Childhood Obesity Prevention in Africa: A Systematic Review of Intervention Effectiveness and Implementation

 , and
, and
Abstract
1. Introduction
- What behaviours have been addressed in past interventions?
- What age groups and settings have the interventions targeted?
- What levels of the social ecological model are the interventions situated within?
- How do these aforementioned characteristics relate to effectiveness of interventions?
- What barriers and facilitators to implementation or effectiveness have been identified in existing studies?
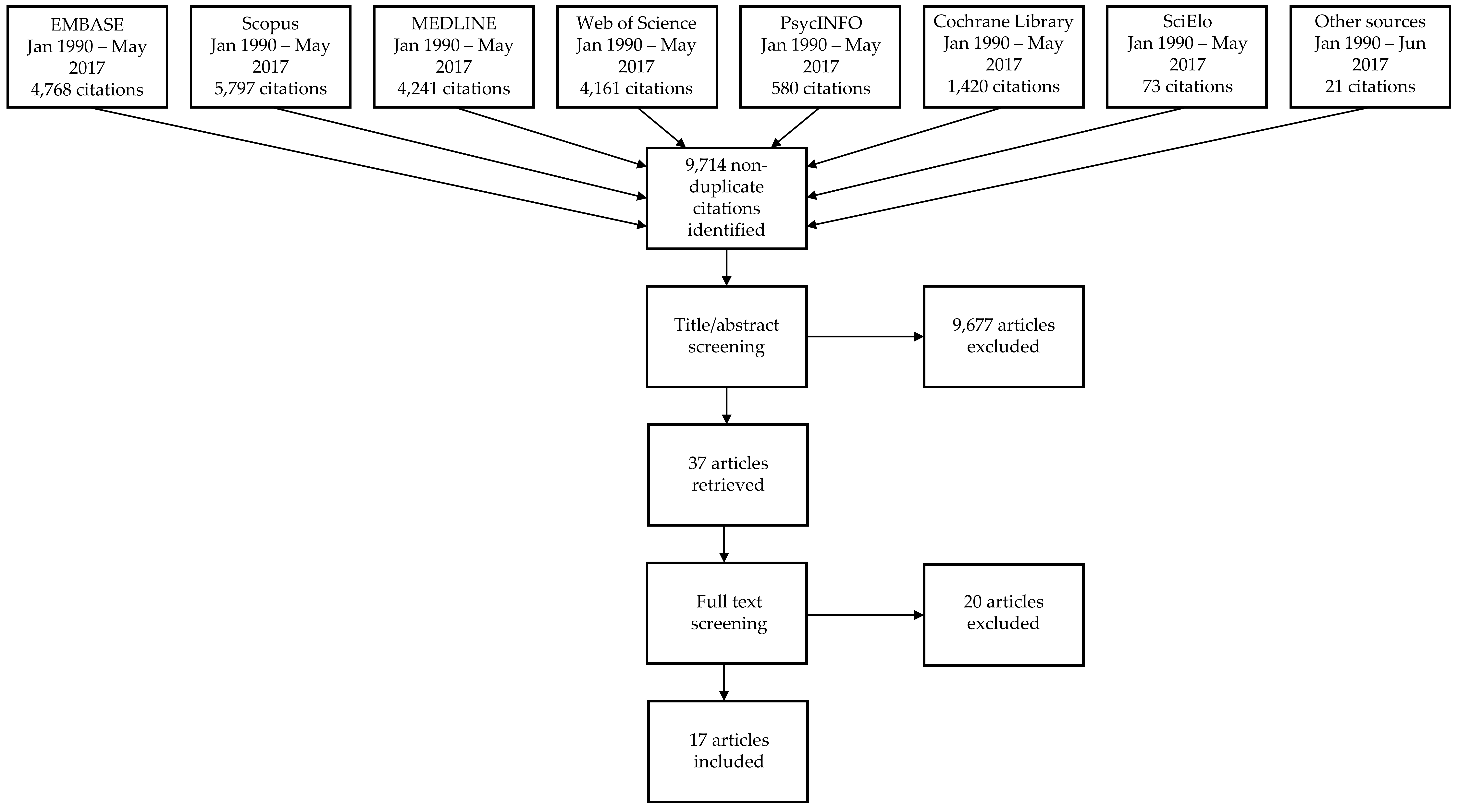
2. Materials and Methods
3. Results
3.1. Design and Quality of Included Interventions
3.2. Targeted Settings, Age Groups and Behaviours
3.3. Outcome Measures
3.4. Intervention Characteristics and Levels of the Social Ecological Model
3.5. Effectiveness
3.6. Implementation Barriers and Facilitators
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Abarca-Gómez, L.; Abdeen, Z.A.; Hamid, Z.A.; Abu-Rmeileh, N.M.; Acosta-Cazares, B.; Acuin, C.; Adams, R.J.; Aekplakorn, W.; Afsana, K.; Aguilar-Salinas, C.A.; et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef]
- WHO. Consideration of the Evidence on Childhood Obesity for the Commission on Ending Childhood Obesity; WHO Press: Geneva, Switzerland, 2016; Available online: http://apps.who.int/iris/bitstream/handle/10665/206549/9789241565332_eng.pdf?sequence=1&isAllowed=y (accessed on 19 June 2018).
- Lundeen, E.A.; Norris, S.A.; Adair, L.S.; Richter, L.M.; Stein, A.D. Sex differences in obesity incidence: 20-year prospective cohort in South Africa. Pediatr. Obes. 2015, 11, 75–80. [Google Scholar] [CrossRef]
- Monyeki, K.D.; Monyeki, M.A.; Brits, S.J.; Kemper, H.C.; Makgae, P.J. Development and tracking of body mass index from preschool age into adolescence in rural South African children: Ellisras Longitudinal Growth and Health Study. J. Health Popul. Nutr. 2008, 26, 405–417. [Google Scholar] [CrossRef]
- Singh, A.S.; Mulder, C.; Twisk, J.W.R.; Van Mechelen, W.; Chinapaw, M.J.M. Tracking of childhood overweight into adulthood: A systematic review of the literature. Obes. Rev. 2008, 9, 474–488. [Google Scholar] [CrossRef] [PubMed]
- Reilly, J.J.; Kelly, J. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: Systematic review. Int. J. Obes. 2011, 35, 891–898. [Google Scholar] [CrossRef]
- Park, M.H.; Falconer, C.; Viner, R.M.; Kinra, S. The impact of childhood obesity on morbidity and mortality in adulthood: A systematic review. Obes. Rev. 2012, 13, 985–1000. [Google Scholar] [CrossRef] [PubMed]
- Quek, Y.-H.; Tam, W.W.S.; Zhang, M.W.B.; Ho, R.C.M. Exploring the association between childhood and adolescent obesity and depression: A meta-analysis. Obes. Rev. 2017, 18, 742–754. [Google Scholar] [CrossRef] [PubMed]
- Caird, J.; Kavanagh, J.; O’Mara-Eves, A.; Oliver, K.; Oliver, S.; Stansfield, C.; Thomas, J. Does being overweight impede academic attainment? A systematic review. Health Educ. J. 2014, 73, 497–521. [Google Scholar] [CrossRef]
- UNICEF-WHO-The World Bank Group. Joint Child Malnutrition Estimates—Levels and Trends, 2018 ed.; World Health Organization: Geneva, Switzerland, 2018; Available online: http://www.who.int/nutgrowthdb/estimates2017/en/ (accessed on 17 May 2018).
- Popkin, B.M. The nutrition transition: An overview of world patterns of change. Nutr. Rev. 2004, 62, S140–S143. [Google Scholar] [CrossRef] [PubMed]
- Manyanga, T.; Barnes, J.D.; Abdeta, C.; Adeniyi, A.F.; Bhawra, J.; Draper, C.E.; Katapally, T.R.; Khan, A.; Lambert, E.; Makaza, D. Indicators of Physical Activity Among Children and Youth in 9 Countries with Low to Medium Human Development Indices: A Global Matrix 3.0 Paper. J. Phys. Activity Health 2018, 15 (Suppl. 2), S274–S283. [Google Scholar] [CrossRef]
- Vorster, H.H.; Kruger, A.; Margetts, B.M. The nutrition transition in Africa: Can it be steered into a more positive direction? Nutrients 2011, 3, 429–441. [Google Scholar] [CrossRef] [PubMed]
- Muthuri, S.K.; Francis, C.E.; Wachira, L.J.; LeBlanc, A.G.; Sampson, M.; Onywera, V.O.; Tremblay, M.S. Evidence of an Overweight/Obesity Transition among School-Aged Children and Youth in Sub-Saharan Africa: A Systematic Review. PLoS ONE 2014, 9, e92846. [Google Scholar] [CrossRef]
- Monyeki, M.; Awotidebe, A.; Strydom, G.; de Ridder, J.; Mamabolo, R.; Kemper, H. The Challenges of Underweight and Overweight in South African Children: Are We Winning or Losing the Battle? A Systematic Review. Int. J. Environ. Res. Public Health 2015, 12, 1156–1173. [Google Scholar] [CrossRef]
- Verstraeten, R.; Roberfroid, D.; Lachat, C.; Leroy, J.L.; Holdsworth, M.; Maes, L.; Kolsteren, P.W. Effectiveness of preventive school-based obesity interventions in low- and middle-income countries: A systematic review. Am. J. Clin. Nutr. 2012, 96, 415–438. [Google Scholar] [CrossRef] [PubMed]
- Barbosa Filho, V.C.; Minatto, G.; Mota, J.; Silva, K.S.; de Campos, W.; da Silva Lopes, A. Promoting physical activity for children and adolescents in low- and middle-income countries: An umbrella systematic review: A review on promoting physical activity in LMIC. Prev. Med. 2016, 88, 115–126. [Google Scholar] [CrossRef]
- Fruhstorfer, B.H.; Mousoulis, C.; Uthman, O.A.; Robertson, W. Socio-economic status and overweight or obesity among school-age children in sub-Saharan Africa—A systematic review. Clin. Obes. 2016, 6, 19–32. [Google Scholar] [CrossRef]
- Wang, Y.; Cai, L.; Wu, Y.; Wilson, R.F.; Weston, C.; Fawole, O.; Bleich, S.N.; Cheskin, L.J.; Showell, N.N.; Lau, B.D.; et al. What childhood obesity prevention programmes work? A systematic review and meta-analysis. Obes. Rev. 2015, 16, 547–565. [Google Scholar] [CrossRef] [PubMed]
- Bleich, S.N.; Vercammen, K.A.; Zatz, L.Y.; Frelier, J.M.; Ebbeling, C.B.; Peeters, A. Interventions to prevent global childhood overweight and obesity: A systematic review. Lancet Diabetes Endocrinol. 2018, 6, 332–346. [Google Scholar] [CrossRef]
- Waters, E.; de Silva-Sanigorski, A.; Burford, B.J.; Brown, T.; Campbell, K.J.; Gao, Y.; Armstrong, R.; Prosser, L.; Summerbell, C.D. Interventions for preventing obesity in children. Cochrane Database Syst Rev. 2011. [Google Scholar] [CrossRef]
- Muthuri, S.; Wachira, L.J.; Leblanc, A.; Francis, C.; Sampson, M.; Onywera, V.; Tremblay, M. Temporal Trends and Correlates of Physical Activity, Sedentary Behaviour, and Physical Fitness among School-Aged Children in Sub-Saharan Africa: A Systematic Review. Int. J. Environ. Res. Public Health 2014, 11, 3327–3359. [Google Scholar] [CrossRef] [PubMed]
- Micklesfield, L.K.; Pedro, T.M.; Kahn, K.; Kinsman, J.; Pettifor, J.M.; Tollman, S.; Norris, S.A. Physical Activity and Sedentary Behavior among Adolescents in Rural South Africa: Levels, Patterns and Correlates. BMC Public Health 2014, 14, 40. [Google Scholar] [CrossRef]
- Bauman, A.E.; Reis, R.S.; Sallis, J.F.; Wells, J.C.; Loos, R.J.; Martin, B.W. Correlates of physical activity: Why are some people physically active and others not? Lancet (Lond. Engl.) 2012, 380, 258–271. [Google Scholar] [CrossRef]
- Temple, N.J.; Steyn, N.P. The cost of a healthy diet: A South African perspective. Nutrition 2011, 27, 505–508. [Google Scholar] [CrossRef] [PubMed]
- Temple, N.J.; Steyn, N.P.; Fourie, J.; De Villiers, A. Price and availability of healthy food: A study in rural South Africa. Nutrition 2011, 27, 55–58. [Google Scholar] [CrossRef] [PubMed]
- Draper, C.E.; Davidowitz, K.J.; Goedecke, J.H. Perceptions relating to body size, weight loss and weight-loss interventions in black South African women: A qualitative study. Public Health Nutr. 2016, 19, 548–556. [Google Scholar] [CrossRef] [PubMed]
- Sedibe, M.; Griffiths, P.; Doak, C.; Feeley, A.; Voorend, C.; Norris, S. Narratives of urban female adolescents in South Africa: Dietary and physical activity practices in an obesogenic environment. S. Afr. J. Clin. Nutr. 2014, 27, 114–119. [Google Scholar] [CrossRef]
- Puoane, T.; Tsolekile, L.; Steyn, N. Perceptions about body image and sizes among black African girls living in Cape Town. Ethn. Dis. 2010, 20, 29–34. [Google Scholar] [PubMed]
- Phillips, E.A.; Comeau, D.L.; Pisa, P.T.; Stein, A.D.; Norris, S.A. Perceptions of diet, physical activity, and obesity-related health among black daughter-mother pairs in Soweto, South Africa: A qualitative study. BMC Public Health 2016, 16, 750. [Google Scholar] [CrossRef] [PubMed]
- Maatoug, J.; Fredj, S.B.; Msakni, Z.; Dendana, E.; Sahli, J.; Harrabi, I.; Chouikha, F.; Boughamoura, L.; Slama, S.; Farpour-Lambert, N. Challenges and results of a school-based intervention to manage excess weight among school children in Tunisia 2012–2014. Int. J. Adolesc. Med. Health 2017, 29. [Google Scholar] [CrossRef] [PubMed]
- Draper, C.E.; de Villiers, A.; Lambert, E.V.; Fourie, J.; Hill, J.; Dalais, L.; Abrahams, Z.; Steyn, N. HealthKick: A nutrition and physical activity intervention for primary schools in low-income settings. BMC Public Health 2010, 10, 398. [Google Scholar] [CrossRef] [PubMed]
- De Villiers, A.; Steyn, N.P.; Draper, C.E.; Fourie, J.M.; Barkhuizen, G.; Lombard, C.J.; Dalais, L.; Abrahams, Z.; Lambert, E.V. “HealthKick”: Formative assessment of the health environment in low-resource primary schools in the Western Cape Province of South Africa. BMC Public Health 2012, 12, 794. [Google Scholar] [CrossRef] [PubMed]
- Kinsman, J.; Norris, S.A.; Kahn, K.; Twine, R.; Riggle, K.; Edin, K.; Mathebula, J.; Ngobeni, S.; Monareng, N.; Micklesfield, L.K. A model for promoting physical activity among rural South African adolescent girls. Glob. Health Action 2015, 8, 28790. [Google Scholar] [CrossRef] [PubMed]
- Golden, S.D.; Earp, J.A.L. Social Ecological Approaches to Individuals and Their Contexts. Health Educ. Behav. 2012, 39, 364–372. [Google Scholar] [CrossRef]
- Rycroft-Malone, J.; McCormack, B.; Hutchinson, A.M.; DeCorby, K.; Bucknall, T.K.; Kent, B.; Schultz, A.; Snelgrove-Clarke, E.; Stetler, C.B.; Titler, M. Realist synthesis: Illustrating the method for implementation research. Implement. Sci. 2012, 7, 33. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- (NCD-RisC) NRFC. Trends in adult body-mass index in 200 countries from 1975 to 2014: A pooled analysis of 1698 population-based measurement studies with 19·2 million participants. Lancet 2016, 387, 1377–1396. [Google Scholar] [CrossRef]
- Hesketh, K.R.; O’Malley, C.; Paes, V.M.; Moore, H.; Summerbell, C.; Ong, K.K.; Lakshman, R.; van Sluijs, E.M. Determinants of Change in Physical Activity in Children 0–6 years of Age: A Systematic Review of Quantitative Literature. Sport Med. 2017, 47, 1349–1374. [Google Scholar] [CrossRef] [PubMed]
- Hinkley, T.; Crawford, D.; Salmon, J.; Okely, A.D.; Hesketh, K. Preschool Children and Physical Activity: A Review of Correlates. Am. J. Prev. Med. 2008, 34, 435–441. [Google Scholar] [CrossRef]
- Trost, S.G.; Owen, N.; Bauman, A.E.; Sallis, J.F.; Brown, W. Correlates of adults’ participation in physical activity: Review and update. Med. Sci. Sports Exerc. 2002, 34, 1996–2001. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Prochaska, J.J.; Taylor, W.C. A review of correlates of physical activity of children and adolescents. Med. Sci. Sports Exerc. 2000, 32, 963–975. [Google Scholar] [CrossRef]
- Effective Public Health Practice Project. Quality Assessment Tool for Quantitative Studies. Published 2009. Available online: https://merst.ca/ephpp/ (accessed on 3 March 2017).
- The World Bank. Sub-Saharan Africa. Published 2016. Available online: http://data.worldbank.org/region/sub-saharan-africa (accessed on 3 March 2017).
- The World Bank. Middle East & North Africa. Published 2017. Available online: http://data.worldbank.org/region/middle-east-and-north-africa?view=chart (accessed on 25 March 2017).
- Steyn, N.P.; de Villiers, A.; Gwebushe, N.; Draper, C.E.; Hill, J.; de Waal, M.; Dalais, L.; Abrahams, Z.; Lombard, C.; Lambert, E.V. Did HealthKick, a randomised controlled trial primary school nutrition intervention improve dietary quality of children in low-income settings in South Africa? BMC Public Health 2015, 15, 948. [Google Scholar] [CrossRef]
- Uys, M.; Draper, C.E.; Hendricks, S.; de Villiers, A.; Fourie, J.; Steyn, N.P. Impact of a South African School-based Intervention, HealthKick, on Fitness Correlates. Am. J. Health Behav. 2016, 40, 55–66. [Google Scholar] [CrossRef]
- Harrabi, I.; Maatoug, J.; Gaha, M.; Kebaili, R.; Gaha, R.; Ghannem, H. School-based intervention to promote healthy lifestyles in Sousse, Tunisia. Indian J. Community Med. 2010, 35, 94–99. [Google Scholar] [CrossRef]
- Jemmott, J.B., III; Jemmott, L.S.; O’Leary, A.; Ngwane, Z.; Icard, L.; Bellamy, S.; Jones, S.; Landis, J.R.; Heeren, G.A.; Tyler, J.C. Cognitive-behavioural health-promotion intervention increases fruit and vegetable consumption and physical activity among South African adolescents: A cluster-randomised controlled trial. Psychol. Health 2011, 26, 167–185. [Google Scholar] [CrossRef] [PubMed]
- Hill, J.; Draper, C.E.; De Villiers, A.; Fourie, J.M.; Mohamed, S.; Steyn, N. Promoting healthy lifestyle behaviour through the Life-Orientation curriculum: Teachers’ perceptions of the HealthKick intervention. S. Afr. J. Educ. 2015, 35, 1–9. [Google Scholar] [CrossRef]
- De Villiers, A.; Steyn, N.P.; Draper, C.E.; Hill, J.; Dalais, L.; Fourie, J.; Lombard, C.; Barkhuizen, G.; Lambert, E.V. Implementation of the HealthKick intervention in primary schools in low-income settings in the Western Cape Province, South Africa: A process evaluation. BMC Public Health 2015, 15, 818. [Google Scholar] [CrossRef] [PubMed]
- Hochfeld, T.; Graham, L.; Patel, L.; Moodley, J.; Ross, E. Does school breakfast make a difference? An evaluation of an in-school breakfast programme in South Africa. Int. J. Educ. Dev. 2016, 51, 1–9. [Google Scholar] [CrossRef]
- Draper, C.E.; De Kock, L.; Grimsrud, A.T.; Rudolph, M.; Nemutandani, S.; Kolbe-Alexander, T.; Lambert, E.V. Evaluation of a school-based physical activity intervention in Alexandra Township. S. Afr. J. Sports Med. 2010, 22, 12–19. [Google Scholar] [CrossRef]
- Nyawose, S.E.; Naidoo, R. The impact of a school-based and family physical activity intervention on learners’ health behaviour. Afr. J. Phys. Activity Health Sci. 2016, 22, 378–393. [Google Scholar]
- Naidoo, R.; Coopoo, Y. The impact of a primary school physical activity intervention in KwaZulu-Natal, South Africa. Afr. J. Phys. Health Educ. Recreat. Dance 2012, 18, 75–85. [Google Scholar]
- Walter, C. Promoting physical activity: A low cost intervention programme for disadvantaged schools in Port Elizabeth, South Africa. Afr. J. Phys. Health Educ. Recreat. Dance 2014, 20, 357–371. [Google Scholar]
- Richards, J.; Foster, C. Sport-for-Development Interventions: Whom Do They Reach and What Is Their Potential for Impact on Physical and Mental Health in Low-Income Countries? Afr. J. Phys. Activity Health 2013, 10, 929–931. [Google Scholar] [CrossRef]
- Jemmott, L.S.; Jemmott, J.B., 3rd; Ngwane, Z.; Icard, L.; O’leary, A.; Gueits, L.; Brawner, B. “Let Us Protect Our Future” a culturally congruent evidenced-based HIV/STD risk-reduction intervention for young South African adolescents. Health Educ. Res. 2014, 29, 166–181. [Google Scholar] [CrossRef] [PubMed]
- Maatoug, J.; Hmad, S.; Bhiri, S.; Nawel, Z.; Imed, H.; Lamia, B.; Hassen, G. Effects of a kindergarten-based intervention to promote healthy lifestyles: Quasi experimental study in Sousse, Tunisia. Clin. Res. Trials 2015, 1, 38–43. [Google Scholar]
- Maatoug, J.; Msakni, Z.; Zammit, N.; Bhiri, S.; Harrabi, I.; Boughammoura, L.; Slama, S.; Larbi, C.; Ghannem, H. School-based intervention as a component of a comprehensive community program for overweight and obesity prevention, Sousse, Tunisia, 2009–2014. Prev. Chronic Dis. 2015, 12, E160. [Google Scholar] [CrossRef] [PubMed]
- Lennox, A.; Pienaar, A. Effects of an after-school physical activity programme on aerobic fitness and physical activity levels of adolescents from a disadvantaged community: PLAY Study. Afr. J. Phys. Health Educ. Recreat. Dance 2013, 19, 154–168. [Google Scholar]
- Naidoo, R.; Coopoo, Y.; Lambert, E.; Draper, C. Impact of a primary school-based nutrition and physical activity intervention on learners in KwaZulu-Natal, South Africa: A pilot study. S. Afr. J. Sports Med. 2009, 21. [Google Scholar] [CrossRef]
- Richards, J.; Foster, C.; Townsend, N.; Bauman, A. Physical fitness and mental health impact of a sport-for-development intervention in a post-conflict setting: Randomised controlled trial nested within an observational study of adolescents in Gulu, Uganda. BMC Public Health 2014, 14, 619. [Google Scholar] [CrossRef] [PubMed]
- De Villiers, A.; Steyn, N.P.; Draper, C.E.; Hill, J.; Gwebushe, N.; Lambert, E.V.; Lombard, C. Primary school children’s nutrition knowledge, self-efficacy, and behavior, after a three-year healthy lifestyle intervention (HealthKick). Ethn. Dis. 2016, 26, 171–180. [Google Scholar] [CrossRef]
- Kebaili, R.; Harrabi, I.; Maatoug, J.; Ghammam, R.; Slim, S.; Ghannem, H. School-based intervention to promote healthy nutrition in Sousse, Tunisia. Int. J. Adolesc. Med. Health 2014, 26, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Naude, D.; Kruger, H.; Pienaar, A.; Mamabol, R. Body fat, body mass index in black South African adolescents after a physical activity intervention programme: PLAY study. Afr. J. Phys. Health Educ. Recreat. Dance 2008, 14, 440–455. [Google Scholar] [CrossRef]
- World Health Organization. Global Nutrition Monitoring Framework Country Profile: Tunisia. Published 2019. Available online: http://apps.who.int/nutrition/landscape/global-monitoring-framework?ISO=tun (accessed on 22 March 2019).
- World Health Organization. Global Nutrition Monitoring Framework Country Profile: South Africa. Published 2019. Available online: http://apps.who.int/nutrition/landscape/global-monitoring-framework?ISO=ZAF (accessed on 22 March 2019).
- World Health Organization. Global Nutrition Monitoring Framework Country Profile: Uganda. Published 2019. Available online: http://apps.who.int/nutrition/landscape/global-monitoring-framework?ISO=UGA (accessed on 22 March 2019).
- Institute for Health Metrics and Evaluation. Country profile: Tunisia. Published 2017. Available online: http://www.healthdata.org/tunisia (accessed on 22 March 2019).
- Institute for Health Metrics and Evaluation. Country profile: South Africa. Published 2017. Available online: http://www.healthdata.org/south-africa (accessed on 22 March 2019).
- Institute for Health Metrics and Evaluation. Country Profile: Uganda. Published 2017. Available online: http://www.healthdata.org/uganda (accessed on 22 March 2019).
- Sweet, S.N.; Fortier, M.S.; Sweet, S.N.; Fortier, M.S. Improving Physical Activity and Dietary Behaviours with Single or Multiple Health Behaviour Interventions? A Synthesis of Meta-Analyses and Reviews. Int. J. Environ. Res. Public Health 2010, 7, 1720–1743. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Owen, N.; Fotheringham, M.J. Behavioral epidemiology: A systematic framework to classify phases of research on health promotion and disease prevention. Ann. Behav. Med. 2000, 22, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. Int. J. Nurs. Stud. 2013, 50, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Moore, G.F.; Audrey, S.; Barker, M.; Bond, L.; Bonell, C.; Hardeman, W.; Moore, L.; O’Cathain, A.; Tinati, T.; Wight, D. Process evaluation of complex interventions: Medical Research Council guidance. BMJ 2015, 350, h1258. [Google Scholar] [CrossRef] [PubMed]
- Grant, A.; Treweek, S.; Dreischulte, T.; Foy, R.; Guthrie, B. Process evaluations for cluster-randomised trials of complex interventions: A proposed framework for design and reporting. Trials 2013, 14, 15. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Included Studies | Excluded Studies | |
|---|---|---|
| Population | Generally healthy, typically developing children and adolescents ages 2–18 years residing in African countries | Studies targeting children and adolescents with specific disease or condition, including asthma, diabetes, and obesity |
| Normal or mixed weight populations | African populations residing outside of Africa | |
| Intervention | Any behavioural (including but not limited to) physical activity- or diet-related interventions aimed at preventing overweight and obesity (even if not explicitly stated) among children in any context (home, community, school, etc.) | Obesity treatment interventions, malnutrition prevention interventions targeting undernutrition, non-behavioural interventions |
| Study design | Primary research question: Randomised or non-randomised controlled trials (cluster or individual), controlled pre-post studies, prospective cohort studies with a control group, interrupted time series and repeated measure studies, quasi-experimental studies and natural experiments | Cross-sectional studies, non-experimental studies, non-human studies, laboratory-based studies |
| Sub-questions: Any design, including qualitative studies, as long as they are describing the same studies as those selected for answering the primary research question of the review | N/A | |
| Outcomes | Primary outcomes: Adiposity-related outcomes, including prevalence of overweight and obesity, and body composition. Intermediate behavioural outcomes such as changes in physical activity and fitness, sedentary behaviour, and dietary behaviour | Other health outcomes, such as blood pressure, if not reporting about relevant adiposity outcomes |
| For behavioural outcomes, both objective and subjective measures of physical activity, dietary behaviour, or other relevant behaviours, such as sedentary behaviour, are acceptable | Other outcomes of behavioural interventions, such as cognitive development, if not reporting about relevant behavioural outcomes (increased physical activity, fitness, sedentary behaviour, or dietary behaviour) | |
| Secondary outcomes from sibling article search: Barriers and facilitators to implementation of childhood obesity prevention interventions | N/A | |
| Publication type | Peer-reviewed journal articles | Conference abstract, working paper, study protocol, report, dissertation, book, website |
| Publication year | 1990 onward | Before 1990 |
| Setting | Any African country according to the World Bank’s regional definitions of Sub-Saharan Africa and North Africa [44,45] | Countries in any other regions |
| Language | Any language | N/A |
| Intervention and Study References | Intervention Context (Targeted Setting) | Baseline Characteristics | Study Design | Components, Dose and Levels of Social Ecological Model | Outcomes |
|---|---|---|---|---|---|
| DoH Health Promoting Schools Nyawose & Naidoo 2016 [54] | Low socio-economic status Clermont Township, KwaZulu-Natal South Africa (School, family) | N = 129 Gender: 51.2% boys Age: 11–15, mean 12.26 years | Quasi-experimental, non-equivalent groups design with an intervention programme and assessment pre- and post- intervention. | 4-month intervention. Introduced various methods of PA and healthy nutritional habits within the PE lessons in the school curriculum. A minimum of two one-hour PE workshops were conducted per month. Activities included warm-up games, circuit and fun group games. Parents took part in four group sessions where PA was discussed, and dietary guidelines were introduced. Unable to estimate overall dose received. Levels: Individual, interpersonal, institution. | Sports and PA participation (learner questionnaires that have been used in other South African studies), fitness (Eurofit Physical Fitness Test Battery adapted for use in South Africa), height and weight. |
| Gum Marom Kids League (GMKL) Richards et al., 2014 [63] | Post-conflict, urban low resource setting, Gulu, Uganda (Community) | N = 1462 Gender: 43.3% boys Age: 11–14 | Single-blinded randomised controlled trial nested within observational study. | 11-week voluntary competitive sport-for-development football league. 32 volunteer adults from the local community trained as football coaches. Each weekend the GMKL participants took part in a 40-min game of football and various peace-building activities. Overall dose: ~7.5 h over 11 weeks. Levels: Individual, interpersonal, community. | Physical fitness (multi-stage fitness test and standing broad jump), anthropometric outcomes (BMI-for-age and height-for-age z-scores compared with WHO reference data). |
| Harrabi et al., 2010 [48] | Secondary public schools in Sousse, Tunisia (School) | N = 2338 Gender: 46.8% boys Age: 12–16 (mean 13.3 ± 1.1) | Pre-test post-test quasi experimental design (with control group). | Intervention over one school year. Components included classroom-based health promotion, student projects, health clubs and discussions. Interventions were delivered by project team with teachers and school doctors. Interclass sport tournaments organised throughout the school year. Award ceremony held at the end. Unable to estimate overall dose received. Levels: Individual, interpersonal, institution. | Dietary habits and PA (pre-tested self-administered questionnaire). |
| HealthKick Steyn et al., 2015 [46], De Villiers et al., 2016 [64], Uys et al., 2016 [47] | Urban and rural primary schools from the lowest 3 socio-economic quintiles, Western Cape, South Africa (School) | N = 998 or 1002 Gender: 47.2% boys Age: 10 years at baseline | Cluster RCT. | 3-year whole-of-school program targeting healthy eating and physical activity by creating a healthier school environment. Educators given training and resources to implement their own action plans. Educators asked to give extra 15 min of PA a day and at least one healthy eating activity per month. Schools set goals and implemented changes over three years. Dose: ~1.5 h/week for 3 school years. Levels: Individual, interpersonal, institution. | Dietary behavior (unquantified 24-h recall) and fitness (modified Eurofit). Used both validated and unvalidated questionnaires. |
| Healthnutz Draper et al., 2010 [53] | Poor urban school setting in Alexandra township, Johannesburg, South Africa (School) | N = Unclear Gender: NR Age: NR | Pre-post test (with control group). | 3-month intervention. Training for teachers 2 months prior to implementation, weekly PA and health education sessions for learners incorporated into curriculum. Unable to estimate overall dose received. Levels: Individual, interpersonal, institution. | Anthropometric measurements (height and weight), physical fitness (Eurofit Fitness Testing protocol adapted for use in South Africa). |
| Hochfeld et al., 2016 [52] | Poor urban school setting in Alexandra township, Johannesburg, South Africa (School, community) | N = 1975 Gender: 52% girls Age: 6–17, median 10 | Pre- and post-test design (no control group). | 14-month intervention. School breakfast provided, school kitchen upgrades, nutrition education, community development activities. Unable to estimate overall dose received. Levels: Individual, institution, community. | Anthropometric measurements (height, weight, BMI using standard protocols). |
| Kebaili et al., 2014 [65] | Public schools in urban setting in Sousse, Tunisia (School) | N = 2338 Gender: I: 46.8% boys, C: 46.5% boys Age: 12–16 | Pre-post quasi-experimental evaluation. | 3-month intervention. Interactive lessons and activities delivered by trained teachers in collaboration with doctors. Unable to estimate overall dose received. Levels: Individual, interpersonal. | Dietary behaviour (pre-tested self-administered questionnaire). |
| Maatoug et al., 2015 [59] | Urban preschools in Sousse, Tunisia (Preschool, family) | N = 539 Gender: I: 53.6% boys, C: 46.4% boys Age: I: Mean 4.50 years (±0.51), C: 4.73 years (±0.34) | Quasi- experiment (with control group). | 8-month preschool-based intervention. Lifestyle intervention with training sessions, workshops, tournaments and educative supports to teachers and parents. Unable to estimate overall dose received. Levels: Individual, interpersonal. | Eating habits, PA, and screen time (parent questionnaire). |
| “Masikhusele iKamva Lethu” (“Let Us Protect Our Future.”) Jemmott et al. [49] | Urban and rural schools in Eastern Cape, South Africa (School) | N = 1057 Gender: 52.8% girls Age: 9–18 (mean 12.4) | Cluster RCT. | 6-day intervention. Theory-based, highly structured health promotion intervention consisting of 12 1-h modules. Sessions included interactive exercises, games, brainstorming, role-playing, and group discussions. Materials included comic workbooks specially designed for the intervention. Dose: 12 h in 1 week. Levels: Individual, interpersonal. | Dietary behaviour (self-report using 7-item food frequency questionnaire developed by the National Cancer Institute) and PA (self-reported PA over past 7 days using CDC-developed 3 item questionnaire). |
| Nutrition and Physical Activity (NAP) Pilot Naidoo et al., 2009 [62] | 4 primary schools in KwaZulu-Natal, South Africa (School) | N = 256 Gender: 44% boys Age: Grade 6 learners | Prospective empirical pilot study with an intervention and an assessment before and after intervention (no control group). | 6-month intervention. Classroom-based materials were developed with cost-effectiveness and sustainability in mind. NAP was integrated into the school curriculum. Educators were trained to lead intervention activities and had some freedom in how to implement these. At least two monthly follow-up visits to schools by the research team was provided. There were also changes to the school food environment. Unable to estimate overall dose received. Levels: Individual, interpersonal, institution. | PA (self-reported through learner questionnaire). |
| Nutrition and Physical Activity (NAP) Naidoo & Coopoo 2012 [55] | Rural, peri-urban and urban schools in KwaZulu-Natal, South Africa (School) | N = 798 at baseline Gender: 54% boys Age: 9–16 years (41% of learners age 12 at the onset of the study) | Pre-post evaluation (with control group). | 18-month intervention. Classroom-based materials were developed with cost-effectiveness and sustainability in mind. NAP was integrated into the school curriculum. Educators were trained to lead intervention activities and had some freedom in how to implement these. Unable to estimate overall dose received. Levels: Individual, interpersonal, institution. | PA (self-reported through learner questionnaire) and fitness (measured using Eurofit Physical Fitness Test Battery, 1993). |
| PLAY Naude et al., 2008 [66] PLAY Lennox & Pienaar 2013 [61] | Secondary schools in a low socio-economic township area in the North-West Province, South Africa (After-school) Secondary schools in a low socio-economic township area in the North-West Province, South Africa (After-school) | N = 279 Gender: 40.5% boys Age: 13–18 | Pre-post evaluation (with reference group). | 19-week voluntary after school PA programme supervised by Biokinetics students. The programme was performed twice weekly for an hour session per day, and consisted of 20 min of aerobic dancing, 20 min of ball games, and 20 min of strength- and flexibility exercises. Dose: 38 h (2 h/week for 19 weeks) Levels: Individual. | BMI (anthropometric measurements according to ISAK-standard) and body fat % (Bod Pod, and tricep and subscapular skinfolds). |
| N = 318 Gender: 43% boys Age: Grade 8 (13–14) | Quasi-experimental before-after evaluation (with control group). | 6-month voluntary after-school physical activity intervention. Two 60-min sessions a week. The sessions were divided into 30 min of aerobic training, 15 min of strength and flexibility training, and 15 min of sport-related ball skills activities. Dose: 52 h (2 h/week for 26 weeks). Levels: Individual. | PA (previous day PA recall) and fitness (“The Bleep test”). | ||
| “Schools in Health” Maatoug et al., 2015 [60] | Urban school setting in Sousse, Tunisia (School, family, community) | N = 4003 Gender: I: 50.2% boys, C: 46.5% boys Age: 11–16 | Quasi-experiment (with control group). | 3-year school-based intervention. Trained student leaders organised events, teachers ran sessions to promote PA and healthy diets. After-school soccer games both within and between schools. Information about healthy behaviours was provided to students and parents. Snack stores were encouraged to stock healthier options, and children were rewarded with stickers for choosing healthy snacks. Unable to estimate overall dose received. Levels: Individual, interpersonal, institution, community. | Overweight/obesity (standard anthropometric measurements), PA (standardised, pretested questionnaire) and dietary behavior (standardised, pretested questionnaire). |
| Walter 2014 [56] | 3 disadvantaged primary schools in Port Elizabeth, South Africa (School, family) | N = 79 Gender: 48.1% boys Age: Mean age 10.27 ± 1.22, range 9–12 | Experimental design (no comparison). | 6-week intervention delivered by University students with parents and teachers. The intervention focused around providing sports and play equipment to schools. Focus on free play. Unable to estimate overall dose received. Levels: Interpersonal, institution. | PA (Actigraph accelerometry). |
| Study | Quality Assessment | Effect on Dietary Behaviours | Effect on Physical Activity | Effect on Anthropometric Outcomes |
|---|---|---|---|---|
| DoH Health Promoting Schools [54] | Weak | . | 0 | + |
| Gum Marom Kids League [63] | Moderate–strong | . | 0 | 0 |
| Harrabi et al. [48] | Weak | 0 | ++ | . |
| HealthKick [46,47,64] | Weak | 0 | 0 | . |
| Healthnutz [53] | Weak | . | + | - |
| Hochfeld et al. [52] | Weak | . | . | + |
| Kebaili et al. [65] | Weak–moderate | + | . | . |
| Maatoug et al. [59] | Weak | 0 | 0 | . |
| “Masikhusele iKamva Lethu” [49] | Weak | ++ | ++ | . |
| NAP pilot [62] | Weak | . | + | 0 |
| NAP [55] | Weak | . | + | 0 |
| PLAY [61,66] | Weak | . | 0 | ++ |
| “Schools in Health” [60] | Weak | 0 | 0 | + |
| Walter [56] | Weak–moderate | . | + | . |
| Overall | Weak | 0 | 0/+ | 0/+ |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klingberg, S.; Draper, C.E.; Micklesfield, L.K.; Benjamin-Neelon, S.E.; van Sluijs, E.M.F. Childhood Obesity Prevention in Africa: A Systematic Review of Intervention Effectiveness and Implementation. Int. J. Environ. Res. Public Health 2019, 16, 1212. https://doi.org/10.3390/ijerph16071212
Klingberg S, Draper CE, Micklesfield LK, Benjamin-Neelon SE, van Sluijs EMF. Childhood Obesity Prevention in Africa: A Systematic Review of Intervention Effectiveness and Implementation. International Journal of Environmental Research and Public Health. 2019; 16(7):1212. https://doi.org/10.3390/ijerph16071212
Chicago/Turabian StyleKlingberg, Sonja, Catherine E. Draper, Lisa K. Micklesfield, Sara E. Benjamin-Neelon, and Esther M. F. van Sluijs. 2019. "Childhood Obesity Prevention in Africa: A Systematic Review of Intervention Effectiveness and Implementation" International Journal of Environmental Research and Public Health 16, no. 7: 1212. https://doi.org/10.3390/ijerph16071212
APA StyleKlingberg, S., Draper, C. E., Micklesfield, L. K., Benjamin-Neelon, S. E., & van Sluijs, E. M. F. (2019). Childhood Obesity Prevention in Africa: A Systematic Review of Intervention Effectiveness and Implementation. International Journal of Environmental Research and Public Health, 16(7), 1212. https://doi.org/10.3390/ijerph16071212