Development and Validation of a Wearable Inertial Sensors-Based Automated System for Assessing Work-Related Musculoskeletal Disorders in the Workspace




Abstract
:1. Introduction
2. Materials and Methods
2.1. System Design
2.2. System Implementation
2.3. System Validation
2.3.1. Participants
2.3.2. Experimental Procedures and Task Design
2.3.3. Data Processing and Analysis
3. Results
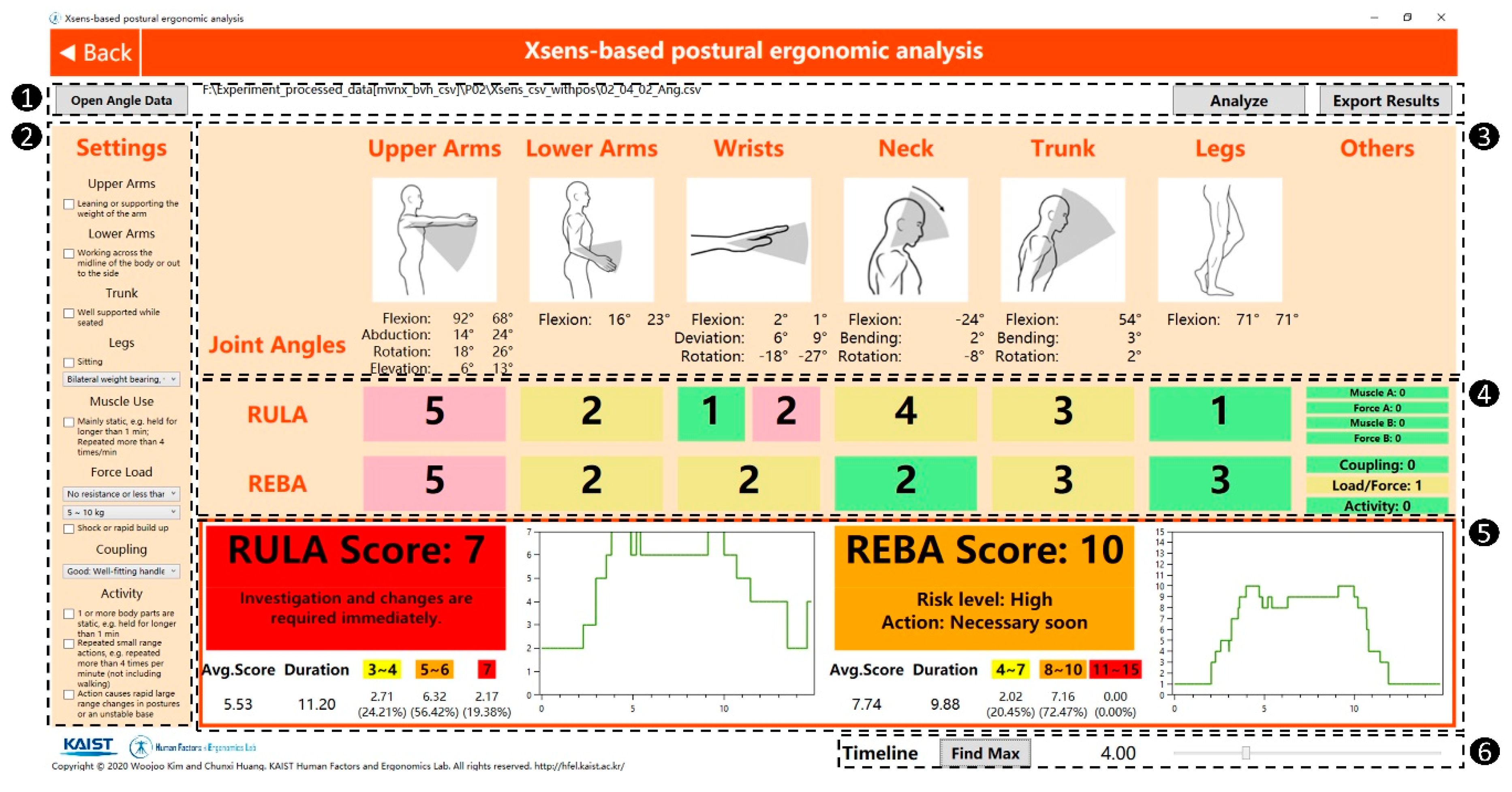
3.1. Validation of the RULA/REBA-Based Postural Ergonomic Analysis
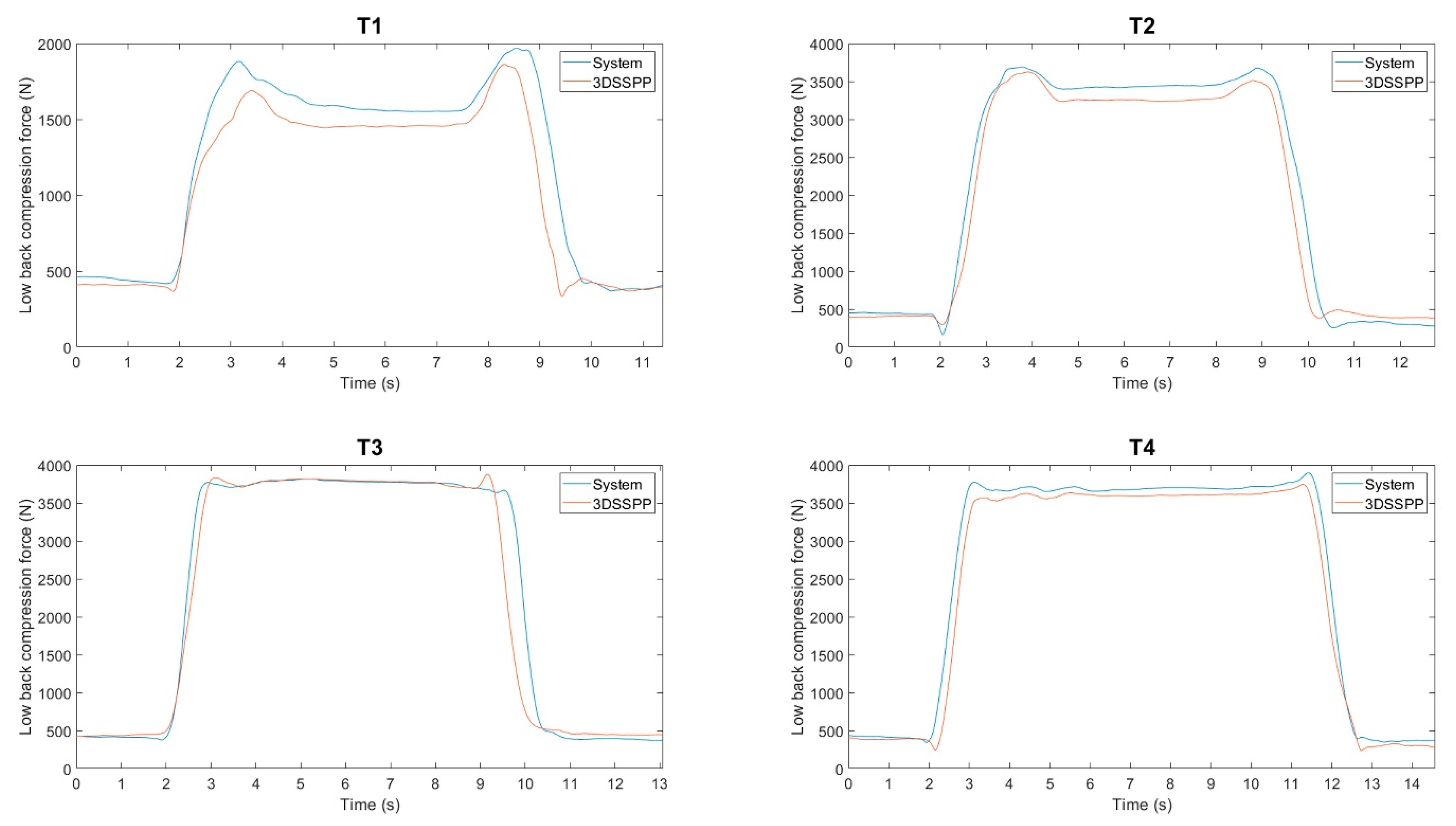
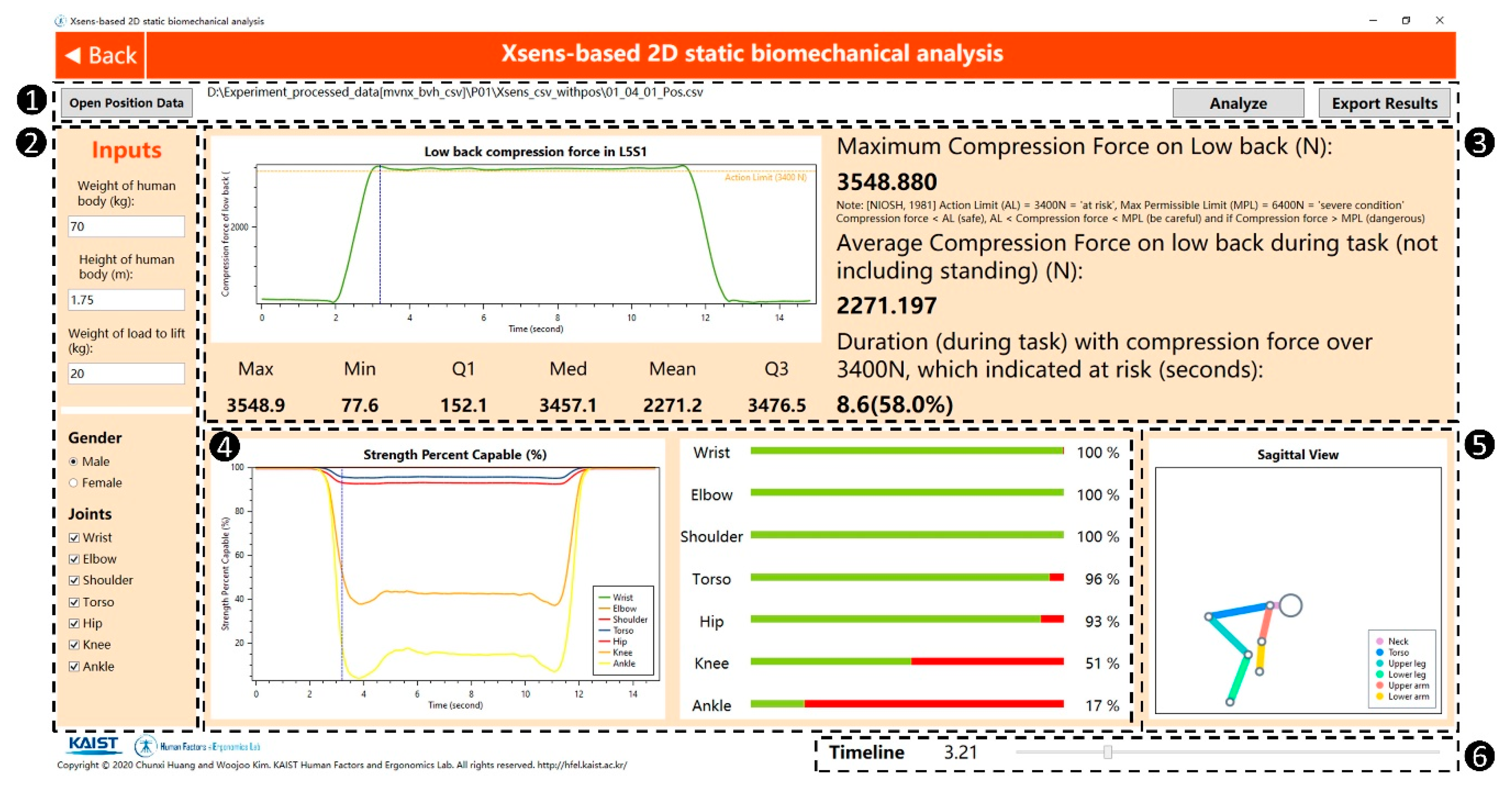
3.2. Validation of the 2D Static Biomechanical Analysis
4. Discussion
4.1. System Development
4.2. System Validation
4.3. Limitations and Future Work
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kim, I.J. The Role of Ergonomics for Construction Industry Safety and Health Improvements. J. Ergon. 2017, 7, 2–5. [Google Scholar] [CrossRef]
- Choobineh, A.; Tabatabaee, S.; Behzadi, M. Musculoskeletal problems among workers of an iranian sugar-producing factory. Int. J. Occup. Saf. Ergon. 2009, 15, 419–424. [Google Scholar] [CrossRef] [PubMed]
- Niu, S. Ergonomics and occupational safety and health: An ILO perspective. Appl. Ergon. 2010, 41, 744–753. [Google Scholar] [CrossRef] [PubMed]
- Badley, E.M.; Rasooly, I.; Webster, G.K. Relative importance of musculoskeletal disorders as a cause of chronic health problems, disability, and health care utilization: Findings from the 1990 Ontario Health Survey. J. Rheumatol. 1994, 21, 505–514. [Google Scholar] [PubMed]
- Faucett, J.; Garry, M.; Nadler, D.; Ettare, D. A test of two training interventions to prevent work-related musculoskeletal disorders of the upper extremity. Appl. Ergon. 2002, 33, 337–347. [Google Scholar] [CrossRef]
- Kee, D.; Chung, M.K.; Kim, J.-H. Legal system and its effect for prevention of work-related musculoskeletal disorders in Korea. Int. J. Ind. Ergon. 2011, 41, 224–232. [Google Scholar] [CrossRef]
- Bhattacharya, A. Costs of occupational musculoskeletal disorders (MSDs) in the United States. Int. J. Ind. Ergon. 2014, 44, 448–454. [Google Scholar] [CrossRef]
- Kumar, S. Theories of musculoskeletal injury causation. Ergonomics 2001, 44, 17–47. [Google Scholar] [CrossRef]
- Golabchi, A.; Han, S.; Seo, J.; Han, S.; Lee, S.; Al-Hussein, M. An Automated Biomechanical Simulation Approach to Ergonomic Job Analysis for Workplace Design. J. Constr. Eng. Manag. 2015, 141, 04015020. [Google Scholar] [CrossRef]
- Kuorinka, I.; Jonsson, B.; Kilbom, A.; Vinterberg, H.; Biering-Sørensen, F.; Andersson, G.; Jørgensen, K. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl. Ergon. 1987, 18, 233–237. [Google Scholar] [CrossRef]
- Aarås, A.; Horgen, G.; Bjørset, H.-H.; Ro, O.; Thoresen, M. Musculoskeletal, visual and psychosocial stress in VDU operators before and after multidisciplinary ergonomic interventions. Appl. Ergon. 1998, 29, 335–354. [Google Scholar] [CrossRef]
- Vieira, E.R.; Kumar, S.; Coury, H.J.C.G.; Narayan, Y. Low back problems and possible improvements in nursing jobs. J. Adv. Nurs. 2006, 55, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Borg, G. Perceived exertion as an indicator of somatic stress. Scand. J. Rehabil. Med. 1970, 2, 92–98. [Google Scholar] [PubMed]
- Dane, D.; Feuerstein, M.; Huang, G.D.; Dimberg, L.; Ali, D.; Lincoln, A. Measurement Properties of a Self-Report Index of Ergonomic Exposures for Use in an Office Work Environment. J. Occup. Environ. Med. 2002, 44, 73–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, T.; Kumar, S. Comparison of Ergonomic Risk Assessment Output in Four Sawmill Jobs. Int. J. Occup. Saf. Ergon. 2010, 16, 105–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kucera, K.L.; Loomis, D.; Lipscomb, H.J.; Marshall, S.W.; Mirka, G.A.; Daniels, J.L. Ergonomic risk factors for low back pain in North Carolina crab pot and gill net commercial fishermen. Am. J. Ind. Med. 2009, 52, 311–321. [Google Scholar] [CrossRef] [Green Version]
- Karhu, O.; Kansi, P.; Kuorinka, I. Correcting working postures in industry: A practical method for analysis. Appl. Ergon. 1977, 8, 199–201. [Google Scholar] [CrossRef]
- Buchholz, B.; Paquet, V.; Punnett, L.; Lee, D.; Moir, S. PATH: A work sampling-based approach to ergonomic job analysis for construction and other non-repetitive work. Appl. Ergon. 1996, 27, 177–187. [Google Scholar] [CrossRef]
- McAtamney, L.; Corlett, E.N. RULA: A survey method for the investigation of work-related upper limb disorders. Appl. Ergon. 1993, 24, 91–99. [Google Scholar] [CrossRef]
- Hignett, S.; McAtamney, L. Rapid Entire Body Assessment (REBA). Appl. Ergon. 2000, 31, 201–205. [Google Scholar] [CrossRef]
- Fagarasanu, M.; Kumar, S. Measurement instruments and data collection: A consideration of constructs and biases in ergonomics research. Int. J. Ind. Ergon. 2002, 30, 355–369. [Google Scholar] [CrossRef]
- Wang, D.; Dai, F.; Ning, X. Risk assessment of work-related musculoskeletal disorders in construction: State-of-the-art review. J. Constr. Eng. Manag. 2015, 141, 04015008. [Google Scholar] [CrossRef]
- Robertson, M.; Amick, B.C.; DeRango, K.; Rooney, T.; Bazzani, L.; Harrist, R.; Moore, A. The effects of an office ergonomics training and chair intervention on worker knowledge, behavior and musculoskeletal risk. Appl. Ergon. 2009, 40, 124–135. [Google Scholar] [CrossRef] [PubMed]
- Richards, J.G. The measurement of human motion: A comparison of commercially available systems. Hum. Mov. Sci. 1999, 18, 589–602. [Google Scholar] [CrossRef]
- Kim, S.; Nussbaum, M.A. Performance evaluation of a wearable inertial motion capture system for capturing physical exposures during manual material handling tasks. Ergonomics 2013, 56, 314–326. [Google Scholar] [CrossRef]
- Plantard, P.; Shum, H.P.H.; Le Pierres, A.S.; Multon, F. Validation of an ergonomic assessment method using Kinect data in real workplace conditions. Appl. Ergon. 2017, 65, 562–569. [Google Scholar] [CrossRef]
- Marras, W.S.; Fathallah, F.A.; Miller, R.J.; Davis, S.W.; Mirka, G.A. Accuracy of a three-dimensional lumbar motion monitor for recording dynamic trunk motion characteristics. Int. J. Ind. Ergon. 1992, 9, 75–87. [Google Scholar] [CrossRef]
- Ning, X.; Zhou, J.; Dai, B.; Jaridi, M. The assessment of material handling strategies in dealing with sudden loading: The effects of load handling position on trunk biomechanics. Appl. Ergon. 2014, 45, 1399–1405. [Google Scholar] [CrossRef]
- Lloyd, D.G.; Besier, T.F. An EMG-driven musculoskeletal model to estimate muscle forces and knee joint moments in vivo. J. Biomech. 2003, 36, 765–776. [Google Scholar] [CrossRef]
- Seo, J.O.; Starbuck, R.; Han, S.; Lee, S.H.; Armstrong, T.J. Dynamic biomechanical analysis for construction tasks using motion data from vision-based motion capture approaches. In Proceedings of the Computing in Civil and Building Engineering (2014), Orlando, FL, USA, 23–25 June 2014; American Society of Civil Engineers: Reston, VA, USA, 2014; pp. 1005–1012. [Google Scholar] [CrossRef] [Green Version]
- Seo, J.; Starbuck, R.; Han, S.U.; Lee, S.H.; Armstrong, T.J. Motion data-driven biomechanical analysis during construction tasks on sites. J. Comput. Civ. Eng. 2015, 29, B4014005. [Google Scholar] [CrossRef]
- Seo, J.; Lee, S.; Armstrong, T.J.; Han, S. Dynamic biomechanical simulation for identifying risk factors for work-related musculoskeletal disorders during construction tasks. In Proceedings of the ISARC 2013—30th International Symposium on Automation and Robotics in Construction and Mining, Montreal, QC, Canada, 11–15 August 2013; pp. 1074–1084. [Google Scholar] [CrossRef] [Green Version]
- Trask, C.; Mathiassen, S.E.; Wahlström, J.; Heiden, M.; Rezagholi, M. Data collection costs in industrial environments for three occupational posture exposure assessment methods. BMC Med. Res. Methodol. 2012, 12, 89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seo, J.; Yin, K.; Lee, S. Automated Postural Ergonomic Assessment Using a Computer Vision-Based Posture Classification. In Proceedings of the Construction Research Congress 2016, San Juan, Puerto Rico, 31 May–2 June 2016; American Society of Civil Engineers: Reston, VA, USA, 2016; pp. 809–818. [Google Scholar] [CrossRef]
- Manghisi, V.M.; Uva, A.E.; Fiorentino, M.; Bevilacqua, V.; Trotta, G.F.; Monno, G. Real time RULA assessment using Kinect v2 sensor. Appl. Ergon. 2017, 65, 481–491. [Google Scholar] [CrossRef] [PubMed]
- Seo, J.O.; Han, S.U.; Lee, S.H.; Armstrong, T.J. Feasibility of on-site biomechanical analysis during ladder climbing. In Proceedings of the Construction Research Congress 2014, Atlanta, GA, USA, 19–21 May 2014; American Society of Civil Engineers: Reston, VA, USA, 2014; pp. 739–748. [Google Scholar] [CrossRef]
- Yu, Y.; Li, H.; Yang, X.; Umer, W. Estimating construction workers’ physical workload by fusing computer vision and smart insole technologies. In Proceedings of the ISARC 2018—35th International Symposium on Automation and Robotics in Construction, Berlin, Germany, 20–25 July 2018. [Google Scholar] [CrossRef]
- Olivas Padilla, B.E.; Glushkova, A.; Menychtas, D.; Manitsaris, S. Designing a web-based Automatic Ergonomic Assessment using Motion Data. In Proceedings of the 12th ACM International Conference on PErvasive Technologies Related to Assistive Environments, Rhodes, Greece, 5–7 June 2019; ACM: New York, NY, USA, 2019; pp. 528–534. [Google Scholar] [CrossRef]
- Vignais, N.; Miezal, M.; Bleser, G.; Mura, K.; Gorecky, D.; Marin, F. Innovative system for real-time ergonomic feedback in industrial manufacturing. Appl. Ergon. 2013, 44, 566–574. [Google Scholar] [CrossRef] [PubMed]
- Peppoloni, L.; Filippeschi, A.; Ruffaldi, E.; Avizzano, C.A. (WMSDs issue) A novel wearable system for the online assessment of risk for biomechanical load in repetitive efforts. Int. J. Ind. Ergon. 2014, 52, 1–11. [Google Scholar] [CrossRef]
- Yan, X.; Li, H.; Li, A.R.; Zhang, H. Wearable IMU-based real-time motion warning system for construction workers’ musculoskeletal disorders prevention. Autom. Constr. 2017, 74, 2–11. [Google Scholar] [CrossRef]
- Xsens MVN: Full 6DOF Human Motion Tracking Using Miniature Inertial Sensors. Available online: https://www.researchgate.net/profile/Per_Slycke/publication/239920367_Xsens_MVN_Full_6DOF_human_motion_tracking_using_miniature_inertial_sensors/links/0f31752f1f60c20b18000000/Xsens-MVN-Full-6DOF-human-motion-tracking-using-miniature-inertial-sensors.pdf (accessed on 12 August 2020).
- Xsens MVN: Consistent Tracking of Human Motion Using Inertial Sensing. Available online: https://www.researchgate.net/profile/Martin_Schepers/publication/324007368_Xsens_MVN_Consistent_Tracking_of_Human_Motion_Using_Inertial_Sensing/links/5ab8be2f0f7e9b68ef51f7ba/Xsens-MVN-Consistent-Tracking-of-Human-Motion-Using-Inertial-Sensing.pdf (accessed on 12 August 2020).
- Faber, G.S.; Chang, C.C.; Kingma, I.; Dennerlein, J.T.; van Dieën, J.H. Estimating 3D L5/S1 moments and ground reaction forces during trunk bending using a full-body ambulatory inertial motion capture system. J. Biomech. 2016, 49, 904–912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karatsidis, A.; Bellusci, G.; Schepers, H.; de Zee, M.; Andersen, M.; Veltink, P. Estimation of Ground Reaction Forces and Moments During Gait Using Only Inertial Motion Capture. Sensors 2016, 17, 75. [Google Scholar] [CrossRef] [Green Version]
- Eckardt, F.; Münz, A.; Witte, K. Application of a Full Body Inertial Measurement System in Dressage Riding. J. Equine Vet. Sci. 2014, 34, 1294–1299. [Google Scholar] [CrossRef]
- Carson, H.J.; Collins, D.; Richards, J. Initiating technical refinements in high-level golfers: Evidence for contradictory procedures. Eur. J. Sport Sci. 2016, 16, 473–482. [Google Scholar] [CrossRef]
- Poitras, I.; Dupuis, F.; Bielmann, M.; Campeau-Lecours, A.; Mercier, C.; Bouyer, L.; Roy, J.-S. Validity and Reliability of Wearable Sensors for Joint Angle Estimation: A Systematic Review. Sensors 2019, 19, 1555. [Google Scholar] [CrossRef] [Green Version]
- Chaffin, D.B.; Andersson, G.B.J.; Martin, B.J. Occupational Biomechanics, 4th Edition. Prof. Saf. 2006. Available online: https://www.wiley.com/en-us/Occupational+Biomechanics%2C+4th+Edition-p-9780471723431 (accessed on 12 August 2020).
- Morris, J.M.; Lucas, D.B.; Bresler, B. Role of the Trunk in Stability of the Spine. J. Bone Jt. Surg. 1961, 43, 327–351. [Google Scholar] [CrossRef]
- Gómez-Espinosa, A.; Espinosa-Castillo, N.; Valdés-Aguirre, B. Foot-Mounted Inertial Measurement Units-Based Device for Ankle Rehabilitation. Appl. Sci. 2018, 8, 2032. [Google Scholar] [CrossRef] [Green Version]
- Cho, K.K.; Chung, K.H.; Park, C.; Park, J.C.; Kim, H.S. A spatial scheduling system for block painting process in shipbuilding. CIRP Ann. Manuf. Technol. 2001, 50, 339–342. [Google Scholar] [CrossRef]
- Cho, K.K.; Sun, J.G.; Oh, J.S. Automated welding operation planning system for block assembly in shipbuilding. Int. J. Prod. Econ. 1999, 60, 203–209. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Shrout, P.E.; Fleiss, J.L. Intraclass correlations: Uses in assessing rater reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef]
- Liljequist, D.; Elfving, B.; Skavberg Roaldsen, K. Intraclass correlation—A discussion and demonstration of basic features. PLoS ONE 2019, 14, e0219854. [Google Scholar] [CrossRef] [Green Version]
- Cicchetti, D.V. Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychol. Assess. 1994, 6, 284–290. [Google Scholar] [CrossRef]
- Kadaba, M.P.; Ramakrishnan, H.K.; Wootten, M.E.; Gainey, J.; Gorton, G.; Cochran, G.V.B. Repeatability of kinematic, kinetic, and electromyographic data in normal adult gait. J. Orthop. Res. 1989, 7, 849–860. [Google Scholar] [CrossRef]
- Ford, K.R.; Myer, G.D.; Hewett, T.E. Reliability of Landing 3D Motion Analysis: Implications for Longitudinal Analyses. Med. Sci. Sport. Exerc. 2007, 39, 2021–2028. [Google Scholar] [CrossRef]
- Pini, A.; Markström, J.L.; Schelin, L. Test–retest reliability measures for curve data: An overview with recommendations and supplementary code. Sport. Biomech. 2019, 1–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cai, L.; Ma, Y.; Xiong, S.; Zhang, Y. Validity and Reliability of Upper Limb Functional Assessment Using the Microsoft Kinect V2 Sensor. Appl. Bionics Biomech. 2019, 2019, 7175240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnett, V.; Neter, J.; Wasserman, W. Applied Linear Statistical Models. J. R. Stat. Soc. Ser. A 1975, 138, 258. [Google Scholar] [CrossRef]
- Pascual, A.; Naqvi, S. An investigation of ergonomics analysis tools used in industry in the identification of work-related musculoskeletal disorders. Int. J. Occup. Saf. Ergon. 2008, 14, 237–245. [Google Scholar] [CrossRef] [Green Version]
- Waters, T.R.; Putz-Anderson, V.; Garg, A.; Fine, L.J. Revised NIOSH equation for the design and evaluation of manual lifting tasks. Ergonomics 1993, 36, 749–776. [Google Scholar] [CrossRef] [PubMed]
- Brooks, P.M. The burden of musculoskeletal disease—A global perspective. Clin. Rheumatol. 2006, 25, 778–781. [Google Scholar] [CrossRef]
- Hayashi, S.; Katsuhira, J.; Matsudaira, K.; Maruyama, H. Effect of pelvic forward tilt on low back compressive and shear forces during a manual lifting task. J. Phys. Ther. Sci. 2016, 28, 802–806. [Google Scholar] [CrossRef] [Green Version]
- Han, S.H.; Al-Hussein, M.; Al-Jibouri, S.; Yu, H. Automated post-simulation visualization of modular building production assembly line. Autom. Constr. 2012, 21, 229–236. [Google Scholar] [CrossRef]
- Golabchi, A.; Han, S.; Fayek, A.R.; Abourizk, S. Stochastic Modeling for Assessment of Human Perception and Motion Sensing Errors in Ergonomic Analysis. J. Comput. Civ. Eng. 2017, 31, 04017010. [Google Scholar] [CrossRef]
- Mehta, S.; Bastero-Caballero, R.F.; Sun, Y.; Zhu, R.; Murphy, D.K.; Hardas, B.; Koch, G. Performance of intraclass correlation coefficient (ICC) as a reliability index under various distributions in scale reliability studies. Stat. Med. 2018, 37, 2734–2752. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Postural Ergonomic Assessment | ICC | Absolute Difference | ||
|---|---|---|---|---|
| Coefficient | 95% CI | Mean ± SD | 95% CI | |
| RULA | 0.836 | (0.757, 0.885) | 0.455 ± 0.418 | (0, 1.5) |
| REBA | 0.830 | (0.736, 0.885) | 0.923 ± 0.774 | (0, 3.0) |
| RULA-Based WMSD Risk Level | Expert Raters | Total | |||
|---|---|---|---|---|---|
| Low Risk | Medium Risk | High Risk | |||
| The developed system | Low risk | 30 | 8 | 0 | 38 |
| Medium risk | 2 | 153 | 15 | 170 | |
| High risk | 0 | 10 | 82 | 92 | |
| Total | 32 | 171 | 97 | 300 | |
| REBA-Based WMSD Risk Level | Expert Raters | Total | |||
|---|---|---|---|---|---|
| Low Risk | Medium Risk | High Risk | |||
| The developed system | Low risk | 18 | 1 | 0 | 19 |
| Medium risk | 1 | 191 | 12 | 204 | |
| High risk | 0 | 11 | 66 | 77 | |
| Total | 19 | 203 | 78 | 300 | |
| Task | T1 | T2 | T3 | T4 |
|---|---|---|---|---|
| CMC (mean ± SD) | 0.896 ± 0.029 | 0.902 ± 0.031 | 0.923 ± 0.026 | 0.927 ± 0.027 |
| Relative error in percentage (mean ± SD) | 9.34% ± 2.19% | 3.42% ± 0.58% | 4.19% ± 0.46% | 3.91% ± 0.45% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, C.; Kim, W.; Zhang, Y.; Xiong, S. Development and Validation of a Wearable Inertial Sensors-Based Automated System for Assessing Work-Related Musculoskeletal Disorders in the Workspace. Int. J. Environ. Res. Public Health 2020, 17, 6050. https://doi.org/10.3390/ijerph17176050
Huang C, Kim W, Zhang Y, Xiong S. Development and Validation of a Wearable Inertial Sensors-Based Automated System for Assessing Work-Related Musculoskeletal Disorders in the Workspace. International Journal of Environmental Research and Public Health. 2020; 17(17):6050. https://doi.org/10.3390/ijerph17176050
Chicago/Turabian StyleHuang, Chunxi, Woojoo Kim, Yanxin Zhang, and Shuping Xiong. 2020. "Development and Validation of a Wearable Inertial Sensors-Based Automated System for Assessing Work-Related Musculoskeletal Disorders in the Workspace" International Journal of Environmental Research and Public Health 17, no. 17: 6050. https://doi.org/10.3390/ijerph17176050
APA StyleHuang, C., Kim, W., Zhang, Y., & Xiong, S. (2020). Development and Validation of a Wearable Inertial Sensors-Based Automated System for Assessing Work-Related Musculoskeletal Disorders in the Workspace. International Journal of Environmental Research and Public Health, 17(17), 6050. https://doi.org/10.3390/ijerph17176050