



Development and Usability Assessment of a Mobile App (Demensia KITA) to Support Dementia Caregivers in Malaysia: A Study Protocol

 ,
,
Abstract
:1. Introduction
1.1. Background
1.2. Study Rationale
1.3. Research Objectives
- To develop suitable and relevant content for the mobile application.
- To develop and design a mobile app prototype that uses the national language (Bahasa Malaysia) as the interface.
- To determine the usability of the mobile app among PLwD caregivers.
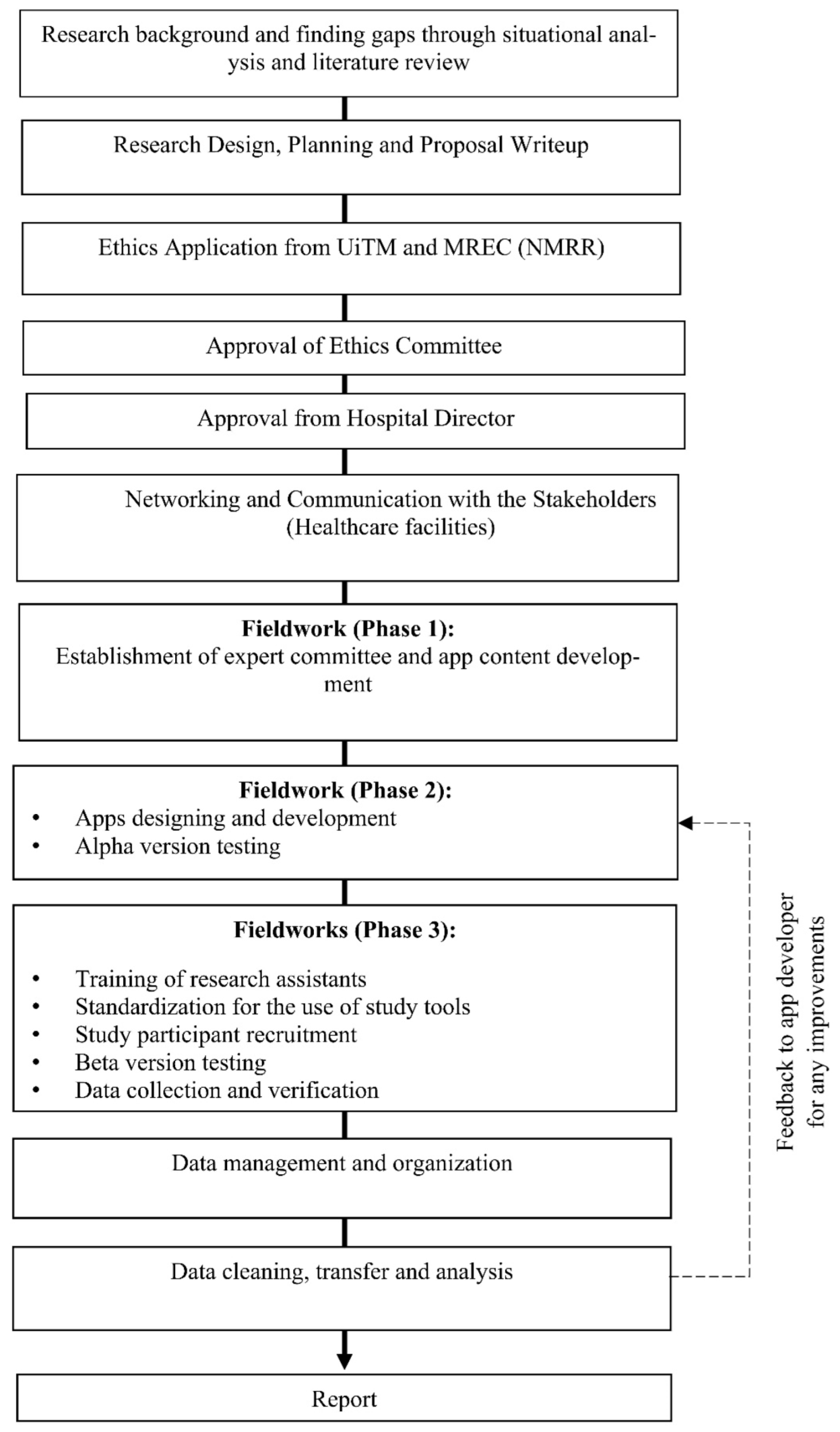
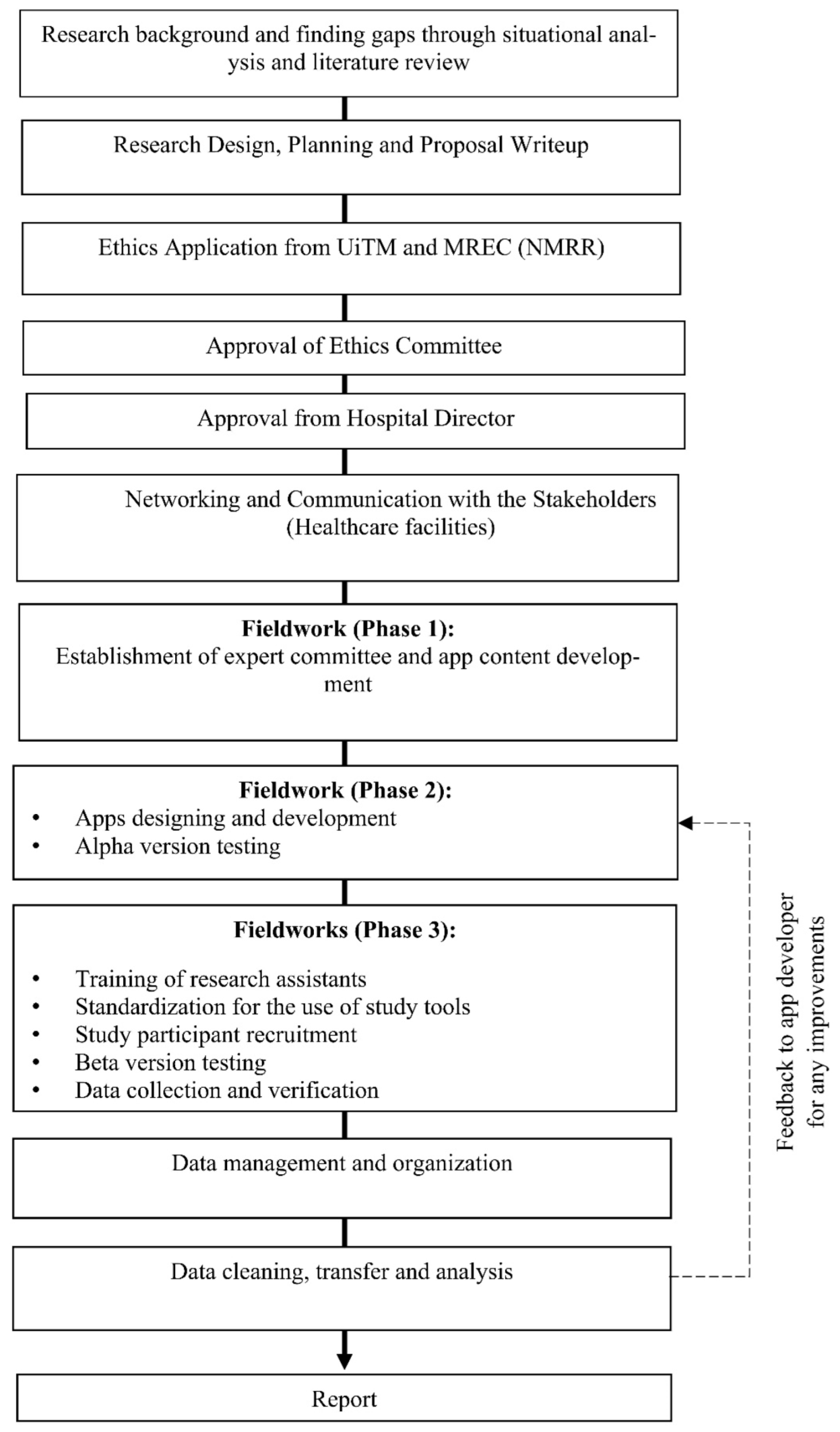
2. Methodology
Study Design
- 1.
- Nominal Group Technique (NGT)
- Aged ≥ 18 years old.
- Primary caregiver of a dependent person aged ≥ 60 years old diagnosed with any form of dementia.
- 2.
- Focus Group Discussion (FGD)
3. Expected Results
- i.
- Phase I:
- (a)
- Educational materials in a written form (i.e., behavioral, and psychological symptoms, pharmaceutical side effects, nutritional and oral health, and disease progression or complications).
- (b)
- Effective communication abilities (communication strategies or sharing experiences with other caregivers)
- (c)
- Reminders (e.g., medication diary and appointment with a physician for PLwD)
- (d)
- Psycho-spiritual assistance (e.g., a list of prayers or motivational quotes that are suited to the Malaysian cultural and religious ethos.)
- (e)
- Access to nearby healthcare facilities or local community resources (a directory of hospitals, geriatric units, dementia centers, non-governmental organizations, police, and fire stations)
- ii.
- Phase II:
- iii.
- Phase III:
4. Discussion
5. Limitations and Strengths
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wimo, A.; Guerchet, M.; Ali, G.C.; Wu, Y.T.; Prina, A.M.; Winblad, B.; Jönsson, L.; Liu, Z.; Prince, M. The worldwide costs of dementia 2015 and comparisons with 2010. Alzheimers Dement. 2017, 13, 1–7. [Google Scholar] [CrossRef] [PubMed]
- WHO Dementia. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 13 May 2022).
- Mattap, S.M.; Mohan, D.; McGrattan, A.M.; Allotey, P.; Stephan, B.C.M.; Reidpath, D.D.; Siervo, M.; Robinson, L.; Chaiyakunapruk, N. The economic burden of dementia in low- and middle-income countries (LMICs): A systematic review. BMJ Glob. Health 2022, 7, e007409. [Google Scholar] [CrossRef] [PubMed]
- Fam, J.; Mahendran, R.; Kua, E.H. Dementia care in low and middle-income countries. Curr. Opin. Psychiatry 2019, 32, 461–464. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention What Is Dementia? Available online: https://www.cdc.gov/aging/dementia/index.html#:~:text=Dementia%20is%20not%20a%20specific,a%20part%20of%20normal%20aging (accessed on 20 November 2021).
- Health in Aging Unique to Older Adults. Available online: https://www.healthinaging.org/a-z-topic/dementia/unique (accessed on 13 November 2021).
- United Nation. World Population Ageing 2019. In Measures of Population Ageing; Department of Economic and Social Affairs Population Division, United Nation: New York, NY, USA, 2019; Available online: https://www.un.org/en/development/desa/population/publications/pdf/ageing/WorldPopulationAgeing2019-Highlights.pdf (accessed on 16 June 2022).
- Cao, Q.; Tan, C.C.; Xu, W.; Hu, H.; Cao, X.P.; Dong, Q.; Tan, L.; Yu, J.T. The Prevalence of Dementia: A Systematic Review and Meta-Analysis. J. Alzheimers Dis. 2020, 73, 1157–1166. [Google Scholar] [CrossRef]
- Ganapathy, S.S.; Sooryanarayana, R.; Ahmad, N.A.; Jamaluddin, R.; Abd Razak, M.A.; Tan, M.P.; Mohd Sidik, S.; Mohamad Zahir, S.; Sandanasamy, K.S.; Ibrahim, N. Prevalence of dementia and quality of life of caregivers of people living with dementia in Malaysia. Geriatr. Gerontol. Int. 2020, 20, 16–20. [Google Scholar] [CrossRef]
- Kaczynski, A.; Michalowsky, B.; Eichler, T.; Thyrian, J.R.; Wucherer, D.; Zwingmann, I.; Hoffmann, W. Comorbidity in Dementia Diseases and Associated Health Care Resources Utilization and Cost. J. Alzheimers Dis. 2019, 68, 635–646. [Google Scholar] [CrossRef]
- Kitching, D. Depression in dementia. Aust. Prescr. 2015, 38, 209–2011. [Google Scholar] [CrossRef]
- Alzheimer’s Association. 2018 Alzheimer’s disease facts and figures. Alzheimer’s Dement. 2018, 14, 367–429. [Google Scholar] [CrossRef]
- Asadzadeh, A.; Kalankesh, L.R. A scope of mobile health solutions in COVID-19 pandemics. Inf. Med. Unlocked 2021, 23, 100558. [Google Scholar] [CrossRef]
- Aungst, T.D. Medical applications for pharmacists using mobile devices. Ann. Pharmacother. 2013, 47, 1088–1095. [Google Scholar] [CrossRef]
- Bier, N.; Brambati, S.; Macoir, J.; Paquette, G.; Schmitz, X.; Belleville, S.; Faucher, C.; Joubert, S. Relying on procedural memory to enhance independence in daily living activities: Smartphone use in a case of semantic dementia. Neuropsychol. Rehabil. 2015, 25, 913–935. [Google Scholar] [CrossRef] [PubMed]
- Leng, F.Y.; Yeo, D.; George, S.; Barr, C. Comparison of iPad applications with traditional activities using person-centred care approach: Impact on well-being for persons with dementia. Dementia 2013, 13, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Lanza, C.; Knörzer, O.; Weber, M.; Riepe, M.W. Autonomous Spatial Orientation in Patients with Mild to Moderate Alzheimer’s Disease by using Mobile Assistive Devices: A Pilot Study. J. Alzheimer’s Dis. 2014, 42, 879–884. [Google Scholar] [CrossRef] [PubMed]
- Klapper, L.; Mobile Phones are Key to Economic Development. Are Women Missing Out? Available online: https://www.brookings.edu/blog/future-development/2019/04/10/mobile-phones-are-key-to-economic-development-are-women-missing-out/ (accessed on 1 January 2022).
- Müller, J. Share of Individuals Owning a Mobile Phone in Malaysia in 2020, by State. Available online: https://www.statista.com/statistics/873913/share-of-individuals-owning-a-mobile-phone-in-malaysia/ (accessed on 31 March 2022).
- Müller, J. Smartphone Market in Malaysia—Statistics and Facts. Available online: https://www.statista.com/topics/6615/smartphones-in-malaysia/#topicHeader__wrapper (accessed on 31 March 2022).
- Brown, E.L.; Ruggiano, N.; Li, J.; Clarke, P.J.; Kay, E.S.; Hristidis, V. Smartphone-Based Health Technologies for Dementia Care: Opportunities, Challenges, and Current Practices. J. Appl. Gerontol. 2017, 38, 73–91. [Google Scholar] [CrossRef]
- Taha, A.R.; Shehadeh, M.; Alshehhi, A.; Altamimi, T.; Housser, E.; Simsekler, M.C.E.; Alfalasi, B.; Al Memari, S.; Al Hosani, F.; Al Zaabi, Y.; et al. The integration of mHealth technologies in telemedicine during the COVID-19 era: A cross-sectional study. PLoS ONE 2022, 17, e0264436. [Google Scholar] [CrossRef]
- Abbaspur-Behbahani, S.; Monaghesh, E.; Hajizadeh, A.; Fehresti, S. Application of mobile health to support the elderly during the COVID-19 outbreak: A systematic review. Health Policy Technol. 2022, 11, 100595. [Google Scholar] [CrossRef]
- Riva, G.; Mantovani, F.; Wiederhold, B.K. Positive Technology and COVID-19. Cyberpsychol. Behav. Soc. Netw. 2020, 23, 581–587. [Google Scholar] [CrossRef]
- Iyengar, K.; Upadhyaya, G.K.; Vaishya, R.; Jain, V. COVID-19 and applications of smartphone technology in the current pandemic. Diabetes Metab. Syndr. 2020, 14, 733–737. [Google Scholar] [CrossRef]
- Yaacob, N.A.; Mohamad Marzuki, M.F.; Yaacob, N.M.; Ahmad, S.B.; Abu Hassan, M.R. Effectiveness of the ColorApp Mobile App for Health Education and Promotion for Colorectal Cancer: Quasi-Experimental Study. JMIR Hum. Factors 2020, 7, e15487. [Google Scholar] [CrossRef]
- Han, M.; Lee, E. Effectiveness of Mobile Health Application Use to Improve Health Behavior Changes: A Systematic Review of Randomized Controlled Trials. Healthc. Inform. Res. 2018, 24, 207. [Google Scholar] [CrossRef]
- Wang, K.; Varma, D.S.; Prosperi, M. A systematic review of the effectiveness of mobile apps for monitoring and management of mental health symptoms or disorders. J. Psychiatr. Res. 2018, 107, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Lee, H.; Kim, Y.; Kim, J.; Cho, M.; Jang, J.; Jang, H. Mobile App-Based Health Promotion Programs: A Systematic Review of the Literature. Int. J. Environ. Res. Public Health 2018, 15, 2838. [Google Scholar] [CrossRef] [PubMed]
- Davis, B.; Nies, M.; Shehab, M.; Shenk, D. Developing a pilot e-mobile app for dementia caregiver support: Lessons learned | OJNI. Online J. Nurs. Inform. 2014, 18, 13. [Google Scholar]
- Désormeaux-Moreau, M.; Michel, C.-M.; Vallières, M.; Racine, M.; Poulin-Paquet, M.; Lacasse, D.; Gionet, P.; Genereux, M.; Lachiheb, W.; Provencher, V. Mobile Apps to Support Family Caregivers of People with Alzheimer Disease and Related Dementias in Managing Disruptive Behaviors: Qualitative Study With Users Embedded in a Scoping Review. JMIR Aging 2021, 4, e21808. [Google Scholar] [CrossRef]
- Brown, E.L.; Ruggiano, N.; Page, T.F.; Roberts, L.; Hristidis, V.; Whiteman, K.L.; Castro, J. CareHeroes Web and Android™ Apps for Dementia Caregivers: A Feasibility Study. Res. Gerontol. Nurs. 2016, 9, 193–203. [Google Scholar] [CrossRef]
- Ye, B.; How, T.V.; Chu, C.H.; Mihailidis, A. Dementia Care Apps for People with Dementia and Informal Caregivers: A Systematic Review Protocol. Gerontology 2021, 67, 633–638. [Google Scholar] [CrossRef]
- CogniCare CogniCare—Support for Dementia Care App. Available online: https://www.healthnavigator.org.nz/apps/c/cognicare-support-for-dementia-care-app/#:~:text=CogniCare%20app%20aims%20to%20support,details%20of%20incidents%20and%20activities (accessed on 1 April 2022).
- House of Memories My House of Memories App. Available online: https://www.liverpoolmuseums.org.uk/house-of-memories/my-house-of-memories-app (accessed on 1 April 2022).
- Accessible Alzheimer Dementia Care Alzheimer’s & Dementia Care App. Available online: https://www.accessiblehomehealthcare.com/alzheimers-dementia-care-app (accessed on 1 April 2022).
- Joygage Joygage: Engage, Enjoy, and Enliven Your Memory! Available online: https://www.joygage.com/ (accessed on 1 April 2022).
- Sala-González, M.; Pérez-Jover, V.; Guilabert, M.; Mira, J.J. Mobile Apps for Helping Informal Caregivers: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 1702. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Gaining Consensus Among Stakeholders Through the Nominal Group Technique; CDC, Ed.; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2018.
- Mason, S.; Ling, J.; Mosoiu, D.; Arantzamendi, M.; Tserkezoglou, A.J.; Predoiu, O.; Payne, S. Undertaking Research Using Online Nominal Group Technique: Lessons from an International Study (RESPACC). J. Palliat. Med. 2021, 24, 1867–1871. [Google Scholar] [CrossRef]
- McMillan, S.S.; King, M.; Tully, M.P. How to use the nominal group and Delphi techniques. Int. J. Clin. Pharm. 2016, 38, 655–662. [Google Scholar] [CrossRef]
- McMillan, S.S.; Kelly, F.; Sav, A.; Kendall, E.; King, M.A.; Whitty, J.A.; Wheeler, A.J. Using the Nominal Group Technique: How to analyse across multiple groups. Health Serv. Outcomes Res. Methodol. 2014, 14, 92–108. [Google Scholar] [CrossRef]
- American Psychological Association How Caregiving is Defined. Available online: https://www.apa.org/pi/about/publications/caregivers/research/methods/definition (accessed on 26 January 2022).
- Kent, E.E.; Rowland, J.H.; Northouse, L.; Litzelman, K.; Chou, W.Y.; Shelburne, N.; Timura, C.; O’Mara, A.; Huss, K. Caring for caregivers and patients: Research and clinical priorities for informal cancer caregiving. Cancer 2016, 122, 1987–1995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naik, S. Nominal Group Technique Definition, Examples Steps. Available online: https://www.lsssimplified.com/nominal-group-technique-definition-step-example-ngt/ (accessed on 3 March 2022).
- Centers for Disease Control and Prevention. Data Collection Methods for Program Evaluation: Focus Groups. Available online: https://www.cdc.gov/healthyyouth/evaluation/pdf/brief13.pdf (accessed on 26 January 2022).
- Mahmud, D.; Abdullah, N.A.S. Mobile application development feasibility studies: A case study in Universiti Teknologi MARA. In Proceedings of the ICOS 2014—2014 IEEE Conference on Open Systems, Subang, Malaysia, 26–28 October 2014; pp. 30–35. [Google Scholar]
- Statista Mobile Operating Systems’ Market Share Worldwide from January 2012 to January 2022. Available online: https://www.statista.com/statistics/272698/global-market-share-held-by-mobile-operating-systems-since-2009/ (accessed on 26 March 2022).
- Zhulidin, A. Guide for Designing Better Mobile Apps Typography. Available online: https://uxdesign.cc/guide-for-designing-better-mobile-apps-typography-5796495ef86f (accessed on 26 March 2022).
- Shaoolian, G. 5 Mobile App Features Your Customers Want. Available online: https://www.forbes.com/sites/gabrielshaoolian/2017/06/07/5-mobile-app-features-your-customers-want/?sh=60608e2647bf (accessed on 26 April 2022).
- Neptune Alpha, Beta, and Launch: App Stages Explained. Available online: http://watchneptune.com/parentingtech/alpha-beta-and-launch-app-stages-explained/ (accessed on 20 July 2022).
- Heynsbergh, N.; Heckel, L.; Botti, M.; O, S.C.; Livingston, P.M. Development of a Smartphone App for Informal Carers of People with Cancer: Processes and Learnings. JMIR Res. 2019, 3, e10990. [Google Scholar] [CrossRef] [PubMed]
- Memon, M.; Ting, H.; Hwa, C.; Ramayah, T.; Chuah, F.; Cham, T.H. Sample Size for Survey Research: Review and Recommendations. J. Appl. Struct. Equ. Model. 2020, 4, 1–20. [Google Scholar] [CrossRef]
- Mohamad Marzuki, M.F.; Yaacob, N.A.; bin Yaacob, N.M.; Abu Hassan, M.R.; Ahmad, S.B. Usable Mobile App for Community Education on Colorectal Cancer: Development Process and Usability Study. JMIR Hum. Factors 2019, 6, e12103. [Google Scholar] [CrossRef]
- Kazi, A.M.; Ahsan, N.; Mughis, W.; Jamal, S.; Allana, R.; Raza, M.; Muneer, S.; Mughal, M.A.K.; Kaleemuddin, H.; Sameen, F.; et al. Usability and Acceptability of a Mobile App for Behavior Change and to Improve Immunization Coverage among Children in Pakistan: A Mixed-Methods Study. Int. J. Environ. Res. Public Health 2021, 18, 9527. [Google Scholar] [CrossRef]
- Swaid, S. Usability of Mobile Apps: An Integrated Approach. Int. J. Comput. Sci. 2017, 11–16. [Google Scholar]
- Davis, F.D. Perceived Usefulness, Perceived Ease of Use, and User Acceptance of Information Technology. MIS Q. 1989, 13, 319–340. [Google Scholar] [CrossRef]
- Li, X.; Zhao, X.; Xu, W.; Pu, W. Measuring ease of use of mobile applications in e-commerce retailing from the perspective of consumer online shopping behaviour patterns. J. Retail. Consum. Serv. 2020, 55, 102093. [Google Scholar] [CrossRef]
- Zamzami, I.; Mahmud, M. User Satisfaction on Smart Phone Interface Design, Information Quality Evaluation. In Proceedings of the 2012 International Conference on Advanced Computer Science Applications and Technologies (ACSAT), Kuala Lumpur, Malaysia, 26–28 November 2012; pp. 78–82. [Google Scholar]
- Usefulness. Merriam-Webster.com Dictionary, Merriam-Webster. 2022. Available online: https://www.merriam-webster.com/dictionary/usefulness (accessed on 25 April 2022).
- Mustafa, N.; Safii, N.S.; Jaffar, A.; Sani, N.S.; Mohamad, M.I.; Abd Rahman, A.H.; Mohd Sidik, S. Malay Version of the mHealth App Usability Questionnaire (M-MAUQ): Translation, Adaptation, and Validation Study. JMIR Mhealth Uhealth 2021, 9, e24457. [Google Scholar] [CrossRef]
- Zhou, L.; Bao, J.; Setiawan, I.M.A.; Saptono, A.; Parmanto, B. The mHealth App Usability Questionnaire (MAUQ): Development and Validation Study. JMIR Mhealth Uhealth 2019, 7, e11500. [Google Scholar] [CrossRef]
- Knight, G. Data Management for Interview and Focus Group Resources in Health; London School of Hygiene & Tropical Medicine: London, UK, 2018. [Google Scholar]
- Deakin University What Data Do I Need to Keep and for How Long? Available online: https://www.deakin.edu.au/library/research/manage-data/store/what-data-do-i-need-to-keep-and-for-how-long (accessed on 1 April 2022).
- National Institutes of Health. Guidelines for Conducting Research in Ministry of Health (MOH) Institutes & Facilities, 3rd ed.; Ministry of Health Malaysia: Putrajaya, Malaysia, 2021.
- Wolff, B.; Mahoney, F.; Lohiniva, A.L.; Corkum, M. Collecting and analyzing qualitative data. In The CDC Field Epidemiology Manual; Oxford University Press: Oxford, UK; New York, NY, USA, 2019; pp. 213–228. [Google Scholar]
- Golinelli, D.; Boetto, E.; Carullo, G.; Nuzzolese, A.G.; Landini, M.P.; Fantini, M.P. Adoption of Digital Technologies in Health Care During the COVID-19 Pandemic: Systematic Review of Early Scientific Literature. J. Med. Internet Res. 2020, 22, e22280. [Google Scholar] [CrossRef] [PubMed]
- Cuffaro, L.; Di Lorenzo, F.; Bonavita, S.; Tedeschi, G.; Leocani, L.; Lavorgna, L. Dementia care and COVID-19 pandemic: A necessary digital revolution. Neurol. Sci. Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol. 2020, 41, 1977–1979. [Google Scholar] [CrossRef] [PubMed]
- Pawi; Putit, Z.; Buncuan, J. Challenges in conducting focus group: Moderators’ experiences in Nursing. J. Malays. Nurses Assoc. 2010, 5, 2–9. [Google Scholar]
- Srivastava, S. Effective Ways to Choose the Best Mobile App Developer. Available online: https://appinventiv.com/blog/effective-ways-choose-best-mobile-app-developer/ (accessed on 27 March 2022).
- Iubenda Laws and Regulations Every App Developer Should Know—And How to Comply. Available online: https://www.iubenda.com/en/help/14787-laws-regulations-every-app-developer-should-know (accessed on 27 March 2022).
- Thomson Reuters Mobile App Development: Key Legal Considerations. Available online: https://uk.practicallaw.thomsonreuters.com/7-525-8637?transitionType=Default&contextData=(sc.Default)&firstPage=true (accessed on 27 March 2022).

{kind=link}
| Solution/Ideas | Participant 1 | Participant 2 | Participant 3 | Participant 4 | Participant 5 | NGT Scores |
|---|---|---|---|---|---|---|
| Solution/Idea 1 | 4 | 4 | 5 | 4 | 5 | 22 |
| Solution/Idea 2 | 2 | 1 | 3 | 2 | 2 | 10 |
| Solution/Idea 3 | 5 | 5 | 5 | 4 | 4 | 23 |
| Solution/Idea 4 | 3 | 1 | 5 | 2 | 4 | 15 |
| Solution/Idea 5 | 4 | 4 | 5 | 4 | 3 | 20 |
| Criteria | Eligibility |
|---|---|
| Inclusion |
|
| Exclusion |
|
| Variable/Domain | Operational Definition |
|---|---|
| Usability of mobile app | Usability is determined by the total and mean scores of all domains (ease of use, interface, and usefulness) derived from the M-MAUQ. Higher scores indicate greater usability. A total mean score equal to, or more than, 72 denotes that the app has good usability and vice versa. |
| (a) Ease of use | There are 5 items under this domain. A total mean score equal to, or more than, 20 under indicates that the app is easy to use, and vice versa. |
| (b) Interface and satisfaction | There are 7 items under this domain. A total mean score equal to, or more than, 28 indicates that the app has a good interface and is satisfactory, and vice versa. |
| (c) Usefulness | There are 6 items under this domain. A total mean score equal to, or more than, 24 indicates that the app is useful and serves its purpose and vice versa. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rashid, N.S.A.; Chen, X.W.; Mohamad Marzuki, M.F.; Takshe, A.A.; Okasha, A.; Maarof, F.; Yunus, R.M. Development and Usability Assessment of a Mobile App (Demensia KITA) to Support Dementia Caregivers in Malaysia: A Study Protocol. Int. J. Environ. Res. Public Health 2022, 19, 11880. https://doi.org/10.3390/ijerph191911880
Rashid NSA, Chen XW, Mohamad Marzuki MF, Takshe AA, Okasha A, Maarof F, Yunus RM. Development and Usability Assessment of a Mobile App (Demensia KITA) to Support Dementia Caregivers in Malaysia: A Study Protocol. International Journal of Environmental Research and Public Health. 2022; 19(19):11880. https://doi.org/10.3390/ijerph191911880
Chicago/Turabian StyleRashid, Nurul Syaireen A., Xin Wee Chen, Muhamad Fadhil Mohamad Marzuki, Aseel A. Takshe, Ahmad Okasha, Faridah Maarof, and Raudah Mohd Yunus. 2022. "Development and Usability Assessment of a Mobile App (Demensia KITA) to Support Dementia Caregivers in Malaysia: A Study Protocol" International Journal of Environmental Research and Public Health 19, no. 19: 11880. https://doi.org/10.3390/ijerph191911880
APA StyleRashid, N. S. A., Chen, X. W., Mohamad Marzuki, M. F., Takshe, A. A., Okasha, A., Maarof, F., & Yunus, R. M. (2022). Development and Usability Assessment of a Mobile App (Demensia KITA) to Support Dementia Caregivers in Malaysia: A Study Protocol. International Journal of Environmental Research and Public Health, 19(19), 11880. https://doi.org/10.3390/ijerph191911880