
Sodium-Glucose Cotransporter-2 Inhibitors—Miracle Drugs for the Treatment of Chronic Kidney Disease Irrespective of the Diabetes Status: Lessons from the Dedicated Kidney Disease-Focused CREDENCE and DAPA-CKD Trials


Abstract
1. Introduction
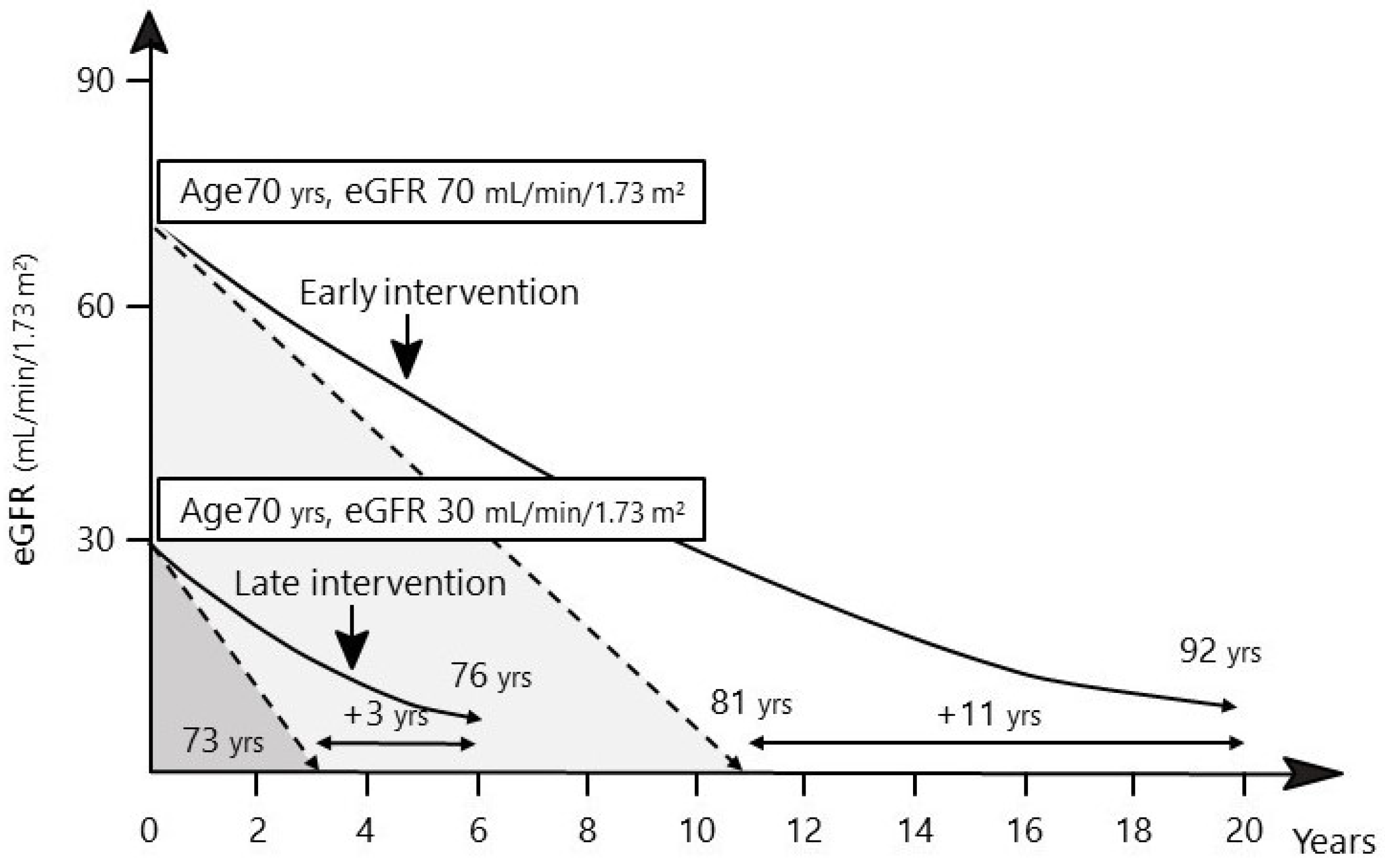
2. Importance of Early Diagnosis and Therapeutic Intervention in Patients with DKD
3. Prognostic Biomarkers of eGFR Decline: Circulating Tumor Necrosis Factor (TNF) Receptors (TNFRs)
4. Effects of the SGLT2 Inhibitors on Kidney Outcomes in Patients with Nondiabetic CKD or Diabetes
5. Renoprotective Effects of the SGLT2 Inhibitors beyond Reductions in Albuminuria
6. Initial eGFR Declines and Volume Depletion: Concerning Side-Effects of the SGLT2 Inhibitors
7. Hyperkalemia
8. Effects of the SGLT2 Inhibitors in Patients with CKD and Normoalbuinuria
9. Effects of the SGLT2 Inhibitors on Atherosclerotic CVD (ASCVD) and HF in Patients with CKD
10. Promising Therapeutic Strategy
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gohda, T.; Murakoshi, M.; Koshida, T.; Ichikawa, S.; Li, Z.I.; Adachi, E.R.I.; Sakuma, H.; Hagiwara, S.; Funabiki, K.; Suzuki, Y. Concept of diabetic kidney disease-paradigm shift from albuminuria-based to GFR-based kidney disease. Juntendo Med. J. 2019, 65, 510–516. [Google Scholar] [CrossRef]
- Nitta, K.; Goto, S.; Masakane, I.; Hanafusa, N.; Taniguchi, M.; Hasegawa, T.; Nakai, S.; Wada, A.; Hamano, T.; Hoshino, J.; et al. Annual dialysis data report for 2018, JSDT Renal Data Registry: Survey methods, facility data, incidence, prevalence, and mortality. Ren. Replace Ther. 2020, 6, 41. [Google Scholar] [CrossRef]
- Chapter 11: International Comparison, the 2018 USRDS Annual Data Report. Washington: United States Renal Data System, 2018. Available online: https://www.usrds.org (accessed on 8 September 2022).
- Afkarian, M.; Sachs, M.C.; Kestenbaum, B.; Hirsch, I.B.; Tuttle, K.R.; Himmelfarb, J.; de Boer, I.H. Kidney disease and increased mortality risk in type 2 diabetes. J. Am. Soc. Nephrol. 2013, 24, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Gohda, T.; Tomino, Y. Novel biomarkers for the progression of diabetic nephropathy: Soluble TNF receptors. Curr. Diab. Rep. 2013, 13, 560–566. [Google Scholar] [CrossRef]
- Nathan, D.M.; Genuth, S.; Lachin, J.; Cleary, P.; Crofford, O.; Davis, M.; Rand, L.; Siebert, C. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N. Engl. J. Med. 1993, 329, 977–986. [Google Scholar]
- UKPDS33. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998, 352, 837–853. [Google Scholar] [CrossRef]
- Gerstein, H.C.; Miller, M.E.; Byington, R.P.; Goff, D.C., Jr.; Bigger, J.T.; Buse, J.B.; Cushman, W.C.; Genuth, S.; Ismail-Beigi, F.; Grimm, R.H., Jr.; et al. Effects of intensive glucose lowering in type 2 diabetes. N. Engl. J. Med. 2008, 358, 2545–2559. [Google Scholar]
- Walker, S.R.; Komenda, P.; Khojah, S.; Al-Tuwaijri, W.; MacDonald, K.; Hiebert, B.; Tangri, N.; Nadurak, S.W.D.; Ferguson, T.W.; Rigatto, C.; et al. Dipeptidyl peptidase-4 inhibitors in chronic kidney disease: A systematic review of randomized clinical trials. Nephron 2017, 136, 85–94. [Google Scholar] [CrossRef]
- Gaede, P.; Vedel, P.; Parving, H.H.; Pedersen, O. Intensified multifactorial intervention in patients with type 2 diabetes mellitus and microalbuminuria: The Steno type 2 randomised study. Lancet 1999, 353, 617–622. [Google Scholar] [CrossRef]
- Epstein, M.; Reaven, N.L.; Funk, S.E.; McGaughey, K.J.; Oestreicher, N.; Knispel, J. Evaluation of the treatment gap between clinical guidelines and the utilization of renin-angiotensin-aldosterone system inhibitors. Am. J. Manag. Care 2015, 21 (Suppl. S11), S212–S2220. [Google Scholar]
- Brenner, B.M.; Cooper, M.E.; de Zeeuw, D.; Keane, W.F.; Mitch, W.E.; Parving, H.H.; Remuzzi, G.; Snapinn, S.M.; Zhang, Z.; Shahinfar, S. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N. Engl. J. Med. 2001, 345, 861–869. [Google Scholar] [CrossRef] [PubMed]
- Lewis, E.J.; Hunsicker, L.G.; Clarke, W.R.; Berl, T.; Pohl, M.A.; Lewis, J.B.; Ritz, E.; Atkins, R.C.; Rohde, R.; Raz, I. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N. Engl. J. Med. 2001, 345, 851–860. [Google Scholar] [CrossRef] [PubMed]
- Mauer, M.; Zinman, B.; Gardiner, R.; Suissa, S.; Sinaiko, A.; Strand, T.; Drummond, K.; Donnelly, S.; Goodyer, P.; Gubler, M.C.; et al. Renal and retinal effects of enalapril and losartan in type 1 diabetes. N. Engl. J. Med. 2009, 361, 40–51. [Google Scholar] [CrossRef] [PubMed]
- Perkovic, V.; Jardine, M.J.; Neal, B.; Bompoint, S.; Heerspink, H.J.L.; Charytan, D.M.; Edwards, R.; Agarwal, R.; Bakris, G.; Bull, S.; et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N. Engl. J. Med. 2019, 380, 2295–2306. [Google Scholar] [CrossRef] [PubMed]
- Heerspink, H.J.L.; Stefansson, B.V.; Correa-Rotter, R.; Chertow, G.M.; Greene, T.; Hou, F.F.; Mann, J.F.E.; McMurray, J.J.V.; Lindberg, M.; Rossing, P.; et al. Dapagliflozin in patients with chronic kidney disease. N. Engl. J. Med. 2020, 383, 1436–1446. [Google Scholar] [CrossRef] [PubMed]
- Bakris, G.L.; Agarwal, R.; Anker, S.D.; Pitt, B.; Ruilope, L.M.; Rossing, P.; Kolkhof, P.; Nowack, C.; Schloemer, P.; Joseph, A.; et al. Effect of finerenone on chronic kidney disease outcomes in type 2 diabetes. N. Engl. J. Med. 2020, 383, 2219–2229. [Google Scholar] [CrossRef]
- Tuttle, K.R.; Lakshmanan, M.C.; Rayner, B.; Busch, R.S.; Zimmermann, A.G.; Woodward, D.B.; Botros, F.T. Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7): A multicentre, open-label, randomised trial. Lancet Diabetes Endocrinol. 2018, 6, 605–617. [Google Scholar] [CrossRef]
- Skupien, J.; Warram, J.H.; Smiles, A.; Galecki, A.; Stanton, R.C.; Krolewski, A.S. Improved glycemic control and risk of ESRD in patients with type 1 diabetes and proteinuria. J. Am. Soc. Nephrol. 2014, 25, 2916–2925. [Google Scholar] [CrossRef]
- Niewczas, M.A.; Gohda, T.; Skupien, J.; Smiles, A.M.; Walker, W.H.; Rosetti, F.; Cullere, X.; Eckfeldt, J.H.; Doria, A.; Mayadas, T.N.; et al. Circulating TNF receptors 1 and 2 predict ESRD in type 2 diabetes. J. Am. Soc. Nephrol. 2012, 23, 507–515. [Google Scholar] [CrossRef]
- Gohda, T.; Niewczas, M.A.; Ficociello, L.H.; Walker, W.H.; Skupien, J.; Rosetti, F.; Cullere, X.; Johnson, A.C.; Crabtree, G.; Smiles, A.M.; et al. Circulating TNF receptors 1 and 2 predict stage 3 CKD in type 1 diabetes. J. Am. Soc. Nephrol. 2012, 23, 516–524. [Google Scholar] [CrossRef]
- Niewczas, M.A.; Pavkov, M.E.; Skupien, J.; Smiles, A.; Md Dom, Z.I.; Wilson, J.M.; Park, J.; Nair, V.; Schlafly, A.; Saulnier, P.J.; et al. A signature of circulating inflammatory proteins and development of end-stage renal disease in diabetes. Nat. Med. 2019, 25, 805–813. [Google Scholar] [CrossRef] [PubMed]
- Gohda, T.; Yanagisawa, N.; Murakoshi, M.; Ueda, S.; Nishizaki, Y.; Nojiri, S.; Ohashi, Y.; Ohno, I.; Shibagaki, Y.; Imai, N.; et al. Association between kidney function decline and baseline TNFR levels or change ratio in TNFR by febuxostat chiefly in non-diabetic CKD patients with asymptomatic hyperuricemia. Front. Med. 2021, 8, 634932. [Google Scholar] [CrossRef] [PubMed]
- Murakoshi, M.; Gohda, T.; Sakuma, H.; Shibata, T.; Adachi, E.; Kishida, C.; Ichikawa, S.; Koshida, T.; Kamei, N.; Suzuki, Y. Progranulin and its receptor predict kidney function decline in patients with type 2 diabetes. Front. Endocrinol. 2022, 13, 849457. [Google Scholar] [CrossRef]
- Waijer, S.W.; Sen, T.; Arnott, C.; Neal, B.; Kosterink, J.G.W.; Mahaffey, K.W.; Parikh, C.R.; de Zeeuw, D.; Perkovic, V.; Neuen, B.L.; et al. Association between TNF receptors and KIM-1 with kidney outcomes in early-stage diabetic kidney disease. Clin. J. Am. Soc. Nephrol. 2022, 17, 251–259. [Google Scholar] [CrossRef]
- Gohda, T.; Maruyama, S.; Kamei, N.; Yamaguchi, S.; Shibata, T.; Murakoshi, M.; Horikoshi, S.; Tomino, Y.; Ohsawa, I.; Gotoh, H.; et al. Circulating TNF receptors 1 and 2 predict mortality in patients with end-stage renal disease undergoing dialysis. Sci. Rep. 2017, 7, 43520. [Google Scholar] [CrossRef] [PubMed]
- Sen, T.; Li, J.; Neuen, B.L.; Neal, B.; Arnott, C.; Parikh, C.R.; Coca, S.G.; Perkovic, V.; Mahaffey, K.W.; Yavin, Y.; et al. Effects of the SGLT2 inhibitor canagliflozin on plasma biomarkers TNFR-1, TNFR-2 and KIM-1 in the CANVAS trial. Diabetologia 2021, 64, 2147–2158. [Google Scholar] [CrossRef]
- Chen, T.K.; Coca, S.G.; Estrella, M.M.; Appel, L.J.; Coresh, J.; Thiessen Philbrook, H.; Obeid, W.; Fried, L.F.; Heerspink, H.J.L.; Ix, J.H.; et al. Longitudinal TNFR1 and TNFR2 and kidney outcomes: Results from AASK and VA NEPHRON-D. J. Am. Soc. Nephrol. 2022, 33, 996–1010. [Google Scholar] [CrossRef] [PubMed]
- Persson, F.; Rossing, P.; Vart, P.; Chertow, G.M.; Hou, F.F.; Jongs, N.; McMurray, J.J.V.; Correa-Rotter, R.; Bajaj, H.S.; Stefansson, B.V.; et al. Efficacy and safety of dapagliflozin by baseline glycemic status: A prespecified analysis from the DAPA-CKD trial. Diabetes Care 2021, 44, 1894–1897. [Google Scholar] [CrossRef]
- Li, J.; Neal, B.; Perkovic, V.; de Zeeuw, D.; Neuen, B.L.; Arnott, C.; Simpson, R.; Oh, R.; Mahaffey, K.W.; Heerspink, H.J.L. Mediators of the effects of canagliflozin on kidney protection in patients with type 2 diabetes. Kidney Int. 2020, 98, 769–777. [Google Scholar] [CrossRef]
- Cannon, C.P.; Perkovic, V.; Agarwal, R.; Baldassarre, J.; Bakris, G.; Charytan, D.M.; de Zeeuw, D.; Edwards, R.; Greene, T.; Heerspink, H.J.L.; et al. Evaluating the effects of canagliflozin on cardiovascular and renal events in patients with type 2 diabetes mellitus and chronic kidney disease according to baseline HbA1c, including those with HbA1c <7%: Results from the CREDENCE trial. Circulation 2020, 141, 407–410. [Google Scholar] [CrossRef]
- Furtado, R.H.M.; Raz, I.; Goodrich, E.L.; Murphy, S.A.; Bhatt, D.L.; Leiter, L.A.; McGuire, D.K.; Wilding, J.P.H.; Aylward, P.; Dalby, A.J.; et al. Efficacy and safety of dapagliflozin in type 2 diabetes according to baseline blood pressure: Observations from DECLARE-TIMI 58 trial. Circulation 2022, 145, 1581–1591. [Google Scholar] [CrossRef] [PubMed]
- Heerspink, H.; Jong, N.; Stefansson, B.; Chertow, G.; Langkilde, A.; Mcmurray, J.; Correa-Rotter, R.; Rossing, P.; Toto, R.; Wheeler, D. Effeects of dapagliflozin in patients with chronic kidney disease according to background angiotensin-converting enzyme inhibitor and angiotensin receptor blocker dose. Nephrol. Dial. Transpl. 2022, 37, i847–i850. [Google Scholar]
- Jongs, N.; Greene, T.; Chertow, G.M.; McMurray, J.J.V.; Langkilde, A.M.; Correa-Rotter, R.; Rossing, P.; Sjostrom, C.D.; Stefansson, B.V.; Toto, R.D.; et al. Effect of dapagliflozin on urinary albumin excretion in patients with chronic kidney disease with and without type 2 diabetes: A prespecified analysis from the DAPA-CKD trial. Lancet Diabetes Endocrinol. 2021, 9, 755–766. [Google Scholar] [CrossRef]
- Jardine, M.J.; Zhou, Z.; Mahaffey, K.W.; Oshima, M.; Agarwal, R.; Bakris, G.; Bajaj, H.S.; Bull, S.; Cannon, C.P.; Charytan, D.M.; et al. Renal, cardiovascular, and safety outcomes of canagliflozin by baseline kidney function: A secondary analysis of the CREDENCE randomized trial. J. Am. Soc. Nephrol. 2020, 31, 1128–1139. [Google Scholar] [CrossRef] [PubMed]
- Cherney, D.Z.I.; Zinman, B.; Inzucchi, S.E.; Koitka-Weber, A.; Mattheus, M.; von Eynatten, M.; Wanner, C. Effects of empagliflozin on the urinary albumin-to-creatinine ratio in patients with type 2 diabetes and established cardiovascular disease: An exploratory analysis from the EMPA-REG OUTCOME randomised, placebo-controlled trial. Lancet Diabetes Endocrinol. 2017, 5, 610–621. [Google Scholar] [CrossRef]
- Neuen, B.L.; Ohkuma, T.; Neal, B.; Matthews, D.R.; de Zeeuw, D.; Mahaffey, K.W.; Fulcher, G.; Li, Q.; Jardine, M.; Oh, R.; et al. Effect of canagliflozin on renal and cardiovascular outcomes across different levels of albuminuria: Data from the CANVAS program. J. Am. Soc. Nephrol. 2019, 30, 2229–2242. [Google Scholar] [CrossRef] [PubMed]
- Mosenzon, O.; Wiviott, S.D.; Heerspink, H.J.L.; Dwyer, J.P.; Cahn, A.; Goodrich, E.L.; Rozenberg, A.; Schechter, M.; Yanuv, I.; Murphy, S.A.; et al. The effect of dapagliflozin on albuminuria in DECLARE-TIMI 58. Diabetes Care 2021, 44, 1805–1815. [Google Scholar] [CrossRef]
- Heerspink, H.J.L.; Sjostrom, C.D.; Inzucchi, S.E.; Hallow, M.K.; Cain, V.A.; Rossing, P.; Stefansson, B.V.; Sartipy, P. Reduction in albuminuria with dapagliflozin cannot be predicted by baseline clinical characteristics or changes in most other risk markers. Diabetes Obes. Metab. 2019, 21, 720–725. [Google Scholar] [CrossRef]
- Oshima, M.; Neuen, B.L.; Li, J.; Perkovic, V.; Charytan, D.M.; de Zeeuw, D.; Edwards, R.; Greene, T.; Levin, A.; Mahaffey, K.W.; et al. Early change in albuminuria with canagliflozin predicts kidney and cardiovascular outcomes: A post hoc analysis from the CREDENCE trial. J. Am. Soc. Nephrol. 2020, 31, 2925–2936. [Google Scholar] [CrossRef]
- Oshima, M.; Jardine, M.J.; Agarwal, R.; Bakris, G.; Cannon, C.P.; Charytan, D.M.; de Zeeuw, D.; Edwards, R.; Greene, T.; Levin, A.; et al. Insights from CREDENCE trial indicate an acute drop in estimated glomerular filtration rate during treatment with canagliflozin with implications for clinical practice. Kidney Int. 2021, 99, 999–1009. [Google Scholar] [CrossRef]
- Jongs, N.; Chertow, G.; Greene, T.; McMurray, J.; Langkilde, A.M.; Correa-Rotter, R.; Kashihara, N.; Rossing, P.; Sjostrom, C.D.; Stefansson, B.; et al. Correlates and consequences of an acute change in eGFR in response to the SGLT2 inhibitor dapagliflozin in patients with chronic kidney disease. J. Am. Soc. Nephrol. 2022, 33, 2094–2107. [Google Scholar] [PubMed]
- Kraus, B.J.; Weir, M.R.; Bakris, G.L.; Mattheus, M.; Cherney, D.Z.I.; Sattar, N.; Heerspink, H.J.L.; Ritter, I.; von Eynatten, M.; Zinman, B.; et al. Characterization and implications of the initial estimated glomerular filtration rate ‘dip’ upon sodium-glucose cotransporter-2 inhibition with empagliflozin in the EMPA-REG OUTCOME trial. Kidney Int. 2021, 99, 750–762. [Google Scholar] [CrossRef] [PubMed]
- Adamson, C.; Docherty, K.F.; Heerspink, H.J.L.; de Boer, R.A.; Damman, K.; Inzucchi, S.E.; Kober, L.; Kosiborod, M.N.; Martinez, F.A.; Petrie, M.C.; et al. Initial decline (dip) in estimated glomerular filtration rate after initiation of dapagliflozin in patients with heart failure and reduced ejection fraction: Insights from DAPA-HF. Circulation 2022, 146, 438–449. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Bowe, B.; Gibson, A.K.; McGill, J.B.; Maddukuri, G.; Al-Aly, Z. Clinical implications of estimated glomerular filtration rate dip following sodium-glucose cotransporter-2 inhibitor initiation on cardiovascular and kidney outcomes. J. Am. Heart Assoc. 2021, 10, e020237. [Google Scholar] [CrossRef]
- Heerspink, H.J.L.; Oshima, M.; Zhang, H.; Li, J.; Agarwal, R.; Capuano, G.; Charytan, D.M.; Craig, J.; de Zeeuw, D.; Di Tanna, G.L.; et al. Canagliflozin and kidney-related adverse events in type 2 diabetes and CKD: Findings from the randomized CREDENCE trial. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2022, 79, 244–256.e1. [Google Scholar] [CrossRef]
- Heerspink, H.J.L.; Cherney, D.; Postmus, D.; Stefansson, B.V.; Chertow, G.M.; Dwyer, J.P.; Greene, T.; Kosiborod, M.; Langkilde, A.M.; McMurray, J.J.V.; et al. A pre-specified analysis of the dapagliflozin and prevention of adverse outcomes in chronic kidney disease (DAPA-CKD) randomized controlled trial on the incidence of abrupt declines in kidney function. Kidney Int. 2022, 101, 174–184. [Google Scholar] [CrossRef]
- Gilbert, R.E.; Thorpe, K.E. Acute kidney injury with sodium-glucose co-transporter-2 inhibitors: A meta-analysis of cardiovascular outcome trials. Diabetes Obes. Metab. 2019, 21, 1996–2000. [Google Scholar] [CrossRef]
- Hougen, I.; Leon, S.J.; Whitlock, R.; Rigatto, C.; Komenda, P.; Bohm, C.; Tangri, N. Hyperkalemia and its association with mortality, cardiovascular events, hospitalizations, and intensive care unit admissions in a population-based retrospective cohort. Kidney Int. Rep. 2021, 6, 1309–1316. [Google Scholar] [CrossRef]
- Miao, Y.; Dobre, D.; Heerspink, H.J.; Brenner, B.M.; Cooper, M.E.; Parving, H.H.; Shahinfar, S.; Grobbee, D.; de Zeeuw, D. Increased serum potassium affects renal outcomes: A post hoc analysis of the Reduction of Endpoints in NIDDM with the Angiotensin II Antagonist Losartan (RENAAL) trial. Diabetologia 2011, 54, 44–50. [Google Scholar] [CrossRef]
- Neuen, B.L.; Oshima, M.; Agarwal, R.; Arnott, C.; Cherney, D.Z.; Edwards, R.; Langkilde, A.M.; Mahaffey, K.W.; McGuire, D.K.; Neal, B.; et al. Sodium-glucose cotransporter 2 inhibitors and risk of hyperkalemia in people with type 2 diabetes: A meta-analysis of individual participant data from randomized, controlled trials. Circulation 2022, 145, 1460–1470. [Google Scholar] [CrossRef]
- Provenzano, M.; Puchades, M.J.; Garofalo, C.; Jongs, N.; D’Marco, L.; Andreucci, M.; De Nicola, L.; Gorriz, J.L.; Heerspink, H.J.L. Albuminuria-lowering effect of dapagliflozin, eplerenone, and their combination in patients with chronic kidney disease: A randomized crossover clinical trial. J. Am. Soc. Nephrol. 2022, 33, 1569–1580. [Google Scholar] [CrossRef] [PubMed]
- Rossing, P.; Filippatos, G.; Agarwal, R.; Anker, S.D.; Pitt, B.; Ruilope, L.M.; Chan, J.C.N.; Kooy, A.; McCafferty, K.; Schernthaner, G.; et al. Finerenone in predominantly advanced CKD and type 2 diabetes with or without sodium-glucose cotransporter-2 inhibitor therapy. Kidney Int. Rep. 2022, 7, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Rossing, P.; Agarwal, R.; Anker, S.D.; Filippatos, G.; Pitt, B.; Ruilope, L.M.; Amod, A.; Marre, M.; Joseph, A.; Lage, A.; et al. Efficacy and safety of finerenone in patients with chronic kidney disease and type 2 diabetes by GLP-1RA treatment: A subgroup analysis from the FIDELIO-DKD trial. Diabetes Obes. Metab. 2022, 24, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Green, J.B.; Mottl, A.K.; Bakris, G.; Heerspink, H.J.L.; Mann, J.F.E.; McGill, J.B.; Nangaku, M.; Rossing, P.; Scott, C.; Gay, A.; et al. Design of the combination effect of fInerenone and empagliflozin in participants with chronic kidney disease and type 2 diabetes using an UACR Endpoint study (CONFIDENCE). Nephrol. Dial. Transpl. 2022. [CrossRef] [PubMed]
- Neuen, B.L.; Young, T.; Heerspink, H.J.L.; Neal, B.; Perkovic, V.; Billot, L.; Mahaffey, K.W.; Charytan, D.M.; Wheeler, D.C.; Arnott, C.; et al. SGLT2 inhibitors for the prevention of kidney failure in patients with type 2 diabetes: A systematic review and meta-analysis. Lancet Diabetes Endocrinol. 2019, 7, 845–854. [Google Scholar] [CrossRef]
- Li, Z.; Murakoshi, M.; Ichikawa, S.; Koshida, T.; Adachi, E.; Suzuki, C.; Ueda, S.; Gohda, T.; Suzuki, Y. The sodium-glucose cotransporter 2 inhibitor tofogliflozin prevents diabetic kidney disease progression in type 2 diabetic mice. FEBS Open Bio. 2020, 10, 2761–2770. [Google Scholar] [CrossRef]
- Nespoux, J.; Vallon, V. Renal effects of SGLT2 inhibitors: An update. Curr. Opin. Nephrol. Hypertens 2020, 29, 190–198. [Google Scholar] [CrossRef]
- Zelniker, T.A.; Wiviott, S.D.; Raz, I.; Im, K.; Goodrich, E.L.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; Furtado, R.H.M.; et al. SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes: A systematic review and meta-analysis of cardiovascular outcome trials. Lancet 2019, 393, 31–39. [Google Scholar] [CrossRef]
- Mahaffey, K.W.; Jardine, M.J.; Bompoint, S.; Cannon, C.P.; Neal, B.; Heerspink, H.J.L.; Charytan, D.M.; Edwards, R.; Agarwal, R.; Bakris, G.; et al. Canagliflozin and cardiovascular and renal outcomes in type 2 diabetes mellitus and chronic kidney disease in primary and secondary cardiovascular prevention groups. Circulation 2019, 140, 739–750. [Google Scholar] [CrossRef]
- Kluger, A.Y.; Tecson, K.M.; Lee, A.Y.; Lerma, E.V.; Rangaswami, J.; Lepor, N.E.; Cobble, M.E.; McCullough, P.A. Class effects of SGLT2 inhibitors on cardiorenal outcomes. Cardiovasc. Diabetol. 2019, 18, 99. [Google Scholar] [CrossRef]
- Barai, S.; Gambhir, S.; Prasad, N.; Sharma, R.K.; Ora, M. Functional renal reserve capacity in different stages of chronic kidney disease. Nephrology 2010, 15, 350–353. [Google Scholar] [CrossRef] [PubMed]
- McMurray, J.J.V.; Wheeler, D.C.; Stefansson, B.V.; Jongs, N.; Postmus, D.; Correa-Rotter, R.; Chertow, G.M.; Greene, T.; Held, C.; Hou, F.F.; et al. Effect of dapagliflozin on clinical outcomes in patients with chronic kidney disease, with and without cardiovascular disease. Circulation 2021, 143, 438–448. [Google Scholar] [CrossRef] [PubMed]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. Cardiovascular and renal outcomes with empagliflozin in heart failure. N. Engl. J. Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef]
- Anker, S.D.; Butler, J.; Filippatos, G.; Ferreira, J.P.; Bocchi, E.; Bohm, M.; Brunner-La Rocca, H.P.; Choi, D.J.; Chopra, V.; Chuquiure-Valenzuela, E.; et al. Empagliflozin in heart failure with a preserved ejection fraction. N. Engl. J. Med. 2021, 385, 1451–1461. [Google Scholar] [CrossRef]
- Packer, M.; Zannad, F.; Butler, J.; Filippatos, G.; Ferreira, J.P.; Pocock, S.J.; Brueckmann, M.; Zeller, C.; Hauske, S.; Anker, S.D.; et al. Influence of endpoint definitions on the effect of empagliflozin on major renal outcomes in the EMPEROR-Preserved trial. Eur. J. Heart Fail. 2021, 23, 1798–1799. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| CREDENCE [15] (Canagliflozin) | DAPA-CKD [16] (Dapagliflozin) | DAPA-CKD (with T2D) | DAPA-CKD (without T2D) | |
|---|---|---|---|---|
| n | 4401 | 4304 | 2906 | 1398 |
| Age (year) | 63 | 62 | 64 | 56 |
| Male sex (%) | 66 | 67 | 67 | 67 |
| Body mass index | 31.3 | 29.5 | 30.3 | 27.9 |
| T2D (%) | 100 | 68 | 100 | 0 |
| HbA1c (%) | 8.3 | 7.1 | 7.8 | 5.6 |
| LSM change in HbA1c: % (95% CI) | −0.3 (−0.2 to −0.3) | −0.1 (−0.1 to 0.0) | −0.1 (−0.2 to 0.0) | 0.0 (−0.2 to 0.2) |
| ACR (mg/g) | 927 | 949 | 1017 | 861 |
| Geometric mean ACR change: % (95% CI) | −31 (−35 to −26) | −29 (−33 to −25) | −35 (−39 to −31) | −15 (−23 to −6) |
| Stage 4 CKD (%) | 4 | 14 | 14 | 16 |
| eGFR (mL/min/1.73 m2) | 56 | 43 | 44 | 42 |
| LSM change in the eGFR slope (mL/min/1.73 m2/year) | 1.52 (1.11 to 1.93) | 0.93 (0.61 to 1.25) | 1.18 (0.79 to 1.56) | 0.46 (−0.10 to 1.03) |
| Initial decline in eGFR * (SGLT2i vs. PBO) (mL/min/1.73 m2) | −3.7 vs. −0.6 | −4.0 vs. −0.8 | −3.2 vs. −0.6 | −2.8 vs. −0.8 |
| Decline in eGFR after initial phase (SGLT2i vs. PBO) (mL/min/1.73 m2/year) | −1.9 vs. −4.6 | −1.7 vs. −3.6 | −1.6 vs. −3.8 | −1.9 vs. −3.2 |
| Prior CV disease (%) | 50 | 37 | 44 | 24 |
| Primary endpoint **: HR (95% CI) | 0.70 (0.59 to 0.82) | 0.61 (0.51 to 0.72) | 0.64 (0.52 to 0.79) | 0.50 (0.35 to 0.72) |
| CV death or HHF ***: HR (95% CI) | 0.69 (0.57 to 0.83) | 0.71 (0.55 to 0.92) | 0.70 (0.53 to 0.92) | 0.79 (0.40 to 1.55) |
| All cause mortality ***: HR (95% CI) | 0.83 (0.68 to 1.02) | 0.69 (0.53 to 0.88) | 0.74 (0.56 to 0.98) | 0.52 (0.29 to 0.93) |
| DECLARE-TIMI58 | CANVAS | EMPA-REG OUTCOME | CREDENCE | DAPA-CKD | |
|---|---|---|---|---|---|
| Prior CVD (%) | 40.6 | 65.6 | 99.2 | 50.4 | 37.4 |
| Baseline eGFR (mL/min/1.73 m2) | 85 | 77 | 74 | 56 | 43 |
| Composite kidney outcomes *: HR (95% CI) | 0.53 (0.43 to 0.66) | 0.60 (0.47 to 0.77) | 0.54 (0.40 to 0.75) | 0.70 (0.59 to 0.82) | 0.61 (0.51 to 0.72) |
| 3P-MACE: HR (95% CI) | 0.93 (0.84 to 1.03) | 0.86 (0.75 to 0.97) | 0.86 (0.74 to 0.99) | 0.80 (0.67 to 0.95) | 0.92 (0.72 to 1.16) |
| HHF: HR (95% CI) | 0.73 (0.61 to 0.88) | 0.67 (0.52 to 0.87) | 0.65 (0.50 to 0.85) | 0.61 (0.47 to 0.80) | 0.51 (0.34 to 0.76) |
| HHF and CV death: HR (95% CI) | 0.85 (0.73 to 0.95) | 0.78 (0.67 to 0.91) | 0.66 (0.55 to 0.79) | 0.69 (0.57 to 0.83) | 0.71 (0.55 to 0.92) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gohda, T.; Murakoshi, M. Sodium-Glucose Cotransporter-2 Inhibitors—Miracle Drugs for the Treatment of Chronic Kidney Disease Irrespective of the Diabetes Status: Lessons from the Dedicated Kidney Disease-Focused CREDENCE and DAPA-CKD Trials. Int. J. Mol. Sci. 2022, 23, 13749. https://doi.org/10.3390/ijms232213749
Gohda T, Murakoshi M. Sodium-Glucose Cotransporter-2 Inhibitors—Miracle Drugs for the Treatment of Chronic Kidney Disease Irrespective of the Diabetes Status: Lessons from the Dedicated Kidney Disease-Focused CREDENCE and DAPA-CKD Trials. International Journal of Molecular Sciences. 2022; 23(22):13749. https://doi.org/10.3390/ijms232213749
Chicago/Turabian StyleGohda, Tomohito, and Maki Murakoshi. 2022. "Sodium-Glucose Cotransporter-2 Inhibitors—Miracle Drugs for the Treatment of Chronic Kidney Disease Irrespective of the Diabetes Status: Lessons from the Dedicated Kidney Disease-Focused CREDENCE and DAPA-CKD Trials" International Journal of Molecular Sciences 23, no. 22: 13749. https://doi.org/10.3390/ijms232213749
APA StyleGohda, T., & Murakoshi, M. (2022). Sodium-Glucose Cotransporter-2 Inhibitors—Miracle Drugs for the Treatment of Chronic Kidney Disease Irrespective of the Diabetes Status: Lessons from the Dedicated Kidney Disease-Focused CREDENCE and DAPA-CKD Trials. International Journal of Molecular Sciences, 23(22), 13749. https://doi.org/10.3390/ijms232213749