
Female Patients with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome or Idiopathic Chronic Fatigue: Comparison of Responses to a Two-Day Cardiopulmonary Exercise Testing Protocol


Abstract
1. Introduction
2. Materials and Methods
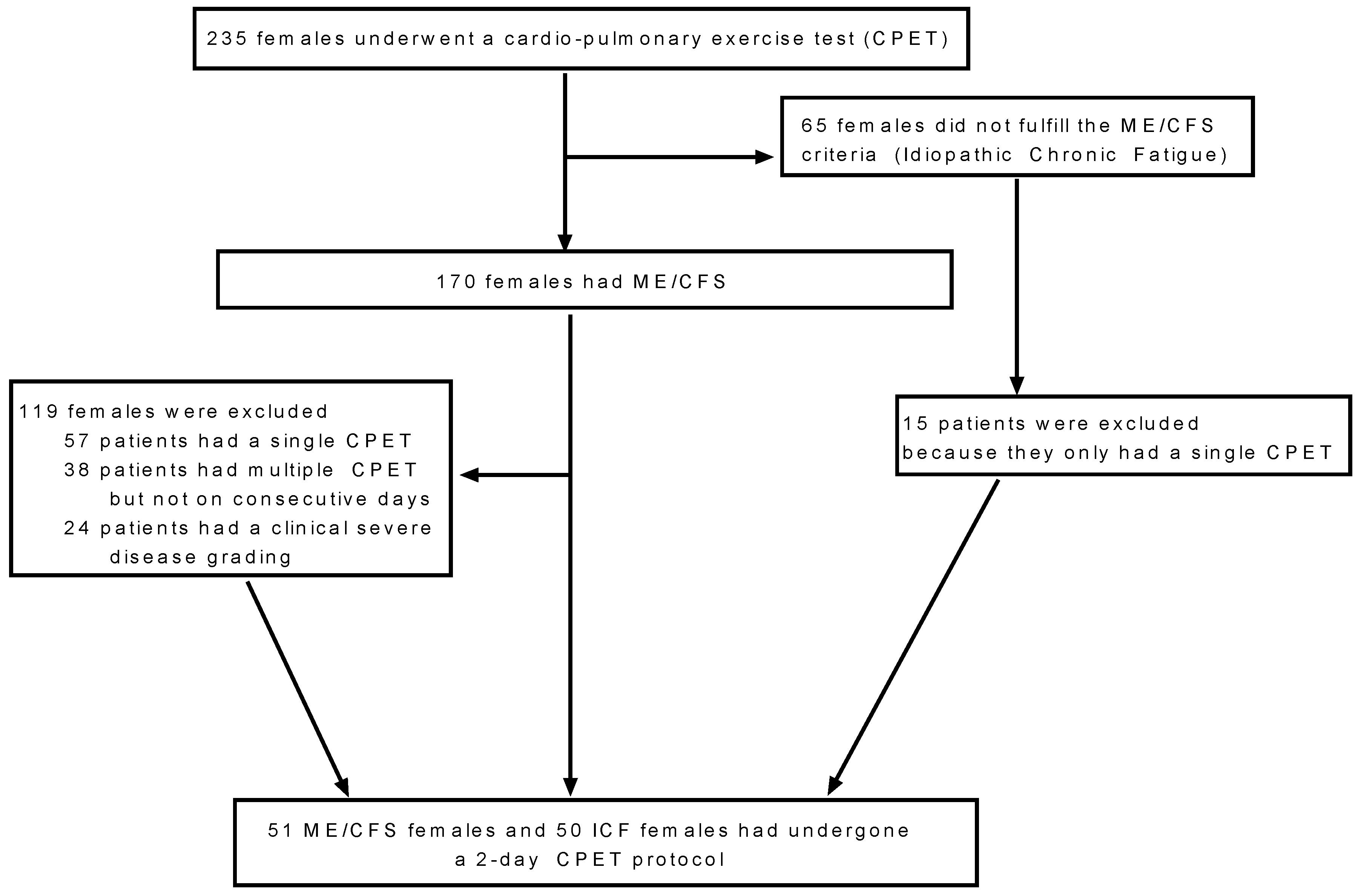
2.1. Participants
2.2. Cardiopulmonary Exercise Testing (CPET)
2.3. Statistical Analysis
3. Results
4. Discussion
4.1. Cardiopulmonary Exercise Testing in Idiopathic Chronic Fatigue: Comparison to Literature
4.2. Cardiopulmonary Exercise Testing 2-Day Protocols: Comparison to Literature
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

References
- Carruthers, B.M.; van de Sande, M.I.; De Meirleir, K.L.; Klimas, N.G.; Broderick, G.; Mitchell, T.; Stevens, S. Myalgic encephalomyelitis: International Consensus Criteria. J. Intern. Med. 2011, 270, 327–338. [Google Scholar] [CrossRef]
- Clayton, E.W. Beyond myalgic encephalomyelitis/chronic fatigue syndrome: An IOM report on redefining an illness. JAMA 2015, 313, 1101–1102. [Google Scholar] [CrossRef]
- Fukuda, K.; Straus, S.E.; Hickie, I.; Sharpe, M.C.; Dobbins, J.G.; Komaroff, A. The chronic fatigue syndrome: A comprehensive approach to its definition and study. International Chronic Fatigue Syndrome Study Group. Ann. Intern. Med. 1994, 121, 953–959. [Google Scholar] [CrossRef]
- Institute of Medicine (IOM) (Ed.) Beyond Mayalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness; The National Academies Press: Washington, DC, USA, 2015. [Google Scholar]
- Jones, D.E.; Hollingsworth, K.G.; Taylor, R.; Blamire, A.M.; Newton, J.L. Abnormalities in pH handling by peripheral muscle and potential regulation by the autonomic nervous system in chronic fatigue syndrome. J. Intern. Med. 2010, 267, 394–401. [Google Scholar] [CrossRef] [PubMed]
- Paul, L.; Wood, L.; Behan, W.M.; Maclaren, W.M. Demonstration of delayed recovery from fatiguing exercise in chronic fatigue syndrome. Eur. J. Neurol. 1999, 6, 63–69. [Google Scholar] [CrossRef]
- Fulle, S.; Pietrangelo, T.; Mancinelli, R.; Saggini, R.; Fano, G. Specific correlations between muscle oxidative stress and chronic fatigue syndrome: A working hypothesis. J. Muscle Res. Cell Motil. 2007, 28, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Gur, A.; Oktayoglu, P. Central nervous system abnormalities in fibromyalgia and chronic fatigue syndrome: New concepts in treatment. Curr. Pharm. Des. 2008, 14, 1274–1294. [Google Scholar] [CrossRef]
- McCully, K.K.; Malucelli, E.; Iotti, S. Increase of free Mg2+ in the skeletal muscle of chronic fatigue syndrome patients. Dyn. Med. 2006, 5, 1. [Google Scholar] [CrossRef] [PubMed]
- McCully, K.K.; Smith, S.; Rajaei, S.; Leigh, J.S., Jr.; Natelson, B.H. Blood flow and muscle metabolism in chronic fatigue syndrome. Clin. Sci. 2003, 104, 641–647. [Google Scholar] [CrossRef] [PubMed]
- Siemionow, V.; Fang, Y.; Calabrese, L.; Sahgal, V.; Yue, G.H. Altered central nervous system signal during motor performance in chronic fatigue syndrome. Clin. Neurophysiol. 2004, 115, 2372–2381. [Google Scholar] [CrossRef]
- Wong, R.; Lopaschuk, G.; Zhu, G.; Walker, D.; Catellier, D.; Burton, D.; Montague, T. Skeletal muscle metabolism in the chronic fatigue syndrome. In vivo assessment by 31P nuclear magnetic resonance spectroscopy. Chest 1992, 102, 1716–1722. [Google Scholar] [CrossRef]
- De Becker, P.; Roeykens, J.; Reynders, M.; McGregor, N.; De Meirleir, K. Exercise capacity in chronic fatigue syndrome. Arch. Intern. Med. 2000, 160, 3270–3277. [Google Scholar] [CrossRef]
- Fulcher, K.Y.; White, P.D. Strength and physiological response to exercise in patients with chronic fatigue syndrome. J. Neurol. Neurosurg. Psychiatry 2000, 69, 302–307. [Google Scholar] [CrossRef]
- Hodges, L.D.; Nielsen, T.; Baken, D. Physiological measures in participants with chronic fatigue syndrome, multiple sclerosis and healthy controls following repeated exercise: A pilot study. Clin. Physiol. Funct. Imaging 2018, 38, 639–644. [Google Scholar] [CrossRef]
- Jammes, Y.; Steinberg, J.G.; Mambrini, O.; Bregeon, F.; Delliaux, S. Chronic fatigue syndrome: Assessment of increased oxidative stress and altered muscle excitability in response to incremental exercise. J. Intern. Med. 2005, 257, 299–310. [Google Scholar] [CrossRef]
- Keller, B.A.; Pryor, J.L.; Giloteaux, L. Inability of myalgic encephalomyelitis/chronic fatigue syndrome patients to reproduce VO(2)peak indicates functional impairment. J. Transl. Med. 2014, 12, 104. [Google Scholar] [CrossRef] [PubMed]
- Sargent, C.; Scroop, G.C.; Nemeth, P.M.; Burnet, R.B.; Buckley, J.D. Maximal oxygen uptake and lactate metabolism are normal in chronic fatigue syndrome. Med. Sci. Sports Exerc. 2002, 34, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Sisto, S.A.; LaManca, J.; Cordero, D.L.; Bergen, M.T.; Ellis, S.P.; Drastal, S.; Natelson, B.H. Metabolic and cardiovascular effects of a progressive exercise test in patients with chronic fatigue syndrome. Am. J. Med. 1996, 100, 634–640. [Google Scholar] [CrossRef]
- Snell, C.R.; Stevens, S.R.; Davenport, T.E.; Van Ness, J.M. Discriminative Validity of Metabolic and Workload Measurements to Identify Individuals with Chronic Fatigue Syndrome. Phys. Ther. 2013, 93, 1484–1492. [Google Scholar] [CrossRef]
- Vanness, J.M.; Snell, C.R.; Stevens, S.R. Diminished cardiopulmonary capacity during post-exertional malaise. J. Chronic Fatigue Syndr. 2007, 14, 77–85. [Google Scholar] [CrossRef]
- Vermeulen, R.C.; Kurk, R.M.; Visser, F.C.; Sluiter, W.; Scholte, H.R. Patients with chronic fatigue syndrome performed worse than controls in a controlled repeated exercise study despite a normal oxidative phosphorylation capacity. J. Transl. Med. 2010, 11, 93. [Google Scholar] [CrossRef]
- Vermeulen, R.C.; Vermeulen van Eck, I.W. Decreased oxygen extraction during cardiopulmonary exercise test in patients with chronic fatigue syndrome. J. Transl. Med. 2014, 12, 20. [Google Scholar] [CrossRef] [PubMed]
- Wallman, K.E.; Morton, A.R.; Goodman, C.; Grove, R. Physiological responses during a submaximal cycle test in chronic fatigue syndrome. Med. Sci. Sports Exerc. 2004, 36, 1682–1688. [Google Scholar] [CrossRef] [PubMed]
- Nelson, M.J.; Buckley, J.D.; Thomson, R.L.; Clark, D.; Kwiatek, R.; Davison, K. Diagnostic sensitivity of 2-day cardiopulmonary exercise testing in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. J. Transl. Med. 2019, 17, 80. [Google Scholar] [CrossRef]
- Lien, K.; Johansen, B.; Veierød, M.B.; Haslestad, A.S.; Bøhn, S.K.; Melsom, M.N.; Iversen, P.O. Abnormal blood lactate accumulation during repeated exercise testing in myalgic encephalomyelitis/chronic fatigue syndrome. Physiol. Rep. 2019, 7, e14138. [Google Scholar] [CrossRef] [PubMed]
- Del Core, M.A.; Ahn, J.; Wukich, D.K.; Liu, G.T.; Lalli, T.; VanPelt, M.D.; Raspovic, K.M. Gender Differences on SF-36 Patient-Reported Outcomes of Diabetic Foot Disease. Int. J. Low Extrem. Wounds 2018, 17, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Elmariah, S.; Goldberg, L.R.; Allen, M.T.; Kao, A. Effects of gender on peak oxygen consumption and the timing of cardiac transplantation. J. Am. Coll. Cardiol. 2006, 47, 2237–2242. [Google Scholar] [CrossRef] [PubMed]
- Faro, M.; Saez-Francas, N.; Castro-Marrero, J.; Aliste, L.; Fernandez de Sevilla, T.; Alegre, J. Gender differences in chronic fatigue syndrome. Reumatol. Clin. 2016, 12, 72–77. [Google Scholar] [CrossRef]
- Lai, N.; Martis, A.; Belfiori, A.; Tolentino-Silva, F.; Nasca, M.M.; Strainic, J.; Cabrera, M.E. Gender differences in V O2 and HR kinetics at the onset of moderate and heavy exercise intensity in adolescents. Physiol. Rep. 2016, 4, e12970. [Google Scholar] [CrossRef]
- Van Campen, C.L.M.C.; Rowe, P.C.; Visser, F.C. Validity of 2-day cardiopulmonary exercise testing in male patients with myalgic encephalomyelities/chronic fatigue syndrome. Adv. Phys. Educ. 2020, 10, 68–80. [Google Scholar] [CrossRef][Green Version]
- Van Campen, C.L.M.; Visser, F.C. Validity of 2-day cardiopulmonary exercise testing in female patients with myalgic encephalomyelitis/chronic fatigue syndrome. Int. J. Curr. Res. 2020, 12, 10436–10442. [Google Scholar]
- Van Campen, C.L.; Rowe, P.C.; Visser, F.C. Two-Day Cardiopulmonary Exercise Testing in Females with a Severe Grade of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Comparison with Patients with Mild and Moderate Disease. Healthcare 2020, 8, 192. [Google Scholar] [CrossRef]
- Martina, J.R.; Westerhof, B.E.; van Goudoever, J.; de Beaumont, E.M.H.; Truijen, J.; Kim, Y.S.; van Lieshout, J.J. Noninvasive continuous arterial blood pressure monitoring with Nexfin(R). Anesthesiology 2012, 116, 1092–1103. [Google Scholar] [CrossRef] [PubMed]
- Mezzani, A. Cardiopulmonary Exercise Testing: Basics of Methodology and Measurements. Ann. Am. Thorac Soc. 2017, 14 (Suppl. 1), S3–S11. [Google Scholar] [CrossRef] [PubMed]
- Neuberg, G.W.; Friedman, S.H.; Weiss, M.B.; Herman, M.V. Cardiopulmonary exercise testing. The clinical value of gas exchange data. Arch. Intern. Med. 1988, 148, 2221–2226. [Google Scholar] [CrossRef] [PubMed]
- Beaver, W.L.; Wasserman, K.; Whipp, B.J. A new method for detecting anaerobic threshold by gas exchange. J. Appl. Physiol. 1986, 60, 2020–2027. [Google Scholar] [CrossRef]
- Sven, G.; Koch, B.; Ittermann, T.; Christoph, S.; Marcus, D.; Felix, S.B.; Hansen, J.E. Influence of age, sex, body size, smoking, and beta blockade on key gas exchange exercise parameters in an adult population. Eur. J. Cardiovasc. Prev. Rehabil. 2010, 17, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Parsaik, A.; Allison, T.G.; Singer, W.; Sletten, D.M.; Joyner, M.J.; Benarroch, E.E.; Sandroni, P. Deconditioning in patients with orthostatic intolerance. Neurology 2012, 79, 1435–1439. [Google Scholar] [CrossRef]
- Nijs, J.; de Meirleir, K.; Duquet, W. Kinesiophobia in chronic fatigue syndrome: Assessment and associations with disability. Arch. Phys. Med. Rehabil. 2004, 85, 1586–1592. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Female ME/CFS (n = 51) | Female ICF (n = 50) | p-Value | |
|---|---|---|---|
| Age (years) | 40 (9) | 40 (10) | 0.68 |
| Height (cm) | 169 (6) | 171 (7) | 0.20 |
| Weight (kg) | 68 (10) | 73 (14) | 0.04 |
| BMI (kg/m2) | 1.4 (0.2) | 1.4 (0.2) | 0.04 |
| BSA (m2) | 23.9 (3.3) | 25.1 (4.2) | 0.13 |
| Disease duration (years) | 13 (9) | 11 (7) | 0.13 |
| Disease severity grade ½ * | 29/22 (57/43%) | 36/14 (72/28%) | 0.11 |
| Fibromyalgia present * | 25 | 7 | <0.0005 |
| ME/CFS Females (n = 51) | ICF Females (n = 50) | |||||
|---|---|---|---|---|---|---|
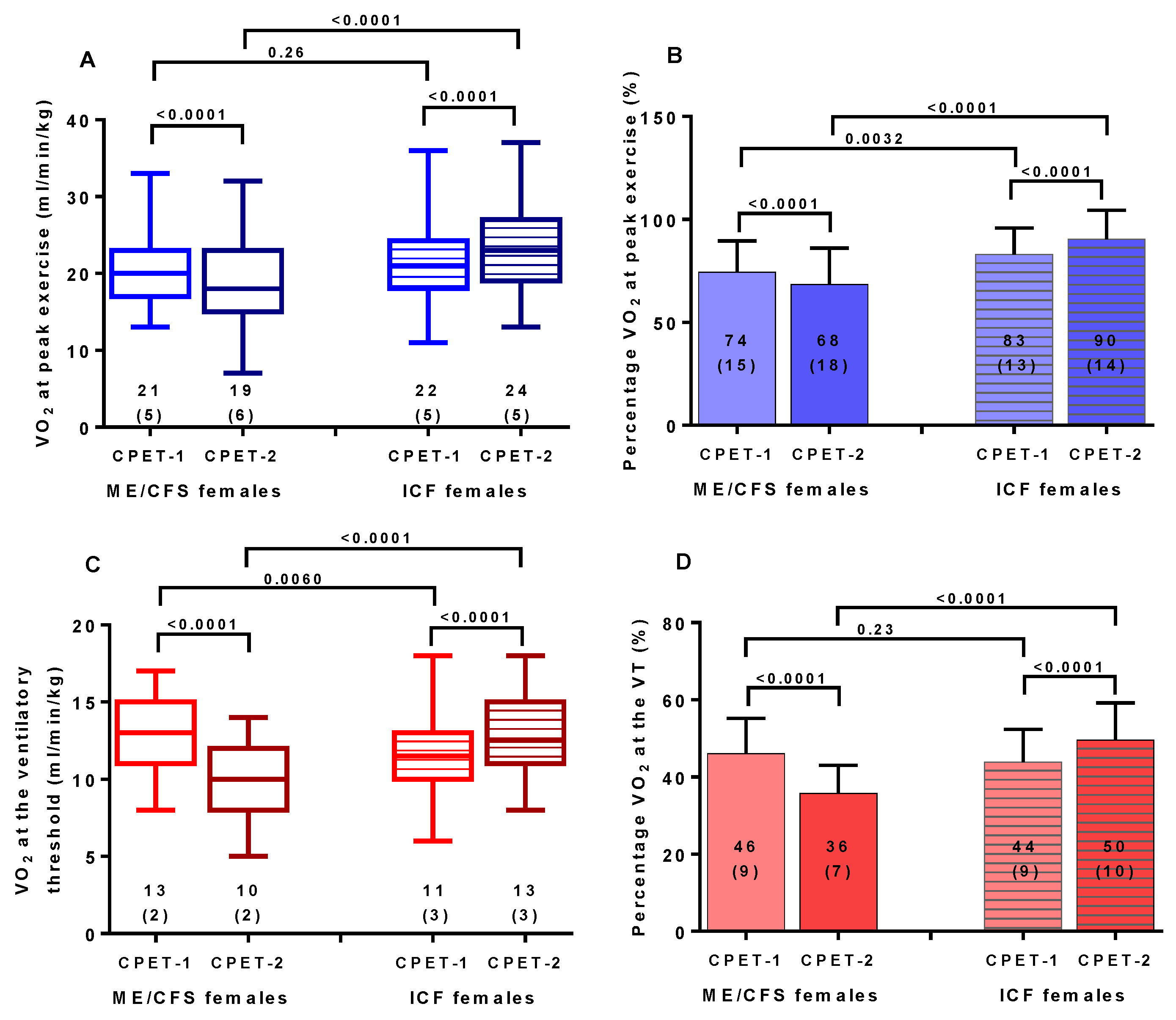
| Peak Exercise | CPET-1 | CPET-2 | p-Value | CPET-1 | CPET-2 | p-Value |
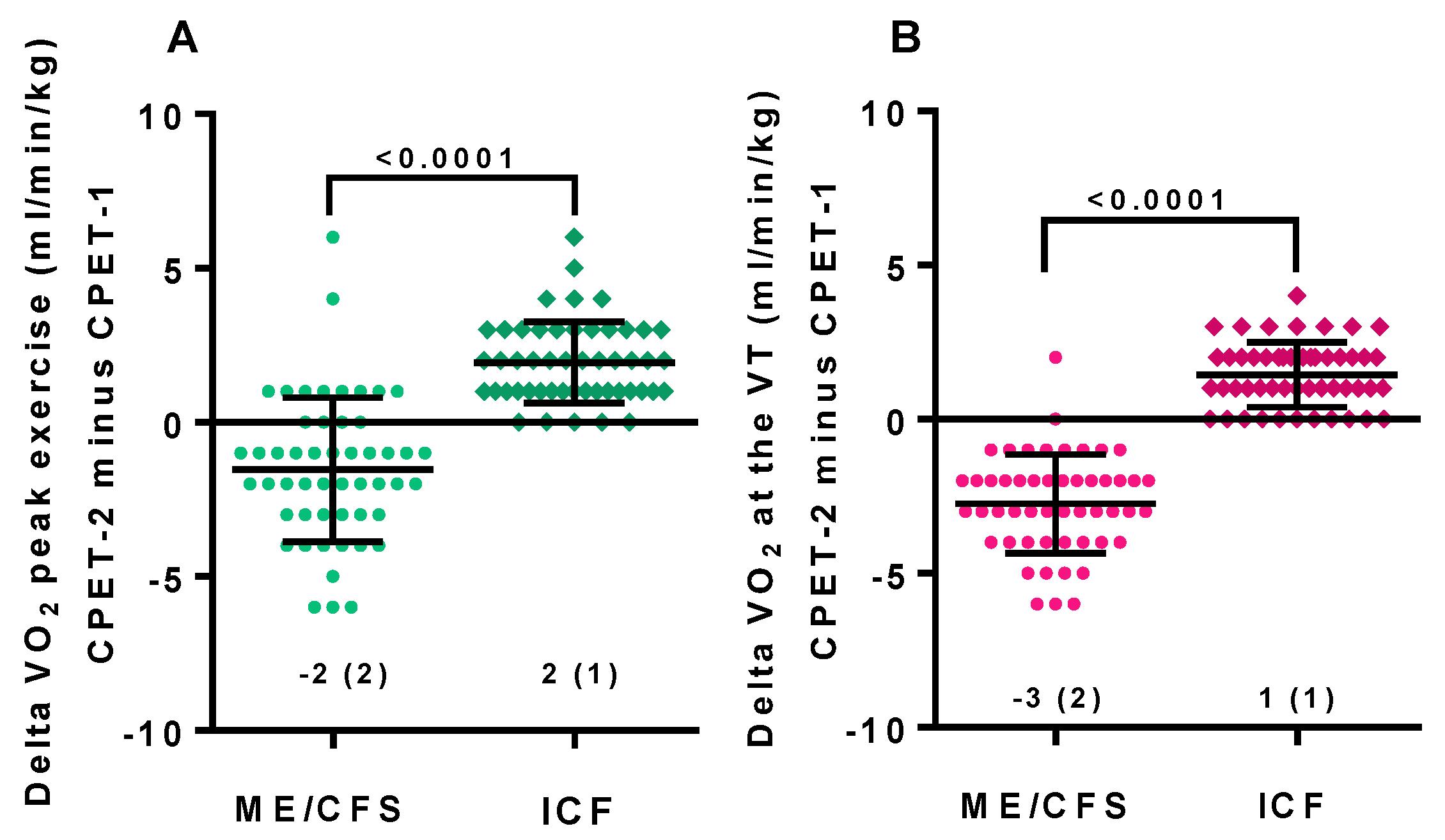
| VO2 peak (ml/min/kg) | 21 (5) | 19 (6) | < 0.0001 | 22 (5) | 24 (5) | < 0.0001 |
| %pred VO2 peak | 74 (15) | 68 (18) | < 0.0001 | 83 (13) | 90 (14) | < 0.0001 |
| HR rest (bpm) | 87 (11) | 87 (11) | 0.80 | 88 (13) | 88 (13) | 0.82 |
| HR peak (bpm) | 156 (17) | 149 (20) | < 0.0001 | 156 (18) | 162 (16) | < 0.0001 |
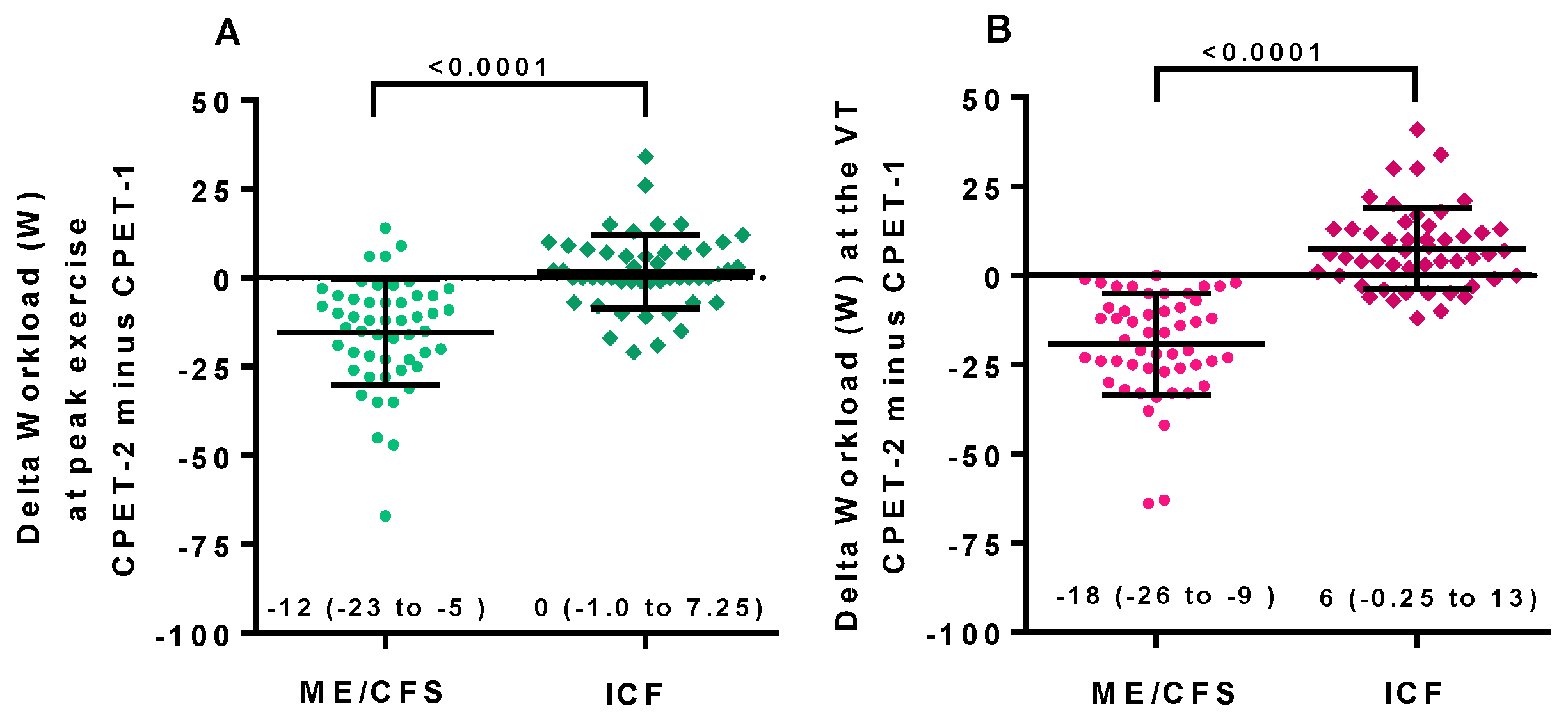
| Workload peak (watts) | 132 (24) | 117 (27) | < 0.0001 | 138 (31) | 140 (30) | 0.23 |
| RER peak | 1.1 (0.1) | 1.1 (0.1) | 0.03 | 1.2 (0.1) | 1.1 (0.1) | 0.80 |
| Ventilatory Threshold | CPET-1 | CPET-2 | p-Value | CPET-1 | CPET-2 | p-Value |
| VO2 VT (ml/min/kg) | 13 (2) | 10 (2) | < 0.0001 | 11 (2) | 13 (3) | < 0.0001 |
| %pred VO2 VT | 46 (9) | 36 (7) | < 0.0001 | 44 (8) | 50 (10) | < 0.0001 |
| HR VT (bpm) | 117 (13) | 106 (12) | < 0.0001 | 107 (14) | 113 (15) | < 0.0001 |
| Workload VT (watts) | 64 (19) | 45 (17) | < 0.0001 | 54 (17) | 62 (17) | < 0.0001 |
| CPET Day 1 | CPET Day 2 | |||||
|---|---|---|---|---|---|---|
| Peak Exercise | ME/CFS | ICF | p-Value | ME/CFS | ICF | p-Value |
| VO2 peak (ml/min/kg) | 21 (5) | 22 (5) | 0.26 | 19 (6) | 24 (5) | < 0.0001 |
| %pred VO2 peak | 74 (15) | 83 (13) | 0.003 | 68 (18) | 90 (14) | < 0.0001 |
| HR rest (bpm) | 87 (11) | 88 (13) | 0.62 | 87 (11) | 88 (13) | 0.60 |
| HR peak (bpm) | 156 (17) | 156 (18) | 0.89 | 149 (20) | 162 (16) | 0.0006 |
| Workload peak (watts) | 132 (24) | 138 (31) | 0.28 | 117 (27) | 140 (30) | 0.0001 |
| RER peak | 1.1 (0.1) | 1.2 (0.1) | 0.03 | 1.1 (0.1) | 1.2 (0.1) | 0.0005 |
| Ventilatory Threshold | ME/CFS | ICF | p-Value | CPET-1 | CPET-2 | p-Value |
| VO2 VT (ml/min/kg) | 13 (2) | 11 (2) | 0.006 | 10 (2) | 13 (3) | < 0.0001 |
| %pred VO2 VT | 46 (9) | 44 (8) | 0.23 | 36 (7) | 50 (10) | < 0.0001 |
| HR VT (bpm) | 117 (13) | 107 (14) | 0.0003 | 106 (12) | 113 (15) | 0.02 |
| ME/CFS Females (n = 51) | ICF Females (n = 50) | |||
|---|---|---|---|---|
| Peak Exercise | CPET-1 | CPET-2 | CPET-1 | CPET-2 |
| %pred VO2 peak ≥ 85% No deconditioning n= | 9 (22%) | 6 (16%) | 24 (48%) | 31 (66%) |
| %pred VO2 peak < 85% Moderate deconditioning n= | 40 (78%) | 43 (84%) | 26 (52%) | 17 (34%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Campen, C.M.C.; Visser, F.C. Female Patients with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome or Idiopathic Chronic Fatigue: Comparison of Responses to a Two-Day Cardiopulmonary Exercise Testing Protocol. Healthcare 2021, 9, 682. https://doi.org/10.3390/healthcare9060682
van Campen CMC, Visser FC. Female Patients with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome or Idiopathic Chronic Fatigue: Comparison of Responses to a Two-Day Cardiopulmonary Exercise Testing Protocol. Healthcare. 2021; 9(6):682. https://doi.org/10.3390/healthcare9060682
Chicago/Turabian Stylevan Campen, C. (Linda) M. C., and Frans C. Visser. 2021. "Female Patients with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome or Idiopathic Chronic Fatigue: Comparison of Responses to a Two-Day Cardiopulmonary Exercise Testing Protocol" Healthcare 9, no. 6: 682. https://doi.org/10.3390/healthcare9060682
APA Stylevan Campen, C. M. C., & Visser, F. C. (2021). Female Patients with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome or Idiopathic Chronic Fatigue: Comparison of Responses to a Two-Day Cardiopulmonary Exercise Testing Protocol. Healthcare, 9(6), 682. https://doi.org/10.3390/healthcare9060682