Abstract
Background: The COVID-19 pandemic has had global effects; cases have been counted in the tens of millions, and there have been over two million deaths throughout the world. Health systems have been stressed in trying to provide a response to the increasing demand for hospital beds during the different waves. This paper analyzes the dynamic response of the hospitals of the Community of Madrid (CoM) during the first wave of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic in the period between 18 March and 31 May 2020. The aim was to model the response of the CoM’s health system in terms of the number of available beds. Methods: A research design based on a case study of the CoM was developed. To model this response, we use two concepts: “bed margin” (available beds minus occupied beds, expressed as a percentage) and “flexibility” (which describes the ability to adapt to the growing demand for beds). The Linear Hinges Model allowed a robust estimation of the key performance indicators for capturing the flexibility of the available beds in hospitals. Three new flexibility indicators were defined: the Average Ramp Rate Until the Peak (ARRUP), the Ramp Duration Until the Peak (RDUP), and the Ramp Growth Until the Peak (RGUP). Results: The public and private hospitals of the CoM were able to increase the number of available beds from 18,692 on 18 March 2020 to 23,623 on 2 April 2020. At the peak of the wave, the number of available beds increased by 160 in 48 h, with an occupancy of 90.3%. Within that fifteen-day period, the number of COVID-19 inpatients increased by 200% in non-intensive care unit (non-ICU) wards and by 155% in intensive care unit (ICU) wards. The estimated ARRUP for non-ICU beds in the CoM hospital network during the first pandemic wave was 305.56 beds/day, the RDUP was 15 days, and the RGUP was 4598 beds. For the ICU beds, the ARRUP was 36.73 beds/day, the RDUP was 20 days, and the RGUP was 735 beds. This paper includes a further analysis of the response estimated for each hospital. Conclusions: This research provides insights not only for academia, but also for hospital management and practitioners. The results show that not all of the hospitals dealt with the sudden increase in bed demand in the same way, nor did they provide the same flexibility in order to increase their bed capabilities. The bed margin and the proposed indicators of flexibility summarize the dynamic response and can be included as part of a hospital’s management dashboard for monitoring its behavior during pandemic waves or other health crises as a complement to other, more steady-state indicators.
1. Introduction
When severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was first discovered in Wuhan (China) in December 2019, even the most qualified experts did not anticipate that it would rapidly spread to create the worst global public health crisis since the 1918 flu pandemic [1]. The total number of COVID-19 cases in the world is counted in the tens of millions, with deaths in over two million cases. It is well known that emerging viral pandemics “can place extraordinary and sustained demands on public health and healthcare systems and on providers of essential community services” [2]. A crisis such as the current COVID-19 pandemic is a dramatic event, which takes place in a difficult environment with enormous emotional tension, coupled with a serious disproportion between needs and available resources. In these circumstances, managing healthcare services is a constant and changing challenge [3]. Therefore, flexibility in the usage of hospital beds is a crucial element for efficiently organizing critical capacity [4]. In Spain, as in many other countries, in the spring of 2020, COVID-19 produced such a significant number of seriously ill patients that the healthcare system almost collapsed. In some of its Autonomous Communities (ACs), particularly in the Autonomous Community of Madrid (CoM), where the capital of Spain (Madrid city) is located, the situation was especially pronounced.
Thus, on 31 March, at least 450,611 cases had been reported in Europe. The CoM registered a cumulative incidence in the previous 14 days of 363.22 and Spain registered 192.3, followed by Italy (122.2), Belgium (103), France (56.6), and the UK (40). The accumulated cases in the CoM were 29,840, 29% those of all of Spain (102.136). The highest fatality rate in Europe was in Italy (11.7), followed by Spain with 8.9, while in the CoM, it reached 13 (46% higher). In the CoM, the deaths per 100,000 inhabitants amounted to 57.7, tripling that of Spain (17.3), which was followed by Belgium (14.8), Italy (13.4), France (6.24), and the UK (5.6). The accumulated deaths in the CoM (3865) represented 42.7% of those registered in Spain (9053) [5,6]. If we look at the situation of beds in the CoM’s hospitals to describe their evolution, which is the main objective of this paper, it can be seen that the number of patients hospitalized just for COVID-19 in the intensive care units (ICUs) was 1514, and 13,713 patients were in beds other than intensive care (non-ICU). However, the situation can be described even better by comparing the figures of the CoM beds with those of Spain: 5872 (ICU) and 45,546 (non-ICU) [5]; Italy: 4023 (ICU) and 32,215 (non-ICU); France: 5496 (ICU) and 22,672 (non-ICU); and Belgium: 1088 (ICU) and 4989 (non-ICU) [7].
Due to the need to hospitalize a huge number of COVID-19 patients, which increased relentlessly with different degrees of severity during this first wave, the CoM’s hospitals rapidly increased their capacity to levels never seen before. Not only the number of hospital beds, but also the intensive support and invasive ventilation were of concern, as COVID-19 is a disease with a potentially fatal evolution. These circumstances meant that the number of available beds had to be increased from 18,692 (18 March 2020) to 23,623 (2 April 2020) in just 15 days, i.e., an increment of 26.4%. Although the first admission for COVID-19 in a CoM hospital occurred on 25 February 2020, in this paper, we analyze the data for the period between 18 March 2020 and 31 May 2020. The first date corresponds to the first day on which we had the complete data of the hospitals that are analyzed in this article.
The COVID-19 pandemic, as mentioned above, forced the CoM’s hospitals to increase the number of available beds. Given the shortage of papers in the world on the capacities of hospitals to increase their numbers of beds with the speed required by a pandemic wave, the aim of this article is to set dynamic performance indicators in order to model the dynamic response in terms of the number of available beds instead of using more stationary approaches. For this purpose, not only are specific visualization graphs used to show the daily evolution of the variables under consideration, such as the bed margin of the CoM’s hospitals, but a new set of indexes for quantifying their flexibility and a robust estimation method are proposed. Thus, the proposed approach to analyzing and quantifying the dynamics related to flexibility could be used for further analysis and as a reference for decision making not only at the hospital level, but also from a centralized or global perspective.
The remainder of this paper is structured as follows. Section 2 describes the materials and methods, and it is composed of three parts: (i) the healthcare system of the hospital network in the CoM; (ii) the data and the variables used in our study; and (iii) the methodology, where the proposed concepts of the bed margin and flexibility are defined. The results are presented in Section 3, first as an aggregate view of the healthcare system, and second as disaggregated view by hospital. Finally, Section 4 contains a discussion of the results, and conclusions and directions for future work are provided in Section 5.
2. Materials and Methods
2.1. The Hospital Network in the CoM
The Spanish National Health System (Sistema Nacional de Salud, SNS) is organized at two levels: national and regional. Its structure is a mirror of the administrative division of the country, i.e., the healthcare competences are transferred to the 17 ACs. The main actors in the ACs are the Departments of Health (Consejerías de Sanidad, CSs), which fulfill the role of a health authority, that is, healthcare delivery, regulation, planning, budgeting, and third-party payment. Above the CSs is the Spanish Ministry of Health, whose fundamental role, according to the law, is the coordination of the 17 CSs (through a collegiate body) and the publication of standards or laws that are mandatory throughout the SNS. In practice, CSs act with enormous autonomy, and there is little tradition of coordination among them [8].
The CoM’s public hospital network is made up of 34 hospitals, which are classified according to the degree of complexity of the medical procedures they offer (e.g., transplants, heart surgery, neurosurgery, radiotherapy, special treatments, etc.) into levels of high, medium, and low complexity, but only 28 of them were considered [9]. The other six are not acute-care general hospitals; therefore, they are of little interest for this study. However, we included a field hospital, Hospital IFEMA (HIFEMA), which began operating on 22 March 2020 and closed on 1 May 2020. In the CoM, although citizens can choose their public hospital and their primary care center, they are assigned a referral hospital depending on the geographic area in which they live. Furthermore, the referral hospitals of the primary care centers are the same as those of the patients under their care. Consequently, when citizens have to be hospitalized, they go to their referral hospital because of its proximity and, as in many cases, because they have been treated there on previous occasions. This explains why, if the geographical area that depends on a hospital has a high incidence of cases that require hospitalization, the hospital in question has a high occupancy.
In the period analyzed in this study, 33 private hospitals in the CoM also admitted COVID-19 patients, although for the purposes of this analysis, all of them were considered as a single hospital (HPRIVATE). This was due to the difference in the number of beds with respect to public hospitals (on 18 March 2020: 5885 vs. 12,807). This was also due to the fact that many of them were monographic hospitals and, above all, because hospital occupancy data were received aggregated as a group during most of the study period. Table 1 shows the main characteristics of the hospitals considered within this study. Note that the numbers of non-ICU and ICU beds were included as a mere reference of the sizes of the hospitals.

Table 1.
List of the Community of Madrid’s (CoM’s) hospitals and their main characteristics.
The Community of Madrid (CoM) is located in the center of Spain, with 6.7 million inhabitants. The population density varies within the community itself, with the vast majority of the population concentrated in the capital, Madrid, and its metropolitan area, making it one of the most densely populated regions in Europe. The population of Madrid, according to the latest 2019 census [10], is approximately 3.3 million. These inhabitants are concentrated in an area of 600 square kilometers. Thus, the population density of the capital city of Spain is 5500 persons per square kilometer. However, the appearance of cases does not only depend on population density, but also on other factors, e.g., mobility and social interaction.
The metropolitan region of Madrid follows a radio-centric spatial structure, which is similar to the organization that can be found in cities such as London or Paris. There is a central core form around which different areas have been developed, forming belts. Figure 1 shows the locations of the public hospitals of the CoM. Note that most of the hospitals are in the metropolitan area of the city (Figure 2). The hospital occupancy demand was heterogeneous in the CoM because the cumulative incidence of COVID-19 varied in the different geographical areas. The areas with the highest incidence in March and April were located in the periphery of the capital—the lower and upper quadrants of the area shown in Figure 2, specifically in the regions where hospitals 17, 10, 12, and 16 are located.
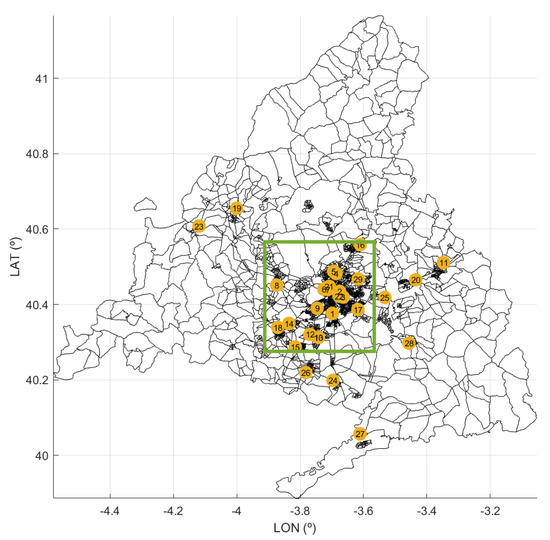
Figure 1.
Map of the CoM with the locations of its public hospitals. The yellow tags correspond with the IDs in Table 1. Black patches represent regions with similar numbers of inhabitants.

2.2. Data Description
It should be clarified that, during the pandemic, hospital beds were divided into two large groups (non-ICU beds and ICU beds); therefore, the collected data were ranked according to this classification. The beds assigned to each group were further subdivided into available beds (beds that had all the equipment and personnel necessary for their function), occupied beds (beds that were occupied by inpatients), and unoccupied beds (i.e., available beds that were not occupied). We also distinguished between the beds that were occupied by COVID-19 patients or non-COVID-19 patients. In pandemic waves, which pushed the CoM’s hospitals beyond their functional limits, it was necessary to organize the beds in a different way in order to control the situation as well as possible. Indeed, this not only happened in the CoM, but also in other countries. So, for example, the National Health Service of England wisely stated that the “hospital capacity has had to be organized in new ways as a result of the pandemic to treat COVID and non-COVID patients separately and safely... As a result caution should be exercised in comparing overall occupancy rates between this year and previous years” [11]. Bearing this advice in mind, this paper analyzes the evolution of beds in the CoM’s hospitals according to the structure and limits of the information received by the COVID-19 Control Center (CCC).
The data used in this study were supplied daily by each hospital, starting on 18 March 2020 and finishing on 31 May 2020. The original dataset consisted of 34 public and 33 private hospitals, although for the purposes of this study, we selected those described in Table 1. Notice that, although hospitals admitted COVID-19 patients prior to 18 March 2020, due to the lack of reliable data from hospitals during the beginning of the first pandemic wave, the series analyzed in this paper begins on 18 March 2020.
The CCC, in which some of the authors of this paper worked during the first wave, was created [12] by the CoM’s Government on 13 March 2020 due to the emergency situation. The CCC aimed to receive daily data from the hospitals, interact with them to filter and debug errors, and use tools that allow their visualization. The information was obtained by means of a spreadsheet in which said hospitals filled out a template shared by all of them on a daily basis, as well as through a web application developed on the Microsoft Teams platform, in which data concerning the situations in the emergency departments were also requested as additional information. For their part, private hospitals sent their daily data in aggregate form only by means of a spreadsheet that had the same template as that used by the public hospitals. The CCC was just in charge of digitizing information; its function was not to make decisions about the management of the hospitals.
2.3. Methodology
To achieve the goal of this research, a case study methodology was used because (1) there was an interest in knowing the “how” and “why” of the phenomenon, (2) there was little or no control over behavioral events, and (3) the study’s focus is a contemporary phenomenon—a “case” [13]. Building theory inductively from cases is likely to have important strengths, such as novelty, testability, and empirical validity, which arise from the intimate linkage with empirical evidence” [14], and it is also “likely to produce theory that is accurate, interesting, and testable”, as a wide range of data sources can be used, such as qualitative and quantitative documentations, data, and/or direct observations [15].
Based on the qualitative and quantitative data gathered for the case study, the dynamic response of the healthcare system consisting of the hospital network in the CoM was analyzed. In particular, both the demand and the capacity of the system were studied. System demand refers to the demand or the number of patients that require a service to be provided at a hospital (in this case, the use of a hospital bed combined with treatment and care services) with non-ICU and ICU beds. The availability of non-ICU and ICU beds refers to the readiness or disposal of beds in a hospital that can be offered to potential new patients that demand this service.
In order to analyze the network’s response to the increase in the bed demand, we used the concepts of the bed margin and flexibility in this paper. According to Green [16], hospital occupancy is defined as the ratio of occupied beds to the total number of beds. Following this concept, we defined the bed margin as the ratio of unoccupied beds to the total number of available beds, where the number of unoccupied beds is the difference between the number of available beds and the occupied beds. Note that the proposed bed margin is also related to the well-known concept of utilization in the context of operations management (see, e.g., [17,18]).
The flexibility of a system is not a novel concept. For example, in electric power systems, it is used to characterize the ability of electricity generators to accommodate variation and uncertainty in demand (see, e.g., [19,20]). In this paper, we define the flexibility of a healthcare system as the system’s ability to accommodate a large and unexpected increase in bed demand by modulating the availability of beds across the hospital network over time. Hospitals are managed in order to maintain the balance between quality and costs. Small variations and uncertainties, as well as seasonal fluctuations, in bed demand are managed by hospitals without problems by maintaining an appropriate bed margin. However, dealing with rare abrupt increases in bed demand, such as those generated by the COVID-19 pandemic, indicates a big challenge for hospitals that requires a different type of response—a flexibility induced by the response to a large perturbation.
In order to quantify this flexibility, we propose three different indexes (see Table 2): the Ramp Duration Until the Peak (RDUP), the Ramp Growth Until the Peak (RGUP), and the Average Ramp Rate Until the Peak (ARRUP). According to Figure 3, the RDUP can be easily computed from the raw data as the difference between the time where the peak was reached and the starting time of the increase in the bed demand . In the same way, the RGUP can be obtained from the difference between the number of available beds at the peak and at the starting time of the increase in the demand .
Table 2.
Proposed flexibility indexes.

Figure 3.
Graphic illustration of the proposed flexibility indicators and their estimation based on the Linear Hinges Model (LHM). The raw data represent the variation in the number of available beds with time, with small random variations around a trend. The LHM is fitted to the raw data in order to estimate the trend, allowing a robust determination of the three indexes.
However, to compute the ARRUP index, a robust estimation of the slope of the underlying non-linear bed curve is required. In this paper, we first fit the Linear Hinges Model (LHM) to the raw data, and then directly compute the slopes from the fitted LHM. The LHM was proposed by Sánchez-Úbeda et al. [21]; it is a piecewise linear model defined by K knots, the points specifying the pieces (see the illustrative example in Figure 3). Based on the slopes given by the LHM, the ARRUP can be estimated by computing the weighted mean of the slopes just before the peak, where the weights are given by the proportion of the number of days within each segment. Furthermore, both the RDUP and the RGUP can also be estimated directly from the LHM, providing a more robust estimation of these indexes. In this paper, an implementation of the LHM fitting algorithm in the Matlab Software [22] was used.
Note that, although there exist plenty of curve-fitting models that can be used to fit the beds’ curve, such as polynomials or splines, the LHM was selected for estimating the flexibility indicators because it is especially suited for this problem, since it is an efficient approach to curve-fitting under stringent high-noise conditions and thus provides straightforward information on slopes. Moreover, the main advantage of the LHM is that its learning algorithm automatically selects the number and locations of the knots, adapting its complexity to the quality and availability of the data, and thus allows the description of a wide range of functional forms. In particular, the number and positions of the knots are obtained automatically by using a learning algorithm that combines a greedy divide-and-conquer strategy with a computationally efficient pruning approach and special updating formulas [23].
3. Results
The results are presented first as an aggregate view of the healthcare system, and second as a disaggregated view by hospital. We distinguish between non-ICU and ICU beds, and apply the proposed bed margin and flexibility indicators in order to quantify the dynamic response.
3.1. Aggregate View of the Healthcare System
3.1.1. System Demand for Non-ICU and ICU Beds
The healthcare system of the CoM was stressed as the number of ill people by SARS-CoV-2 steeply increased in March 2020. Figure 4 shows the daily non-ICU beds occupied by COVID-19 patients for the CoM’s hospitals, as well as the daily total non-ICU occupied beds (i.e., COVID-19 and non-COVID-19). Similarly, Figure 5 shows both the daily ICU beds occupied by COVID-19 patients and the total occupied ICU beds. In the interpretation of the evolution of the curves for each type of bed, it should be taken into account that the average length of stay in an ICU bed was longer than that in a non-ICU bed, and that the flow of patients into ICU beds had a double origin: from the emergency department—in patients with severe clinical presentation—or from non-ICU beds after clinical worsening of the symptoms, which occurred between 2 and 4 days after admission to the hospital [24]. Finally, note that if the patient’s stay in the ICU was successful, they were re-admitted to a non-ICU bed.

Figure 4.
Daily number of total occupied non-intensive care unit (ICU) beds and COVID-19-occupied non-ICU beds.
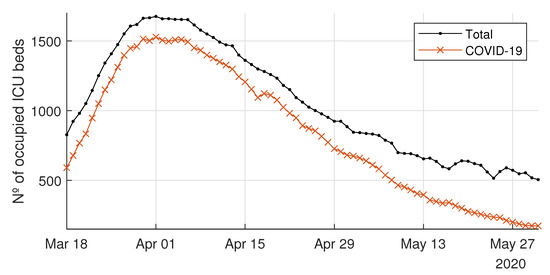
Figure 5.
Daily number of total occupied intensive care unit (ICU) beds and COVID-19-occupied ICU beds.
This increase in hospital inpatients caused by the new disease implied that the demand for beds in the CoM’s healthcare system grew rapidly during that period. Note that the weekly seasonal pattern, which is visible in the second part of the occupied bed time series (beyond 29 April 2020), was due to the recovery of the regular activity after the peak, where elective patients were usually not admitted on weekends.
From 18 March 2020 to 31 March 2020 (13 days), the daily non-ICU inpatients with COVID-19 increased from 4578 up to 13,725, i.e., an increase of 200%. During the same period, the ICU admissions due to COVID-19 increased by 155% (from 590 to 1502). According to newspapers and television, during the peak period, the time spent by patients in emergency rooms and hallways waiting for a bed increased dramatically in many hospitals of the CoM (see, e.g., [25]).
3.1.2. Availability of Non-ICU and ICU Beds
Creating enough capacity in the CoM’s hospitals to deal with the COVID-19 demand was a big challenge during March 2020. This capacity expansion meant not only increasing the availability of physical beds, but also of specialized personnel and the required equipment.
In order to fulfill this objective, hospitals implemented several strategies. At first, operating rooms and semi-intensive care beds were transformed into fully operating ICU beds within existing hospitals. Later, several hotels were turned into recovery units to which non-critical patients could be transferred. A field hospital was also opened on 22 March 2020 in an existing convention center (IFEMA) to release some of the pressure on permanent hospitals. This hospital started with 185 non-ICU beds and reached a maximum at 3 April 2020 with 1150 and 10 non-ICU and ICU beds, respectively. It was operative until 30 April 2020. Furthermore, from the demand side, the Spanish government implemented the confinement of the country with severe restrictive measures to lower the spread of the virus and to reduce the demand for beds in the short term, i.e., the so-called “flattening the curve” [26,27].
Figure 6 compares the system’s capacity and the demand for non-ICU and ICU beds. This capacity is measured as the number of available beds. The numbers of non-ICU and ICU beds provided by the system rose drastically to follow the growth of the demand for beds.
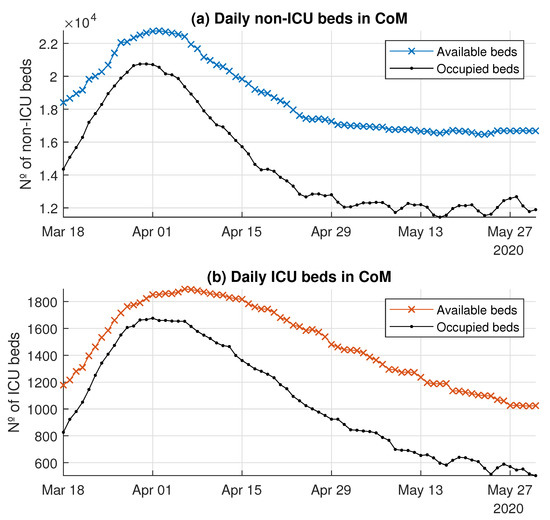
Figure 6.
Daily availability and occupation of beds in the CoM’s hospital system.
3.1.3. System Bed Margin
Figure 7 shows the daily number of unoccupied beds and the bed margin for both the non-ICU and ICU beds. On 18 March 2020, at the beginning of the peak, the number of unoccupied non-ICU beds was 4053, whereas the number of unoccupied ICU beds was 351, making the bed margins 22% and 29.8%, respectively. However, 29 March 2020 was the worst day in terms of the non-ICU bed margin (7.6%) for the health system as a whole; the number of unoccupied non-ICU beds reached a minimum value of 1688. For the ICU beds, the worst day was 30 March 2020, with 128 unoccupied ICU beds, which represents an ICU bed margin of 7.1%. From 1 April 2020, the margin started to recover. In particular, the non-ICU bed margin stabilized in May, with an average value of 27.3% (4664 unoccupied beds). On the other hand, the ICU bed margin continued increasing up to 50% (around 500 unoccupied beds).

Figure 7.
Daily unoccupied beds and the bed margin (%) in the CoM’s hospital system.
3.1.4. Healthcare System Flexibility
Figure 8 shows the LHM obtained for the available non-ICU and ICU beds. The LHM for the non-ICU beds consisted of eight knots, whereas the model for the ICU beds had .

Figure 8.
Model of the available beds using LHM.
According to the LHM for non-ICU beds (Figure 8, top), the peak was on 2 April 2020, when the maximum number of available non-ICU beds was reached. This model detected two different ramps until the peak (see Table 3). In the first period, the slope was around 384 beds/day over 11 days. Just four days, before the peak, during the second segment given by the model, the ramp rate went down to around 92 non-ICU beds/day. Something similar happened for the available ICU beds, where the slope also slowed down just before the peak (Figure 8, bottom). In this case the LHM estimated three segments until 7 April 2020 (see Table 4), with a slope of nearly 61 ICU beds/day during the first 10 days. The duration of the third ramp was six days, with a rate of around 9 beds/day. The reduction with time in the slopes of both non-ICU and ICU available beds confirmed the great efforts during the first days to increase the bed capacity, as well as the difficulties in obtaining additional capacity near the peak.
Table 3.
Estimated slopes for available non-ICU beds.
Table 4.
Estimated slopes for available ICU beds.
Based on these LHMs, the flexibility indicators were estimated (see Table 3 and Table 4). In particular, the ARRUP for non-ICU beds was 305.56 beds/day (), the RDUP was 15 days, and the RGUP was 4598 beds. For the ICU beds, the ARRUP was 36.73 beds/day, the RDUP was 20 days, and the RGUP was 735 beds.
3.2. Disaggregated View by Hospital
In the previous section, the system’s response to the COVID-19 pandemic was analyzed. This provided a global view of the aggregated response of the CoM’s hospital network as a unique system. However, not all the hospitals were confronted with the same bed demand, nor did they provide the same flexibility in order to increase the bed capabilities. In this section, we provide a disaggregated view by hospital. In order to quantify the response of each hospital, the concepts of the bed margin and flexibility were applied straightforwardly to each hospital.
3.2.1. Demand and Availability of Beds by Hospital
Figure 9 shows the daily number of occupied non-ICU beds by hospital, whereas Figure 10 shows the demand for ICU beds for each hospital. The demand for beds at HIFEMA, the hospital that was available on 22 April 2020, was different from the rest because it was created specifically to release some of the pressure on permanent hospitals during the critical days of the peak. Logically, the daily bed demand of a given hospital is limited by its daily availability of beds.
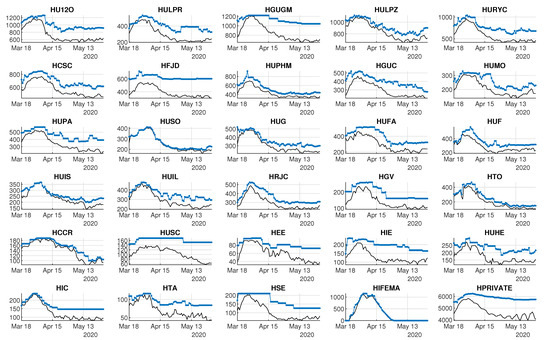
Figure 9.
Capacity and demand for non-ICU beds by hospital. Black lines represent occupied beds. Colored lines represent available beds.

Figure 10.
Capacity and demand for ICU beds by hospital. Black lines represent occupied beds. Colored lines represent available beds.
Concerning the availability of beds, Figure 9 and Figure 10 also show the daily numbers of available non-ICU and ICU beds, respectively. Note that most of the hospitals were able to increase their bed capacity during the critical days, although some of them had more difficulties with maintaining a reasonable bed margin.
3.2.2. Bed Margin by Hospital
From 18 March 2020 to 15 April 2020 the system’s margin was lower than 30% for both types of beds (see Figure 7). In particular, the daily minimum bed margins were 7.6% and 7.1% for non-ICU and ICU beds, respectively. However, during this period, the bed margins varied from hospital to hospital. Figure 11 shows a boxplot of the bed margins for each hospital computed for this period of 29 days. The hospitals are sorted according to the third empirical quartile for each type of bed.
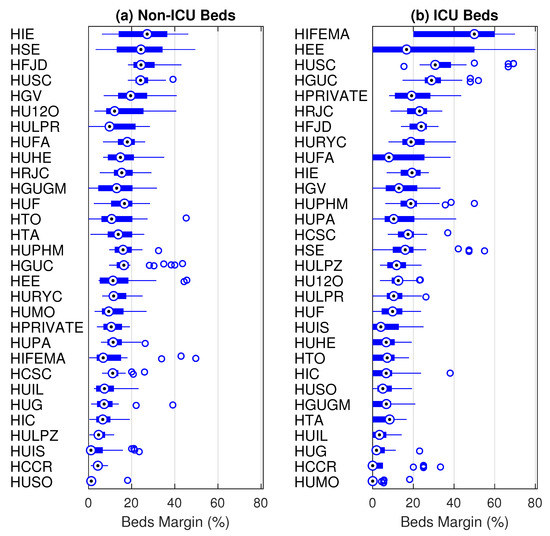
Figure 11.
Compact boxplot representation of the non-ICU and ICU bed margins (%) by hospital. For each distribution, the median is represented by a circled dot, the interquartile range by a rectangle, the whiskers by lines, and the outliers by empty circles.
For non-ICU beds (Figure 11, left), the margin was lower than 60% for all hospitals. In fact, all but seven hospitals had a non-ICU bed margin lower than 25% for at least 75% of the days, i.e., the third quartile of the bed margin was lower than 25%. HUSO was the most stressed hospital in terms of non-ICU beds during this period, with a median bed margin of 1.3% (five beds). Concerning ICU beds, the lack of unoccupied beds in several hospitals over several days is obvious. Table 5 shows the hospitals where the ICU bed margin was lower than or equal to 15% for at least 75% of the days, i.e., those where the third quartile of the bed margin was lower than 15%. Furthermore, the second quartile of the number of unoccupied ICU beds was equal to 1 for many hospitals, i.e., for half of the days, no more than one ICU bed was unoccupied in those hospitals. HUMO and HCCR did not have unoccupied ICU beds for at least 75% of the days.
Table 5.
Quartiles (1 to 3) of the bed margin (%) and number of unoccupied ICU beds for hospitals. Q1, Q2, and Q3 are the three quartiles.
3.2.3. Flexibility by Hospital
It was possible to calculate the previously defined indexes—RDUP, RGUP, and ARRUP (see Table 2)—for each hospital using the same approach based on the LHM. In this case, it was even more necessary to have a robust slope estimation mechanism because the random variations around the main curve were more important. For example, Figure 12 shows the details of the LHM fitted to the available ICU beds of four different hospitals. Notice that the LHM allows the extraction of the main underlying response for each particular hospital by assimilating the daily fluctuations in the original data.

Figure 12.
Model of the number of available ICU beds using the LHM (details of four hospitals).
Table 6 shows the estimated values of the indexes for the non-ICU beds for each hospital, whereas Table 7 shows the results for the ICU beds. According to the first table, larger public hospitals, such as HU120, HGUGM, and HULPZ, which had more than 1000 regular beds on 18 March 2020, had a lower RGUP and ARRUP than other medium-sized hospitals, such as HUF, HRJC, or HUPHM. For example, HU120 increased the number of available non-ICU beds by 188 (10%), whereas the HUF was able to increase by 241 non-ICU beds (70%). However, according to Table 7, the HULPZ was the public hospital with the largest RGUP in ICU beds, as it was able to increase by 82 ICU beds (120%) in 15 days. HU12O and HGUGM also had a large RGUP.
Table 6.
Non-ICU bed flexibility by hospital. The initial and the maximum numbers of available beds, as well as the three flexibility indicators, are shown for each hospital. The top eight hospitals have a high complexity (see Table 1).
Table 7.
ICU bed flexibility by hospital. The initial and the maximum numbers of available beds, as well as the three flexibility indicators, are shown for each hospital. The top eight hospitals have a high complexity (see Table 1).
4. Discussion
Analyzing healthcare data through the first wave of SARS-CoV-2 has brought up an opportunity to better understand hospital performance under these severe circumstances. Specifically, by analyzing the flexibility and bed margin, it is possible to dynamically graph—as an alternative or complement to other, more static models—not only the day-to-day response of the system as a whole for all of the hospitals within the CoM region, but also the response of each hospital (Figure 9 and Figure 10). These graphs provide information for hospital managers and healthcare system supervisors, since they can check (in a dynamic way) certain situations that are referred to later on.
This paper focuses on modeling the hospital capacities in terms of ICU and non-ICU beds during the pandemic while distinguishing between patients with and without COVID-19, since most publications focus on bed management in other contexts [28,29,30,31,32,33] (except for Condes and Arribas [34] and Fanelli et al. [35]). We have not found a work in the literature that gives information on this topic with the details and large number of hospital and inpatients that this article uses, highlighting the fact that the hospitals involved in this study were in the epicenter of the first wave of the COVID-19 pandemic at the European level. Therefore, the data presented here could be beneficial in the future in order to compare what happened during the first wave in other healthcare systems and to better prepare in the event new epidemic waves caused by SARS-CoV-2 or other pathogens. Finally, this article shows a way to classify hospitalized patients in pandemic situations and to manage infected and uninfected inpatients. Among other things, this classification makes it possible, with the previously mentioned safeguards, to compare the first wave with the pre-pandemic situation in order to know how many patients could not be admitted to hospitals for diseases other than COVID-19. The previous situation, in our opinion, should be a clear invitation to other researchers to address such a critical scenario when that information is available.
The above-mentioned achievements were obtained by analyzing and extracting information from the available data from the CCC. The relevant figures of the first pandemic wave in the CoM were: From 18 March 2020 to 31 March 2020 (13 days), COVID-19 inpatients increased by 200% in non-ICU wards and by 155% in ICU wards. The maximum occupancy of available beds took place on 31 March 2020. On that day, in all of the hospitals that we analyzed, the total number of available beds was 23,463, of which 21,549 (92%) were occupied. The capacity in many hospitals was exhausted, but the fear that the demand would continue to increase caused the number of available beds to increase by 160 in 48 h, reaching the figure of 23,623 beds on 2 April 2020, with an occupancy of 90.3%.
The previous paragraph describes the first wave scenario in the CoM. Our analysis, which was focused on the proposed bed margin and flexibility indexes, shows that hospitals adapted to unexpected requirements with different responses. Notice the following fact: All but seven hospitals presented a non-ICU bed margin (Figure 11, left) lower than 25% for at least 75% of the days, and one of them presented a median bed margin of 1.3% (five beds). Focusing on ICU beds, the lack of unoccupied beds in several hospitals over several days was notorious (Table 5). For at least 75% of the days, in 14 of the 30 hospitals analyzed, the ICU bed margin was lower than or equal to 15%, and two hospitals lacked free ICU beds. Occupied non-ICU beds and ICU beds did not return to the values of 18 March 2020 until the third week of April and the first week of May, respectively.
Under normal conditions, hospitals sometimes operate with difficulties, especially in emergency departments. Contrary to popular belief, hospitals are complex but vulnerable institutions [36]. This vulnerability is mainly due to three factors: First, as seen with personal protective equipment and laboratory reagents, they are highly dependent on external supplies. Second, the key staff is highly specialized and is not easy to increase or replace. Third, their infrastructure (beds, doctor offices, medical equipment, etc.) is dimensioned to care for a range of pathologies and a maximum number of patients. Therefore, a modest variation in the admission volume, as happens when the seasonal flu arrives, can lead the hospital beyond its functional reserves.
It is worth noting how unexpected demands cause situations like those shown in Figure 4 and Figure 5. These figures compare the beds occupied by patients with or without COVID-19 who were hospitalized inside and outside ICUs. Moreover, they show how the demand for hospitalizations due to COVID-19 severely reduced the hospitals’ capacities to admit new patients with other types of pathologies, especially in the ICUs. Flexibility in available beds is a significant driver for managing hospitals efficiently, and its importance acquires greater relevance in situations such as the COVID-19 pandemic.
Quantifying the flexibility with a regression technique such as the LHM is an attempt to model the dynamic performance from the observed data. More specifically, the LHM was used to obtain a robust estimation of the proposed flexibility indexes by means of the piecewise slope estimations that it provided for the time series of the number of available beds. In particular, the LHM obtained for available non-ICU and ICU beds in the CoM’s whole health system detected several different ramps before and after the peak (see Figure 8). The reduction of the available beds after the peak is explained easily by the systematic decrease in bed demand. However, the slowdown in the ramp rate of available beds started before the bed demand decreased (see Figure 5). The systematic reduction in the bed margin before the peak is noticeable for both non-ICU and ICU beds (see Figure 6); thus, the ramps began to slow down as they approached the peak. The justification is supported by the reduction in bed demand and the system’s limitations for additional capacity when the bed demand was peaking. These limitations show up due to the lack of extra physical space, equipment, and qualified personnel.
The flexibility performance indicators and the LHM model were used in an attempt to provide insights that could help improve the hospitals’ management and decision making. However, it cannot be determined a priori what the optimal level of beds or human resources for facing a pandemic crisis should be. Unfortunately, it is not possible to respond to this question until after a new epidemic wave is addressed.
Figure 9 and Figure 10 show the supply of and demand for beds. The observed variations can be explained, in a summarized way, by saying that hospitals of high complexity, which are those with more beds, generally fared better than hospitals of lower complexity (which are the ones with the fewest beds). This fact emphasizes the importance of having a real-time control panel that could avoid having hospitals under the pressure of a very narrow bed margin. Distributing inpatients throughout the hospital system can ease the pressure on some hospitals. In this way, two main objectives will be achieved in a very complex environment: avoiding the professionals’ exhaustion and providing the best care to patients. Let us remember that both objectives are intimately interweaved.
This paper focuses on the first wave of the COVID-19 pandemic in a specific geographic area (the CoM in Spain). The proposed model is dynamic (compared to existing static models) and could be used in other geographic regions, as well as in future waves of pandemics or other health crises. The introduction of new mathematical models for emulating the dynamics of a hospital network in terms of capacity, flexibility, and bed margin will pave the way to a better understanding of the impacts of health policies and resource management during health crises. An example of this type of research is the work by Wood [37], where the ICU capacity of a large British public hospital in the context of COVID-19 was analyzed using public data from the Intensive Care National Audit and Research Centre [38].
5. Conclusions
The main objective of our study was to analyze the dynamic response of the CoM’s hospitals during the first wave of the SARS-CoV-2 pandemic. In order to carry out this analysis, a set of very informative indicators was proposed. These indexes were able to summarize the observed dynamics of the curve of the available beds during the pandemic in a simple way. In particular, we proposed the bed margin as a useful index of the available resources, as well as three new indicators for capturing the flexibility with respect to the growing demand for beds. The main indicator of flexibility is the Average Ramp Rate Until the Peak (ARRUP), but it cannot be interpreted in isolation. The Ramp Duration Until the Peak (RDUP) and the Ramp Growth Until the Peak (RGUP) provide useful information that allows one to answering questions, such as: For how many days can the observed ramp rate be maintained? What is the maximum number of beds that can be available?
Our results, which are based on the proposed bed margin and flexibility indexes, show that the hospital network in the CoM can increase the number of available ICU beds with a rate of at least 61 beds/day for 10 days. Furthermore, the considered hospitals were able to adapt to unexpected requirements with different responses. This study offers valuable insights concerning not only the system’s response, but also about the individual responses of the CoM’s hospitals.
The proposed indicators are ready to use for monitoring of networks of hospitals. For example, the estimated indexes for a particular hospital during the first pandemic wave can be used as a reference for this hospital, which is useful for monitoring its behavior during a similar pandemic wave. Future research could apply the proposed methodology based on the bed margin and flexibility indexes in order to analyze a health system’s response during other pandemic waves or similar catastrophes. The comparison of our findings during this first wave with those of future responses may provide additional insights. Moreover, due to the existence of particular characteristics of the hospitals that could affect their dynamic responses under these critical circumstances, future research may be developed in order to identify machine learning models that are able to estimate a given hospital’s flexibility as a function of its characteristics.
Author Contributions
Conceptualization, E.F.S.-Ú., P.S.-M., M.T.-E., Á.D.R.-M., M.F.M.-C., and J.-L.P.; methodology, E.F.S.-Ú.; software, E.F.S.-Ú.; validation, E.F.S.-Ú., P.S.-M., M.T.-E., Á.D.R.-M., M.F.M.-C., and J.-L.P.; formal analysis, E.F.S.-Ú. and P.S.-M.; data curation, M.T.-E. and E.F.S.-Ú.; writing—original draft preparation, E.F.S.-Ú., J.-L.P., and M.T.-E.; writing—review and editing, E.F.S.-Ú., P.S.-M., M.T.-E., Á.D.R.-M., M.F.M.-C., and J.-L.P.; visualization, E.F.S.-Ú. and P.S.-M.; supervision, E.F.S.-Ú. and M.F.M.-C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Submission for ethical approval is not applicable. The study did not involve humans or animals, limiting itself to the use of hospital resources.
Informed Consent Statement
Not applicable.
Data Availability Statement
Restrictions apply to the availability of these data. The data were obtained from the network of public and private hospitals in the CoM and are available from the CCC with the permission of the Department of Health, CoM Government. The dataset is neither public nor available in the way that it has been used as a source in this article.
Acknowledgments
We would like to thank all of the hospital personnel who worked with and helped those in need during the arrival of this pandemic. They coped with scarce resources in dangerous situations, enduring long working hours. We could not have overcome the first fight against COVID-19 without them.
Conflicts of Interest
The authors declare no conflict of interest.
Software Availability Statement
The LHM fitting software used in this study is available from IIT http://www.iit.comillas.edu/, but restrictions apply to the availability of the software, which is not publicly available.
Abbreviations
The following abbreviations are used in this manuscript:
| AC | Autonomous Community |
| ARRUP | Ramp Duration Until the Peak |
| CCC | COVID-19 Control Center |
| CoM | Autonomous Community of Madrid |
| COVID-19 | Coronavirus Disease 2019 |
| CS | Consejería de Sanidad—Departments of Health |
| DEA | Data Envelopment Analysis |
| ICU | Intensive Care Unit |
| LHM | Linear Hinges Model |
| non-ICU | Non-Intensive Care Unit |
| RDUP | Ramp Duration Until the Peak |
| RGUP | Ramp Growth Until the Peak |
| SARS-CoV-2 | Severe Acute Respiratory Syndrome Coronavirus 2 |
| SNS | Sistema Nacional de Salud—Spanish National Health System |
References
- Kaplan, E.H. Containing 2019-nCoV (Wuhan) coronavirus. Health Care Manag. Sci. 2020, 23, 311–314. [Google Scholar] [CrossRef] [PubMed]
- US Department of Health and Human Services. Pandemic Influenza Plan: 2017 Update. Technical Report. 2017. Available online: https://www.cdc.gov/flu/pandemic-resources/pdf/pan-flu-report-2017v2.pdf (accessed on 25 October 2020).
- Leiva, C. Manual de Procedimientos en Gestión de Crisis Volume 2; Crisis Management: Madrid, Spain, 2007. [Google Scholar]
- Bekker, R.; Koole, G.; Roubos, D. Flexible bed allocations for hospital wards. Health Care Manag. Sci. 2016, 20, 453–466. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Sanidad, Consumo y Bienestar de España. Centro de Coordinación de Alertas y Emergencias Sanitarias. Actualización n° 62. Enfermedad por el Coronavirus (Covid-19). 2020. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/documentos/Actualizacion_62_COVID-19.pdf (accessed on 22 January 2021).
- European Centre for Disease Prevention and Control. Historical Data (to 14 December 2020) on the Daily Number of New Reported COVID-19 Cases and Deaths Worldwide. Available online: https://www.ecdc.europa.eu/en/publications-data/download-todays-data-geographic-distribution-covid-19-cases-worldwide (accessed on 22 January 2021).
- European Centre for Disease Prevention and Control. Data on Hospital and ICU Admission Rates and Current Occupancy for COVID-19. Available online: https://www.ecdc.europa.eu/en/publications-data/download-data-hospital-and-icu-admission-rates-and-current-occupancy-covid-19 (accessed on 22 January 2021).
- Bernal-Delgado, E.; García-Armesto, S.; Oliva, J.; Sánchez Martínez, F.I.; Repullo, J.R.; Peña-Longobardo, L.M.; Manuel, R.L.; Hernández-Quevedo, C. Spain: Health system review. In Health Systems in Transition; World Health Organization: Geneva, Switzerland, 2018; Volume 20, pp. 1–179. [Google Scholar]
- Consejería de Sanidad de la Comunidad de Madrid. Memoria Anual de Actividad del Servicio Madrileño de Salud 2018. Technical Report. Consejería de Sanidad de la Comunidad de Madrid. 2019. Available online: http://www.madrid.org/bvirtual/BVCM020283.pdf (accessed on 10 September 2020).
- The National Statistics Institute. The National Statistics Institute Data Base. Available online: https://www.ine.es (accessed on 3 September 2020).
- National Health Service (NHS). Bed Availability and Occupancy. Available online: https://www.england.nhs.uk/statistics/statistical-work-areas/bed-availability-and-occupancy/ (accessed on 24 January 2021).
- Comunidad de Madrid. Díaz Ayuso Visita el Nuevo Centro de Control Permanente del Coronavirus de la Comunidad de Madrid. Available online: https://www.comunidad.madrid/noticias/2020/03/14/diaz-ayuso-visita-nuevo-centro-control-permanente-coronavirus-comunidad-madrid (accessed on 27 January 2021).
- Yin, R. Case Study Research and Applications: Design and Methods; SAGE Publications: Thousand Oaks, CA, USA, 2017. [Google Scholar]
- Eisenhardt, K.M. Building Theories from Case Study Research. Acad. Manag. Rev. 1989, 14, 532–550. [Google Scholar] [CrossRef]
- Eisenhardt, K.M.; Graebner, M.E. Theory Building From Cases: Opportunities And Challenges. Acad. Manag. J. 2007, 50, 25–32. [Google Scholar] [CrossRef]
- Green, L.V. How Many Hospital Beds? INQUIRY J. Health Care Organ. Provis. Financ. 2002, 39, 400–412. [Google Scholar] [CrossRef] [PubMed]
- Chase, F.; Jacobs, F.; Aquilano, N. Operations Management for Competitive Advantage; McGraw-Hill/Irwin Series; Tata McGraw-Hill: New York, NY, USA, 2006. [Google Scholar]
- Gellman, M.; Turner, J. Encyclopedia of Behavioral Medicine; Springer: New York, NY, USA, 2019. [Google Scholar]
- Lannoye, E.; Flynn, D.; O’Malley, M. Evaluation of Power System Flexibility. IEEE Trans. Power Syst. 2012, 27, 922–931. [Google Scholar] [CrossRef]
- Mohandes, B.; Moursi, M.S.E.; Hatziargyriou, N.; Khatib, S.E. A Review of Power System Flexibility With High Penetration of Renewables. IEEE Trans. Power Syst. 2019, 34, 3140–3155. [Google Scholar] [CrossRef]
- Sánchez-Úbeda, E.F.; Wehenkel, L. The Hinges model: A one-dimensional continuous piecewise polynomial model. In Proceedings of the International Congress on Information Processing and Management of Uncertainty in Knowledge Based Systems, IPMU98, Paris, France, 6–10 July 1998. [Google Scholar]
- MATLAB. 9.6.0.1114505 (R2019a) Update 2. Available online: https://www.mathworks.com/ (accessed on 16 March 2021).
- Sánchez-Úbeda, E.F. Models for Data Analysis: Contributions to Automatic Learning. Ph.D. Thesis, Universidad Pontificia Comillas de Madrid, Madrid, Spain, 1999. [Google Scholar]
- European Centre for Disease Prevention and Control. Clinical Characteristics of COVID-19. Available online: https://www.ecdc.europa.eu/en/covid-19/latest-evidence/clinical (accessed on 5 September 2020).
- Abril, G. La Paz: A Madrid Hospital at War against Covid-19. El Pais Semanal. 24 April 2020. Available online: https://english.elpais.com/eps/2020-04-24/la-paz-a-madrid-hospital-at-war-against-covid-19.html (accessed on 15 September 2020).
- Anderson, R.; Heesterbeek, H.; Klinkenberg, D.; Déirdre Hollingsworth, T. How will country-based mitigation measures influence the course of the COVID-19 epidemic? Lancet 2020, 395, 931–934. [Google Scholar] [CrossRef]
- Casares, M.; Khan, H. The Timing and Intensity of Social Distancing to Flatten the COVID-19 Curve: The Case of Spain. Int. J. Environ. Res. Public Health 2020, 17, 7283. [Google Scholar] [CrossRef] [PubMed]
- Kuntz, L.; Scholtes, S.; Vera, A. Incorporating efficiency in hospital-capacity planning in Germany. Eur. J. Health Econ. 2007, 8, 213–223. [Google Scholar] [CrossRef] [PubMed]
- National Audit Office. Inpatient Admissions and Bed Management in NHS Acute Hospitals; Technical Report; National Audit Office: London, UK, 2000. [Google Scholar]
- Proudlove, N.; Brown, C. Winter planning. Seasonal cycles. Health Serv. J. 2002, 112, 24–25. [Google Scholar] [PubMed]
- Ravaghi, H.; Alidoost, S.; Mannion, R.; Bèlorgeot, V.D. Models and methods for determining the optimal number of beds in hospitals and regions: A systematic scoping review. BMC Health Serv. Res. 2020, 20, 186. [Google Scholar] [CrossRef] [PubMed]
- da Costa Lino, D.O.; Barreto, R.; de Souza, F.D.; de Lima, C.J.M.M.; da Silva Junior, G.B. Impact of lockdown on bed occupancy rate in a referral hospital during the COVID-19 pandemic in northeast Brazil. Braz. J. Infect. Dis. 2020, 24, 466–469. [Google Scholar] [CrossRef] [PubMed]
- Walford, S. Unexpected Medical Illness and the Hospital Response. Models of Emergency Care; University of Warwick: Coventry, UK, 2002. [Google Scholar]
- Condes, E.; Arribas, J.R. Impact of COVID-19 on Madrid hospital system. Enfermedades Infecc. Microbiol. Clin. 2020. [Google Scholar] [CrossRef] [PubMed]
- Fanelli, S.; Lanza, G.; Francesconi, A.; Zangrandi, A. Facing the Pandemic: The Italian Experience From Health Management Experts’ Perspective. Am. Rev. Public Adm. 2020, 50, 753–761. [Google Scholar] [CrossRef]
- World Health Organization Regional Office for Europe. Hospital Readiness Checklist for COVID-19; Technical Report; World Health Organization Regional Office for Europe: Geneva, Switzerland, 2020; Available online: https://apps.who.int/iris/bitstream/handle/10665/333972/WHO-EURO-2020-1012-40758-54954-eng.pdf (accessed on 1 March 2020).
- Wood, R.M.; McWilliams, C.J.; Thomas, M.J.; Bourdeaux, C.P.; Vasilakis, C. COVID-19 scenario modelling for the mitigation of capacity-dependent deaths in intensive care. Health Care Manag. Sci. 2020, 23, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Richards-Belle, A.; Orzechowska, I.; Gould, D.W.; Thomas, K.; Doidge, J.C.; Mouncey, P.R.; Christian, M.D.; Shankar-Hari, M.; Harrison, D.A.; Rowan, K.M.; et al. COVID-19 in critical care: Epidemiology of the first epidemic wave across England, Wales and Northern Ireland. Intensive Care Med 2020, 11, 2035–2047. [Google Scholar] [CrossRef] [PubMed]












Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).