Abstract
Personality is one of the most crucial aspects of human life, since it influences all human behaviours in both personal and social life, and might also trigger important conflicts with a person’s surroundings in the setting of incompatible traits and characteristics. It is true that ‘one must be born’ for a certain medical specialty, but several components of personality might be educated with proper training. Increased levels of Conscientiousness, Agreeableness, and Openness associated with lower levels of Neuroticism might represent the key combination for achieving professional satisfaction in the medical profession. Medical students should receive proper interprofessional education, since effective interprofessional relationships among healthcare providers definitely improve patients’ safety. Empathy contributes to effective patient–physician communication, improving patient trust, compliance, and satisfaction, being positively correlated with Openness, Agreeableness, Conscientiousness and Extraversion. Emotional intelligence—the capacity to respond to one’s own and others’ emotions—was proven to contribute, in a synergistic way with empathy, to increasing empathic ability. Clinical communication skills represent a key component in medical students in order to achieve the best patient care, and they are certainly related and/or influenced by empathy, interprofessional collaboration skills, emotional intelligence and, especially, personality traits. Taking into account the complex interactions mentioned above, the implementation of effective courses based on these concepts in medical students, intending to promote the development of clinical communication skills, represents a real emergency, since it might result in a reduction in medical errors and subsequent related deaths. A thorough understanding of students’ personality is mandatory before designing these courses in order to provide a training tailored to their personality styles.
1. Introduction
The ways people think, feel, and behave impact their daily social interactions and should be properly assessed and trained whenever possible, especially in terms of professions that require interhuman interactions. The medical profession is by far the most peculiar of all in terms of communication, since it might act dichotomously resulting in either a strong doctor–patient partnership or, on the contrary, in a poor relationship defined by a lack of trust and respect, which will have a major negative impact on a patient’s treatment outcome. However, the importance of medical communication is not always fully acknowledged and valued properly during medical education; once medical students graduate and begin to practice, they become aware of this crucial gap in their education. Moreover, this reflects on their medical actions and decreases their quality considerably. Medical communication should be based on empathy, defined as a complex social emotion consisting of the ability to identify and understand the feelings and thoughts of others and to respond with adequate emotions [1,2,3]. In terms of the medical profession, the concept of empathy was specified as being defined as a major cognitive attribute that implies the quality of understanding a patient’s concerns, experiences and perspective, as well as communicating this perception with the aim of helping them [4]. Thus, we emphasise the close interdependence between personality, medical empathy and communication. Medical education should consist of a holistic approach in terms of implementing and monitoring appropriate training strategies for developing proper communication skills, but also for shaping certain personality traits in order to achieve the best level of communication with the future patient. Nevertheless, it is a well-documented fact that personality traits are influenced mostly by genetic background [5], a fact that might represent a real challenge in medical undergraduates, taking into account that genetic inheritance is the most difficult to be modified or trained. Albeit minor, the influence of social skills on the development of personality should not be neglected, since it is the main component that could be modified with proper education.
Personality traits were also proven to be essential for medical students in choosing the most suitable specialty [6] based on a proper assessment and fair acknowledgement of their self-strengths and limitations. This takes into account that professional satisfaction influences not only the doctor’s quality of life and performance, but also the patient’s outcome. Thus, medical educators should also focus their attention on guiding undergraduates in making the best choice based on their personality and personal interests. Several studies proved that medical students reported personal satisfaction and interest as the most important factors that influenced their decision when choosing their specialty [7]. As additional proof of the complex relationship between personality traits, medical empathy and communication were stated by Hojat et al., who emphasised that a proper understanding of this relationship would not only guide specialty choice, but could also be helpful in selecting students that match the medical profession by predicting possible behaviours [4]. Medical performance represents the top of the pyramid built on personality traits, medical empathy, and communication—the final supreme goal of each physician.
Interprofessional collaboration, teamwork and multidisciplinary approach represent highly desirable skills in the medical profession, taking into account the current medical trends that support and focus on inter- and multidisciplinary medical teams for conveying patient safety, trust, and improving their outcomes [6]. The World Health Organisation emphasised the major importance of interprofessional teamwork in the medical field by implementing medical training focused on developing students’ collaboration skills [8]. However, certain personality traits such as neuroticism and introversion might display a negative influence on interprofessional collaboration if not shaped properly during medical school in order to diminish traits that alter this collaboration as much as possible.
Based on these aforementioned facts, we might state that personality traits represent the core of medical performance, irrespective of their chosen specialty, and a thorough understanding and assessment of these traits are the missing puzzle piece for implementing proper medical training and improving patient outcomes.
Thus, the main aim of this narrative overview was to underline the impact of personality traits on a physician’s work, academic satisfaction, and their patient’s outcome.
2. Literature Search
An electronic literature search was performed for the present review on the lines of search for a narrative overview, including three databases: PubMed, Google Scholar and EMBASE. We used the following search terms: ‘personality traits’, ‘medical empathy’, ‘interprofessional collaboration’, ’career choice’, ‘emotional intelligence’, and ‘professional satisfaction’ (Figure 1). We should mention that Google Scholar was an auxiliary database used if the full text of a particular article was not found in PubMed or Embase. The inclusion criteria consisted of all types of articles that involved medical students, young residents or physicians, irrespective of the year of publication, in order to also highlight the progress of medical education in terms of acknowledging the importance of personality traits in the professional development of medical students. Each of the included articles was critically assessed according to the following: key results, quality of the results, interpretation of the results, suitability of the methods used to verify the hypothesis, limitations, and impact of conclusions to the field [9]. Moreover, we applied critical reading tools for scientific articles according to Jean-Baptist du Prel et al. [10], by analysing the study design of each article, the structure, the role of each section, as well as the potential sources of bias and limitations. Thus, analysis and inference were the most reliable critical reading tools used for the assessment of articles included in this review. We excluded articles that did not fit to the aforementioned criteria, as well as articles that were not written in English and those for which the full text was not available. We also identified additional references that fulfilled our criteria by a manual search of the reference list from the articles retrieved in the first round of search, for which we followed the same steps before including them in the review. We synthetized the findings from the remaining articles, highlighting both the similarities and inconsistencies between them in order to provide an objective narrative overview related to the impact of personality traits on a physician’s work, academic satisfaction, and their patient’s outcome. The methodological characteristics of the research-type studies included in this review are described in Table 1.
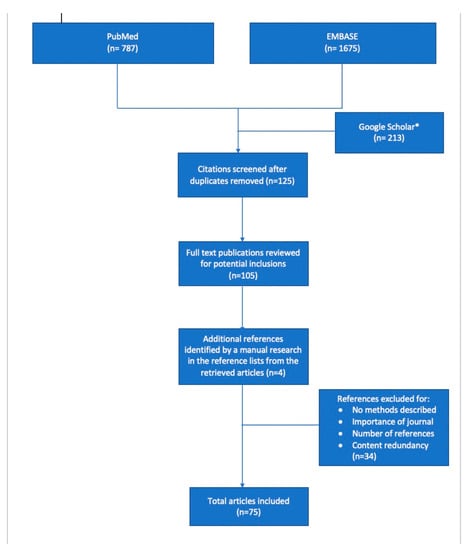
Figure 1.
Flowchart of the literature selection. * Google Scholar was an auxiliary database used if the full text of a particular article was not found in PubMed or Embase.

Table 1.
The methodological characteristics of the research-type studies included in this review.
3. Personality Traits in Medical Students—The Core of the Doctor–Patient Relationship
As mentioned above, each individual has their own way of thinking, behaving and expressing feelings or emotions, characteristics that define an individual’s personality. Moreover, personality is known as one of the most crucial aspects of human life [11]. It is also known to influence all human behaviours in both personal and social life, but it might also trigger important conflicts with a person’s surroundings in the setting of incompatible traits and characteristics [12]. Two famous personality theorists, Zweig and Webster, emphasise that the differences in an individual’s personality represent probably the most important factor that influences a human’s motivation in learning, performance, and behaviour, considering that all the controversies in areas such as thinking, intelligence, perception, emotions, learning, and motivation are based on this issue [11]. Taking into account that effective doctor–patient communication represents the cornerstone of patient- and family-centred care, medical training should focus on improving personality traits that influence this communication. Nevertheless, this fact cannot be achieved without a proper assessment of personality traits.
One of the most frequently used tools for assessing personality is represented by the ‘big-five model’ and its derivatives, e.g., Personality Inventory NEO-PI-R [13]. The big-five model or the five-factor model has been used for assessing intercultural differences among different countries, defining the underlying qualities of personality traits [57,58]. Thus, the big-five model is based on the assessment of five dimensions of personality and its related facets, six for each dimension: Openness, facets—fantasy, aesthetics, feelings, actions, ideas, values; Extraversion, facets—warmth, gregariousness, assertiveness, activity, excitement-seeking, positive emotions; Conscientiousness, facets—competence, order, dutifulness, achievement striving, self-discipline, deliberation; Agreeability, facets—trust, straightforwardness, altruism, compliance, modesty, tender-mindedness; Neuroticism, facets—anxiety, angry hostility, depression, self-consciousness, impulsiveness, vulnerability [14,59]. Each of these dimensions is related to specific personality aspects and defines particular personality subdimensions. Thus, Openness is related to an individual’s intellectual interests, culture and openness to experiences [15]. Extraversion is a reliable indicator of energy, enthusiasm, sociability, orientation towards others and task perseverance [60,61]. Conscientiousness is another personality dimension that implies prudence, responsibility, moral integrity, the need for structure and order, as well as perseverance in action [60]. Interpersonal relationships represent a fair reflection of agreeability, which is related to altruism, goodwill, gentleness, direct behaviour and trust in people [60]. Emotional Stability or Neuroticism is associated with depression, impulsivity, anxiety, vulnerability and the tendency to worry [60]. This model was assessed in multiple general studies, but unfortunately, its utility in medical students is far from being properly assessed. Taking into account the great impact of their personality on their professional skills and performance, a proper understanding of their personality would be of great benefit during medical school.
Professional satisfaction is a strong hallmark of wellbeing during adulthood. In terms of the medical profession, this is choosing a specialty that matches best with an individual’s personality traits. Multiple factors were identified as essential contributors for medical specialty choice such as personality, gender, personal interest, economic status, clinical experience during clerkship, mentoring from professor, expected income, lifestyle, family or public media influence [16,17,18]. Thus, extrinsic factors display a greater influence on a student’s decision when choosing their specialty. Nevertheless, personality remains a major determinant in specialty decision making. Taking into account the major impact of this choice on public medical services and policy on medical education, each career counsellor or professor that mentors medical students should focus more on finding an effective method to assess their personality [62]. Moreover, a proper assessment of personality traits might predict performance in carrying out tasks entailed by each medical specialty [6]. Thus, we are definitely entitled to say that ‘one must be born’ for a certain medical profession in order to achieve the desired performance. A recent study performed on medical students aimed to identify the relationship between specialty choice and personality traits, and concluded that students with more Agreeableness preferred clinical medicine instead of basic medicine [6]. The authors also underlined that students with an increased level of Openness intended to choose medical departments [6]. Openness was also proved to be directly related to satisfaction and personal interest when choosing the medical specialty [6]. Unsurprisingly, age was shown to influence certain personality traits such as Conscientiousness and Agreeableness, which seem to be higher in older students [6]. Another study that compared surgical residents with the general population in terms of personality traits pointed out that surgeons scored significantly higher for Extraversion, Conscientiousness and Openness [19]. According to the study of Hoffman et al., who compared the personalities of surgical residents, nonsurgical residents and medical students, surgical residents scored better for Conscientiousness and Extraversion, but worse for Openness than medical students [20]. Thus, previous studies emphasised the fact that surgeons possess a particular personality distinct from that of trainees in other medical specialties or the general population [19,63], suggesting there is an innate character of their personality that enables them to perform this specialty. Nevertheless, the question of whether surgeons are born or made is rather challenging. Thus, a recent study performed on surgical trainees and medical students who intend to pursue a surgical specialty proved that the two groups display multiple similarities regarding both personality traits and learning styles [21], indicating that most likely an innate personality is required for this profession and these traits are neither learnt or developed during surgical training. Both groups included in this study scored high for Conscientiousness, Agreeableness and Openness, and low for Neuroticism [21]. These findings suggest that trainees adjust their Neuroticism during residency programs and become more emotionally stable over the course of surgical training, experiencing lower anxiety and depression levels as compared to undergraduates that aim to pursue a surgical career. Moreover, the combination between increased levels of Conscientiousness, Agreeableness and Openness and lower levels of Neuroticism might represent the key attribute for enabling students to accept better and cope with the tasks and rigor of a stressful residency program such as surgical training. Thus, personality testing should be mandatory during medical education since it was clearly showed that personality profiling is an extremely useful tool for distinguishing between high- and low-performing residents [22]. Taking into account the crucial impact of the match between personality traits and medical career on the health care services and national economy, each university should implement a program designed for personality testing during the medical training in order to properly guide medical students in their specialty choice.
Interprofessional collaboration between healthcare providers is essential in order to achieve the best outcome for each patient and improve patient safety. Thus, the collaboration of different healthcare professionals in well-functioning teams by contributing with their specific knowledge related to each medical specialty, resulting in a holistic approach, will definitely impact both medical performance and patient satisfaction [22,64]. Interprofessional education is meant to provide students opportunities to develop, train, and learn collaboration skills and each medical university should implement this type of education as a regular training, since it is often challenging to achieve good interprofessional teamwork [64]. It is true that awareness regarding the need for interprofessional education during medical school has increased considerably during the last few years, but students’ attitudes towards this type of training remain an issue since they seem to be influenced by multiple factors such as gender, learning styles or personality traits [8,23,24,25,26,27]. Thus, once more, we emphasise that a thorough understanding of personality traits in medical students could considerably improve their attitudes towards interprofessional education and collaboration by providing teachers the opportunity to design proper teaching methods adjusted to medical students’ personality traits and their preferences for different learning styles.
Medical empathy, defined as the ability to understand a patient’s experiences, concerns, and perspectives and to express this understanding in their favour [24], is another essential concept that contributes to effective patient–physician communication, improving patient trust, compliance, and satisfaction in order to achieve the best outcome in clinical practice [28]. Thus, it was fairly stated that the physician’s performance, clinical skills, and biomedical knowledge are strongly influenced by empathy and emotional abilities, which, in turn, are shaped by personality [29]. In terms of personality traits, Openness and Agreeableness were proven to be positively correlated with empathy [30]. Moreover, it seems that empathy is also positively correlated with two other personality dimensions, i.e., Conscientiousness and Extraversion [1]. Nevertheless, it is also true that increased empathy might result in emotional fatigue, increased risk of stress, and subsequent ‘burn out’ [65]. Self-assessment and understanding of personality traits could considerably decrease the previously mentioned risks by approaching suitable training strategies in order to improve unfavourable traits. The main daily goal for each physician is to provide the best of care for their patients and, therefore, the relationship between empathy, emotional intelligence, and personality was found to be the main factor that contributes to successful achievement of this goal. Multiple studies proved that emotional intelligence is associated with increased empathy, improved patient–physician relationship, teamwork, communication skills, stress management, and leadership resulting in higher academic performance [31,32,65]. The relationship between emotional intelligence and personality is further emphasised by the fact that the first one includes the ability to understand, perceive, and manage self-emotions, but also to perceive and understand the emotions of other humans [66]. In spite of their inherited and innate pattern, studies proved that emotional intelligence and empathy can be improved through proper education, implying an urgent need to implement communication training in medical students, since they seem to have a positive influence on both emotional intelligence and empathy [33,34,67]. Thus, an effective program designed for enhancing emotional intelligence and empathy in medical students should definitely take into account students’ personality [35,67,68]. The implementation of such a program during medical school is crucial, since it was proved that empathy declines during academic medical school training [36]. In addition, the decreasing pattern of empathy continues after they begin to practice their profession, since a doctor’s life is best characterised by resulting in an impairment of personality traits and devotion to patients. Therefore, programs for enhancing empathy would be of major benefit for improving professional experiences and performance.
A close interplay between personality traits, empathy, and interprofessional collaboration was emphasised by recent studies, which proved that empathy is positively associated with collaborative interprofessional work in postgraduates who are at the beginning of their specialisation [37], being well-documented that both empathy and interprofessional work are influenced by personality traits. Moreover, it was underlined that general empathy might be predicted by different personality styles, such as styles of protection, sensation, and accommodation [38]. In terms of interprofessional collaboration and communication skills, it was noticed that individuals that display a greater degree of empathy find it easier to accept failures in their life, being more optimistic regarding the future, motivated to satisfy others first, and trying to change their environment to fulfil their goals [38]. According to Zaki et al., empathy is a motivated phenomenon implying a close interaction between social desirability and intrinsic motivation [69]. Thus, a student’s self-efficacy is moderated mainly by two motivational factors, i.e., value of the goal for which they work and the expectation to achieve that goal [39]. Nevertheless, intrinsic motivation and self-efficacy are not enough to achieve the goal in medicine if not supported by empathy. The complexity of practicing and understanding empathy in clinical situations requires a solid basis provided by intense training in terms of personal development, relationship and system maintenance, chance, and goal progress [40].
Emotional intelligence is another crucial ability for medical students, since it represents a measure of emotional awareness and the capacity to respond to one’s own and others’ emotions. Thus, Mayer and Salovey stated that emotional intelligence ability implies not only the ability to perceive and integrate emotion, but also to understand and regulate emotion in order to favour personal growth [29,70]. The Accreditation Council for Graduate Medical Education defined emotional intelligence competency as a set of assessment methods for interpersonal and communication skills, patient care, and professional behaviours in residents [71]. Thus, 12 abilities were related to emotional intelligence competency: emotional self-awareness, emotional self-control, achievement orientation, adaptability, empathy, positive outlook, coach and mentor, organisational awareness, influence, inspirational leadership, teamwork, and conflict management, which represent, along with empathy, the most important traits of 21st century physicians [41]. An increased level of emotional intelligence was shown to positively influence doctor–patient relationship, teamwork, communication skills, level of empathy, organisation commitment, as well as stress management [31,32,65,72]. Emotional intelligence and empathy synergistically contribute to increasing empathic ability [29]. One of the most important deficiencies in medical students is a lack of confidence and resources to implement empathic behaviour, despite them fully acknowledging and understanding its value [29], emphasising once more the need for proper dedicated training during medical school. Therefore, medical education should focus not only on improving empathy and empathic behaviour in medical students, but also promoting and teaching methods for its effective implementation in residents and young physicians. Emotional intelligence is definitely influenced by personality. A recent study performed on US medical students, which focused on assessing emotional intelligence, revealed a strong positive association with Extraversion, a moderate positive one with Conscientiousness, Agreeability and Openness, as well as a weak negative association with Neuroticism [35]. Moreover, Conscientiousness and Openness were found to be reliable predictors for medical students’ competencies in clinical contexts [42]; Openness and Agreeability promote the development of patient–physician relationships [43], as well as training proficiency [73]; and Conscientiousness was identified as the most important trait required for effective task completion [74]. Considering the complex aforementioned findings, emotional intelligence has an incontestable influence on patient–physician relationships, medical students’ and physicians’ communication skills, professional performance, and proficiency, creating important bridges with empathy and interprofessional collaboration skills under the close guidance of personality traits.
Clinical communication skills represent the key component in medical students in order to achieve the best patient care, and they are certainly related and/or influenced by empathy, interprofessional collaboration skills, emotional intelligence, and especially personality traits. Nevertheless, effective communication between physician and patient/caregivers represents the ‘cornerstone’ of care by improving the patient’s outcome. Good communication skills improve not only the physical but also the mental health of patients, increasing their compliance and satisfaction regarding the provided care [44]. The physician’s ability to communicate and their knowledge represent two major factors that equally contribute to the patient’s outcome [45]. In addition, personality traits were proven to also affect attitudes regarding communication skills training, although these skills are currently considered a crucial attribute for all people working in primary health care systems [46]. Medical errors, a continuous cause of death displaying an increasing pattern worldwide, seem to be mainly related to a major lack of communication skills [47]. It is indeed a real fact that the current trends in medicine focus on the acquisition of proper communication skills in medical students and not only on enhancing the theoretical aspects of each medical field, underlining that these skills should be considered when determining physicians’ competence [11]. Thus, medical educators should pay close attention and combine students’ personality and the ability to learn the communication skills in order to develop effective communication skills training to reduce medical errors in the long run [45]. Based on these findings, we hypothesise that physicians’ appropriate and effective ability to communicate might result in a considerable reduction in medical errors and subsequent deaths. Medical educators should also focus on increasing students’ awareness regarding the importance of learning communication skills, since it was underlined that they find no merit in improving these skills because they do not acknowledge them as an important aspect of medical and practical education [11]. This fact is rather concerning considering the effectiveness of students’ attitudes and satisfaction with learning in motivating and promoting knowledge quality [45]. Recent studies focusing on medical students’ personality traits and their attitude towards learning communication skills concluded that anxiety was associated with a negative perspective regarding communication skills training during medical school [48,49], while students with increased sociability levels were found to have a positive attitude towards this training [45,48]. Moreover, Agreeableness, Extraversion, and Conscientiousness were positively correlated with medical students’ attitudes regarding the interaction with patients, underlining that these personality dimensions might also be related to students’ attitudes in terms of communication [50]. Contrariwise, aggression/hostility represents the main characteristic of antisocial and bold behaviours, and it was associated with a negative attitude towards learning communication skills, since individuals with this type of personality express no interest in communicating with others by lacking this desired attitude [45].
The importance of clinically focused skills and behaviours in medical education has been acknowledged by both the Association of American Medical Colleges and the European Board of Internal Medicine for over a decade [75,76]. The competencies related to clinical communication skills and to clinical practice include trust building; respect; compassion; altruism; empathy; understanding patient’s spirituality, beliefs and meaning; professionalism; information sharing and mutual decision making; relationship building; cultural sensitivity; responsiveness to distress; appreciation of psychological factors; self-awareness; ethical issues; and acting with honesty [75,76]. These competencies were related to personality dimensions in several studies, but the results remain contradictory depending on the studied populations. Therefore, Sims et al. assessed the relationship between personality traits and communication skills in adults and showed that Agreeableness and Openness might predict assertiveness and empathic listening in communication [51]. Contrariwise, a study performed on psychology students revealed no significant correlation between the same neither before nor after communication training [52]. Studies performed on medical students remain scarce. Nevertheless, Agreeableness, Openness, and Extraversion were found to be the most important factors that positively influence students’ attitude towards communication and learning, enhancing a better connection between the patient and physician [53]. Moreover, each of these dimensions were proven to have a major contribution to achieving the ultimate goal of improving students’ attitudes towards communication in different ways: Agreeableness enables students to initiate a relationship with patients easier by providing the tendency to be friendly [54], Openness promotes the better acceptance of adversity and willingness to change [55], while Extraversion favours energy to social interaction better expressing the inner disposition [56]. Based on all these evidence-based statements, medical teachers should focus more on assessing students’ personality traits and implement their teaching activities tailored accordingly or even support the development of personality dimensions that favour an effective doctor–patient communication.
4. Conclusions
The relationship between physician and patient represents the core of medicine and all efforts should focus on improving this relationship. A thorough assessment of medical students’ personality traits is crucial for educators in order to acknowledge the main deficiencies in their students and to design effective tailored communication and clinical practice training for improving and educating these deficiencies. Professional satisfaction is definitely influenced by career choice, which should be properly guided after an individual assessment of personality traits. Interprofessional collaboration and teamwork are mandatory for patient safety and medical students should be made aware of its importance even before graduating. Emotional intelligence and empathy act as partners for improving empathic ability in order to reach the best doctor–patient relationship. Empathy is positively influenced by being positively correlated with Openness, Agreeableness, Conscientiousness, and Extraversion, and thus, training should focus on improving these components in medical students. The ultimate goal of the medical profession is to achieve the best outcome for each patient. Empathy, emotional intelligence, and clinical communication skills are essential for building an effective doctor–patient relationship, while interprofessional collaboration and teamwork are mandatory for assuring the best of care in practice, altogether being closely governed by personality traits and crucial for providing the best outcome for the patients. Taking into account students’ personality traits, courses should aim to improve empathy, clinical communication skills, interprofessional collaboration, teamwork, and practical competencies for the patients’ best outcomes. Thus, proper training should begin in medical students and should never end.
Author Contributions
N.S.—Conceptualisation, Data curation, Investigation, Methodology, Project administration, Visualisation, Writing—original draft, Writing—review and editing, C.O.M.—Conceptualisation, Project administration, Visualisation, Supervision, Writing—original draft, Writing—review and editing, L.E.M.—Conceptualisation, Visualisation, Writing—original draft, Writing—review and editing. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of the University of Medicine, Pharmacy, Sciences and Technology from Târgu Mureș (No. 1157/20.10.2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Guilera, T.; Batalla, I.; Forné, C.; Soler-González, J. Empathy and Big Five Personality Model in Medical Students and Its Relationship to Gender and Specialty Preference: A Cross-Sectional Study. BMC Med. Educ. 2019, 19, 57. [Google Scholar] [CrossRef]
- Baron-Cohen, S.; Wheelwright, S. The Empathy Quotient: An Investigation of Adults with Asperger Syndrome or High Functioning Autism, and Normal Sex Differences. J. Autism Dev. Disord. 2004, 34, 163–175. [Google Scholar] [CrossRef] [PubMed]
- Sulzer, S.H.; Feinstein, N.W.; Wendland, C.L. Assessing Empathy Development in Medical Education: A Systematic Review. Med. Educ. 2016, 50, 300–310. [Google Scholar] [CrossRef] [PubMed]
- Hojat, M.; Gonnella, J.S. Eleven Years of Data on the Jefferson Scale of Empathy-Medical Student Version (JSE-S): Proxy Norm Data and Tentative Cutoff Scores. Med. Princ. Pract. Int. J. Kuwait Univ. Health Sci. Cent. 2015, 24, 344–350. [Google Scholar] [CrossRef]
- Yusoff, M. Which Personality Traits Have Favourable Impact on Psychological Health during Stressful Condition? Educ. Med. J. 2018, 10, 35–42. [Google Scholar] [CrossRef][Green Version]
- Kwon, O.Y.; Park, S.Y. Specialty Choice Preference of Medical Students According to Personality Traits by Five-Factor Model. Korean J. Med. Educ. 2016, 28, 95–102. [Google Scholar] [CrossRef]
- McCrae, R.R.; Costa, P.T. Reinterpreting the Myers-Briggs Type Indicator from the Perspective of the Five-Factor Model of Personality. J. Personal. 1989, 57, 17–40. [Google Scholar] [CrossRef] [PubMed]
- Olsson, C.; Lachmann, H.; Kalén, S.; Ponzer, S.; Mellstrand Navarro, C. Personality and Learning Styles in Relation to Attitudes towards Interprofessional Education: A Cross-Sectional Study on Undergraduate Medical Students during Their Clinical Courses. BMC Med. Educ. 2020, 20, 398. [Google Scholar] [CrossRef] [PubMed]
- Derish, P.A.; Annesley, T.M. How to Write a Rave Review. Clin. Chem. 2011, 57, 388–391. [Google Scholar] [CrossRef]
- Du Prel, J.-B.; Röhrig, B.; Blettner, M. Critical Appraisal of Scientific Articles: Part 1 of a Series on Evaluation of Scientific Publications. Dtsch. Arztebl. Int. 2009, 106, 100–105. [Google Scholar] [CrossRef]
- Tamannaeifar, M.; Mansourinik, A. The Relationship between Personality Characteristics, Social Support and Life Satisfaction with University Students’ Academic Performance. Q. J. Res. Plan. High. Educ. 2014, 20, 149–166. [Google Scholar]
- Nasri, S.; Heydari Bafghi, R.; Jararh, J. Personality Characteristics, Irrational Beliefs, and Communication Skills as Predictors School Counselors’ Job Performance. Biannu. J. Appl. Couns. 2017, 7, 27–46. [Google Scholar] [CrossRef]
- Vassend, O.; Skrondal, A. The NEO Personality Inventory Revised (NEO-PI-R): Exploring the Measurement Structure and Variants of the Five-Factor Model. Personal. Individ. Differ. 2011, 50, 1300–1304. [Google Scholar] [CrossRef]
- Lievens, F.; Coetsier, P.; De Fruyt, F.; De Maeseneer, J. Medical Students’ Personality Characteristics and Academic Performance: A Five-Factor Model Perspective. Med. Educ. 2002, 36, 1050–1056. [Google Scholar] [CrossRef] [PubMed]
- Han, S.; Pistole, M.C. Big Five Personality Factors and Facets as Predictors of Openness to Diversity. J. Psychol. 2017, 151, 752–766. [Google Scholar] [CrossRef] [PubMed]
- Borges, N.J.; Stratton, T.D.; Wagner, P.J.; Elam, C.L. Emotional Intelligence and Medical Specialty Choice: Findings from Three Empirical Studies. Med. Educ. 2009, 43, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Hojat, M.; Zuckerman, M. Personality and Specialty Interest in Medical Students. Med. Teach. 2008, 30, 400–406. [Google Scholar] [CrossRef]
- Lambert, E.M.; Holmboe, E.S. The Relationship between Specialty Choice and Gender of U.S. Medical Students, 1990–2003. Acad. Med. J. Assoc. Am. Med. Coll. 2005, 80, 797–802. [Google Scholar] [CrossRef]
- McGreevy, J.; Wiebe, D. A Preliminary Measurement of the Surgical Personality. Am. J. Surg. 2002, 184, 121–125. [Google Scholar] [CrossRef]
- Hoffman, B.M.; Coons, M.J.; Kuo, P.C. Personality Differences between Surgery Residents, Nonsurgery Residents, and Medical Students. Surgery 2010, 148, 187–193. [Google Scholar] [CrossRef]
- Preece, R.A.; Cope, A.C. Are Surgeons Born or Made? A Comparison of Personality Traits and Learning Styles Between Surgical Trainees and Medical Students. J. Surg. Educ. 2016, 73, 768–773. [Google Scholar] [CrossRef] [PubMed]
- Foster, K.N.; Neidert, G.P.M.; Brubaker-Rimmer, R.; Artalejo, D.; Caruso, D.M. A Psychological Profile of Surgeons and Surgical Residents. J. Surg. Educ. 2010, 67, 359–370. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, T.; Shinozaki, H.; Makino, T.; Ogawara, H.; Asakawa, Y.; Iwasaki, K.; Matsuda, T.; Abe, Y.; Tozato, F.; Koizumi, M.; et al. Changes in Attitudes toward Interprofessional Health Care Teams and Education in the First- and Third-Year Undergraduate Students. J. Interprof. Care 2012, 26, 100–107. [Google Scholar] [CrossRef]
- Wilhelmsson, M.; Ponzer, S.; Dahlgren, L.-O.; Timpka, T.; Faresjö, T. Are Female Students in General and Nursing Students More Ready for Teamwork and Interprofessional Collaboration in Healthcare? BMC Med. Educ. 2011, 11, 15. [Google Scholar] [CrossRef]
- Alghasham, A.A. Effect of Students’ Learning Styles on Classroom Performance in Problem-Based Learning. Med. Teach. 2012, 34 (Suppl. 1), S14–S19. [Google Scholar] [CrossRef]
- Tariq, S.; Khan, M.A.; Afzal, S.; Shahzad, S.R.; Hamza, M.; Khan, H.A.; Qamar, F.; Javed, M.; Ashraf, M.F.; Mubarak, F.; et al. Association between Academic Learning Strategies and Annual Examination Results among Medical Students of King Edward Medical University. Ann. King Edw. Med. Univ. 2016, 22. [Google Scholar] [CrossRef]
- Avrech Bar, M.; Katz Leurer, M.; Warshawski, S.; Itzhaki, M. The Role of Personal Resilience and Personality Traits of Healthcare Students on Their Attitudes towards Interprofessional Collaboration. Nurse Educ. Today 2018, 61, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Hojat, M.; Spandorfer, J.; Louis, D.Z.; Gonnella, J.S. Empathic and Sympathetic Orientations toward Patient Care: Conceptualization, Measurement, and Psychometrics. Acad. Med. J. Assoc. Am. Med. Coll. 2011, 86, 989–995. [Google Scholar] [CrossRef] [PubMed]
- Abe, K.; Niwa, M.; Fujisaki, K.; Suzuki, Y. Associations between Emotional Intelligence, Empathy and Personality in Japanese Medical Students. BMC Med. Educ. 2018, 18, 47. [Google Scholar] [CrossRef]
- Costa, P.; Alves, R.; Neto, I.; Marvão, P.; Portela, M.; Costa, M.J. Associations between Medical Student Empathy and Personality: A Multi-Institutional Study. PLoS ONE 2014, 9, e89254. [Google Scholar] [CrossRef]
- Chew, B.H.; Zain, A.M.; Hassan, F. Emotional Intelligence and Academic Performance in First and Final Year Medical Students: A Cross-Sectional Study. BMC Med. Educ. 2013, 13, 44. [Google Scholar] [CrossRef]
- Aithal, A.P.; Kumar, N.; Gunasegeran, P.; Sundaram, S.M.; Rong, L.Z.; Prabhu, S.P. A Survey-Based Study of Emotional Intelligence as It Relates to Gender and Academic Performance of Medical Students. Educ. Health Abingdon Engl. 2016, 29, 255–258. [Google Scholar] [CrossRef]
- Magalhães, E.; Costa, P.; Costa, M.J. Empathy of Medical Students and Personality: Evidence from the Five-Factor Model. Med. Teach. 2012, 34, 807–812. [Google Scholar] [CrossRef] [PubMed]
- Hojat, M.; Axelrod, D.; Spandorfer, J.; Mangione, S. Enhancing and Sustaining Empathy in Medical Students. Med. Teach. 2013, 35, 996–1001. [Google Scholar] [CrossRef]
- Bertram, K.; Randazzo, J.; Alabi, N.; Levenson, J.; Doucette, J.T.; Barbosa, P. Strong Correlations between Empathy, Emotional Intelligence, and Personality Traits among Podiatric Medical Students: A Cross-Sectional Study. Educ. Health Abingdon Engl. 2016, 29, 186–194. [Google Scholar] [CrossRef]
- Youssef, F.F.; Nunes, P.; Sa, B.; Williams, S. An Exploration of Changes in Cognitive and Emotional Empathy among Medical Students in the Caribbean. Int. J. Med. Educ. 2014, 5, 185–192. [Google Scholar] [CrossRef]
- San-Martín, M.; Roig-Carrera, H.; Villalonga-Vadell, R.M.; Benito-Sevillano, C.; Torres-Salinas, M.; Claret-Teruel, G.; Robles, B.; Sans-Boix, A.; Alcorta-Garza, A.; Vivanco, L. Empathy, inter-professional collaboration, and lifelong medical learning in Spanish and Latin-American physicians-in-training who start their postgraduate training in hospitals in Spain. Preliminary outcomes. Aten. Primaria 2017, 49, 6–12. [Google Scholar] [CrossRef][Green Version]
- Dávila-Pontón, Y.; Reyes-Reyes, A.; Calzadilla-Núñez, A.; Utsman, R.; Torres-Martínez, P.; Díaz-Narváez, V. Empathy and Personality Styles in Medical Students. Rev. Colomb. Psicol. 2020, 29, 73–87. [Google Scholar] [CrossRef]
- Ratelle, C.F.; Guay, F.; Vallerand, R.J.; Larose, S.; Senecal, C. Autonomous, Controlled, and Amotivated Types of Academic Motivation: A Person-Oriented Analysis. J. Educ. Psychol. 2007, 99, 734–746. [Google Scholar] [CrossRef]
- Doménech-Betoret, F.; Abellán-Roselló, L.; Gómez-Artiga, A. Self-Efficacy, Satisfaction, and Academic Achievement: The Mediator Role of Students’ Expectancy-Value Beliefs. Front. Psychol. 2017, 8, 1193. [Google Scholar] [CrossRef]
- Webb, A.R.; Young, R.A.; Baumer, J.G. Emotional Intelligence and the ACGME Competencies. J. Grad. Med. Educ. 2010, 2, 508–512. [Google Scholar] [CrossRef] [PubMed]
- Gough, H.G.; Bradley, P.; McDonald, J.S. Performance of Residents in Anesthesiology as Related to Measures of Personality and Interests. Psychol. Rep. 1991, 68, 979–994. [Google Scholar] [CrossRef]
- LePine, J.A.; Colquitt, J.A.; Erez, A. Adaptability to Changing Task Contexts: Effects of General Cognitive Ability, Conscientiousness, and Openness to Experience. Pers. Psychol. 2000, 53, 563–593. [Google Scholar] [CrossRef]
- Shankar, P.; Dubey, A.; Balasubramanium, R.; Dwivedi, N. Student Attitude towards Communication Skills Learning in a Caribbean Medical School. Australas. Med. J. 2013, 6, 466–475. [Google Scholar] [CrossRef]
- Akbarilakeh, M.; Fargah, F.; Razjouyan, K.; Rahimzadeh, M. Predicating Attitude Toward Learning Communication Skills in Medical Students of Shahid Beheshti University. Dis. Diagn. 2020, 9, 21–25. [Google Scholar] [CrossRef]
- Gheirati, E.; Shabanifar, A.; Akhlaghi, M.; Peyman, N. Relationship Between Communication Skills and Mental Health Among the Students of Mashhad University of Medical Sciences, Mashhad, Iran. J. Sch. Public Health Inst. Public Health Res. 2016, 14, 61–72. [Google Scholar]
- Nami, K.; Ghalavandi, H.; Hosseinpoor, A.R. The Role of Students Personality Traits on Students Learning Style in University of Medical Sciences. Dev. Strateg. Med. Educ. 2014, 1, 59–68. [Google Scholar]
- Molinuevo, B.; Torrubia, R. Does Personality Predict Medical Students’ Attitudes to Learning Communication Skills? Int. J. Med. Educ. 2013, 4, 155–161. [Google Scholar] [CrossRef]
- Zare-Alamshiri, M.; Saber, S. Prediction of Communication Skills Based on Psycho-Social Class Atmosphere and Social Anxiety of High School Students. Community Health 2017, 4, 127–136. [Google Scholar]
- O’Tuathaigh, C.M.P.; Nadhirah Idris, A.; Duggan, E.; Costa, P.; Costa, M.J. Medical Students’ Empathy and Attitudes towards Professionalism: Relationship with Personality, Specialty Preference and Medical Programme. PLoS ONE 2019, 14, e0215675. [Google Scholar] [CrossRef]
- Sims, C.M. Do the Big-Five Personality Traits Predict Empathic Listening and Assertive Communication? Int. J. Listening 2017, 31, 163–188. [Google Scholar] [CrossRef]
- Kuntze, J.; van der Molen, H.T.; Born, M.P. Big Five Personality Traits and Assertiveness Do Not Affect Mastery of Communication Skills. Health Prof. Educ. 2016, 2, 33–43. [Google Scholar] [CrossRef]
- Franco, C.A.G.d.S.; Franco, R.S.; Cecilio-Fernandes, D.; Severo, M.; Ferreira, M.A. The Assessment of Personality Traits and Its Association with Learning Communication Skills. Sci. Med. Porto Alegre Online 2020, 30, 37326. [Google Scholar]
- Vermetten, Y.J.; Lodewijks, H.G.; Vermunt, J.D. The Role of Personality Traits and Goal Orientations in Strategy Use. Contemp. Educ. Psychol. 2001, 26, 149–170. [Google Scholar] [CrossRef] [PubMed]
- Holen, A.; Manandhar, K.; Pant, D.S.; Karmacharya, B.M.; Olson, L.M.; Koju, R.; Mansur, D.I. Medical Students’ Preferences for Problem-Based Learning in Relation to Culture and Personality: A Multicultural Study. Int. J. Med. Educ. 2015, 6, 84–92. [Google Scholar] [CrossRef]
- Tsou, K.-I.; Lin, C.-S.; Cho, S.-L.; Powis, D.; Bore, M.; Munro, D.; Sze, D.M.-Y.; Wu, H.-C.; Hsieh, M.-S.; Lin, C.-H. Using Personal Qualities Assessment to Measure the Moral Orientation and Personal Qualities of Medical Students in a Non-Western Culture. Eval. Health Prof. 2013, 36, 174–190. [Google Scholar] [CrossRef]
- Costa, P.T.; McCrae, R.R. Revised NEO Personality Inventory (NEO PI-R) and NEO Five-Factor Inventory (NEO-FFI); Psychological Assessment Resources: Odessa, FL, USA, 1992. [Google Scholar]
- Saucier, G.; Hampson, S.; Goldberg, L. Cross-language Studies of Lexical Personality Factors. In Advances in Personality Psychology; Hampson, S.E., Ed.; Psychology Press: Philadelphia, PA, USA, 2000; Volume 1, pp. 1–36. [Google Scholar]
- John, O.; Pervin, R.; Pervin, L. The Five-Factor Theory of Personality. In Handbook of Personality: Theory and Research; McCrae, R., Costa, P.J., Eds.; Guilford Press: New York, NY, USA, 2008; p. 171. [Google Scholar]
- Sava, F. Inventarul de Personalitate DECAS; ArtPress: Timişoara, Romania, 2008. [Google Scholar]
- Extraversion and Happiness: The Mediating Role of Social Support and Hope—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/30015375/ (accessed on 29 June 2021).
- Bennett, K.L.; Phillips, J.P. Finding, Recruiting, and Sustaining the Future Primary Care Physician Workforce: A New Theoretical Model of Specialty Choice Process. Acad. Med. J. Assoc. Am. Med. Coll. 2010, 85, S81–S88. [Google Scholar] [CrossRef]
- Thomas, J.H. The Surgical Personality: Fact or Fiction. Am. J. Surg. 1997, 174, 573–577. [Google Scholar] [CrossRef]
- Zwarenstein, M.; Goldman, J.; Reeves, S. Interprofessional Collaboration: Effects of Practice-Based Interventions on Professional Practice and Healthcare Outcomes. Cochrane Database Syst. Rev. 2009, CD000072. [Google Scholar] [CrossRef]
- Stoller, J.K.; Taylor, C.A.; Farver, C.F. Emotional Intelligence Competencies Provide a Developmental Curriculum for Medical Training. Med. Teach. 2013, 35, 243–247. [Google Scholar] [CrossRef]
- Petrides, K. Technical Manual for the Trait Emotional Intelligence Questionnaires (TEIQue), 1st ed.; 2nd Printing; London Psychometric Laboratory: London, UK, 2009. [Google Scholar]
- Cherry, M.G.; Fletcher, I.; O’Sullivan, H.; Shaw, N. What Impact Do Structured Educational Sessions to Increase Emotional Intelligence Have on Medical Students? BEME Guide No. 17. Med. Teach. 2012, 34, 11–19. [Google Scholar] [CrossRef]
- Johnson, D.R. Emotional Intelligence as a Crucial Component to Medical Education. Int. J. Med. Educ. 2015, 6, 179–183. [Google Scholar] [CrossRef] [PubMed]
- Zaki, J. Empathy: A Motivated Account. Psychol. Bull. 2014, 140, 1608–1647. [Google Scholar] [CrossRef]
- Goleman, D. Emotional Intelligence: Why It Can Matter More than IQ; Bantam Books: New York, NY, USA, 1995. [Google Scholar]
- ECFMG-ACGME Webinar: ACGME Core Competencies and Milestones. Available online: https://www.ecfmg.org/echo/webinars-acgme-core-competencies-2018.html (accessed on 22 September 2021).
- Arora, S.; Ashrafian, H.; Davis, R.; Athanasiou, T.; Darzi, A.; Sevdalis, N. Emotional Intelligence in Medicine: A Systematic Review through the Context of the ACGME Competencies. Med. Educ. 2010, 44, 749–764. [Google Scholar] [CrossRef] [PubMed]
- Barrick, M.R.; Mount, M.K. The Big Five Personality Dimensions and Job Performance: A Meta-Analysis. Pers. Psychol. 1991, 44, 1–26. [Google Scholar] [CrossRef]
- Burch, G.; Anderson, N. Personality as a Predictor of Working-Related Behavior and Performance: Recent Advances and Directions for Future Research. In International Review of Industrial and Organizational Psychology; Hodgkinson, G., Ford, J., Eds.; Wiley-Blackwell: Chichester, UK, 2008; pp. 261–305. [Google Scholar]
- The AAMC Project on the Clinical Education of Medical Students—MOAM.INFO. Available online: https://moam.info/the-aamc-project-on-the-clinical-education-of-medical-students_59fa642f1723dd0b1e9cf133.html (accessed on 25 September 2021).
- Palsson, R.; Kellett, J.; Lindgren, S.; Merino, J.; Semple, C.; Sereni, D.; EFIM/UEMS Working Group on Competencies in Internal Medicine in Europe. Core Competencies of the European Internist: A Discussion Paper. Eur. J. Intern. Med. 2007, 18, 104–108. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).