/10.3390/ijerph15081789
APA StyleLiang, E. F., Lim, S. Z., Tam, W. W., Ho, C. S., Zhang, M. W., McIntyre, R. S., & Ho, R. C. (2018). The Effect of Methylphenidate and Atomoxetine on Heart Rate and Systolic Blood Pressure in Young People and Adults with Attention-Deficit Hyperactivity Disorder (ADHD): Systematic Review, Meta-Analysis, and Meta-Regression. International Journal of Environmental Research and Public Health, 15(8), 1789. https://doi.org/10.3390/ijerph15081789