Is Perceived Exertion a Useful Indicator of the Metabolic and Cardiovascular Responses to a Metabolic Conditioning Session of Functional Fitness?

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
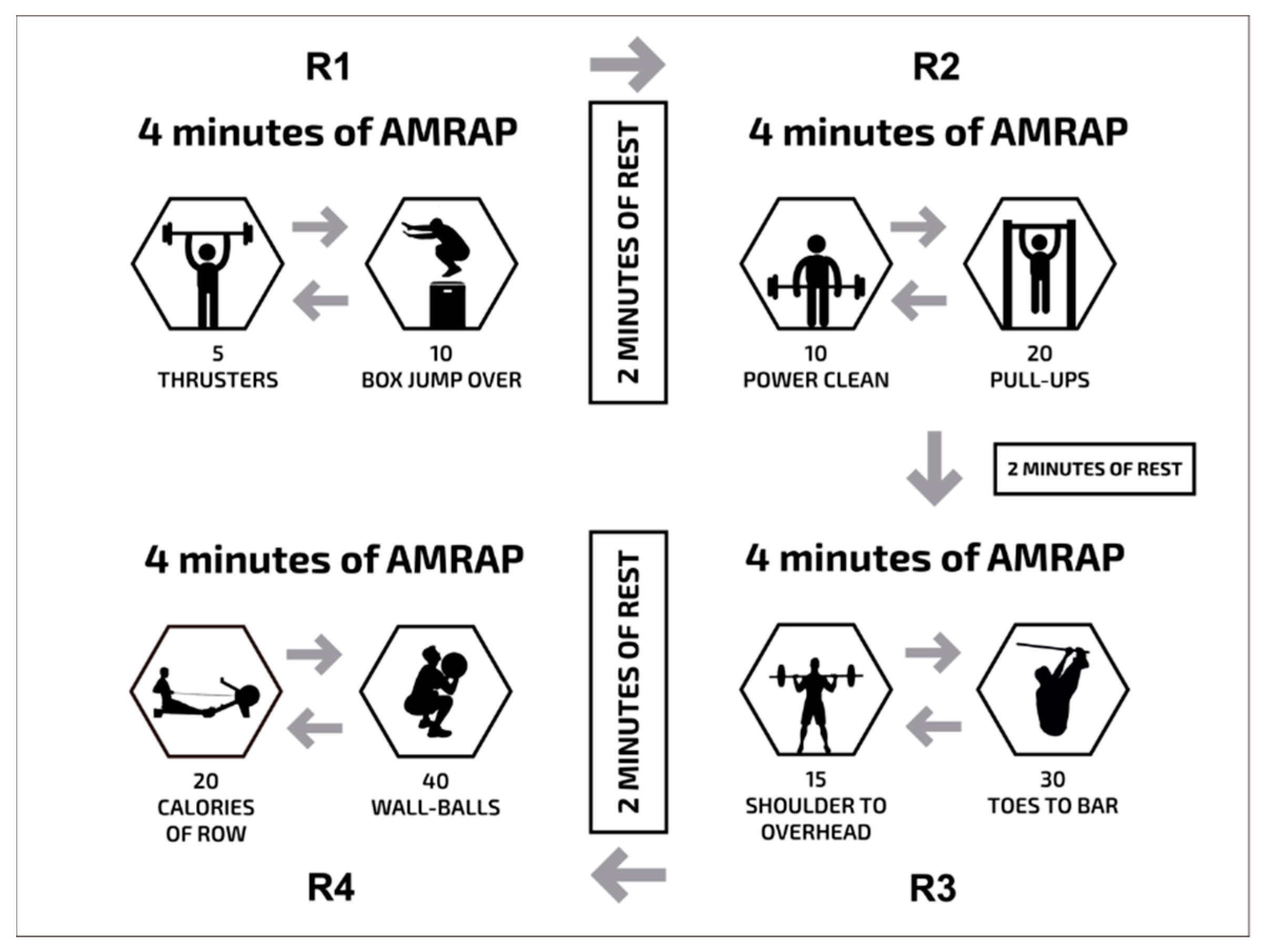
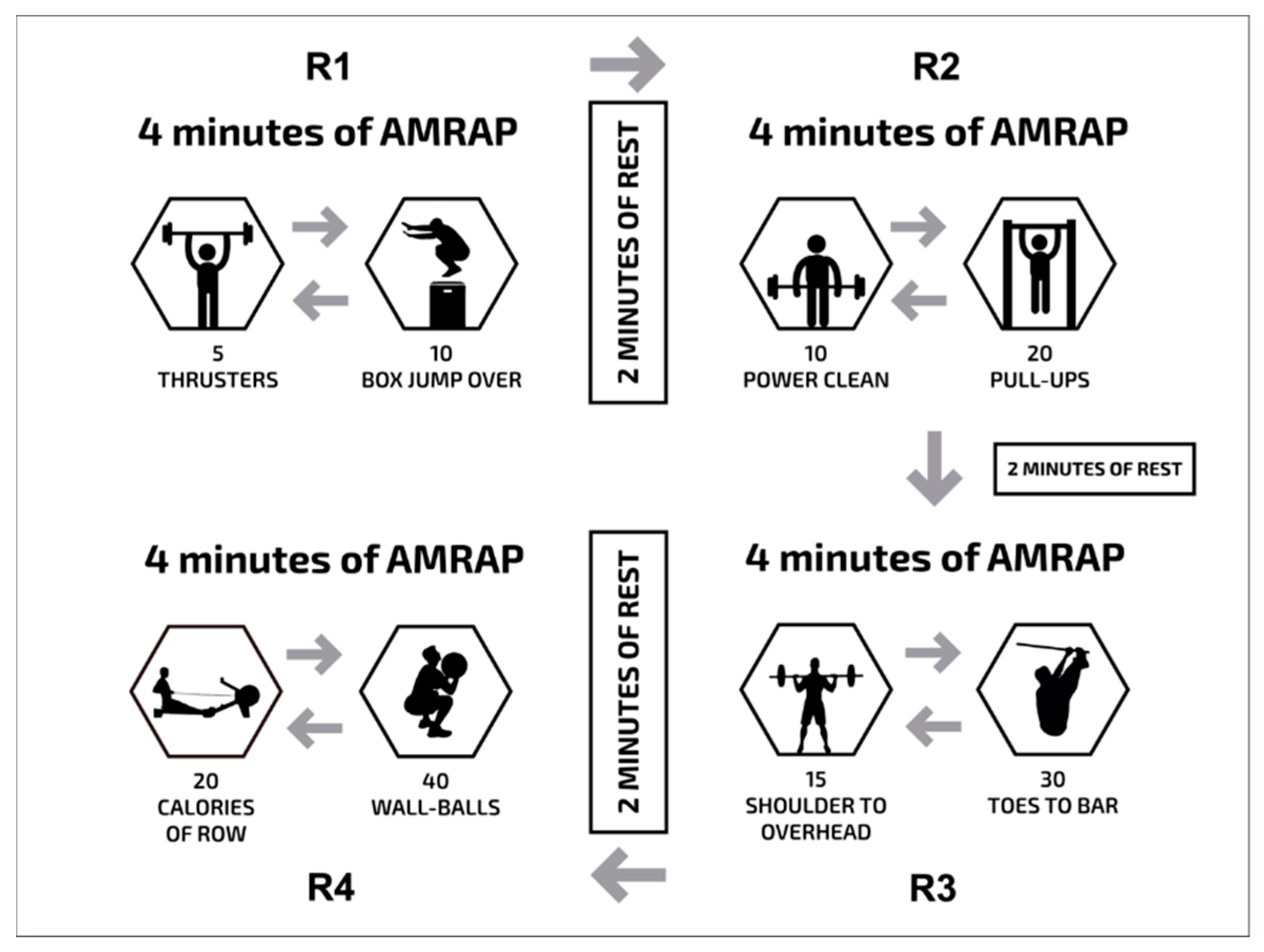
2.2. Experimental Design
2.3. Blood Lactate
2.4. Heart Rate (HR)
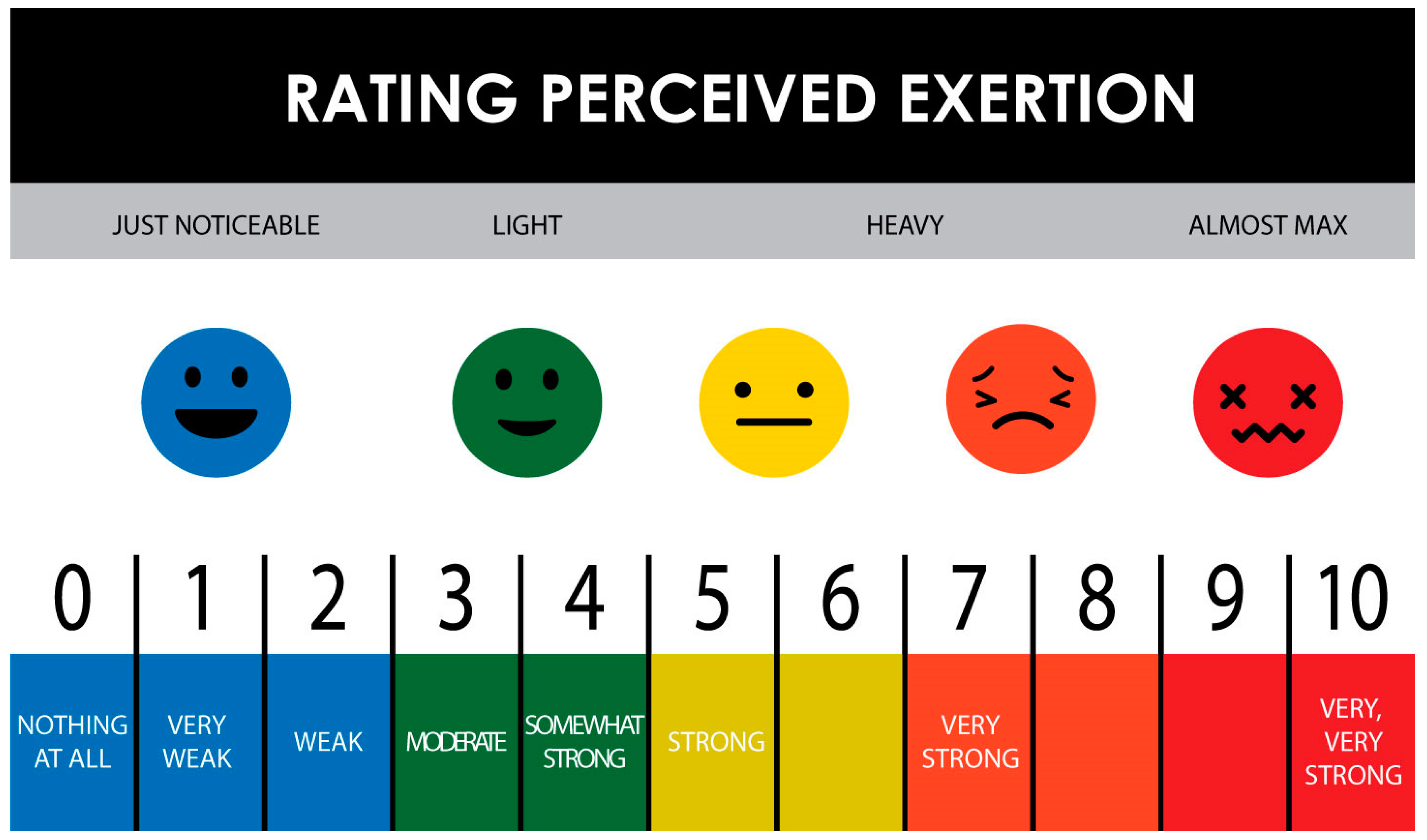
2.5. Rating of Perceived Exertion (RPE)
2.6. Statistical Analysis
3. Results
3.1. Number of Repetitions Performed
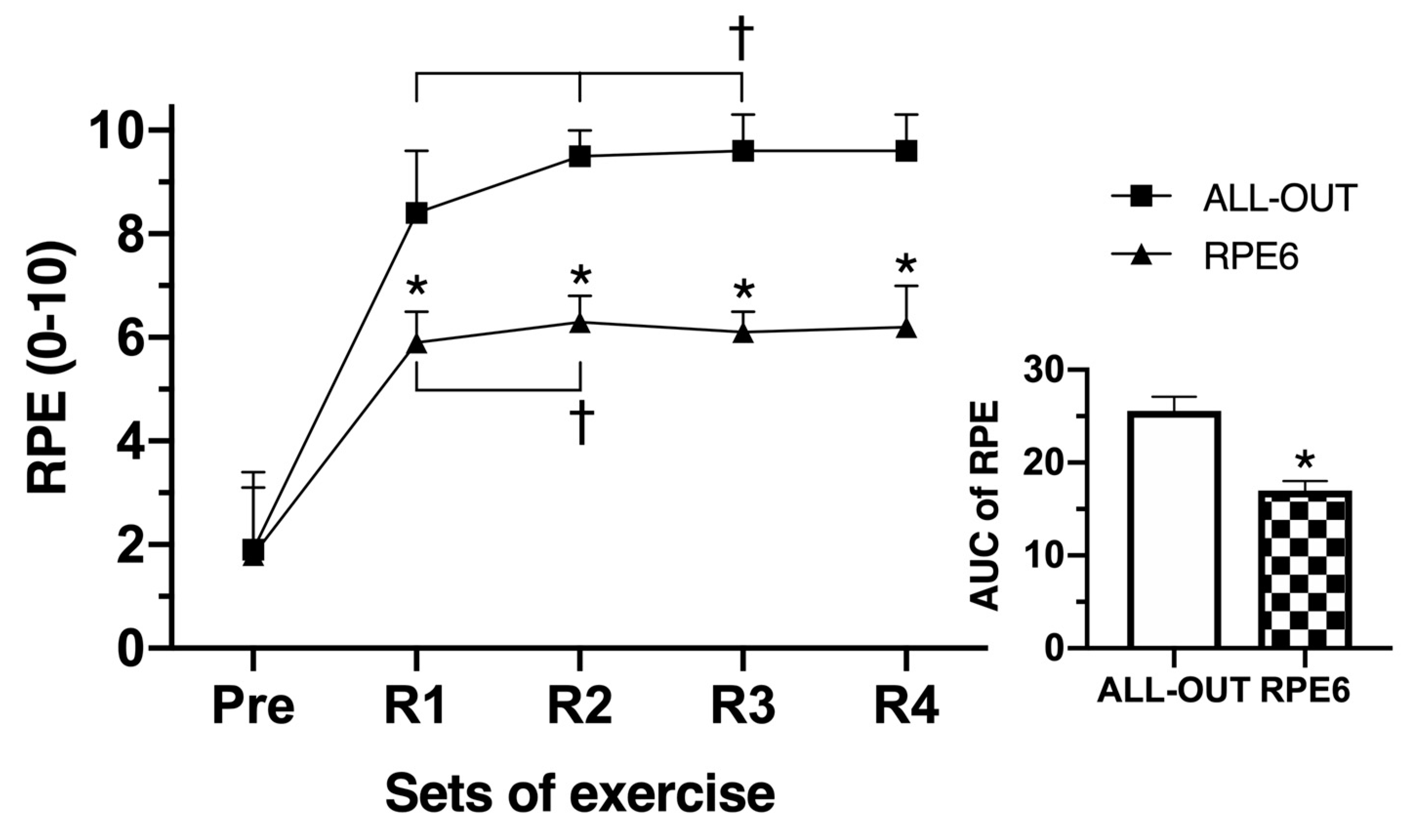
3.2. Rating of Perceived Exertion
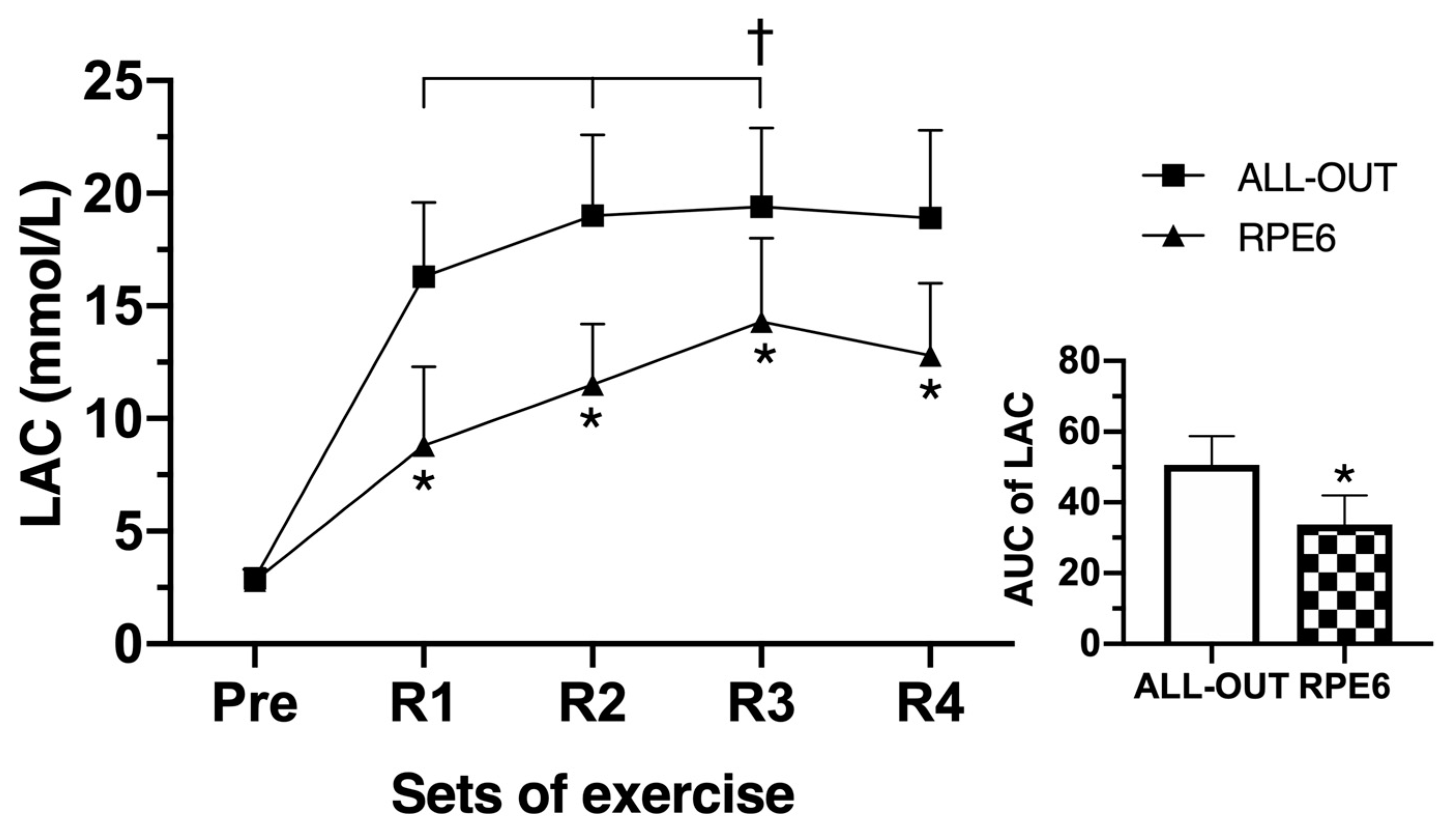
3.3. Blood Lactate Concentration
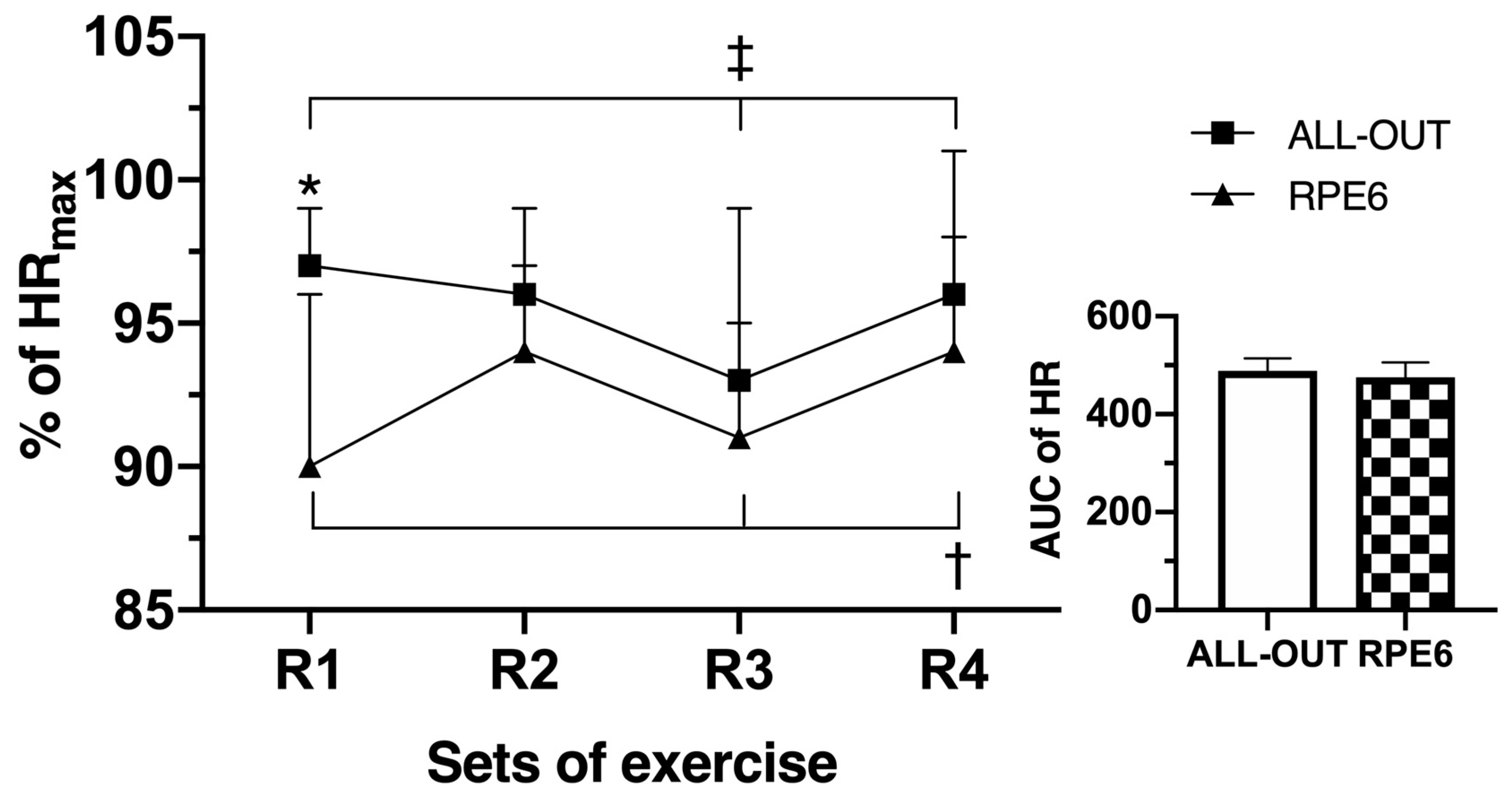
3.4. Heart Rate
3.5. Correlations between RPE and Physiological Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Tibana, R.A.; Sousa, N.M.F.d. Are extreme conditioning programmes effective and safe? A narrative review of high-intensity functional training methods research paradigms and findings. BMJ Open Sport Exerc. Med. 2018, 4, e000435. [Google Scholar] [CrossRef] [PubMed]
- Falk Neto, J.H.; Kennedy, M.D. The Multimodal Nature of High-Intensity Functional Training: Potential Applications to Improve Sport Performance. Sports 2019, 7, 33. [Google Scholar] [CrossRef] [PubMed]
- Crawford, D.A.; Drake, N.B.; Carper, M.J.; DeBlauw, J.; Heinrich, K.M. Are Changes in Physical Work Capacity Induced by High-Intensity Functional Training Related to Changes in Associated Physiologic Measures? Sports 2018, 6, 26. [Google Scholar] [CrossRef] [PubMed]
- Mate-Munoz, J.L.; Lougedo, J.H.; Barba, M.; Garcia-Fernandez, P.; Garnacho-Castano, M.V.; Dominguez, R. Muscular fatigue in response to different modalities of CrossFit sessions. PLoS ONE 2017, 12, e0181855. [Google Scholar] [CrossRef] [PubMed]
- Tibana, R.; Sousa, N.; Cunha, G.; Prestes, J.; Navalta, J.; Voltarelli, F. Exertional Rhabdomyolysis after an Extreme Conditioning Competition: A Case Report. Sports 2018, 6, 40. [Google Scholar] [CrossRef] [PubMed]
- Kliszczewicz, B.; Quindry, C.J.; Blessing, L.D.; Oliver, D.G.; Esco, R.M.; Taylor, J.K. Acute Exercise and Oxidative Stress: CrossFit(TM) vs. Treadmill Bout. J. Hum. Kinet. 2015, 47, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Tibana, R.A.; de Almeida, L.M.; Frade de Sousa, N.M.; Nascimento Dda, C.; Neto, I.V.; de Almeida, J.A.; de Souza, V.C.; Lopes Mde, F.; Nobrega Ode, T.; Vieira, D.C.; et al. Two Consecutive Days of Crossfit Training Affects Pro and Anti-inflammatory Cytokines and Osteoprotegerin without Impairments in Muscle Power. Front. Physiol. 2016, 7, 260. [Google Scholar] [CrossRef] [PubMed]
- Tibana, R.A.; Almeida, L.A.; Sousa Neto, I.V.; Sousa, N.M.F.; Almeida, J.A.; de Salles, B.F.; Bentes, C.M.; Voltarelli, F.A.; Collier, S.R.; Prestes, J. Extreme conditioning program induced acute hypotensive effects are independent of the exercise session intensity. Int. J. Exerc. Sci. 2017, 10, 1165–1173. [Google Scholar] [PubMed]
- Kliszczewicz, B.; Williamson, C.; Bechke, E.; McKenzie, M.; Hoffstetter, W. Autonomic response to a short and long bout of high-intensity functional training. J. Sports Sci. 2018, 36, 1872–1879. [Google Scholar] [CrossRef]
- Drake, N.B.; Smeed, J.; Carper, M.J.; Crawford, D. Effects of short-term CrossFit training: A magnitude-based approach. J. Exerc. Physiol. Online 2017, 20, 111–133. [Google Scholar]
- Drum, S.N.; Bellovary, B.N.; Jensen, R.L.; Moore, M.T.; Donath, L. Perceived demands and postexercise physical dysfunction in CrossFit (R) compared to an ACSM based training session. J. Sports Med. Phys. Fit. 2017, 57, 604–609. [Google Scholar]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Lagally, K.M.; McCaw, S.T.; Young, G.T.; Medema, H.C.; Thomas, D.Q. Ratings of perceived exertion and muscle activity during the bench press exercise in recreational and novice lifters. J. Strength Cond. Res. 2004, 18, 359–364. [Google Scholar] [PubMed]
- Ciolac, E.G.; Mantuani, S.S.; Neiva, C.M.; Verardi, C.; Pessoa-Filho, D.M.; Pimenta, L. Rating of perceived exertion as a tool for prescribing and self regulating interval training: A pilot study. Biol. Sport 2015, 32, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Ueda, T.; Kurokawa, T. Relationships between perceived exertion and physiological variables during swimming. Int. J. Sports Med. 1995, 16, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Klusiewicz, A.; Borkowski, L.; Sitkowski, D.; Burkhard-Jagodzinska, K.; Szczepanska, B.; Ladyga, M. Indirect Methods of Assessing Maximal Oxygen Uptake in Rowers: Practical Implications for Evaluating Physical Fitness in a Training Cycle. J. Hum. Kinet. 2016, 50, 187–194. [Google Scholar] [CrossRef]
- Tibana, R.A.; de Sousa, N.M.F.; Cunha, G.V.; Prestes, J.; Fett, C.; Gabbett, T.J.; Voltarelli, F.A. Validity of Session Rating Perceived Exertion Method for Quantifying Internal Training Load during High-Intensity Functional Training. Sports 2018, 6, 68. [Google Scholar] [CrossRef]
- Foster, C.; Florhaug, J.A.; Franklin, J.; Gottschall, L.; Hrovatin, L.A.; Parker, S.; Doleshal, P.; Dodge, C. A new approach to monitoring exercise training. J. Strength Cond. Res. 2001, 15, 109–115. [Google Scholar]
- Morishita, S.; Tsubaki, A.; Nashimoto, S.; Fu, J.B.; Onishi, H. Face scale rating of perceived exertion during cardiopulmonary exercise test. BMJ Open Sport Exerc. Med. 2018, 4, e000474. [Google Scholar] [CrossRef] [Green Version]
- Glass, G.V.; Hopkins, K.D. Statistical Methods in Education and Psychology, 3rd ed.; Allyn and Bacon: Boston, MA, USA, 1996; p. 674. [Google Scholar]
- Heinrich, K.M.; Patel, P.M.; O’Neal, J.L.; Heinrich, B.S. High-intensity compared to moderate-intensity training for exercise initiation, enjoyment, adherence, and intentions: An intervention study. BMC Public Health 2014, 14, 789. [Google Scholar] [CrossRef]
- Brisebois, M.F.; Rigby, B.R.; Nichols, D.L. Physiological and Fitness Adaptations after Eight Weeks of High-Intensity Functional Training in Physically Inactive Adults. Sports 2018, 6, 146. [Google Scholar] [CrossRef] [PubMed]
- Sobrero, G.; Arnett, S.; Schafer, M.; Stone, W.; Tolbert, T.A.; Salyer-Funk, A.; Crandall, J.; Farley, L.B.; Brown, J.; Lyons, S.; et al. A Comparison of High Intensity Functional Training and Circuit Training on Health and Performance Variables in Women: A Pilot Study. Women Sport Phys. Act. J. 2017, 25, 1–10. [Google Scholar] [CrossRef]
- Nieuwoudt, S.; Fealy, C.E.; Foucher, J.A.; Scelsi, A.R.; Malin, S.K.; Pagadala, M.; Rocco, M.; Burguera, B.; Kirwan, J.P. Functional high-intensity training improves pancreatic beta-cell function in adults with type 2 diabetes. Am. J. Physiol. Endocrinol. Metab. 2017, 313, E314–E320. [Google Scholar] [CrossRef] [PubMed]
- Ceci, R.; Hassmen, P. Self-monitored exercise at three different RPE intensities in treadmill vs field running. Med. Sci. Sports Exerc. 1991, 23, 732–738. [Google Scholar] [CrossRef] [PubMed]
- Fusco, A.; Knutson, C.; King, C.; Mikat, R.P.; Porcari, J.P.; Cortis, C.; Foster, C. Session RPE during Prolonged Exercise Training. Int. J. Sports Physiol. Perform. 2019, 7, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Edwards, A.M.; Polman, R.C. Pacing and awareness: Brain regulation of physical activity. Sports Med. 2013, 43, 1057–1064. [Google Scholar] [CrossRef] [PubMed]
- Gabbett, T.J. The training-injury prevention paradox: Should athletes be training smarter and harder? Br. J. Sports Med. 2016, 50, 273–280. [Google Scholar] [CrossRef]
- Gabbett, T.J. Debunking the myths about training load, injury and performance: Empirical evidence, hot topics and recommendations for practitioners. Br. J. Sports Med. 2018. [Google Scholar] [CrossRef]
- Seiler, S.; Haugen, O.; Kuffel, E. Autonomic recovery after exercise in trained athletes: Intensity and duration effects. Med. Sci. Sports Exerc. 2007, 39, 1366–1373. [Google Scholar] [CrossRef]
- Navalta, J.W.; Tibana, R.A.; Fedor, E.A.; Vieira, A.; Prestes, J. Three consecutive days of interval runs to exhaustion affects lymphocyte subset apoptosis and migration. Biomed. Res. Int. 2014, 2014, 694801. [Google Scholar] [CrossRef]
- Tibana, R.A.; Sousa, N.M.F.; Prestes, J.; Feito, Y.; Ferreira, C.E.; Voltarelli, F.A. Monitoring Training Load, Well-Being, Heart Rate Variability, and Competitive Performance of a Functional-Fitness Female Athlete: A Case Study. Sports 2019, 7, 35. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, B.S.; Li, D.; Svet, M.; Kesavabhotla, K.; Dahdaleh, N.S. CrossFit and rhabdomyolysis: A case series of 11 patients presenting at a single academic institution. J. Sci. Med. Sport 2019, 22, 758–762. [Google Scholar] [CrossRef] [PubMed]
- Beckham, S.G.; Earnest, C.P. Metabolic cost of free weight circuit weight training. J. Sports Med. Phys. Fit. 2000, 40, 118–125. [Google Scholar] [CrossRef]
- Fusi, F.; Carletti, L.; Sauer, D.; Simão Junior, R.F.; Perez, A. Acute cardiopulmonary responses to kettlebell exercise. Revista Brasileira de Ciências do Esporte 2017, 39, 408–416. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All-Out | RPE6 | Δ (%) | p-Value | ES | |
|---|---|---|---|---|---|
| Round 1 | 63.9 ± 4.4 | 46.6 ± 5.8 * | 27.1% | ≤0.0005 * | 3.36 |
| Round 2 | 58.0 ± 7.7 | 46.4 ± 7.0 * | 20% | 0.006 * | 1.58 |
| Round 3 | 41.9 ± 6.6 | 48.0 ± 1.9 * | −14.5% | 0.049 * | 1.26 |
| Round 4 | 50.6 ± 6.5 | 49.5 ± 4.0 | 2.2% | 0.663 | 0.20 |
| Total | 214.4 ± 18.6 | 190.5 ± 12.5 * | 11.1% | 0.020 * | 1.51 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alsamir Tibana, R.; Manuel Frade de Sousa, N.; Prestes, J.; da Cunha Nascimento, D.; Ernesto, C.; Falk Neto, J.H.; Kennedy, M.D.; Azevedo Voltarelli, F. Is Perceived Exertion a Useful Indicator of the Metabolic and Cardiovascular Responses to a Metabolic Conditioning Session of Functional Fitness? Sports 2019, 7, 161. https://doi.org/10.3390/sports7070161
Alsamir Tibana R, Manuel Frade de Sousa N, Prestes J, da Cunha Nascimento D, Ernesto C, Falk Neto JH, Kennedy MD, Azevedo Voltarelli F. Is Perceived Exertion a Useful Indicator of the Metabolic and Cardiovascular Responses to a Metabolic Conditioning Session of Functional Fitness? Sports. 2019; 7(7):161. https://doi.org/10.3390/sports7070161
Chicago/Turabian StyleAlsamir Tibana, Ramires, Nuno Manuel Frade de Sousa, Jonato Prestes, Dahan da Cunha Nascimento, Carlos Ernesto, Joao Henrique Falk Neto, Michael D. Kennedy, and Fabrício Azevedo Voltarelli. 2019. "Is Perceived Exertion a Useful Indicator of the Metabolic and Cardiovascular Responses to a Metabolic Conditioning Session of Functional Fitness?" Sports 7, no. 7: 161. https://doi.org/10.3390/sports7070161
APA StyleAlsamir Tibana, R., Manuel Frade de Sousa, N., Prestes, J., da Cunha Nascimento, D., Ernesto, C., Falk Neto, J. H., Kennedy, M. D., & Azevedo Voltarelli, F. (2019). Is Perceived Exertion a Useful Indicator of the Metabolic and Cardiovascular Responses to a Metabolic Conditioning Session of Functional Fitness? Sports, 7(7), 161. https://doi.org/10.3390/sports7070161