1. Introduction
The Jackson Heart Study (JHS) is a large, community-based study of 5301 African Americans residing in the tri-county area of Hinds, Madison and Rankin counties in Mississippi. It is very well documented that African Americans in Mississippi communities and the Jackson Heart Study are faced with ongoing health challenges and that there is a large disparity in cardiovascular mortality between Mississippi African Americans and Mississippi Whites or African Americans from other parts of the US [
1,
2]. To eliminate some of the disparities observed in the African American communities, committed academic-community collaborative and sustained research may be beneficial [
3]. Since little has changed in the health status of African Americans through the years, innovative methods and culturally appropriate interventions are needed [
4] to reverse the deprivation and disadvantage that are often characteristic of the social landscape for African Americans [
5,
6]. Many of these factors occurring at the individual and community levels have implications for development of chronic disease and long-term disability [
7,
8,
9].
The JHS Community Outreach Center (CORC) ascribes to a community-based participatory research (CBPR) approach that promotes the equitable involvement of partners in the entire research process, having a voice in the formulation of the project purpose and questions, outputs and outcomes, while contributing expertise, and sharing decision making and ownership [
10,
11]. For members of the JHS community, this arrangement promises to build community capacity as it enables them to become actively involved in the full range of JHS research-related activities. The principles of CBPR that are particularly important and relevant for the Jackson Heart Study are the following: (1) support for an approach that clearly illustrates cultural relevance in its activities where the JHS communities have the opportunity to define their health priorities and research agenda themselves; (2) willingness to operate in an environment that exudes mutual trust and respect where the JHS and its collaborating partners establish, develop, and openly cultivate respect and trust); (3) allocation of adequate and sustained resources needed for long-term health interventions that are readily made available; and (4) support for sustainable partnerships where there is an agreement for a long-term committed relationship between academic partners and the community partners [
10,
11,
12,
13]. The main JHS academic partner with the community is Jackson State University that was awarded a contract with the National Heart, Lung, and Blood Institute (NHLBI) of the National Institutes of Health (NIH) in 2013 to develop the Community Outreach Center (CORC). The JHS CORC is the first center developed within a national study by NHLBI that is dedicated exclusively to community outreach and engagement and operates under the auspices of the Jackson State University (JSU) School of Public Health. For the JHS CORC, community engagement and outreach includes providing avenues to reduce health disparities and engaging the community in health disparities discussions. Effective strategies can only be accomplished by convening ongoing academic-community discussion where community members can exchange ideas and be involved in the decisions that are made regarding strategies needed to address community concerns from the formative stages.
The JHS CORC has infused innovative strategies to engage the public and the scientific community in understanding the risks for development of CVD and accelerating interest in collaborative approaches to reducing the impact of CVD.
To be successful in adequately addressing the objective of community outreach and engagement, the JHS Community Outreach Center (CORC) at Jackson State University sought to, according to the principles of CBPR, create an environment of trust and long-term support of the JHS. This trust building mission was solidified by providing opportunities for substantive community involvement in all phases of the study development, conducting health promotion/education activities, and educating the community and study participants on the progress and processes of the JHS. The CORC staff emphasized that the success of this history-making medical research study depends on sustained involvement by the residents in the tri-county area of Hinds, Madison, and Rankin counties. This type of commitment is necessary to ensure that the academic-community union can effectively lay a strong foundation for establishing improved cardiovascular health within the African-American community [
14].
The information presented in this manuscript highlights the key procedures implemented by the JHS CORC to engage the community and the collaborative efforts that inspired the development of the academic-community partnerships. This paper highlights the operations and the actions that were implemented to sustain the Community Health Advisory Networks (CHAN) in all three JHS counties, (Hinds, Madison, and Rankin counties) under the premise that a successful academic-community partnership can increase participation in health education and health promotion activities, empowering community members to take an active role in improving their individual and community health status.
2. Methods
One key initial organizational strategy was a two-day Strategic Planning Retreat that was convened to create a vision of expected long-term change. The Strategic Planning Retreat was planned jointly by CHAN leaders and JHS CORC, and attended by selected representatives from the CHANs located in the three JHS counties -Hinds, Madison, and Rankin counties. The Strategic Planning Retreat was also attended by the members of the CORC staff. In deciding the process of engagement, several issues had to be resolved by the partners. They were: 1.identify the problem or the community needs, aligning all activities and decisions with CBPR principles; 2. decide on the expected outcome or the vision for the future; and 3. decide on a strategy for achieving the goals.
The final plan included creating the academic-community mission statement, a tagline, and the establishment of five CORC Working Groups charged with developing and implementing action plans, strategies, and steps to allocate resources to address the five specific aims of the CORC that were developed to fulfill the objectives of the JHS. The Working Groups were developed based on needs, suggestions, and input from the community partners, with the expectation that community members would continue to participate and provide input in the operations of the Working Groups that manage the operations of the CORC. The partners decided that the Mission Statement for the JHS CORC would be to foster a welcoming, respectful, and collaborative community-academic environment that promotes health equity through prevention, education, training, and research. This is a critical component of the CBPR principles. The group also decided on a tagline which is “Enriching CommUNITY one heart at a time”.
2.1. CORC Logic Models for Effective Academic-Community Partnerships
In order to effectively plan the program of activities and initiate the academic-community partners’ initiatives, it was decided that the CBPR principles and methodologies would be infused into CORC’s overall mission, activities, and evaluation. To ensure successful delivery of its objectives, CORC program administrators sought community input and developed an action plan and a roadmap with clear outcomes and explicit steps to implement an effective academic-community partnership. The result of these deliberations was the creation of a logic model. The plan of action was cultivated using the power of consensus and relying upon the group’s examination of the community’s values and beliefs. This process of collaboration facilitated the academic-community partners’ development of realistic expectations for the resources needed for operation, the visualization of the activities to be initiated, and the vision of changes or results expected to be achieved. A comprehensive logic model was developed to explain the relationships of these elements to the expected outcomes (see
Table 1). The intention of this logic model was to guide the overall scientific integrity of the academic-community partnership ensuring that knowledge acquired could be transferred into action that could influence individual and societal lifestyle, behavioral, and structural change [
15].
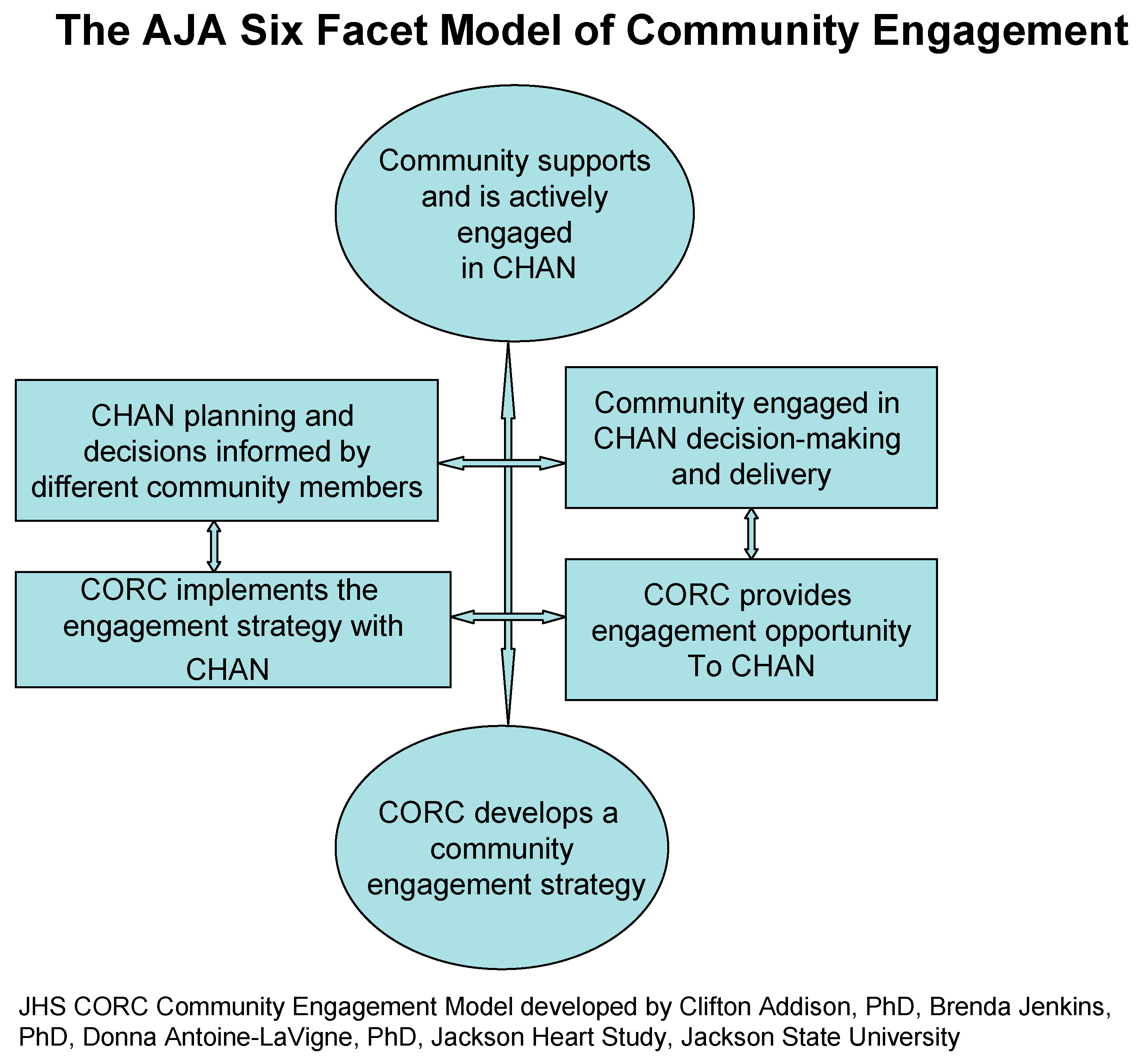
Prior to the development of the Logic Model, the academic-community continuing partnership was solidified with the development of a conceptual model for continuing engagement and outreach with the community partners. The collaboration and interaction between the CORC staff and the CHANs led to development of the Addison-Jenkins-Antoine-LaVigne (AJA) Six-Facet Model of Community Engagement. The AJA model's Six Types of Involvement (see
Figure 1) provides specific ideas on how the JHS CORC and community members can best impact community outreach, inspiring community members to participate in decision-making and leadership regarding health promotion and elimination of health disparities. The AJA model was developed by infusing experiences and ideas generated over a period of 13 years of community mobilizing/partnership-building that was the focus of the functions of the JHS Community Partnership Office (CPO). During the first contract period of the JHS (2000–2013), the CPO was infused into the operations of the JHS Coordinating Center and became recognized as a major force in the JHS cohort recruitment and retention efforts [
16,
17].
Table 1.
Community outreach center (CORC) logic model 1. Logic model: building institution and community partnership/commitment.
Table 1.
Community outreach center (CORC) logic model 1. Logic model: building institution and community partnership/commitment.
| SITUATION: Developing institutional and community commitment to CBPR through facilitating respect for the knowledge and expertise the community brings to the table. Outreach programs and activities are conducted and supported through the Jackson Heart Study (JHS) Community Outreach Center (CORC). The premise is that the community will support what it helps to create. |
|---|
| Priorities: Building and sustaining relationships with community partners |
|---|
| INPUTS: JHS CORC, NHLBI, Community Groups |
|---|
| Outputs | Outcomes-Impact |
|---|
| Activities | Participants | Short-Term | Medium-Term | Long Term |
|---|
| What we do | Who we reach | Learning changes | Indicators | Action changes | Indicators | Condition changes | Indicators |
|---|
Develop a model for assembling an effective community partnership
Sponsor seminars, forums, and conferences
Address barriers of distrust and cultural insensitivity
Disseminate health-related research findings to community-based primary care providers, community members
Enhance community health education and awareness using cardiovascular disease-related research training in health education
Design media messages and build capacity for community partners | African American scientists, health care providers and scholars
Faith and community-based organizations, and other grassroots organizations | Increase awareness, knowledge, and understanding about the JHS and the importance of African American participation
Accessibility to this information will further enhance the knowledge of the area providers | List of contacted potential partners
List of types of contacts made
Outline agreements reached
Completed program evaluation
List of media activities and training programs
List of capacity building activities | Attend JHS- sponsored activities
Clinic appointments are scheduled
Formation of a coalition, an organized body of diverse individuals, organizations and social and civic groups from Hinds, Madison and Rankin counties
JHS committee assignments
Implementation of Community Health Advisors Networks (CHAN)
leadership trainings, conferences/forums, focus groups, town hall meetings, health fairs | Attendance /Sign-in register
Documented list of coalition members
Compiled list of committees and assignments
List of established CHAN
List of trainings, conferences, meetings, health fairs | Sense of partnership and continued participation in JHS activities
Continuing participation in Community Partnership activities
Elimination of barriers of distrust and cultural insensitivity
Substantive community involvement in all phases of the study’s development and implementation
Receipt of the JHS newsletter | Transcripts from meetings
List of meetings/ appointments scheduled
Completion of evaluation instruments demonstrating change in attitudes, beliefs, practices, status
Indication of long-term improvements in health status
Indication of reduction of CVD risk behaviors,
Collecting and utilizing health care and public health material |
Figure 1.
Model to initiate community engagement.
Figure 1.
Model to initiate community engagement.
2.2. CORC Theoretical Model for Community Engagement (AJA Model)—JHS CORC Community Engagement Model (Developed by Clifton Addison, PhD; Brenda Jenkins, PhD; and Donna Antoine-LaVigne, PhD (Jackson Heart Study, School of Public Health, Jackson State University)
This model provided a pathway for effective academic-community partnerships and laid the foundation for effective program evaluation. According to the AJA Model, CORC is responsible for providing support to the JHS communities to develop the programs and activities that lead to the organization and management of the Community Health Advisory Networks. The AJA model outlines activities and roles for both the CORC staff and for the JHS CHAN. This is a system that encourages and supports full participatory community involvement efforts. The AJA model proposes that the partners create an official body within their respective communities with specific assignments to manage the day-to-day responsibilities. They operate with a definite plan of action, with clear objectives, roles, schedule of events, timelines, and deadlines.
2.3. CORC Evaluation
After infusing the Community-Based Participatory Research (CBPR) principles into the academic-community partnership’s mission, activities, and evaluation, it became necessary to generate practice-based evidence through analysis of the ongoing activities and practices of the partnership. Based on the sequence of activities generated through the logic model, an evaluation plan was developed to document the effectiveness of the activities. The Contact, Initiation, Acceptance, Success, and Continuation Evaluation Framework (CIASC) was developed to guide the evaluation of the CORC CHAN activities. CIASC represents the sequence of activities utilized by the academic-community partners to address the mission and objectives of the partners. The following are the components of the CIASC Evaluation Model, highlighting the areas of CORC CHAN activities that provide a framework for analyzing the partners’ ability and capacity to meet objectives.
CONTACT—Develop a framework/model and identify, contact, and interact with potential partners.
INITIATE (OUTREACH)—Introduction of CORC/Community planned activities and ensuring performance.
ACCEPTANCE (ADOPTION)—Recording partners’ acceptance of the model and agreement to participate and adopt plan of activities.
SUCCESS—Documenting results, value, and usefulness of activities.
CONTINUATION—commitment to sustainability of activities, long-term preservation of ideals developed.
3. Results
Given the need to increase CBPR in the JHS community, the use of CORC CHAN activities was an important community intervention vehicle. Utilizing CBPR principles was crucial for facilitating and encouraging community involvement in health promotion and created the platform for the community partners to work cooperatively to effect a reduction in health disparities and premature development of morbidity and mortality. The JHS CORC has promoted and supported the JHS community's involvement by modeling CBPR, co-participating in health promotion/health education activities, encouraging or prompting health promotion, and providing support. Through the CHAN mechanism, CORC staff, in collaboration with the community partners, has promoted a model of effective academic-community-family-partnerships, through which CORC can maintain contact, continue to build relationships, communicate awareness, and provide support, while serving as a valuable resource for JHS community members. CORC has endorsed, identified, and introduced opportunities for the CHAs to become more involved in the conduct of research. The interaction and collaboration between the JHS CORC and the CHAN have paved the way for a new community interest in research activities.
4. Discussion
The impetus for forming the academic-community collaborative partnership emanated from a small group of community members seeking answers for a particular problem-the well documented cardiovascular disease and obesity prevalence among African Americans in Mississippi. CORC and the CHAN aspired to build a culture of health by working together. The accomplishments described by the Jackson Heart Study (JHS) Community Outreach Center (CORC) is a testament that community commitment is more than an expression, a thought, or an idea. In true CBPR fashion, CORC began this collaboration with the expectation that the academic-community partnership would result in real action that involves active planning and participation by our community partners. The Strategic Planning Retreat and subsequent collaborations between CORC and its community partners illustrated that the partners became engaged in real activities where CORC provided resources and services to the community where needed. CORC’s goal is to continue to inspire, motivate, and facilitate community involvement in research, health education, and health promotion to fulfill its goal to empower the local communities through a wide array of education and information initiatives.
CORC’s goal is to improve health status by working closely with the CHAN in the three counties of Hinds, Madison, and Rankin to foster research, mentoring, teaching, service, outreach, capacity-building, and leadership. In order to reduce health disparities, there must be a long-term commitment to transform the traditional academic/researcher/community relationship into a more collaborative partnership where community partners can be respected and their input and contributions solicited, valued, adopted, and utilized. It is evident that health disparities affect the daily lives and experiences of individuals and families, and that negative impact can certainly affect entire communities in the long run. Elevating the CHAN contributions regarding elimination of risk factors and health disparities from being simply a consumer of information to one of equal partner leading the way and contributing to developing solutions can help to expedite the discovery of meaningful alternatives that ordinarily would be kept in obscurity.
5. Conclusions
The purpose of this study was to highlight the impact of the multilevel strategies employed by the JHS CORC to build trust and capacity within an academic-community partnership, a primary feature of the JHS, the largest investigation of causes of CVD in an African-American population. The key components of the JHS CORC’s strategies underscored in this study exemplify multilevel strategies that are interrelated and linked to the major CBPR concepts. One such component is the theoretical model AJA Six-Facet Model of Community Engagement that builds the foundation for developing continuing engagement, outreach, and collaboration with the community partners. Another key component is the implementation of a logic model to guide the overall scientific integrity of the academic-community partnership ensuring that knowledge acquired could lead to action that could inspire lifestyle, behavioral, and structural change on an individual basis, as well as community-wide.
The AJA model and the logic model developed can stimulate community-engaged research and community outreach for the purpose of health education and health promotion because they are designed to facilitate long term sustainability and increased capacity of the CHANs so that they can share knowledge with other CHANs and other community members empowering them to do the work themselves. Future studies that aspire to reduce health disparities and adverse health in the at-risk populations, such as African American or other minority participants, can benefit from the strategies observed in the community engagement and outreach efforts of the JHS since these strategies and approaches have contributed to the successes and durability of the JHS research endeavors.
The strategies utilized by the JHS CORC can be used as a basis for rethinking community outreach and engagement, particularly in hard to reach populations, such as minority and rural populations. The JHS CORC utilizes its resources and intellectual capital to build research capacity to protect the community’s health and environment, while at the same time promoting policy building/policy changing capacity. The JHS CORC is increasing capacity among the CHANs and their communities to facilitate a community wide assault on risk factors for development of cardiovascular and other chronic diseases as well as negative behavior practices. The rich collaborations that have ensued through this fully engaged academic-community partnerships can facilitate action and policy change where needed, as Mississippi struggles to combat the unequal burden of the prevalence of obesity and cardiovascular diseases. The strategies described in this account serve as an example of how multilevel strategies targeting, high risk, vulnerable populations and communities can be implemented to begin the process of reversing the epidemic of CVD in African Americans.


 ,
, 

{kind=link}
