Implementing a Physical Activity Promoting Program in a Flex-Office: A Process Evaluation with a Mixed Methods Design

Abstract
:1. Introduction
2. Materials and Methods
2.1. The Overarching Research Project—The Active Office Design Study
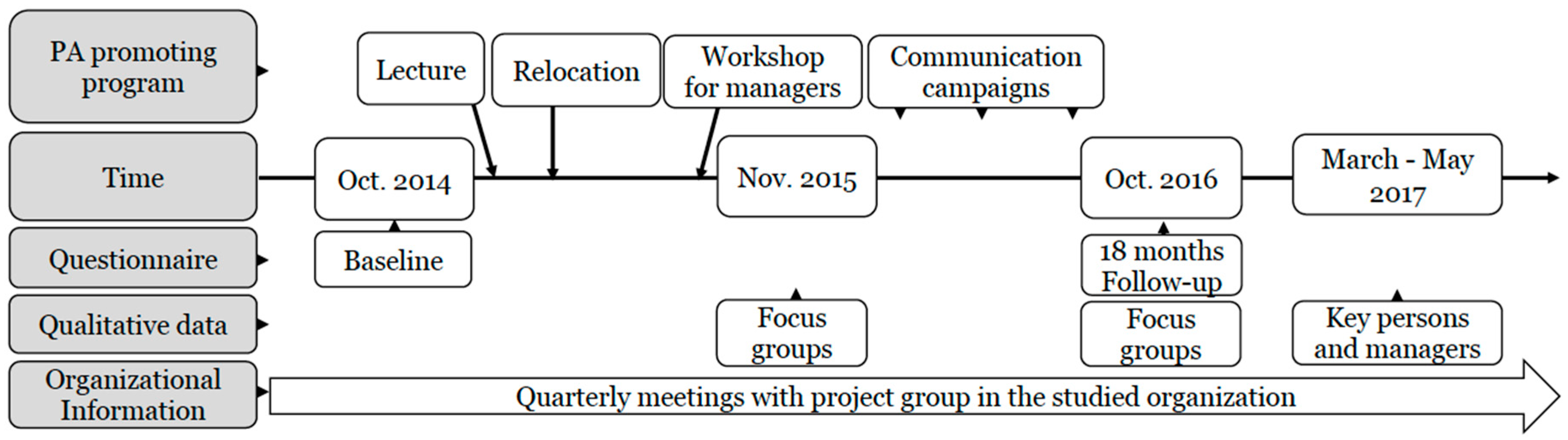
2.2. Development and Implementation of the Physical Activity Promoting Program
2.3. Data Collection
2.3.1. Qualitative Data
2.3.2. Quantitative Data
2.3.3. Description of the Process Evaluation Model
2.3.4. Analysis of Qualitative Data
2.3.5. Analysis of Quantitative Data
3. Results
3.1. Participants and Background Characteristics
3.2. Context of the PA-Promoting Program
3.2.1. Support for Physical Activity
3.2.2. Environmental and Ergonomic Challenges
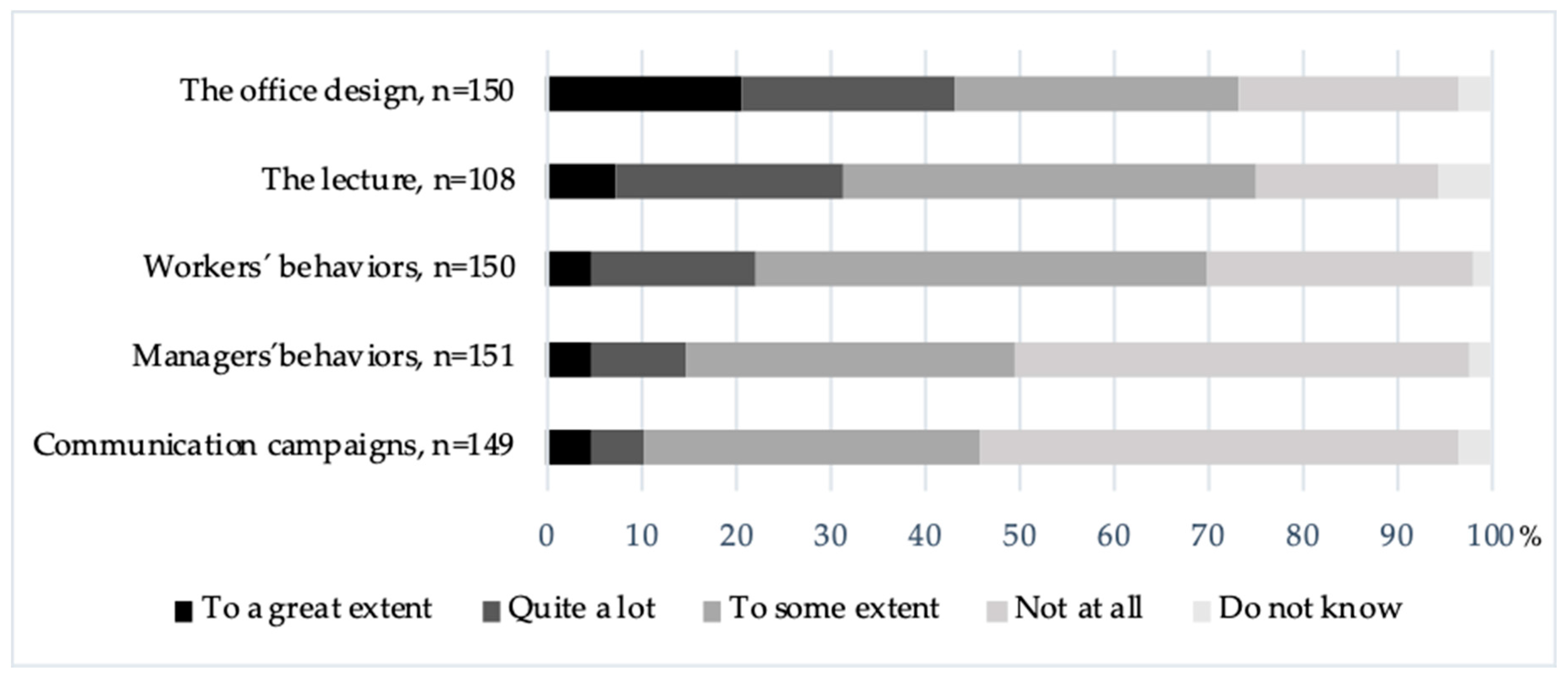
3.3. Intervention Development and Implementation of the PA-Promoting Program
Clarity in the Organization
3.4. Behaviors
Voluntary and Involuntary Physical Activity and Mediators
3.5. Mental Models
3.5.1. Balance of Communication Intensity
3.5.2. Openness for Activity
4. Discussion
4.1. Finding the Appropriate and Optimal Level of Standing
4.2. Walking for Good and Bad
4.3. Need, Timing and Responsibility for Being Active
4.4. The Challenge of Balancing the Message and Still Moving forward
4.5. Methodological Considerations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Church, T.S.; Thomas, D.M.; Tudor-Locke, C.; Katzmarzyk, P.T.; Earnest, C.P.; Rodarte, R.Q.; Martin, C.K.; Bouchard, C. Trends over 5 decades in U.S. occupation-related physical activity and their associations with obesity. PLoS ONE 2011, 6, e19657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tremblay, M.S.; Aubertm, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M. Sedentary Behavior Research Network (SBRN)-Terminology Consensus Project process and outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biswas, A.; Oh, P.I.; Faulkner, G.E.; Bajaj, R.R.; Silver, M.A.; Mitchell, M.S.; Alter, D.S. Sedentary time and its association with risk for disease incidence, mortality, and hospitalization in adults a systematic review and meta-analysis. Ann. Intern. Med. 2015, 162, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Katzmarzyk, P.T.; Church, T.S.; Craig, C.L.; Bouchard, C. Sitting time and mortality from all causes, cardiovascular disease, and cancer. Med. Sci. Sports Exerc. 2009, 41, 998–1005. [Google Scholar] [CrossRef] [PubMed]
- Parry, S.; Straker, L.; Gilson, N.D.; Smith, A.J. Participatory workplace interventions can reduce sedentary time for office workers-A randomised controlled trial. PLoS ONE 2013, 8, e78957. [Google Scholar] [CrossRef]
- Dunstan, D.W.; Howard, B.; Healy, G.N.; Owen, N. Too much sitting-a health hazard. Diabetes Res. Clin. Pract. 2012, 97, 368–376. [Google Scholar] [CrossRef]
- Healy, G.N.; Eakin, E.G.; Owen, N.; LaMontagne, A.D.; Moodie, M.; Winkler, E.A.H.; Fjeldsoe, J.S.; Wiesner, G.; Willenberg, L.; Dunstan, D.W. A Cluster Randomized Controlled Trial to Reduce Office Workers’ Sitting Time: Effect on Activity Outcomes. Med. Sci. Sports Exerc. 2016, 48, 1787–1797. [Google Scholar] [CrossRef]
- Straker, L.; Abbott, R.A.; Heiden, M.; Mathiassen, S.E.; Toomingas, A. Sit-stand desks in call centres: Associations of use and ergonomics awareness with sedentary behavior. Appl. Ergon. 2013, 44, 517–522. [Google Scholar] [CrossRef]
- Chu, A.H.Y.; Ng, S.H.X.; Tan, C.S.; Win, A.M.; Koh, D.; Müller-Riemenschneider, F. A systematic review and meta-analysis of workplace intervention strategies to reduce sedentary time in white-collar workers. Obes. Rev. 2016, 17, 467–481. [Google Scholar] [CrossRef]
- Danquah, I.H.; Kloster, S.; Holtermann, A.; Aadahl, M.; Bauman, A.; Ersbøll, A.K.; Tolstrup, J.S. Take a Stand! - A multi-component intervention aimed at reducing sitting time among office workers-a cluster randomized trial. Int. J. Epidemiol. 2017, 46, 128–140. [Google Scholar] [CrossRef]
- Edwardson, C.L.; Yates, T.; Biddle, S.J.H.; Davies, M.J.; Dunstan, D.W.; Esliger, D.W.; Gray, L.J.; Jackson, B.; O´Connel, S.W.; Waheed, G.; et al. Effectiveness of the stand more at (SMArT) work intervention: Cluster randomised controlled trial. BMJ 2018, 363, k3870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keadle, S.K.; Conroy, D.E.; Buman, M.P.; Dunstan, D.W.; Matthews, C.E. Targeting reductions in sitting time to increase physical activity and improve health. Med. Sci. Sports Exerc. 2017, 49, 1572–1582. [Google Scholar] [CrossRef] [PubMed]
- Mackenzie, K.; Such, E.; Norman, P.; Goyder, E. The development, implementation and evaluation of interventions to reduce workplace sitting: A qualitative systematic review and evidence-based operational framework. BMC Public Health 2018, 18, 833. [Google Scholar] [CrossRef] [PubMed]
- Lahtinen, M.; Ruohomäki, V.; Haapakangas, A.; Reijula, K. Developmental needs of workplace design practices. Intell. Build. Int. 2015, 7, 198–214. [Google Scholar] [CrossRef]
- Wohlers, C.; Hertel, G. Choosing where to work at work–towards a theoretical model of benefits and risks of activity-based flexible offices. Ergonomics 2017, 60, 467–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engelen, L.; Chau, J.; Young, S.; Mackey, M.; Jeyapalan, D.; Bauman, A. Is activity-based working impacting health, work performance and perceptions? A systematic review. Build. Res. Inf. 2019, 47, 468–479. [Google Scholar] [CrossRef]
- De Been, I.; Beijer, M. The influence of office type on satisfaction and perceived productivity support. J. Facil. Manag. 2014, 12, 142–157. [Google Scholar] [CrossRef] [Green Version]
- Danielsson, B.C.; Bodin, L. Office type in relation to health, well-being, and job satisfaction among employees. Environ. Behav. 2008, 40, 636–668. [Google Scholar] [CrossRef]
- Hallman, D.M.; Mathiassen, S.E.; Jahncke, H. Sitting patterns after relocation to activity-based offices: A controlled study of a natural intervention. Prev. Med. 2018, 111, 384–390. [Google Scholar] [CrossRef]
- Moore, G.F.; Audrey, S.; Barker, M.; Bond, L.; Bonell, C.; Hardeman, W.; Moore, L.; O´Cathain, A.; Tinati, T.; Wight, D.; et al. Process evaluation of complex interventions: Medical Research Council guidance. BMJ 2015, 350, h1258. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, K.; Randall, R. Opening the black box: Presenting a model for evaluating organizational- level interventions. Eur. J. Work Organ. Psychol. 2013, 22, 601–617. [Google Scholar] [CrossRef]
- Neuhaus, M.; Healy, G.N.; Dunstan, D.W.; Owen, N.; Eakin, E.G. Workplace sitting and height-adjustable workstations: A randomized controlled trial. Am. J. Prev. Med. 2014, 46, 30–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mackenzie, K.; Goyder, E.; Eves, F. Acceptability and feasibility of a low-cost, theory-based and co-produced intervention to reduce workplace sitting time in desk-based university employees. BMC Public Health 2015, 15, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wahlström, V.; Bergman, F.; Öhberg, F.; Eskilsson, T.; Olsson, T.; Järvholm, L.S. Effects of a multicomponent physical activity promoting program on sedentary behavior, physical activity and body measures: A longitudinal study in different office types. Scand. J. Work Environ. Health 2019, 45, 493–504. [Google Scholar] [CrossRef] [PubMed]
- Fetters, M.D.; Curry, L.A.; Creswell, J.W. Achieving integration in mixed methods designs-Principles and practices. Health Serv. Res. 2013, 48, 2134–2156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nielsen, K.; Abildgaard, J.S. Organizational interventions: A research-based framework for the evaluation of both process and effects. Work Stress 2013, 27, 278–297. [Google Scholar] [CrossRef]
- Gill, P.; Stewart, K.; Treasure, E.; Chadwick, B. Methods of data collection in qualitative research: Interviews and focus groups. Br. Dent. J. 2008, 204, 291–295. [Google Scholar] [CrossRef]
- Wahlström, J.; Hagberg, M.; Toomingas, A.; Wigaeus Tornqvist, E. Perceived muscular tension, job strain, physical exposure, and associations with neck pain among VDU users; a prospective cohort study. Occup. Environ. Med. 2004, 61, 523–528. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, M.; Karlsson, J.; Ware, J.E. The Swedish SF-36 Health Survey-I. Evaluation of data quality, scaling assumptions, reliability and construct validity across general populations in Sweden. Soc. Sci. Med. 1995, 41, 1349–1358. [Google Scholar] [CrossRef]
- Ng, N.; Söderman, K.; Norberg, M.; Öhman, A. Increasing physical activity, but persisting social gaps among middle-aged people: Trends in Northern Sweden from 1990 to 2007. Glob. Health Action 2011, 4, 6347. [Google Scholar] [CrossRef]
- Bergman, F.; Wahlström, V.; Stomby, A.; Otten, J.; Lanthén, E.; Renklint, R.; Waling, M.; Sörlin, A.; Boraxxbeck, C.J.; Wennberg, P.; et al. Treadmill workstations in office workers who are overweight or obese: A randomised controlled trial. Lancet Public Health 2018, 3, e523–e535. [Google Scholar] [CrossRef] [Green Version]
- Kerr, N.A.; Yore, M.M.; Ham, S.A.; Dietz, W.H. Increasing stair use in a worksite through environmental changes. Environ. Chang. 2004, 18, 312–316. [Google Scholar] [CrossRef] [PubMed]
- Elo, S.; Kyngäs, H. The qualitative content analysis process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Graneheim, U.H.; Lundman, B. Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Educ. Today 2004, 24, 105–112. [Google Scholar] [CrossRef]
- Elo, S.; Kääriänien, M.; Kanste, O.; Pölkki, T.; Utriainen, K.; Kyngäs, H. Qualitative Content Analysis. SAGE Open 2014, 1, 1–10. [Google Scholar] [CrossRef]
- Renaud, L.R.; Huysmans, M.A.; van der Ploeg, H.P.; Speklé, E.M.; van der Beek, A.J. Long-term access to sit-stand workstations in a large office population: User profiles reveal differences in sitting time and perceptions. Int. J. Environ. Res. Public Health 2018, 15, 2019. [Google Scholar] [CrossRef] [Green Version]
- Nooijen, C.F.J.; Kallings, L.V.; Blom, V.; Ekblom, Ö.; Forsell, Y.; Ekblom, M.M. Common perceived barriers and facilitators for reducing sedentary behaviour among office workers. Int. J. Environ. Res. Public Health 2018, 15, 792. [Google Scholar] [CrossRef] [Green Version]
- De Cocker, K.; Veldeman, C.; De Bacquer, D.; Braeckman, L.; Owen, N.; Cardon, G.; Bourdeaudhuij, I.D. Acceptability and feasibility of potential intervention strategies for influencing sedentary time at work: Focus group interviews in executives and employees. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Gilson, N.; Straker, L.; Parry, S. Occupational sitting: Practitioner perceptions of health risks, intervention strategies and influences. Health Promot. J. Aust. 2012, 23, 208–212. [Google Scholar] [CrossRef]
- Agarwal, S.; Steinmaus, C.; Harris-Adamson, C. Sit-stand workstations and impact on low back discomfort: A systematic review and meta-analysis. Ergonomics 2018, 61, 538–552. [Google Scholar] [CrossRef]
- Coenen, P.; Gilson, N.; Healy, G.N.; Dunstan, D.W.; Straker, L.M. A qualitative review of existing national and international occupational safety and health policies relating to occupational sedentary behaviour. Appl. Ergon. 2017, 60, 320–333. [Google Scholar] [CrossRef] [PubMed]
- Haapakangas, A.; Hallman, D.M.; Mathiassen, S.E.; Jahncke, H. Self-rated productivity and employee well-being in activity-based offices: The role of environmental perceptions and workspace use. Build. Environ. 2018, 145, 115–124. [Google Scholar] [CrossRef]
- Fletcher, E.A.; Salmon, J.; McNaughton, S.A.; Orellana, L.; Wadley, G.D.; Bruce, C.; Dempsey, P.D.; Lacy, K.E.; Dunstan, D.W. Effects of breaking up sitting on adolescents’ postprandial glucose after consuming meals varying in energy: A cross-over randomised trial. J. Sci. Med. Sport. 2018, 2, 280–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dempsey, P.C.; Blankenship, J.M.; Larsen, R.N.; Sacre, J.W.; Sethi, P.; Straznicky, N.E.; Cohen, N.D.; Cerin, E.; Lambert, G.W.; Owen, N.; et al. Interrupting prolonged sitting in type 2 diabetes: Nocturnal persistence of improved glycaemic control. Diabetologia 2017, 60, 499–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cifuentes, M.; Qin, J.; Fulmer, S.; Bello, A. Facilitators and barriers to using treadmill workstations under real working conditions: A qualitative study in female office workers. Am. J. Health Promot. 2015, 30, 93–100. [Google Scholar] [CrossRef]
- Tudor-Locke, C.; Hendrick, C.A.; Duet, M.T.; Swift, D.L.; Schuna, J.M.; Martin, C.K.; Johnson, W.D.; Church, T.S. Implementation and adherence issues in a workplace treadmill desk intervention. Appl. Physiol. Nutr. Metab. 2014, 39, 1104–1111. [Google Scholar] [CrossRef]
- Van Berkel, J.; Meershoek, A.; Janssens, R.M.; Boot, C.R.; Proper, K.I.; Van Der Beek, A.J. Ethical considerations of worksite health promotion: An exploration of stakeholders’ views. BMC Public Health 2014, 14, 458. [Google Scholar] [CrossRef] [Green Version]
- Hadgraft, N.T.; Brakenridge, C.L.; Lamontagne, A.D.; Fjeldsoe, B.S.; Lynch, B.M.; Dunstan, D.W.; Owen, N.; Healy, G.N.; Lawler, S.P. Feasibility and acceptability of reducing workplace sitting time: A qualitative study with Australian office workers. BMC Public Health 2016, 16, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Waters, C.N.; Ling, E.P.; Chu, A.H.Y.; Ng, S.H.X.; Chia, A.; Lim, Y.W.; Müller-Riemenschneider, F. Assessing and understanding sedentary behaviour in office-based working adults: A mixed-method approach. BMC Public Health 2016, 16, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Abildgaard, J.S.; Saksvik, P.; Nielsen, K. How to measure the intervention process? An assessment of qualitative and quantitative approaches to data collection in the process evaluation of organizational interventions. Front. Psychol. 2016, 7, 1380. [Google Scholar] [CrossRef] [Green Version]
- O’Cathain, A.; Murphy, E.; Nicholl, J. The quality of mixed methods studies in health services research. J. Health Serv. Res. Policy 2008, 13, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Hadgraft, N.T.; Healy, G.; Neville, O.; Winkler, E.; Lynch, B.; Sethi, P.; Eakin, E.G.; Moodie, M.; LaMontagne, A.D.; Wiesner, G.; et al. Office workers objectively assessed total and prolonged sitting time: Individual-level correlates and worksite variations. Prev. Med. Rep. 2016, 4, 148–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hadgraft, N.T.; Winkler, E.A.H.; Healy, G.N.; Lynch, B.M.; Neuhaus, M.; Eakin, E.G.; Dunstan, D.W.; Owen, N.; Fjeldsoe, B.S. Intervening to reduce workplace sitting: Mediating role of social-cognitive constructs during a cluster randomised controlled trial. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Demography and Work Characteristics | Women (%) | Men (%) | All (%) |
|---|---|---|---|
| Managerial position | 25 | 28 | 26 |
| Age groups | |||
| 18–39 years | 28 | 26 | 28 |
| 40–49 years | 24 | 30 | 26 |
| >50 years | 48 | 44 | 46 |
| Employment degree | |||
| 100% | 94 | 98 | 95 |
| 75–99% | 6 | 2 | 5 |
| Computer work per workday | |||
| 0–4 h | 20 | 26 | 22 |
| 4–6 h | 34 | 46 | 38 |
| 6–8 h | 46 | 28 | 40 |
| Meetings outside the office | |||
| Never | 23 | 20 | 22 |
| 1–2 times per month | 28 | 36 | 31 |
| 3–4 times per month | 22 | 18 | 20 |
| 1–2 times per week | 17 | 16 | 16 |
| 3 times per week to daily | 10 | 10 | 11 |
| Standing while working individually | |||
| Never | 5 | 8 | 6 |
| 1–3 times per month | 21 | 26 | 22 |
| 1–2 times per week | 20 | 20 | 20 |
| 3–5 times per week | 17 | 8 | 14 |
| Daily | 37 | 38 | 38 |
| Health and Lifestyle | |||
| Self-rated general health | |||
| Very good or excellent | 55 | 70 | 60 |
| Good and fair | 44 | 28 | 38 |
| Bad | 1 | 2 | 1 |
| Physical exercise | |||
| No exercise | 2 | 6 | 3 |
| Occasionally—not regular | 24 | 22 | 23 |
| Once a week | 16 | 8 | 13 |
| 2–3 times a week | 45 | 30 | 40 |
| >3 times a week | 14 | 34 | 21 |
| Musculoskeletal neck-shoulder symptoms | |||
| Never or seldom | 46 | 60 | 51 |
| Sometimes | 29 | 20 | 26 |
| Often | 13 | 10 | 12 |
| Always | 12 | 10 | 11 |
| Symptoms of stress | |||
| Never or seldom | 42 | 50 | 44 |
| Sometimes | 32 | 30 | 31 |
| Often | 22 | 14 | 19 |
| Always | 5 | 6 | 5 |
| Subcategories | Categories | Element in PE-Model |
|---|---|---|
| Knowledge about PA and SB | Support for physical activity | Context |
| Worksite policy and routines | ||
| Interior design | ||
| Crowded office | Environmental and ergonomic challenges | |
| Workstation adjustments | ||
| Role models | Clarity in the organization | Intervention |
| Responsibility at various levels | ||
| Program ownership | ||
| Focus in health promotion | ||
| Strive for variation | Voluntary and involuntary physical activity | Behaviors |
| Walks to find a workplace | ||
| Equipment and activities stimulate | ||
| Productivity in focus | Mediators | |
| Physical discomfort | ||
| Perception and interpretation | Balance of communication intensity | Mental models |
| of communication | ||
| Conflicting needs | ||
| Strive for physical activity | Openness for activity | |
| Necessities for progress |
| How frequent is it… | ||||||
| Never | Seldom | Sometimes | Often | p-Value | ||
| …with regular breaks from sitting during meetings? (%) | Baseline | 23.2 | 33.8 | 36.4 | 6.6 | 0.002 |
| 18 m | 13.2 | 33.1 | 43.7 | 9.9 | ||
| …that you or a colleague suggest a walking meeting? (%) | Baseline | 82.0 | 13.8 | 3.3 | 0.0 | 0.001 |
| 18 m | 69.5 | 22.5 | 7.9 | 0.0 | ||
| …that you or a colleague suggest a walk during breaks? (%) | Baseline | 20.5 | 35.1 | 37.7 | 6.6 | 0.522 |
| 18 m | 28.5 | 27.8 | 35.8 | 7.9 | ||
| To what degree… | ||||||
| Not at all | Somewhat | To some extent | To a big extent | p-Value | ||
| … is it socially accepted to stand or walk while working? 1 (%) | Baseline | 5.4 | 12.8 | 11.4 | 70.5 | < 0.001 |
| 18 m | 0.0 | 6.0 | 9.9 | 84.1 | ||
| … are your clothes a barrier for standing or walking at work? (%) | Baseline | 88.1 | 4.0 | 7.3 | 0.7 | 0.062 |
| 18 m | 80.8 | 7.3 | 9.9 | 2.0 | ||
| How often do you use the following possibilities to work standing or walking? | ||||||||
| Never | 1–3 times per month | 1–2 times per week | 3–5 times per week | Daily | NA 1 or missing | p-Value | ||
| Standing while working individually, % | Baseline | 6 | 22.5 | 19.9 | 13.9 | 37.7 | 1 | 0.194 |
| 18 m | 10.0 | 20.7 | 22.0 | 12.0 | 35.3 | 2 | ||
| Standing at meetings, % | Baseline | 84.1 | 11.0 | 3.4 | 0.7 | 0.7 | 7 | < 0.001 |
| 18 m | 58.5 | 32.0 | 5.4 | 3.4 | 0.7 | 5 | ||
| Taking the stairs, % | Baseline | 2.6 | 3.3 | 13.2 | 8.6 | 72.4 | 0 | < 0.001 |
| 18 m | 1.3 | 0.7 | 2.0 | 2.7 | 93.3 | 3 | ||
| Participating in walking meetings, % | Baseline | 87.4 | 10.5 | 1.4 | 0,0 | 0.7 | 9 | 0.689 |
| 18 m | 87.1 | 12.2 | 0.7 | 0.0 | 0.0 | 5 | ||
| Walk or cycle to meetings outside the office, % | Baseline | 17.7 | 41.5 | 18.4 | 9.5 | 12.9 | 5 | 0.776 |
| 18 m | 16.7 | 44.4 | 15.3 | 13.2 | 10.4 | 7 | ||
| Treadmill station, % | 18 m | 87.9 | 9.4 | 2.0 | 0.7 | 0 | 3 | |
| How do you like the following possibilities to stand or walk at work? | ||||||||
| Do not like at all | Do not like so much | Like it somewhat | Like a lot | No opinion 2 | Missing | p-Value | ||
| Standing while working individually, % | Baseline | 2.0 | 12.2 | 42.9 | 42.9 | 5 | 0 | 0.003 |
| 18 m | 6.2 | 19.3 | 37.2 | 37.2 | 5 | 2 | ||
| Standing at meetings, % | Baseline | 39.1 | 23.4 | 23.4 | 14.1 | 88 | 0 | 0.056 |
| 18 m | 21.6 | 28.8 | 35.1 | 14.4 | 39 | 2 | ||
| Taking the stairs, % | Baseline | 2.0 | 4.7 | 26.0 | 67.3 | 2 | 0 | < 0.001 |
| 18 m | 1.3 | 0.0 | 8.7 | 90.0 | 1 | 1 | ||
| Participating in walking meetings, % | Baseline | 22.8 | 21.1 | 29.8 | 26.3 | 95 | 0 | 0.122 |
| 18 m | 35.2 | 20.9 | 27.5 | 16.4 | 59 | 2 | ||
| Walk or cycle to meetings outside the office, % | Baseline | 6.2 | 7.0 | 36.4 | 50.4 | 22 | 2 | 0.452 |
| 18 m | 6.6 | 2.9 | 33.8 | 56.6 | 14 | 2 | ||
| Treadmill station, % | 18 m | 44.7 | 15.8 | 9.2 | 2.6 | 39 | 3 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wahlström, V.; Fjellman-Wiklund, A.; Harder, M.; Slunga Järvholm, L.; Eskilsson, T. Implementing a Physical Activity Promoting Program in a Flex-Office: A Process Evaluation with a Mixed Methods Design. Int. J. Environ. Res. Public Health 2020, 17, 23. https://doi.org/10.3390/ijerph17010023
Wahlström V, Fjellman-Wiklund A, Harder M, Slunga Järvholm L, Eskilsson T. Implementing a Physical Activity Promoting Program in a Flex-Office: A Process Evaluation with a Mixed Methods Design. International Journal of Environmental Research and Public Health. 2020; 17(1):23. https://doi.org/10.3390/ijerph17010023
Chicago/Turabian StyleWahlström, Viktoria, Anncristine Fjellman-Wiklund, Mette Harder, Lisbeth Slunga Järvholm, and Therese Eskilsson. 2020. "Implementing a Physical Activity Promoting Program in a Flex-Office: A Process Evaluation with a Mixed Methods Design" International Journal of Environmental Research and Public Health 17, no. 1: 23. https://doi.org/10.3390/ijerph17010023
APA StyleWahlström, V., Fjellman-Wiklund, A., Harder, M., Slunga Järvholm, L., & Eskilsson, T. (2020). Implementing a Physical Activity Promoting Program in a Flex-Office: A Process Evaluation with a Mixed Methods Design. International Journal of Environmental Research and Public Health, 17(1), 23. https://doi.org/10.3390/ijerph17010023