
Telemedicine Treatment and Care for Patients with Intellectual Disability





Abstract
1. Introduction
2. Methods
3. Telemedicine Applications for People with Intellectual Disabilities
4. Telemedicine among People with Intellectual Disabilities during the COVID-19 Pandemic
5. Experiences of the Berlin Treatment Center for Health in Patients with Developmental Disabilities during the COVID-19 Pandemic
6. The Use of Telemedicine among People with Intellectual Disabilities in Different Health Conditions
7. Risks Related to the Use of Telemedicine in People with Intellectual Disabilities
8. Limitations of Studies on the Use of Telemedicine in People with Intellectual Disabilities
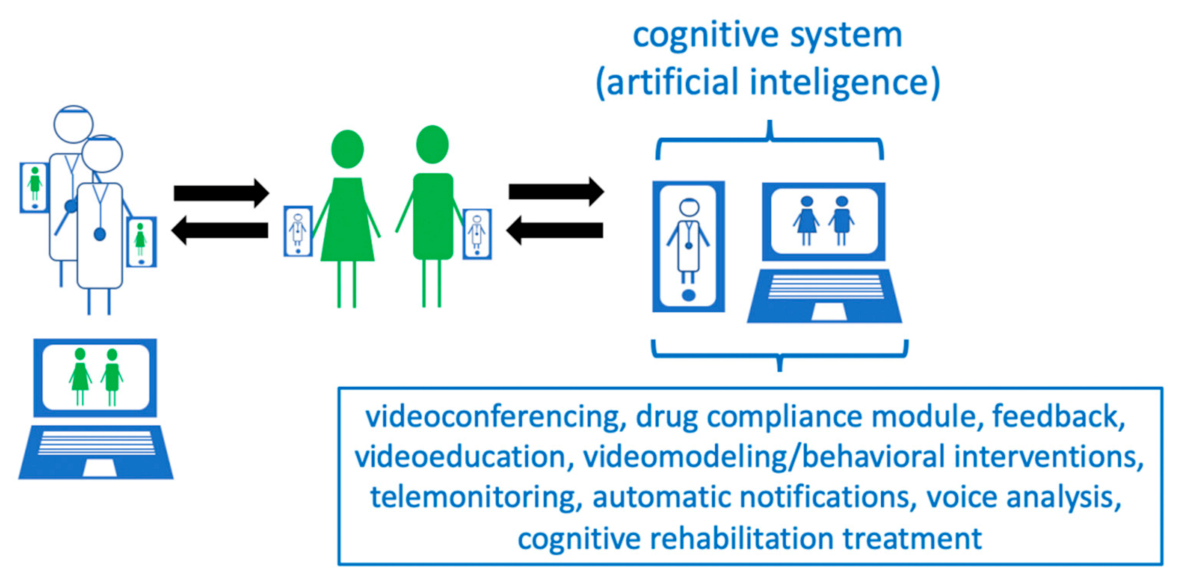
9. The New Vision of the Application for People with Intellectual Disabilities
- -
- Pharmacological treatment with feedback function, given by the caregiver; information correlating drug use with their effectiveness can be collected in a database.
- -
- Behavioral interventions programmed by a behavioral psychotherapist, the effectiveness of which can, as in the case of pharmacological interventions, be assessed and introduced into the system by the caregiver.
- -
- Video interviews, enabling remote contact of the therapist with the patient and his/her caregiver.
- -
- A voice analysis module, recording the patient’s voice and providing feedback for the system to correlate it with the effectiveness of pharmacological and behavioral interventions.
- -
- A video recording module that allows for the analysis of the patient’s kinetics and facial expressions, enabling the caregiver to record the behavior of a person, which can be analyzed by the telemedicine system, providing the system with further medical data.
- -
- Cognitive training, which may be based on simple mobile or computer games, which may, on the one hand, support cognition and, on the other hand, provide relaxation and be an effective strategy for dealing with negative emotions and behaviors.
10. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Public Health England. People with Learning Disabilities in England 2015: Main Report; Public Health England: London, UK, 2016. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5), 5th ed.; American Psychiatric Pub: Washington, DC, USA, 2013. [Google Scholar]
- Sheehan, R.; Hassiotis, A. Digital mental health and intellectual disabilities: State of the evidence and future directions. Evid. Based Ment. Health 2017, 20, 107–111. [Google Scholar] [CrossRef] [PubMed]
- Ofcom. Communications Market Report 2016. Available online: https://www.ofcom.org.uk/ research-and-data/multi-sector-research/cmr/cmr16/the-communications-marketreport-uk (accessed on 10 May 2017).
- Carey, A.C.; Friedman, M.G.; Bryen, D.N.; Taylor, S.J. Use of electronic technologies by people with intellectual disabilities. Ment. Retard. 2005, 43, 322–333. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Recacha, P.; Martorell-Cafranga, A. People with intellectual disability and ICTs. Rev. Comun. 2011, 18, 173–180. [Google Scholar] [CrossRef]
- Chadwick, D.; Wesson, C.; Fullwood, C. Internet access by people with intellectual disabilities: Inequalities and opportunities. Future Internet 2013, 5, 376–397. [Google Scholar] [CrossRef]
- Cullen, R. Addressing the digital divide. Online Inform. Rev. 2001, 25, 311–320. [Google Scholar] [CrossRef]
- Li-Tsang, C.W.; Lee, M.Y.; Yeung, S.S.; Siu, A.M.; Lam, C.S. A 6-month follow-up of the effects of an information and communication technology (ICT) training programme on people with intellectual disabilities. Res. Dev. Disabil. 2007, 28, 559–566. [Google Scholar] [CrossRef]
- Davies, D.K.; Stock, S.E.; Wehmeyer, M.L. Computer-mediated, self-directed computer training and skill assessment for individuals with mental retardation. J. Dev. Phys. Disabil. 2004, 16, 95–105. [Google Scholar] [CrossRef]
- Holburn, S.; Nguyen, D.; Vietze, P.M. Computer-assisted learning for adults with profound multiple disabilities. Behav. Interv. 2004, 19, 25–37. [Google Scholar] [CrossRef]
- Caton, S.; Chapman, M. The use of social media and people with intellectual disability: A systematic review and thematic analysis. J. Intellect. Dev. Disabil. 2016, 41, 125–139. [Google Scholar] [CrossRef]
- Weiss, P.L.; Bialik, P.; Kizony, R. Virtual reality provides leisure time opportunities for young adults with physical and intellectual disabilities. Cyberpsychol. Behav. 2003, 6, 335–342. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira Malaquias, F.F.; Malaquias, R.F.; Lamounier, E.A., Jr.; Cardoso, A. VirtualMat: A serious game to teach logical-mathematical concepts for students with intellectual disability. Technol. Disabil. 2013, 25, 107–116. [Google Scholar] [CrossRef]
- Lotan, M.; Yalon-Chamovitz, S.; Weiss, P.L. Virtual reality as means to improve physical fitness of individuals at a severe level of intellectual and developmental disability. Res. Dev. Disabil. 2010, 31, 869–874. [Google Scholar] [CrossRef] [PubMed]
- Story, M.F.; Mueller, J.L.; Mace, R.L. The Universal Design File: Designing for People of All Ages and Abilities; NC State University: Raleigh, NC, USA, 1998. [Google Scholar]
- Standen, P.J.; Brown, D.J. Virtual reality and its role in removing the barriers that turn cognitive impairments into intellectual disability. Virtual Real. 2006, 10, 241–252. [Google Scholar] [CrossRef]
- Salgado, T.M.; Fedrigon, A.; Omichinski, D.R.; Meade, M.A.; Farris, K.B. Identifying Medication Management Smartphone App Features Suitable for Young Adults With Developmental Disabilities: Delphi Consensus Study. JMIR mHealth uHealth 2018, 6, e129. [Google Scholar] [CrossRef]
- Ptomey, L.T.; Willis, E.A.; Greene, J.L.; Danon, J.C.; Chumley, T.K.; Washburn, R.A.; Donnelly, J.E. The Feasibility of Group Video Conferencing for Promotion of Physical Activity in Adolescents With Intellectual and Developmental Disabilities. Am. J. Intellect. Dev. Disabil. 2017, 122, 525–538. [Google Scholar] [CrossRef] [PubMed]
- Taber-Doughty, T.; Shurr, J.; Brewer, J.; Kubik, S. Standard care and telecare services: Comparing the effectiveness of two service systems with consumers with intellectual disabilities. J. Intellect. Disabil. Res. 2010, 54, 843–859. [Google Scholar] [CrossRef] [PubMed]
- Szeftel, R.; Federico, C.; Hakak, R.; Szeftel, Z.; Jacobson, M. Improved access to mental health evaluation for patients with developmental disabilities using telepsychiatry. J. Telemed. Telecare 2012, 18, 317–321. [Google Scholar] [CrossRef] [PubMed]
- Annaswamy, T.M.; Verduzco-Gutierrez, M.; Frieden, L. Telemedicine barriers and challenges for persons with disabilities: COVID-19 and beyond. Disabil. Health J. 2020, 13, 100973. [Google Scholar] [CrossRef]
- Bhaskar, S.; Bradley, S.; Chattu, V.K.; Adisesh, A.; Nurtazina, A.; Kyrykbayeva, S.; Sakhamuri, S.; Yaya, S.; Sunil, T.; Thomas, P.; et al. Telemedicine Across the Globe-Position Paper From the COVID-19 Pandemic Health System Resilience PROGRAM (REPROGRAM) International Consortium (Part 1). Front. Public Health 2020, 8, 556720. [Google Scholar] [CrossRef]
- Jeste, S.; Hyde, C.; Distefano, C.; Halladay, A.; Ray, S.; Porath, M.; Wilson, R.B.; Thurm, A. Changes in access to educational and healthcare services for individuals with intellectual and developmental disabilities during COVID-19 restrictions. J. Intellect. Disabil. Res. 2020, 64, 825–833. [Google Scholar] [CrossRef]
- Zaagsma, M.; Volkers, K.M.; Swart, E.A.K. The use of online support by people with intellectual disabilities living independently during COVID-19. J. Intellect. Disabil. Res. 2020, 64, 750–756. [Google Scholar] [CrossRef]
- Cooper, S.A.; Smiley, E.; Morrison, J.; Williamson, A.; Allan, L. Mental ill-health in adults with intellectual disabilities: Prevalence and associated factors. Br. J. Psychiatry 2007, 190, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Vereenooghe, L.; Gega, L.; Langdon, P.E. Intellectual disability and computers in therapy: Views of service users and clinical psychologists. Cyberpsychology 2017, 11, 1–11. [Google Scholar] [CrossRef]
- Cooney, P.; Jackman, C.; Coyle, D.; O’Reilly, G. Computerised cognitive-behavioural therapy for adults with intellectual disability: Randomised controlled trial. Br. J. Psychiatry 2017, 211, 95–102. [Google Scholar] [CrossRef]
- O’Reilly, G.; Cooney, P.; Jackman, C.; Coyle, D. Pesky Gnats: The Feel Good Island. A CBT Computer Game to Assist Adults Who Have an Intellectual Disability with Anxiety or Depression; Handaxe Community Interest Company: Bristol, UK, 2015. [Google Scholar]
- Wentzel, J.; van der Vaart, R.; Bohlmeijer, E.T.; van Gemert-Pijnen, J.E. Mixing online and face-to-face therapy: How to benefit from blended care in mental health care. JMIR Ment. Health 2016, 3, e9. [Google Scholar] [CrossRef] [PubMed]
- Emerson, E. Challenging Behaviour: Analysis and Intervention in People with Learning Disabilities; Cambridge University Press: Cambridge, UK, 1995. [Google Scholar]
- National Center on Secondary Education and Transition. Parent Brief: Promoting Effective Parent Involvement in Secondary Education and Transition. February 2006. Available online: http://www.ncset.org/publications/viewdesc.asp?id=2967 (accessed on 20 December 2020).
- Reichard, A.; Stolzle, H.; Fox, M.H. Health disparities among adults with physical disabilities or cognitive limitations compared to individuals with no disabilities in the United States. Disabil. Health J. 2011, 4, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Rimmer, J.H.; Yamaki, K.; Lowry, B.M.; Wang, E.; Vogel, L.C. Obesity and obesity-related secondary conditions in adolescents with intellectual/developmental disabilities. J. Intellect. Disabil. Res. 2010, 54, 787–794. [Google Scholar] [CrossRef]
- Emerson, E. Health status and health risks of the “hidden majority” of adults with intellectual disability. Intellect. Dev. Disabil. 2011, 49, 155–165. [Google Scholar] [CrossRef]
- Stancliffe, R.J.; Larkin, K.C.; Larson, S.A.; Engler, J.; Taub, S.; Fortune, J.; Bershadsky, J. Demographic characteristics, health conditions, and residential service use in adults with Down Syndrome in 25 U.S. States. Intellect. Dev. Disabil. 2012, 40, 92–108. [Google Scholar] [CrossRef] [PubMed]
- Ozaki, R.R.; Schneider, J.I.; Hall, J.P.; Moore, J.M.; Linkins, K.W.; Brya, J.J.; Oelschlaeger, A.; Bohman, T.; Christensen, K.; Wallisch, L.; et al. Personal navigation, life coaching, and case management: Approaches for enhancing health and employment services. J. Vocat. Rehabil. 2011, 34, 83–95. [Google Scholar] [CrossRef]
- Marks, B.; Sisirak, J.; Heller, T. Health Matters: The Exercise and Nutrition Health Education Curriculum for People with Developmental Disabilities; Paul Brooks: Baltimore, MD, USA, 2010. [Google Scholar]
- Kagohara, D.M.; Van der Meer, L.; Ramdoss, S.; O’Reilly, M.F.; Lancioni, G.E.; Davis, T.N.; Rispoli, M.; Lang, R.; Marschik, P.B.; Sutherland, D.; et al. Using iPods and iPads in teaching programs for individuals with developmental disabilities: A systematic review. Res. Dev. Disabil. 2013, 34, 147–156. [Google Scholar] [CrossRef]
- Pontow, I.; Theil, J.; Diefenbacher, A. Comorbidity of hypoglycemia anxiety and panic disorder in a patient with type-1 diabetes—Combined treatment with cognitive—behavioral therapy and Continuous Glucose Monitoring (CGM) in a psychosomatic day-treatment center. Dtsch. Med. Wochenschr. 2020, 145, 1–4. [Google Scholar] [CrossRef]
- Haymes, L.K.; Storey, K.; Maldonado, A.; Post, M.; Montgomery, J. Using applied behavior analysis and smart technology for meeting the health needs of individuals with intellectual disabilities. Dev. Neurorehabil. 2015, 18, 407–419. [Google Scholar] [CrossRef]
- Charlop, M.H.; Milstein, J.P. Teaching autistic children conversational speech using video modeling. J. Appl. Behav. Anal. 1989, 22, 275–285. [Google Scholar] [CrossRef] [PubMed]
- Charlop, M.H.; Dennis, B.; Carpenter, M.H.; Greenberg, A.L. Teaching socially expressive behaviors to children with autism through video modeling. Educ. Treat. Child. 2010, 33, 371–393. [Google Scholar] [CrossRef]
- Geiger, K.B.; LeBlanc, L.A.; Dillon, C.M.; Bates, S.L. An evaluation of preference for video and in vivo modeling. J. Appl. Behav. Anal. 2010, 43, 279–383. [Google Scholar] [CrossRef]
- Sherer, M.; Pierce, K.L.; Paredes, S.; Kisacky, K.L.; Ingersoll, B.; Schreibman, L. Enhancing conversation skills in children with autism via video technology. Which is better, “self” or “other” as a model? Behav. Modif. 2001, 25, 140–158. [Google Scholar] [CrossRef] [PubMed]
- Ben-Pazi, H.; Beni-Adani, L.; Lamdan, R. Accelerating Telemedicine for Cerebral Palsy During the COVID-19 Pandemic and Beyond. Front. Neurol. 2020, 11, 746. [Google Scholar] [CrossRef]
- Autism Speaks. COVID-19 (Coronavirus) Information and Resources. Available online: https://www.autismspeaks.org/covid-19-information-and-resources (accessed on 20 December 2020).
- Bhaskar, S.; Bradley, S.; Israeli-Korn, S.; Menon, B.; Chattu, V.K.; Thomas, P.; Chawla, J.; Kumar, R.; Prandi, P.; Ray, D.; et al. Chronic Neurology in COVID-19 Era: Clinical Considerations and Recommendations from the REPROGRAM Consortium. Front. Neurol. 2020, 11, 664. [Google Scholar] [CrossRef] [PubMed]
- Pictograms for People with Learning Disabilities and Caregivers (In German). Available online: www.keh-berlin.de>Fachabteilungen>Behandlungszentrum für psychische Gesundheit bei Entwicklungsstörungen (Intelligenzminderung) (accessed on 17 December 2020).
- Lough, E.; Fisher, M. Internet use and online safety in adults with Williams syndrome. J. Intellect. Disabil. Res. 2016, 60, 1020–1030. [Google Scholar] [CrossRef]
- Huckvale, K.; Prieto, J.T.; Tilney, M.; Benghozi, P.J.; Car, J. Unaddressed privacy risks in accredited health and wellness apps: A cross-sectional systematic assessment. BMC Med. 2015, 13, 214. [Google Scholar] [CrossRef]
- Vázquez, A.; Jenaro, C.; Flores, N.; Bagnato, M.J.; Pérez, M.C.; Cruz, M. E-Health Interventions for Adult and Aging Population With Intellectual Disability: A Review. Front. Psychol. 2018, 9, 2323. [Google Scholar] [CrossRef] [PubMed]
- Madhavan, G. Telepsychiatry in intellectual disability psychiatry: Literature review. BJPsych Bull. 2019, 43, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Krysta, K.; Krzystanek, M.; Cubała, W.J.; Wiglusz, M.S.; Jakuszkowiak-Wojten, K.; Gałuszko-Węgielnik, M.; Czarnowska-Cubała, M.; Szarmach, J.; Włodarczyk, A.; Janas-Kozik, M. Telepsychiatry and virtual reality in the treatment of patients with intellectual and developmental disabilities. Psychiatr. Danub. 2017, 29, 656–659. [Google Scholar] [PubMed]
- Bhaskar, S.; Bradley, S.; Sakhamuri, S.; Moguilner, S.; Chattu, V.K.; Pandya, S.; Schroeder, S.; Ray, D.; Banach, M. Designing Futuristic Telemedicine Using Artificial Intelligence and Robotics in the COVID-19 Era. Front. Public Health 2020, 8, 556789. [Google Scholar] [CrossRef]


{kind=link}
| Authors | Year | n | Characteristics of Participants | Intervention Used | Results | Conclusions |
|---|---|---|---|---|---|---|
| Salgado T. et al. [18] | 2018 | 52 | Patients with developmental disabilities and their caregivers as well as specialists in the field of intellectual disability. | Based on the available functions in telemedicine applications (42 functions grouped into 4 modules (drug list, drug reminder, drug administration record and additional functions)), the respondents were to come to a consensus as to the most preferred ones for controlling drug intake. Consensus for the first, second and third rounds was defined as ≥90%, ≥80%, and ≥75% agreement, respectively. | In addition to the drug list, medication reminders, and drug administration recording functions, it was shown that experts selected three of the most important additional functions: automatic drug refilling in pharmacies; the ability to share information about drugs from the application with suppliers; and the ability to share information about drugs from the application with family, friends and caregivers. | Telemedicine applications containing the indicated functions may be effective in the care of patients with intellectual disabilities. |
| Ptomey L. et al. [19] | 2017 | 31 | An intervention study involving adolescents with developmental and intellectual disabilities. | The subjects participated in 30 min group sessions of physical activity 3 times a week. Classes were held at their homes through videoconferences on a tablet computer for 12 weeks. | Thirty-one patients enrolled and 29 completed the 12-week intervention. Participants participated in 77.2% ± 20.8% of scheduled sessions with an average of 26.7 ± 2.8 min PA/session, with 11.8 ± 4.8 min at moderate to high intensity. | The use of telemedicine techniques may enable increased physical activity in patients with developmental and intellectual disabilities. |
| Taber-Doughty T. et al. [20] | 2010 | 4 | Clinical trial in patients with intellectual disability. | Traditional care and teleconsultation took place alternately for 6 weeks. The subjects were to perform specific tasks, such as addressing the envelope, cooking pudding, brewing tea, etc. Teleconsultation was conducted using the Voice over Internet Protocol (VoIP) protocol, which provided audio communication over the Internet. | It has been shown that the use of tele-visits, despite the fact that it extended the time of task completion, increased the independence of the respondents. | The use of telemedicine techniques may increase the independence of patients with intellectual disabilities in performing daily activities. |
| Proved telemedicine functionality in care of people with mental disability; communication with the doctor via electronic devices |
| Proved Telemedicine Functionality in Care of People with Intellectual Disability |
|
| Proved telemedicine functionality in care of people with specific conditions |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krysta, K.; Romańczyk, M.; Diefenbacher, A.; Krzystanek, M. Telemedicine Treatment and Care for Patients with Intellectual Disability. Int. J. Environ. Res. Public Health 2021, 18, 1746. https://doi.org/10.3390/ijerph18041746
Krysta K, Romańczyk M, Diefenbacher A, Krzystanek M. Telemedicine Treatment and Care for Patients with Intellectual Disability. International Journal of Environmental Research and Public Health. 2021; 18(4):1746. https://doi.org/10.3390/ijerph18041746
Chicago/Turabian StyleKrysta, Krzysztof, Monika Romańczyk, Albert Diefenbacher, and Marek Krzystanek. 2021. "Telemedicine Treatment and Care for Patients with Intellectual Disability" International Journal of Environmental Research and Public Health 18, no. 4: 1746. https://doi.org/10.3390/ijerph18041746
APA StyleKrysta, K., Romańczyk, M., Diefenbacher, A., & Krzystanek, M. (2021). Telemedicine Treatment and Care for Patients with Intellectual Disability. International Journal of Environmental Research and Public Health, 18(4), 1746. https://doi.org/10.3390/ijerph18041746