
A Multidisciplinary Telerehabilitation Approach for Supporting Social Interaction in Autism Spectrum Disorder Families: An Italian Digital Platform in Response to COVID-19

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
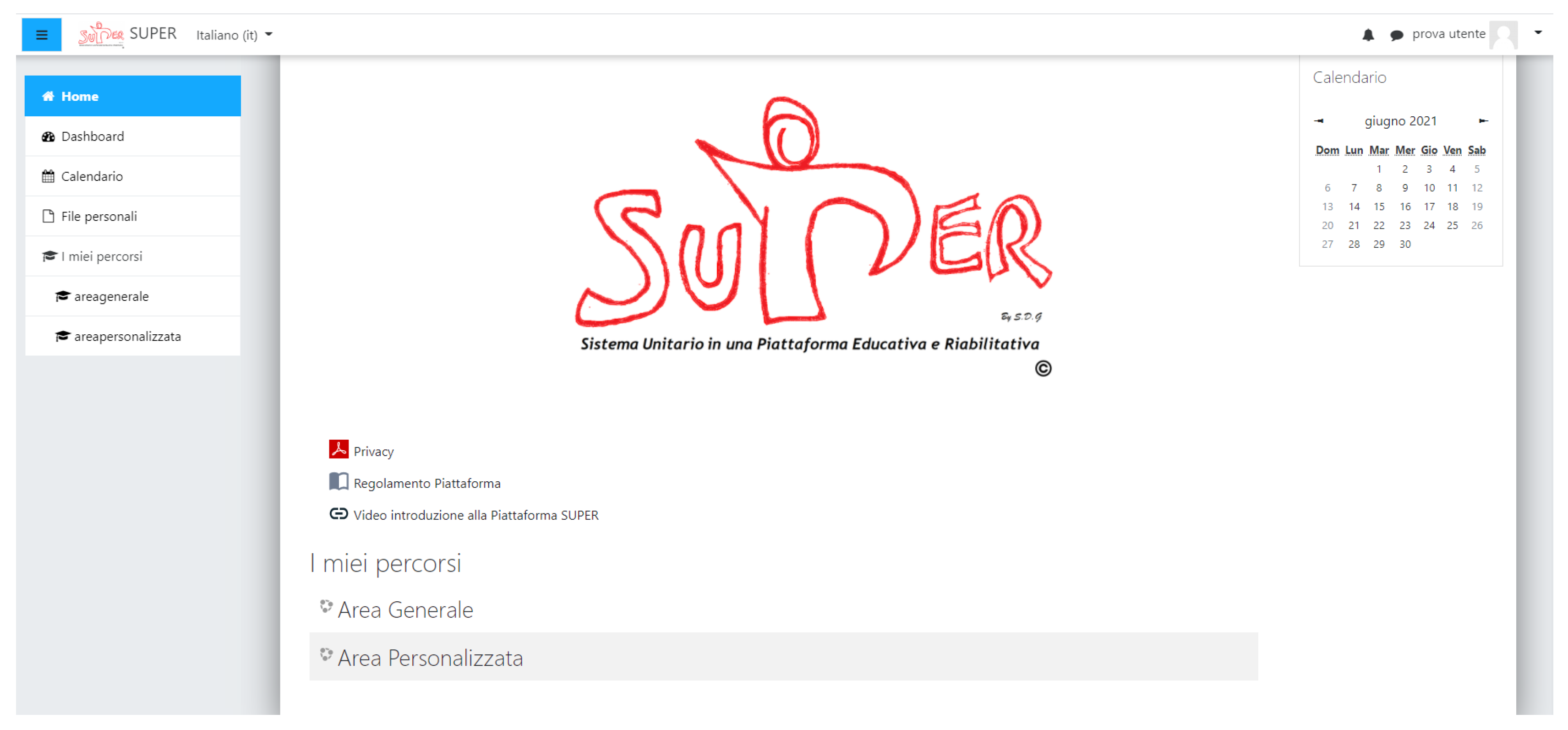
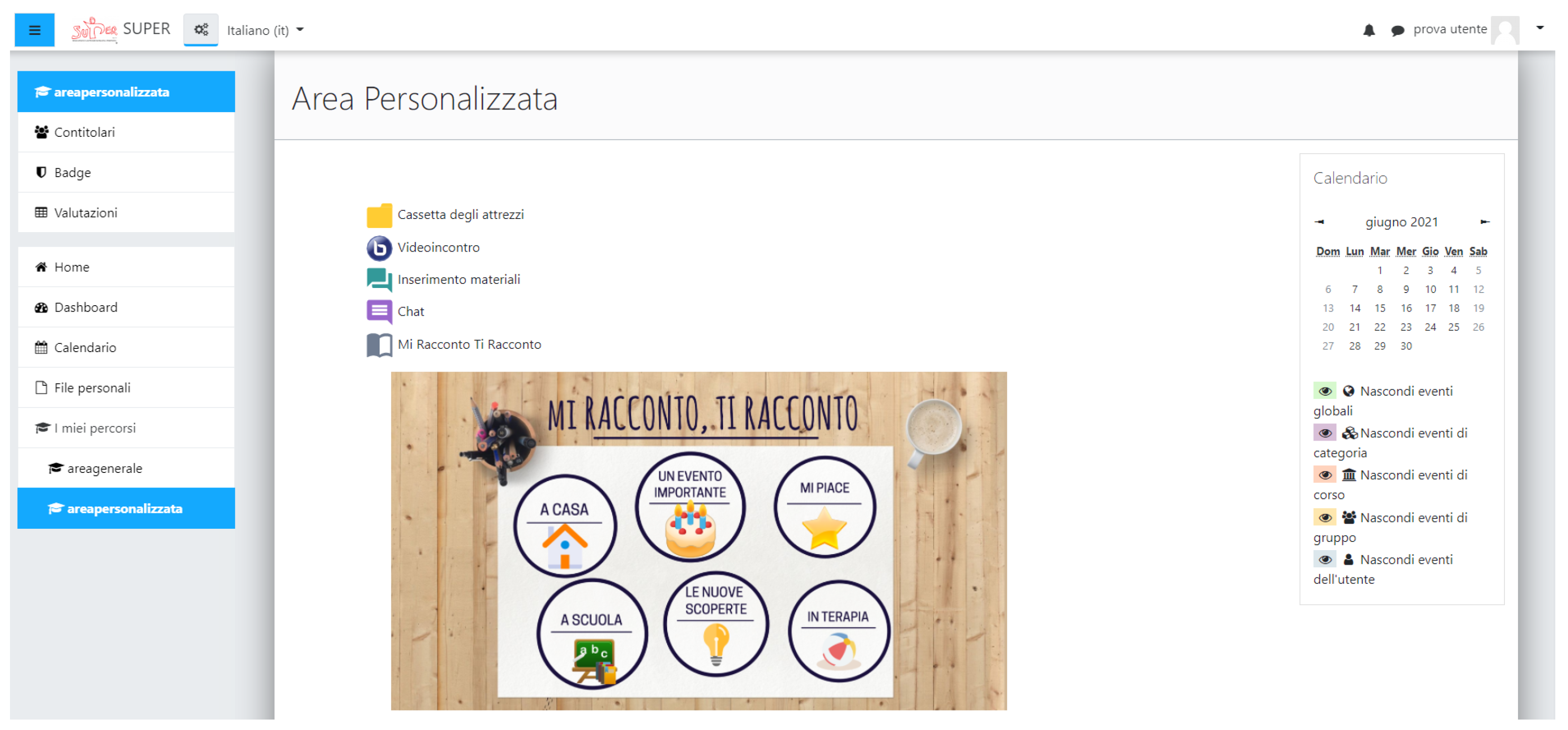
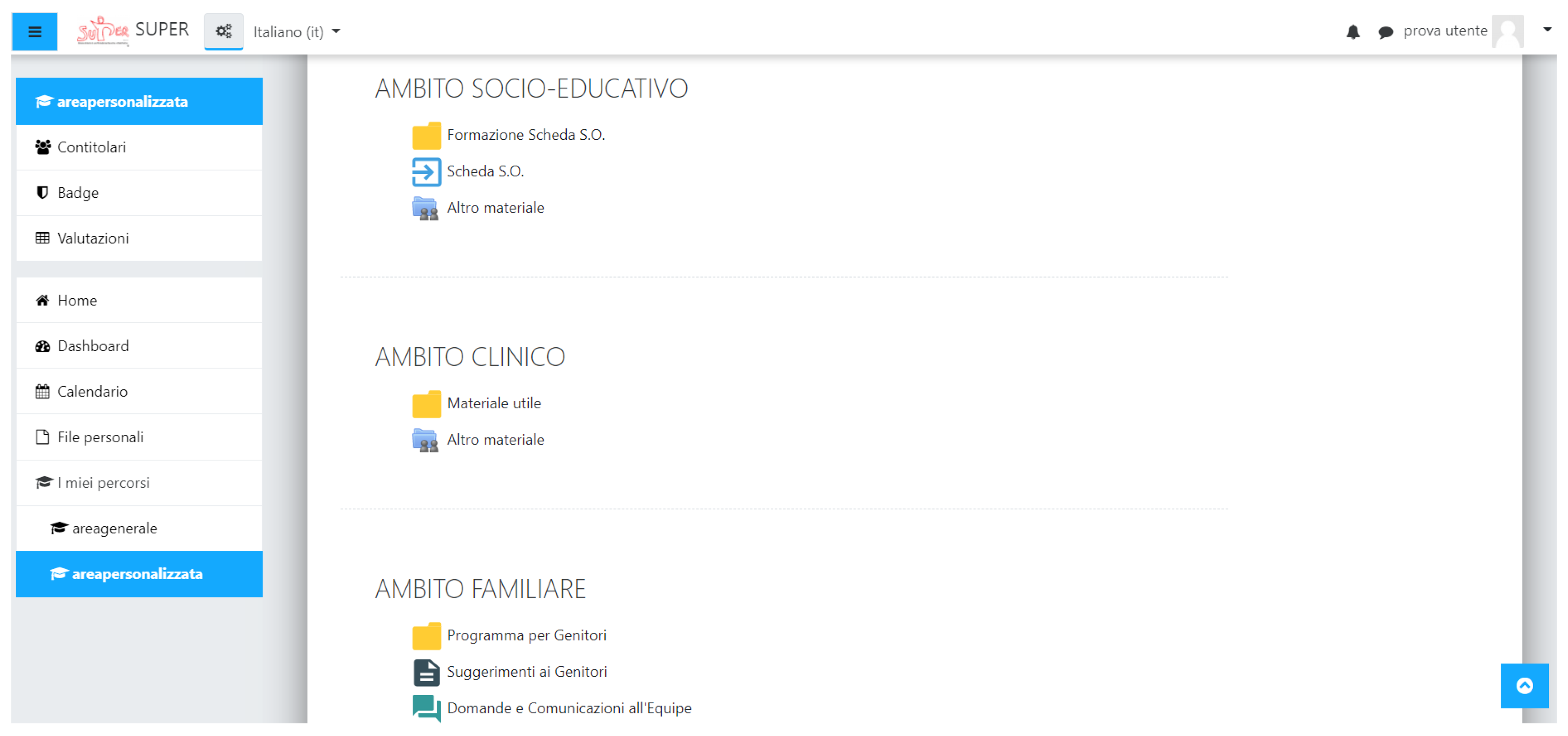
2.1. The SUPER Platform
- Understanding ASD: providing information on ASD and its clinical features (including etiopathogenesis, epidemiology, symptoms, diagnostic tools, interventions).
- Contexts: providing information on how ASD can affect different life contexts (including family, school, clinical settings, society).
- Research material: providing content on specific topics.
2.2. Usability Evaluation
2.2.1. Participants
2.2.2. Procedure
2.2.3. Outcome Measures
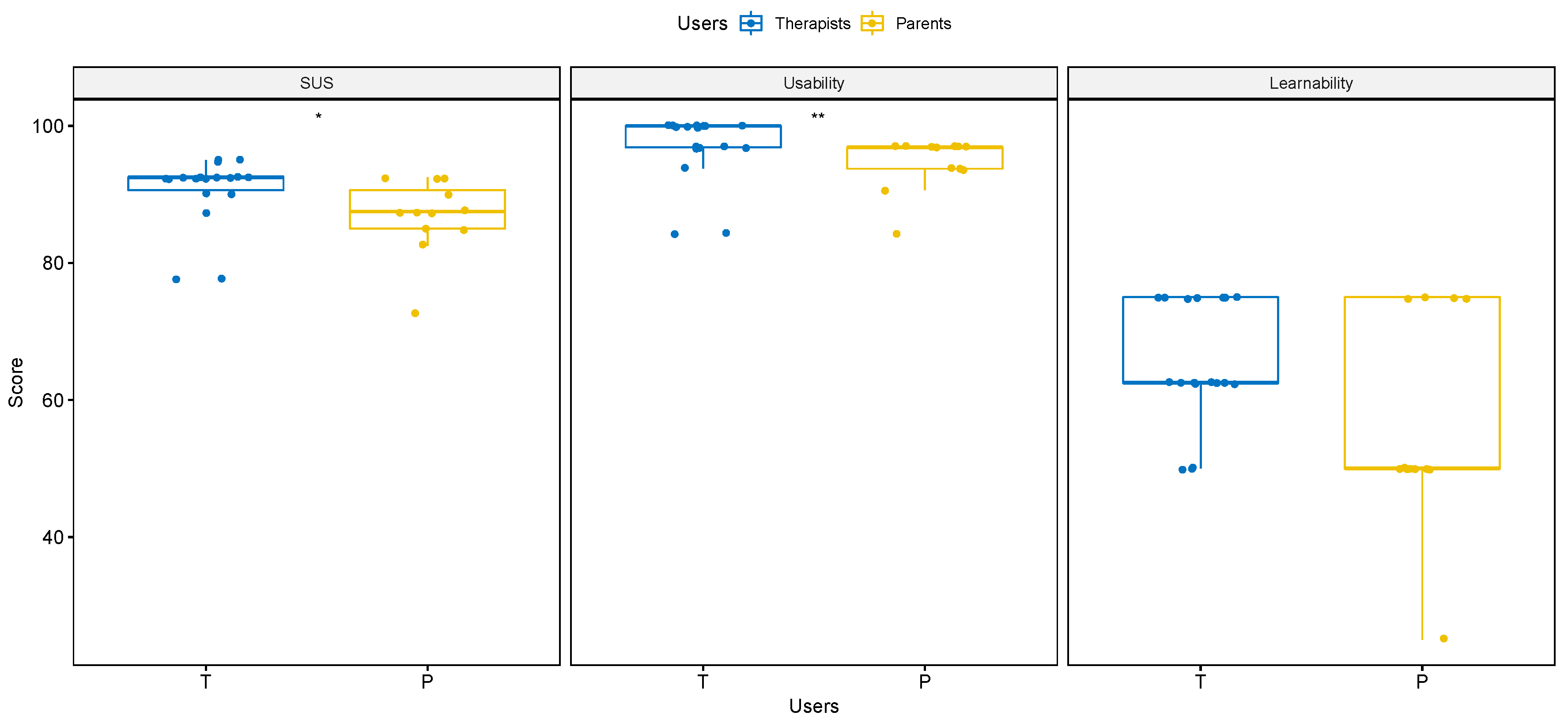
2.2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ASD | Autism spectrum disorder |
| ICF-CY | International Classification of Functioning, Disability and Health for children and youth |
| SUPER | Sistema Unitario in una Piattaforma Riabilitativa ed Educativa |
| SUS | System usability scale |
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Chita-Tegmark, M. Social attention in ASD: A review and meta-analysis of eye-tracking studies. Res. Dev. Disabil. 2016, 48, 79–93. [Google Scholar] [CrossRef]
- Mouga, S.; Castelhano, J.; Café, C.; Sousa, D.; Duque, F.; Oliveira, G.; Castelo-Branco, M. Social Attention Deficits in Children with Autism Spectrum Disorder: Task Dependence of Objects vs. Faces Observation Bias. Front. Psychiatry 2021, 12, 185. [Google Scholar] [CrossRef]
- Purpura, G.; Tagliabue, L.; Petri, S.; Cerroni, F.; Mazzarini, A.; Nacinovich, R. Caregivers’ Burden of School-Aged Children with Neurodevelopmental Disorders: Implications for Family-Centred Care. Brain Sci. 2021, 11, 875. [Google Scholar] [CrossRef] [PubMed]
- Davis, N.O.; Carter, A.S. Parenting stress in mothers and fathers of toddlers with autism spectrum disorders: Associations with child characteristics. J. Autism Dev. Disord. 2008, 38, 1278. [Google Scholar] [CrossRef]
- Baykal, S.; Karakurt, M.N.; Çakır, M.; Karabekiroğlu, K. An examination of the relations between symptom distributions in children diagnosed with autism and caregiver burden, anxiety and depression levels. Community Ment. Health J. 2019, 55, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Diggle, T.; McConachie, H. Parent-mediated early intervention for young children with autism spectrum disorder. Cochrane Database Syst. Rev. 2002. [Google Scholar] [CrossRef]
- Hyman, S.L.; Levy, S.E.; Myers, S.M.; Council on Children with Disabilities; Section on Developmental and Behavioral Pediatrics. Identification, Evaluation, and Management of Children with Autism Spectrum Disorder. Pediatrics 2020, 145, e20193447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellerbeck, K.; Smith, C.; Courtemanche, A. Care of Children with Autism Spectrum Disorder. Prim. Care Clin. Off. Pract. 2015, 42, 85–98. [Google Scholar] [CrossRef]
- Scottish Intercollegiate Guidelines Network (SIGN). Assessment, Diagnosis and Interventions for Autism Spectrum Disorders; SIGN: Edinburgh, UK, 2016; Available online: https://www.sign.ac.uk/assets/sign145.pdf (accessed on 20 September 2021).
- Fuentes, J.; Hervás, A.; Howlin, P. ESCAP practice guidance for autism: A summary of evidence-based recommendations for diagnosis and treatment. Eur. Child Adolesc. Psychiatry 2021, 30, 961–984. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence (UK). Autism Spectrum Disorder in under 19s: Support and Management (NICE Clinical Guideline 170). 2013. Available online: https://www.nice.org.uk/guidance/cg170 (accessed on 23 September 2021).
- Whitehouse, A.; Evans, K.; Eapen, V.; Prior, M.; Wray, J. The Diagnostic Process for Children, Adolescents and Adults Referred for Assessment of Autism Spectrum Disorder in Australia: A National Guideline (Draft Version for Community Consultation). 2017. Available online: https://www.autismcrc.com.au/sites/default/files/inline-files/Australian%20National%20Guideline%20for%20ASD%20Assessment%20-%20Draft%20Version%20for%20Community%20Consultation_0.pdf (accessed on 21 September 2021).
- Myers, S.M.; Johnson, C.P. Management of Children with Autism Spectrum Disorders. Pediatrics 2007, 120, 1162–1182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palisano, R.J.; Di Rezze, B.; Stewart, D.; Rosenbaum, P.L.; Hlyva, O.; Freeman, M.; Nguyen, T.; Gorter, J.W. Life course health development of individuals with neurodevelopmental conditions. Dev. Med. Child Neurol. 2017, 59, 470–476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayes, M.J. An evaluation of the impacts of the Social Communication Emotional Regulation and Transactional Support (SCERTS®) Model on multidisciplinary collaboration. Int. J. Cross-Discip. Subj. Educ. 2015, 5, 2411–2415. [Google Scholar]
- World Health Organization. Statement on the Second Meeting of the International Health Regulations. Emergency Committee Regarding the Outbreak of Novel Coronavirus (2019-nCoV). 2020. Available online: https://www.who.int/news/item/30-01-2020-statement-on-the-second-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov) (accessed on 20 July 2021).
- Narzisi, A. Phase 2 and Later of COVID-19 Lockdown: Is it Possible to Perform Remote Diagnosis and Intervention for Autism Spectrum Disorder? An Online-Mediated Approach. J. Clin. Med. 2020, 9, 1850. [Google Scholar] [CrossRef] [PubMed]
- Conti, E.; Sgandurra, G.; De Nicola, G.; Biagioni, T.; Boldrini, S.; Bonaventura, E.; Buchignani, B.; Della Vecchia, S.; Falcone, F.; Fedi, C.; et al. Behavioural and Emotional Changes during COVID-19 Lockdown in an Italian Paediatric Population with Neurologic and Psychiatric Disorders. Brain Sci. 2020, 10, 918. [Google Scholar] [CrossRef]
- Dhiman, S.; Sahu, P.K.; Reed, W.R.; Ganesh, G.S.; Goyal, R.K.; Jain, S. Impact of COVID-19 outbreak on mental health and perceived strain among caregivers tending children with special needs. Res. Dev. Disabil. 2020, 107, 103790. [Google Scholar] [CrossRef] [PubMed]
- Conti, E.; Chericoni, N.; Costanzo, V.; Lasala, R.; Mancini, A.; Prosperi, M.; Tancredi, R.; Muratori, F.; Calderoni, S.; Apicella, F. Moving Toward Telehealth Surveillance Services for Toddlers at Risk for Autism During the COVID-19 Pandemic. Front. Psychiatry 2020, 11, 1285. [Google Scholar] [CrossRef]
- Daulay, N. Home education for children with autism spectrum disorder during the COVID-19 pandemic: Indonesian mothers experience. Res. Dev. Disabil. 2021, 114, 103954. [Google Scholar] [CrossRef] [PubMed]
- Desideri, L.; Pérez-Fuster, P.; Herrera, G. Information and Communication Technologies to Support Early Screening of Autism Spectrum Disorder: A Systematic Review. Children 2021, 8, 93. [Google Scholar] [CrossRef] [PubMed]
- Gevarter, C.; Najar, A.M.; Flake, J.; Tapia-Alvidrez, F.; Lucero, A. Naturalistic Communication Training for Early Intervention Providers and Latinx Parents of Children with Signs of Autism. J. Dev. Phys. Disabil. 2021, 1–23. [Google Scholar] [CrossRef]
- Wagner, L.; Corona, L.L.; Weitlauf, A.S.; Marsh, K.L.; Berman, A.F.; Broderick, N.A.; Francis, S.; Hine, J.; Nicholson, A.; Stone, C.; et al. Use of the TELE-ASD-PEDS for Autism Evaluations in Response to COVID-19: Preliminary Outcomes and Clinician Acceptability. J. Autism Dev. Disord. 2020, 51, 3063–3072. [Google Scholar] [CrossRef] [PubMed]
- Pecini, C.; Spoglianti, S.; Michetti, S.; Bonetti, S.; Di Lieto, M.C.; Gasperini, F.; Cristofani, P.; Bozza, M.; Brizzolara, D.; Casalini, C.; et al. Telerehabilitation in developmental dyslexia: Methods of implementation and expected results. Minerva Pediatr. 2018, 70, 529–538. [Google Scholar] [CrossRef]
- Provenzi, L.; Grumi, S.; Borgatti, R. Alone with the kids: Tele-medicine for children with special healthcare needs during COVID-19 emergency. Front. Psychol. 2020, 11, 2193. [Google Scholar] [CrossRef]
- Faccioli, S.; Lombardi, F.; Bellini, P.; Costi, S.; Sassi, S.; Pesci, M.C. How did Italian adolescents with disability and parents deal with the COVID-19 emergency? Int. J. Environ. Res. Public Health 2021, 18, 1687. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. International Classification of Functioning, Disability and Health: Children & Youth Version: ICF-CY; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Brooke, J. SUS: A quick and dirty usability scale. Usabil. Eval. Ind. 1996, 189, 4–7. [Google Scholar]
- Aldred, C.; Taylor, C.; Wan, M.; Green, J. Using video feedback strategies in parent-mediated early autism intervention. In Handbook of Parent-Implemented Interventions for Very Young Children with Autism; Siller, M., Morgan, L., Eds.; Autism and Child Psychopathology Series; Springer International Publishing: Cham, Switzerland, 2018; pp. 221–239. [Google Scholar]
- Modular Object-Oriented Dynamic Learning Environment—MOODLE. Available online: https://moodle.org (accessed on 12 June 2021).
- Gogan, M.L.; Sirbu, R.; Draghici, A. Aspects Concerning the Use of the Moodle Platform—Case Study. Procedia Technol. 2015, 19, 1142–1148. [Google Scholar] [CrossRef] [Green Version]
- The European Parliament. Regulation (EU) 2016/679 of the European Parliament and of the Council of 27 April 2016 on the Protection of Natural Persons with Regard to the Processing of Personal Data and on the Free Movement of Such Data, and Repealing Directive 95/46/EC (General Data Protection Regulation). 2016. Available online: https://eur-lex.europa.eu/eli/reg/2016/679/oj (accessed on 14 July 2021).
- Borsci, S.; Federici, S.; Lauriola, M. On the dimensionality of the System Usability Scale: A test of alternative measurement models. Cogn. Process. 2009, 10, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Bangor, A.; Kortum, P.; Miller, J. Determining what individual SUS scores mean: Adding an adjective rating scale. J. Usabil. Stud. 2009, 4, 114–123. [Google Scholar]
- Othman, M.K.; Nogoibaeva, A.; Leong, L.S.; Barawi, M.H. Usability evaluation of a virtual reality smartphone app for a living museum. Univers. Access Inf. Soc. 2021, 1–18. [Google Scholar] [CrossRef]
- Lewis, J.R.; Sauro, J. The factor structure of the system usability scale. In Proceedings of the International Conference on Human Centered Design, San Diego, CA, USA, 19–24 July 2009; Springer: Berlin/Heidelberg, Germany, 2009; pp. 94–103. [Google Scholar]
- Golomb, M.R.; Mcdonald, B.C.; Warden, S.J.; Yonkman, J.; Saykin, A.J.; Shirley, B.; Huber, M.; Rabin, B.; Abdelbaky, M.; Nwosu, M.E.; et al. In-Home Virtual Reality Videogame Telerehabilitation in Adolescents with Hemiplegic Cerebral Palsy. Arch. Phys. Med. Rehabil. 2010, 91, 1–8.e1. [Google Scholar] [CrossRef] [PubMed]
- Tinelli, F.; Cioni, G.; Purpura, G. Development and Implementation of a New Telerehabilitation System for Audiovisual Stimulation Training in Hemianopia. Front. Neurol. 2017, 8, 621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Philpott-Robinson, K.; Lane, A.E.; Harpster, K. Sensory features of toddlers at risk for autism spectrum disorder. Am. J. Occup. Ther. 2016, 70, 7004220010p1–7004220010p8. [Google Scholar] [CrossRef]
- Purpura, G.; Costanzo, V.; Chericoni, N.; Puopolo, M.; Scattoni, M.L.; Muratori, F.; Apicella, F. Bilateral Patterns of Repetitive Movements in 6- to 12-Month-Old Infants with Autism Spectrum Disorders. Front. Psychol. 2017, 8, 1168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- LeBarton, E.S.; Landa, R.J. Infant motor skill predicts later expressive language and autism spectrum disorder diagnosis. Infant Behav. Dev. 2019, 54, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Apicella, F.; Costanzo, V.; Purpura, G. Are early visual behavior impairments involved in the onset of autism spectrum disorders? Insights for early diagnosis and intervention. Eur. J. Pediatr. 2020, 179, 225–234. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| User Profile | User Type |
|---|---|
| Clinical profile | Pediatrics, neuropsychiatrists, therapists, psychologists, and other clinical professionals |
| Social and educational profile | Teachers, educators, special needs teachers, social workers, and other social and educational professionals |
| Family profile | Parents, relatives, caregivers, and legal guardians |
| Sections of the Personalized Area | User Access |
|---|---|
| General section | Accessible to all users |
| Clinical section | Access restricted to users with a clinical profile |
| Socio-educational section | Access restricted to users with socio-educational and clinical profiles |
| Family section | Access restricted to users with family and clinical profiles |
| Tasks | |
|---|---|
| 1 | Explore the platform |
| 2 | Play videos in the General Area |
| 3 | Download materials from the General Area |
| 4 | Use tools in the Personalized Area |
| SUS English Version | SUS Italian Version |
|---|---|
| 1. I think I would like to use this system frequently. | 1. Penso che mi piacerebbe utilizzare questo sistema frequentemente. |
| 2. I found the system unnecessarily complex. | 2. Ho trovato il sistema complesso senza che ce ne fosse bisogno. |
| 3. I thought the system was easy to use. | 3. Ho trovato il sistema molto semplice da usare. |
| 4. I think I would need the support of a technical person to be able to use this system. | 4. Penso che avrei bisogno del supporto di una persona già in grado di utilizzare il sistema. |
| 5. I found the various functions in this system were well integrated. | 5. Ho trovato le varie funzionalità del sistema bene integrate. |
| 6. I thought there was too much inconsistency in this system. | 6. Ho trovato incoerenze tra le varie funzionalità del sistema. |
| 7. I would imagine that most people would learn to use this system very quickly. | 7. Penso che la maggior parte delle persone potrebbero imparare ad utilizzare il sistema facilmente. |
| 8. I found the system very cumbersome to use. | 8. Ho trovato il sistema molto macchinoso da utilizzare. |
| 9. I felt very confident using the system. | 9. Ho avuto molta confidenza con il sistema durante l’uso. |
| 10. I needed to learn a lot of things before I could get going with this system. | 10. Ho avuto bisogno di imparare molti processi prima di riuscire ad utilizzare al meglio il sistema. |
| Scale | Total Participants | Therapist Group | Parent Group |
|---|---|---|---|
| (n = 30) | (n = 18) | (n = 12) | |
| SUS | 89.2 (SD = 5.5) | 90.7 (SD = 5.1) | 86.9 (SD = 5.5) |
| Usability | 96.1 (SD = 4.6) | 97.1 (SD = 5.0) | 94.6 (SD = 3.8) |
| Learnability | 61.7 (SD = 12.5) | 65.3 (SD = 9.1) | 56.2 (SD = 15.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vallefuoco, E.; Purpura, G.; Gison, G.; Bonifacio, A.; Tagliabue, L.; Broggi, F.; Scuccimarra, G.; Pepino, A.; Nacinovich, R. A Multidisciplinary Telerehabilitation Approach for Supporting Social Interaction in Autism Spectrum Disorder Families: An Italian Digital Platform in Response to COVID-19. Brain Sci. 2021, 11, 1404. https://doi.org/10.3390/brainsci11111404
Vallefuoco E, Purpura G, Gison G, Bonifacio A, Tagliabue L, Broggi F, Scuccimarra G, Pepino A, Nacinovich R. A Multidisciplinary Telerehabilitation Approach for Supporting Social Interaction in Autism Spectrum Disorder Families: An Italian Digital Platform in Response to COVID-19. Brain Sciences. 2021; 11(11):1404. https://doi.org/10.3390/brainsci11111404
Chicago/Turabian StyleVallefuoco, Ersilia, Giulia Purpura, Giovanna Gison, Andrea Bonifacio, Luca Tagliabue, Fiorenza Broggi, Goffredo Scuccimarra, Alessandro Pepino, and Renata Nacinovich. 2021. "A Multidisciplinary Telerehabilitation Approach for Supporting Social Interaction in Autism Spectrum Disorder Families: An Italian Digital Platform in Response to COVID-19" Brain Sciences 11, no. 11: 1404. https://doi.org/10.3390/brainsci11111404
APA StyleVallefuoco, E., Purpura, G., Gison, G., Bonifacio, A., Tagliabue, L., Broggi, F., Scuccimarra, G., Pepino, A., & Nacinovich, R. (2021). A Multidisciplinary Telerehabilitation Approach for Supporting Social Interaction in Autism Spectrum Disorder Families: An Italian Digital Platform in Response to COVID-19. Brain Sciences, 11(11), 1404. https://doi.org/10.3390/brainsci11111404