Managing Asthma and Obesity Related Symptoms (MATADORS): An mHealth Intervention to Facilitate Symptom Self-Management among Youth

 ,
, 
Abstract
1. Introduction
1.1. Significance
1.2. Asthma and Obesity
1.3. Symptom Self-Management
1.4. Motivational Enhancement (ME) and Behavioral Activation (BA)
1.5. Ecological Momentary Assessment (EMA)
1.6. Use of Technology Enhanced Interventions to Facilitate Symptom Self-Management
1.7. Theoretical Frameworks
2. Materials and Methods
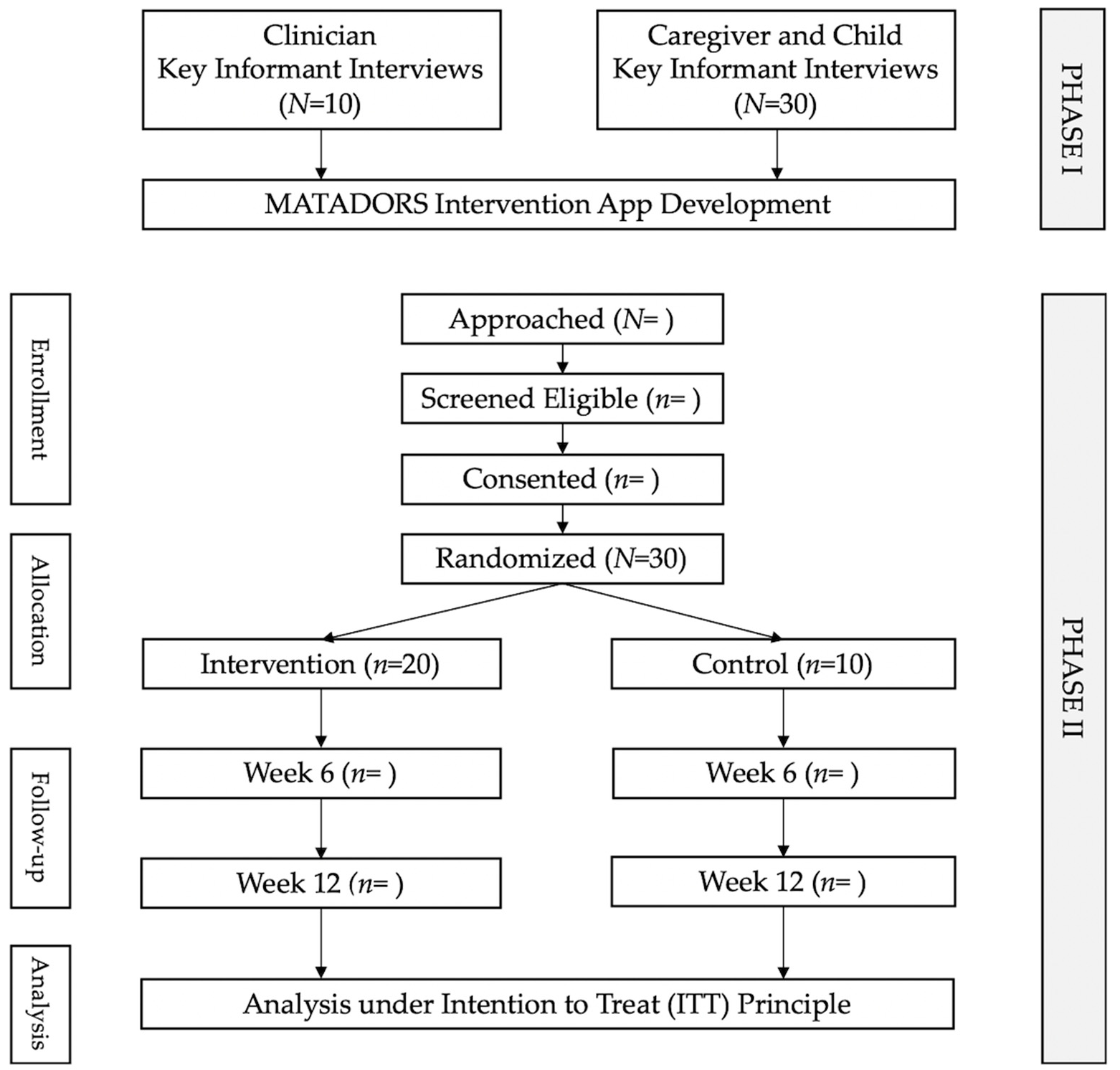
2.1. Study Design
2.1.1. Phase I
2.1.2. Phase II
2.2. Recruitment and Eligibility Criteria
- Male and female youth age 10–17 years
- Adult primary caregiver
- English speaking
- Youth diagnosis of asthma
- Youth Body Mass Index at or above the 95th percentile for age and sex based on the Centers for Disease Control (CDC) growth charts
- Inability or unwillingness of youth participant to assent and/or primary caregiver/legal guardian/representative to give informed consent.
- Inability or unwillingness to participate in the audio-recorded interview session.
- Clinical professional (Physician, nurse, nurse practitioner, dietician, or respiratory or physical therapist) involved in providing care to youth with asthma and/or obesity
- English speaking.
- Inability or unwillingness to participate in the audio-recorded interview session.
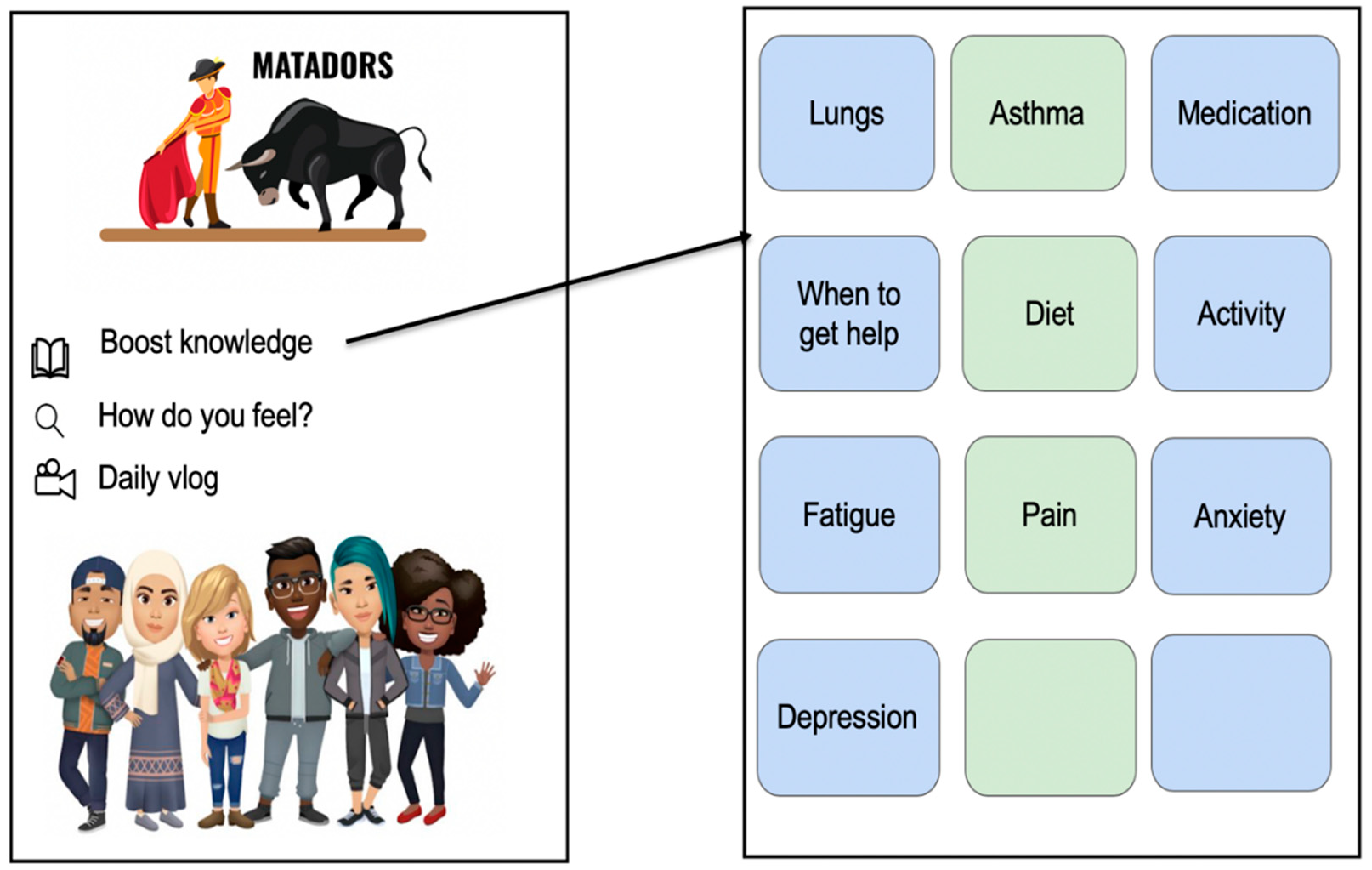
2.3. Intervention Group
2.4. Control Group
2.5. Data Collection and Measures
2.6. Data Management
2.7. Data Analysis
2.7.1. Phase I
2.7.2. Phase II
2.8. Data Safety and Monitoring
2.9. Ethical Considerations
2.10. Potential Challenges
2.11. Resource Sharing
3. Results
Progress to Date
4. Discussion
5. Conclusion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Nishtar, S.; Niinisto, S.; Sirisena, M.; Vázquez, T.; Skvortsova, V. Commissioners of the WHO Independent High-Level Commission on NCDs. Time to deliver: Report of the WHO Independent High-Level Commission on NCDs. Lancet 2018, 392, 245–252. [Google Scholar] [CrossRef]
- Clarke, R.; Heath, G.; Pattison, H.; Farrow, C. Weight-management in children living with asthma: A qualitative study of the experiences of paediatric healthcare professionals. J. Asthma 2018, 56, 1274–1281. [Google Scholar] [CrossRef]
- Alexander, G.L.; Olden, H.A.; Troy, T.; Miree, C.A.; Joseph, C.L.M. Overweight adolescents and asthma: Revealing motivations and challenges with adolescent-provider communication. J. Asthma 2018, 55, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Azizpour, Y.; Delpisheh, A.; Montazeri, Z.; Sayehmiri, K.; Darabi, B. Effect of childhood BMI on asthma: A systematic review and meta-analysis of case-control studies. BMC Pediatr. 2018, 18, 143. [Google Scholar] [CrossRef] [PubMed]
- Khalid, F.; Holguin, F. A review of obesity and asthma across the life span. J. Asthma 2018, 55, 1286–1300. [Google Scholar] [CrossRef] [PubMed]
- Heyduck, K.; Bengel, J.; Farin-Glattacker, E.; Glattacker, M. Adolescent and parental perceptions about asthma and asthma management: A dyadic qualitative analysis. Child Care Health Dev. 2015, 41, 1227–1237. [Google Scholar] [CrossRef]
- Ebell, M.H.; Marchello, C.; Meng, L.; O’Connor, J. The burden and social determinants of asthma among children in the state of Georgia. J. Community Health 2019, 44, 941–947. [Google Scholar] [CrossRef]
- Wray-Lake, L.; Crouter, A.C.; McHale, S.M. Developmental patterns in decision-making autonomy across middle childhood and adolescence: European American parents’ perspectives. Child Dev. 2010, 81, 636–651. [Google Scholar] [CrossRef]
- Modi, A.C.; Pai, A.L.; Hommel, K.A.; Hood, K.K.; Cortina, S.; E Hilliard, M.; Guilfoyle, S.M.; Gray, W.N.; Drotar, D. Pediatric self-management: A framework for research, practice, and policy. Pediatrics 2012, 129, e473–e485. [Google Scholar] [CrossRef]
- Murphy, S.L.; Xu, J.; Kochanek, K.D.; Arias, E. Mortality in the United States, 2017; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2018. Available online: www.cdc.gov/nchs/products/databriefs/db328.htm (accessed on 5 May 2019).
- Hurst, J.R.; Dickhaus, J.; Maulik, P.K.; Miranda, J.J.; Pastakia, S.D.; Soriano, J.B.; GACD Multi-morbidity Working Group. Global Alliance for Chronic Disease researchers’ statement on multimorbidity. Lancet Glob. Health 2018, 6, e1270–e1271. [Google Scholar] [CrossRef]
- Raghupathi, W.; Raghupathi, V. An empirical study of chronic diseases in the United States: A visual analytics approach to public health. Int. J. Environ. Res. Public Health 2018, 15, 431. [Google Scholar] [CrossRef] [PubMed]
- Sicouri, G.; Sharpe, L.; Hudson, J.L.; Dudeney, J.; Jaffé, A.; Selvadurai, H.; Lorimer, S.; Hunt, C. Threat interpretation and parental influences for children with asthma and anxiety. Behav. Res. Ther. 2017, 89, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Kornblit, A.; Cain, A.; Bauman, L.J.; Brown, N.M.; Reznik, M. Parental perspectives of barriers to physical activity in urban schoolchildren with asthma. Acad. Pediatr. 2018, 18, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Elliott, J.P.; Marcotullio, N.; Skoner, D.P.; Lunney, P.; Gentile, D.A. An asthma sports camp series to identify children with possible asthma and cardiovascular risk factors. J. Asthma 2014, 51, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Marko, M.; Pawliczak, R. Obesity and asthma: Risk, control and treatment. Adv. Dermatol. Allergol. 2018, 6, 563–571. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Overweight & Obesity. Childhood obesity Facts: Prevalence of Childhood Obesity in the United States. Available online: https://www.cdc.gov/obesity/data/childhood.html (accessed on 20 October 2020).
- Rank, M.; Siegrist, M.; Wilks, D.C.; Langhof, H.; Wolfarth, B.; Haller, B.; Koenig, W.; Halle, M. The cardio-metabolic risk of moderate and severe obesity in children and adolescents. J. Pediatr. 2013, 163, 137–142. [Google Scholar] [CrossRef]
- Zabarsky, G.; Beek, C.; Hagman, E.; Pierpoint, B.; Caprio, S.; Weiss, R. Impact of severe obesity on cardiovascular risk factors in youth. J. Pediatr. 2017, 192, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Appleton, A.A.; Holdsworth, E.; Ryan, M.; Tracy, M. Measuring childhood adversity in life course cardiovascular research: A systematic review. Psychosom. Med. 2017, 79, 434–440. [Google Scholar] [CrossRef] [PubMed]
- Tattersall, M.C.; Guo, M.; Korcarz, C.E.; Gepner, A.D.; Kaufman, J.D.; Liu, K.J.; Stein, J.H. Asthma predicts cardiovascular disease events: The Multi-Ethnic Study of Atherosclerosis. Arter. Thromb. Vasc. Biol. 2015, 35, 1520–1525. [Google Scholar] [CrossRef]
- Xu, M.; Xu, J.; Yang, X. Asthma and risk of cardiovascular disease or all cause mortality: A meta-analysis. Ann. Saudi Med. 2017, 37, 99–105. [Google Scholar] [CrossRef]
- Global Burden of Cardiovascular Diseases Collaboration. The burden of cardiovascular diseases among US states, 1990–2016. JAMA Cardiol. 2018, 3, 375–389. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The Top 10 Causes of Death. 2018. Available online: www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 20 October 2020).
- Calhoun, S.L.; Vgontzas, A.N.; Fernandez-Mendoza, J.; Mayes, S.D.; Tsaoussoglou, M.; Basta, M.; Bixler, E.O. Prevalence and risk factors of excessive daytime sleepiness in a community sample of young children: The role of obesity, asthma, anxiety/depression, and sleep. Sleep 2011, 34, 503–507. [Google Scholar] [CrossRef] [PubMed]
- Herring, M.P.; Monroe, D.C.; Kline, C.E.; O’Connor, P.J.; MacDonncha, C. Sleep quality moderates the association between physical activity and feelings of energy and fatigue in adolescents. Eur. Child Adolesc. Psychiatry 2018, 27, 1425–1432. [Google Scholar] [CrossRef]
- Boulet, L.-P. Asthma and obesity. Clin. Exp. Allergy 2012, 43, 8–21. [Google Scholar] [CrossRef]
- Barat, P.; Meiffred, M.-C.; Brossaud, J.; Fuchs, D.; Corcuff, J.-B.; Thibault, H.; Capuron, L. Inflammatory, endocrine and metabolic correlates of fatigue in obese children. Psychoneuroendocrinology 2016, 74, 158–163. [Google Scholar] [CrossRef]
- Kuula, L.; Pesonen, A.-K.; Martikainen, S.; Kajantie, E.; Lahti, J.; Strandberg, T.; Tuovinen, S.; Heinonen, K.; Pyhälä, R.; Lahti, M.; et al. Poor sleep and neurocognitive function in early adolescence. Sleep Med. 2015, 16, 1207–1212. [Google Scholar] [CrossRef]
- Martin, S.R.; Boergers, J.; Kopel, S.J.; McQuaid, E.L.; Seifer, R.; LeBourgeois, M.; Klein, R.B.; Esteban, C.A.; Fritz, G.K.; Koinis-Mitchell, D. Sleep hygiene and sleep outcomes in a sample of urban children with and without asthma. J. Pediatr. Psychol. 2017, 42, 825–836. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.M.; Sumar, B.; Dixon, K.A. Musculoskeletal pain in overweight and obese children. Int. J. Obes. 2014, 38, 11–15. [Google Scholar] [CrossRef]
- Mammen, J.R.; Rhee, H.; Norton, S.A.; Butz, A.M.; Halterman, J.S.; Arcoleo, K. An integrated operational definition and conceptual model of asthma self-management in teens. J. Asthma 2018, 55, 1315–1327. [Google Scholar] [CrossRef]
- Shanahan, L.; Copeland, W.E.; Worthman, C.M.; Angold, A.; Costello, E.J. Children with both asthma and depression are at risk for heightened inflammation. J. Pediatr. 2013, 163, 1443–1447. [Google Scholar] [CrossRef]
- Morrison, K.M.; Shin, S.; Tarnopolsky, M.; Taylor, V.H. Association of depression & health related quality of life with body composition in children and youth with obesity. J. Affect. Disord. 2015, 172, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Dudeney, J.; Sharpe, L.; Jaffe, A.; Jones, E.B.; Hunt, C. Anxiety in youth with asthma: A meta-analysis. Pediatr. Pulmonol. 2017, 52, 1121–1129. [Google Scholar] [CrossRef]
- Tevyaw, T.O.; Monti, P.M. Motivational enhancement and other brief interventions for adolescent substance abuse: Foundations, applications and evaluations. Addiction 2004, 99 (Suppl. 2), 63–75. [Google Scholar] [CrossRef]
- Lejuez, C.W.; Hopko, D.R.; Acierno, R.; Daughters, S.B.; Pagoto, S.L. Ten year revision of the brief behavioral activation treatment for depression: Revised treatment manual. Behav. Modif. 2011, 35, 111–161. [Google Scholar] [CrossRef] [PubMed]
- MacDonell, K.K.; Gibson-Scipio, W.; Lam, P.; Naar-King, S.; Chen, X. Text messaging to measure asthma medication use and symptoms in urban African American emerging adults: A feasibility study. J. Asthma 2012, 49, 1092–1096. [Google Scholar] [CrossRef]
- Mulvaney, S.A.; Ho, Y.; Cala, C.M.; Chen, Q.; Nian, H.; Patterson, B.L.; Johnson, K.B. Assessing adolescent asthma symptoms and adherence using mobile phones. J. Med Internet Res. 2013, 15, e141. [Google Scholar] [CrossRef]
- Teufel, R.J.; Patel, S.K.; Shuler, A.B.; Andrews, A.L.; Nichols, M.; Ebeling, M.; Dawley, E.; Mueller, M.; Ruggiero, K.J.; Treiber, F.A. Smartphones for real-time assessment of adherence behavior and symptom exacerbation for high-risk youth with asthma: Pilot study. JMIR Pediatr. Parent. 2018, 1. [Google Scholar] [CrossRef] [PubMed]
- Silver, L. Smartphone Ownership is Growing Rapidly around the World, but not Always Equally. Available online: https://www.pewresearch.org/global/2019/02/05/smartphone-ownership-is-growing-rapidly-around-the-world-but-not-always-equally/ (accessed on 20 October 2020).
- Feter, N.; Dos Santos, T.S.; Caputo, E.; Da Silva, M. What is the role of smartphones on physical activity promotion? A systematic review and meta-analysis. Int. J. Public Health 2019, 64, 679–690. [Google Scholar] [CrossRef]
- Michie, S.; Yardley, L.; West, R.; Patrick, K.; Greaves, F. Developing and evaluating digital interventions to promote behavior change in health and health care: Recommendations resulting from an international workshop. J. Med Internet Res. 2017, 19. [Google Scholar] [CrossRef]
- Yardley, L.; Spring, B.J.; Riper, H.; Morrison, L.G.; Crane, D.H.; Curtis, K.; Merchant, G.C.; Naughton, F.; Blandford, A. Understanding and promoting effective engagement with digital behavior change interventions. Am. J. Prev. Med. 2016, 51, 833–842. [Google Scholar] [CrossRef]
- O’Cathain, A.; Croot, L.; Duncan, E.; Rousseau, N.; Sworn, K.; Turner, K.M.; Yardley, L.; Hoddinott, P. Guidance on how to develop complex interventions to improve health and healthcare. BMJ Open 2019, 9, e029954. [Google Scholar] [CrossRef] [PubMed]
- Ownby, R.L.; Acevedo, A.; Waldrop-Valverde, D.; Caballero, J.; Simonson, M.; Davenport, R.; Kondwani, K.; Jacobs, R.J. A mobile app for chronic disease self-management: Protocol for a randomized controlled trial. JMIR Res. Protoc. 2017, 6, e53. [Google Scholar] [CrossRef] [PubMed]
- Glasgow, R.E.; Vogt, T.M.; Boles, S.M. Evaluating the public health impact of health promotion interventions: The RE-AIM framework. Am. J. Public Health 1999, 89, 1322–1327. [Google Scholar] [CrossRef] [PubMed]
- Liew, M.S.; Zhang, J.; See, J.; Ong, Y.L. Usability challenges for health and wellness mobile apps: Mixed-methods study among mHealth experts and consumers. JMIR mHealth uHealth 2019, 7, e12160. [Google Scholar] [CrossRef]
- Hesse-Biber, S.; Johnson, B. The Oxford Handbook of Multimethod and Mixed Methods Research Inquiry; Oxford University Press: Oxford, UK, 2015. [Google Scholar]
- Nichols, M.; Miller, S.; Treiber, F.; Ruggiero, K.; Dawley, E.; Teufel, R. Patient and parent perspectives on improving pediatric asthma self-management through a mobile health intervention: Pilot study. JMIR Form. Res. 2020, 4, e15295. [Google Scholar] [CrossRef]
- Hsieh, H.-F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- Sandelowski, M. Whatever happened to qualitative description? Res. Nurs. Health 2000, 23, 334–340. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)-A metadata-driven methodology and workforce process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- MAXQDA 2018 Analytics Pro: Qualitative & Mixed Methods Software. Available online: https://www.maxqda.com (accessed on 20 October 2020).
- IBM Corp. IBM SPSS Statistics for Macintosh, Version 25.0; IBM Corp: Armonk, NY, USA.
- Lv, S.; Ye, X.; Wang, Z.; Xia, W.; Qi, Y.; Wang, W.; Chen, Y.; Cai, X.; Qian, X. A randomized controlled trial of a mobile application-assisted nurse led model used to improve treatment outcomes in children with asthma. J. Adv. Nurs. 2019, 75, 3058–3067. [Google Scholar] [CrossRef]
- Fedele, D.; Lucero, R.J.; Janicke, D.; Abu-Hasan, M.; McQuaid, E.L.; Moon, J.K.; Fidler, A.; Wallace-Farquharson, T.; Lindberg, D.; Duncan, C.; et al. Protocol for the Development of a Behavioral Family Lifestyle Intervention Supported by Mobile Health to Improve Weight Self-Management in Children With Asthma and Obesity. JMIR Res. Protoc. 2019, 8, e13549. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Timepoint | Study Period | ||||
|---|---|---|---|---|---|
| Enrollment | Allocation | Post-Allocation | |||
| Baseline | Day 1 | Week 6 | Week 12 (Close Out) | ||
| Phase I | |||||
| Caregiver and child dyad enrollment | |||||
| Eligibility screening checklist | X | ||||
| Informed consent | X | ||||
| Assessments | X | ||||
| Demographics | X | ||||
| Short Assessment of Health Literacy-English (SAHL-E) | X | ||||
| Key Informant Interview | X | ||||
| Clinician enrollment | |||||
| Eligibility screening checklist | X | ||||
| Key Informant Interview | X | ||||
| Phase II | |||||
| Child enrollment | |||||
| Eligibility screening checklist | X | ||||
| Informed consent | X | ||||
| Allocation (2-1 randomization) | X | X | |||
| Interventions | |||||
| Matadors (intervention) | X | X | |||
| Enhanced Usual Care (control) | X | X | |||
| Assessments and measures | |||||
| Demographics and characteristics | X | ||||
| Short Assessment of Health Literacy-English (SAHL-E) | X | ||||
| Asthma Control Test (ACT) | X | X | X | ||
| Asthma Belief Scale | X | X | X | ||
| PROMIS Pediatric Depressive Symptoms 8a | X | X | X | ||
| PROMIS Pediatric Anxiety 8a | X | X | X | ||
| PROMIS Pediatric Pain Interference | X | X | X | ||
| PROMIS Pediatric Fatigue 10a | X | X | X | ||
| Neuro Quality of Life-Pain | X | X | X | ||
| Neuro Quality of Life-Fatigue | X | X | X | ||
| Self-Efficacy for Managing Chronic Disease-6 item | X | X | X | ||
| Fitbit physical activity tracker | X | X | |||
| Program satisfaction survey | X | ||||
| Semi-structured interview | X | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nichols, M.; Teufel, R.; Miller, S.; Madisetti, M.; Giovanni, C.S.; Chike-Harris, K.; Jones, L.; Prentice, M.; Ruggiero, K.; Kelechi, T. Managing Asthma and Obesity Related Symptoms (MATADORS): An mHealth Intervention to Facilitate Symptom Self-Management among Youth. Int. J. Environ. Res. Public Health 2020, 17, 7750. https://doi.org/10.3390/ijerph17217750
Nichols M, Teufel R, Miller S, Madisetti M, Giovanni CS, Chike-Harris K, Jones L, Prentice M, Ruggiero K, Kelechi T. Managing Asthma and Obesity Related Symptoms (MATADORS): An mHealth Intervention to Facilitate Symptom Self-Management among Youth. International Journal of Environmental Research and Public Health. 2020; 17(21):7750. https://doi.org/10.3390/ijerph17217750
Chicago/Turabian StyleNichols, Michelle, Ronald Teufel, Sarah Miller, Mohan Madisetti, Christine San Giovanni, Katherine Chike-Harris, Lacy Jones, Margaret Prentice, Kenneth Ruggiero, and Teresa Kelechi. 2020. "Managing Asthma and Obesity Related Symptoms (MATADORS): An mHealth Intervention to Facilitate Symptom Self-Management among Youth" International Journal of Environmental Research and Public Health 17, no. 21: 7750. https://doi.org/10.3390/ijerph17217750
APA StyleNichols, M., Teufel, R., Miller, S., Madisetti, M., Giovanni, C. S., Chike-Harris, K., Jones, L., Prentice, M., Ruggiero, K., & Kelechi, T. (2020). Managing Asthma and Obesity Related Symptoms (MATADORS): An mHealth Intervention to Facilitate Symptom Self-Management among Youth. International Journal of Environmental Research and Public Health, 17(21), 7750. https://doi.org/10.3390/ijerph17217750