
Combined Endoscopic Endonasal Transclival and Contralateral Transmaxillary Approach to the Petrous Apex and the Petroclival Synchondrosis: Working “Around the Corner” of the Internal Carotid Artery—Quantitative Anatomical Study and Clinical Applications
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Anatomical Study
2.2. Surgical Technique
- (1)
- The nasal step
- (2)
- The clival step
- (3)
- The maxillary step
- (4)
- The petrosal step
2.3. Quantitative Analysis and Surgical Operability
2.4. Statistical Analysis
2.5. Surgical Series
3. Results
3.1. Anthropometric Measurements and Surgical Operability
3.2. Surgical Series
- Case 1
- Case 2
- Case 3
4. Discussion
4.1. Surgical Anatomy Considerations
4.2. Advantages and Drawbacks of the Combined EETC and CTM Approach
4.3. Surgical Considerations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kassam, A.B.; Gardner, P.; Snyderman, C.; Mintz, A.; Carrau, R. Expanded endonasal approach: Fully endoscopic, completely transnasal approach to the middle third of the clivus, petrous bone, middle cranial fossa, and infratemporal fossa. Neurosurg. Focus 2005, 19, E6. [Google Scholar] [CrossRef] [PubMed]
- Fortes, F.S.G.; Pinheiro-Neto, C.D.; Carrau, R.L.; Brito, R.V.; Prevedello, D.M.; Sennes, L.U. Endonasal endoscopic exposure of the internal carotid artery: An anatomical study. Laryngoscope 2012, 122, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Gardner, P.A.; Tormenti, M.J.; Pant, H.; Fernandez-Miranda, J.C.; Snyderman, C.H.; Horowitz, M.B. Carotid artery injury during endoscopic endonasal skull base surgery: Incidence and outcomes. Neurosurgery 2013, 73, ons261–ons269, discussion ons269–ons270. [Google Scholar] [CrossRef] [PubMed]
- Zanation, A.M.; Snyderman, C.H.; Carrau, R.L.; Gardner, P.A.; Prevedello, D.M.; Kassam, A.B. Endoscopic endonasal surgery for petrous apex lesions. Laryngoscope 2008, 119, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Zimmer, L.A.; Hart, C.; Theodosopoulos, P.V. Endoscopic Anatomy of the Petrous Segment of the Internal Carotid Artery. Am. J. Rhinol. Allergy 2009, 23, 192–196. [Google Scholar] [CrossRef] [PubMed]
- Freeman, J.L.; Sampath, R.; Casey, M.A.; Quattlebaum, S.C.; Ramakrishnan, V.R.; Youssef, A.S. Transposition of the paraclival carotid artery: A novel concept of self-retaining vascular retraction during endoscopic endonasal skull base surgery technical report. Acta Neurochir. 2016, 158, 1625–1629. [Google Scholar] [CrossRef] [PubMed]
- Patel, C.R.; Wang, E.W.; Fernandez-Miranda, J.C.; Gardner, P.A.; Snyderman, C.H. Contralateral transmaxillary corridor: An augmented endoscopic approach to the petrous apex. J. Neurosurg. 2018, 129, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Mangussi-Gomes, J.; Alves-Belo, J.T.; Truong, H.Q.; Nogueira, G.F.; Wang, E.W.; Fernandez-Miranda, J.C.; Gardner, P.A.; Snyderman, C.H. Anatomical Limits of the Endoscopic Contralateral Transmaxillary Approach to the Petrous Apex and Petroclival Region. J. Neurol. Surg. B Skull Base 2022, 83, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Pamias-Portalatin, E.; Mahato, D.; Rincon-Torroella, J.; Vivas-Buitrago, T.; Quiñones-Hinojosa, A.; Boahene, K.O. Endoscope-assisted contralateral transmaxillary approach to the clivus and the hypoglossal canal: Technical case report. J. Neurosurg. 2019, 130, 1609–1615. [Google Scholar] [CrossRef] [PubMed]
- Snyderman, C.H.; Gardner, P.A.; Wang, E.W.; Fernandez-Miranda, J.C.; Valappil, B. Experience with the Endoscopic Contralateral Transmaxillary Approach to the Petroclival Skull Base. Laryngoscope 2020, 131, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Corvino, S.; Guizzardi, G.; Sacco, M.; Corrivetti, F.; Bove, I.; Enseñat, J.; Colamaria, A.; Prats-Galino, A.; Solari, D.; Cavallo, L.M.; et al. The feasibility of three port endonasal, transorbital, and sublabial approach to the petroclival region: Neurosurgical audit and multiportal anatomic quantitative investigation. Acta Neurochir. 2023, 165, 1821–1831. [Google Scholar] [CrossRef] [PubMed]
- Yanez-Siller, J.C.; Noiphithak, R.; Porto, E.; Beer-Furlan, A.L.; Barbero, J.M.R.; Martinez-Perez, R.; Howe, E.; Prevedello, D.M.; Carrau, R.L. Endoscopic Approaches to the Paramedian Skull Base: An Anatomic Comparison of Contralateral Endonasal and Transmaxillary Strategies. Oper. Neurosurg. 2023, 24, e421–e428. [Google Scholar] [CrossRef] [PubMed]
- Peris-Celda, M.; Kucukyuruk, B.; Monroy-Sosa, A.; Funaki, T.; Valentine, R.; Rhoton Jr, A.L. The recesses of the sellar wall of the sphenoid sinus and their intracranial relationships. Oper. Neurosurg. 2013, 73, ons117–ons131, discussion ons131. [Google Scholar] [CrossRef] [PubMed]
- Iwanaga, J.; Boggio, N.A.; Bui, C.J.; Dumont, A.S.; Tubbs, R.S. Can anatomical feasibility studies drive neurosurgical procedures and reach patients faster than traditional translational research? Neurosurg. Rev. 2022, 45, 891–896. [Google Scholar] [CrossRef] [PubMed]
- Labib, M.A.; Prevedello, D.M.; Carrau, R.; Kerr, E.E.; Naudy, C.; Al-Shaar, H.A.; Corsten, M.; Kassam, A. A road map to the internal carotid artery in expanded endoscopic endonasal approaches to the ventral cranial base. Neurosurgery 2014, 10, 448–471, discussion 471. [Google Scholar] [CrossRef] [PubMed]
- Gagliardi, F.; Donofrio, C.A.; Spina, A.; Bailo, M.; Gragnaniello, C.; Gallotti, A.L.; Elbabaa, S.K.; Caputy, A.J.; Mortini, P. Endoscope-Assisted Transmaxillosphenoidal Approach to the Sellar and Parasellar Regions: An Anatomic Study. World Neurosurg. 2016, 95, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Donofrio, C.A.; Riccio, L.; Pathmanaban, O.N.; Fioravanti, A.; Caputy, A.J.; Mortini, P. Endoscopic sublabial transmaxillary approach to the inferior orbit: Pearls and pitfalls-A comparative anatomical study. Neurosurg. Rev. 2021, 44, 3297–3307. [Google Scholar] [CrossRef] [PubMed]
- Simal-Julián, J.A.; Miranda-Lloret, P.; Botella-Asunción, C.; Kassam, A. Full endoscopic endonasal expanded approach to the petroclival region: Optimizing the carotid-clival window. Acta Neurochir. 2014, 156, 1627–1629. [Google Scholar] [CrossRef] [PubMed]
- Donofrio, C.A.; Capitanio, J.F.; Riccio, L.; Herur-Raman, A.; Caputy, A.J.; Mortini, P. Mini Fronto-Orbital Approach: “Window Opening” Towards the Superomedial Orbit—A Virtual Reality-Planned Anatomic Study. Oper. Neurosurg. 2020, 19, 330–340. [Google Scholar] [CrossRef] [PubMed]
- Donofrio, C.A.; Riccio, L.; Capitanio, J.F.; Herur-Raman, A.; Panni, P.; Gagliardi, F.; Caputy, A.J.; Mortini, P. Transcortical endoportal subchoroidal endoscope-assisted approach to the third ventricle: From virtual reality to anatomical laboratory. J. Neurosurg. Sci. 2023, 67, 175–184. [Google Scholar] [CrossRef] [PubMed]
- de Notaris, M.; Sacco, M.; Corrivetti, F.; Dallan, I.; Cavallo, L.M.; Somma, T.; Parbonetti, G.; Colamaria, A.; Solari, D. Indocyanine Green Endoscopy for Pituitary Adenomas with Parasellar Extension: Results from a Preliminary Case Series. World Neurosurg. 2022, 166, e692–e702. [Google Scholar] [CrossRef] [PubMed]
- Kassam, A.B.; Vescan, A.D.; Carrau, R.L.; Prevedello, D.M.; Gardner, P.; Mintz, A.H.; Snyderman, C.H.; Rhoton, A.L. Expanded endonasal approach: Vidian canal as a landmark to the petrous internal carotid artery. J. Neurosurg. 2008, 108, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Oakley, G.M.; Ebenezer, J.; Hamizan, A.; Sacks, P.-L.; Rom, D.; Sacks, R.; Winder, M.; Davidson, A.; Teo, C.; Solares, C.A.; et al. Finding the Petroclival Carotid Artery: The Vidian-Eustachian Junction as a Reliable Landmark. J. Neurol. Surg. B Skull Base 2018, 79, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Falcon, R.T.; Rivera-Serrano, C.M.; Miranda, J.F.; Prevedello, D.M.; Snyderman, C.H.; Kassam, A.B.; Carrau, R.L. Endoscopic endonasal dissection of the infratemporal fossa: Anatomic relationships and importance of eustachian tube in the endoscopic skull base surgery. Laryngoscope 2011, 121, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Alikhani, P.; van Loveren, H.; Agazzi, S.; Sivakanthan, S. Paraclival or Cavernous Internal Carotid Artery: One Segment but Two Names. J. Neurol. Surg. B Skull Base 2016, 77, 304–307. [Google Scholar] [CrossRef] [PubMed]
- Borghei-Razavi, H.; Truong, H.Q.; Cabral, D.T.F.; Sun, X.; Celtikci, E.; Wang, E.; Snyderman, C.; Gardner, P.A.; Fernandez-Miranda, J.C. Endoscopic Endonasal Petrosectomy: Anatomical Investigation, Limitations, and Surgical Relevance. Oper. Neurosurg. 2019, 16, 557–570. [Google Scholar] [CrossRef] [PubMed]
- Fournier, H.D.; Mercier, P.; Roche, P.H. Surgical anatomy of the petrous apex and petroclival region. Adv. Tech. Stand. Neurosurg. 2007, 32, 91–146. [Google Scholar] [PubMed]
- Donofrio, C.A.; Badaloni, F.; Riccio, L.; Morandini, A.; Bertuccio, A.; Generali, D.; Calbucci, F.; Servadei, F.; Fioravanti, A. Posterior Petrous Meningiomas: Surgical Classification and Postoperative Outcomes in a Case Series of 130 Patients Operated via the Retrosigmoid Approach. World Neurosurg. 2023, 171, e301–e308. [Google Scholar] [CrossRef] [PubMed]
- Khonsary, S.; Ma, Q.; Villablanca, P.; Emerson, J.; Malkasian, D. Clinical functional anatomy of the pterygopalatine ganglion, cephalgia and related dysautonomias: A review. Surg. Neurol. Int. 2013, 4 (Suppl. S6), S422–S428. [Google Scholar] [CrossRef] [PubMed]
- Nturibi, E.; Bordoni, B. Anatomy, Head and Neck: Greater Petrosal Nerve. In StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2023. [Google Scholar]
- Iaconetta, G.; Fusco, M.; Cavallo, L.M.; Cappabianca, P.; Samii, M.; Tschabitscher, M. The abducens nerve: Microanatomic and endoscopic study. Neurosurgery 2007, 61, 7–14, discussion 14. [Google Scholar] [CrossRef] [PubMed]
- Little, A.S.; Nakaji, P.; Milligan, J. Endoscopic endonasal transmaxillary approach and endoscopic sublabial transmaxillary approach: Surgical decision-making and implications of the nasolacrimal duct. World Neurosurg. 2013, 80, 583–590. [Google Scholar] [CrossRef] [PubMed]
- Wilson, D.A.; Williamson, R.W.; Preul, M.C.; Little, A.S. Comparative analysis of surgical freedom and angle of attack of two minimal-access endoscopic transmaxillary approaches to the anterolateral skull base. World Neurosurg. 2014, 82, e487–e493. [Google Scholar] [CrossRef] [PubMed]
- Schilder, A.G.; Bhutta, M.F.; Butler, C.C.; Holy, C.; Levine, L.; Kvaerner, K.; Norman, G.; Pennings, R.; Poe, D.; Silvola, J.; et al. Eustachian tube dysfunction: Consensus statement on definition, types, clinical presentation and diagnosis. Clin. Otolaryngol. 2015, 40, 407–411. [Google Scholar] [CrossRef] [PubMed]
- Komotar, R.J.; Starke, R.M.; Raper, D.M.; Anand, V.K.; Schwartz, T.H. The endoscope-assisted ventral approach compared with open microscope-assisted surgery for clival chordomas. World Neurosurg. 2011, 76, 318–327, discussion 259–362. [Google Scholar] [CrossRef] [PubMed]
- Komotar, R.J.; Starke, R.M.; Raper, D.M.; Anand, V.K.; Schwartz, T.H. Endoscopic endonasal compared with microscopic transsphenoidal and open transcranial resection of giant pituitary adenomas. Pituitary 2012, 15, 150–159. [Google Scholar] [CrossRef] [PubMed]
- Rahimli, T.; Hidayetov, T.; Yusifli, Z.; Memmedzade, H.; Rajabov, T.; Aghayev, K. Endoscopic Endonasal Approach to Giant Pituitary Adenomas: Surgical Outcomes and Review of the Literature. World Neurosurg. 2021, 149, e1043–e1055. [Google Scholar] [CrossRef] [PubMed]
- Mirza, A.B.; Ravindran, V.; Okasha, M.; Boardman, T.M.; Maratos, E.; Sinan, B.; Thomas, N. Systematic Review Comparing Open versus Endoscopic Surgery in Clival Chordomas and a 10-Year Single-Center Experience. J. Neurol.Surg. B Skull Base 2022, 83 (Suppl. S2), e113–e125. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.K.; Zhao, K.; Vazquez, A.; Eloy, J.A. Combined endoscopic endonasal and sublabial transmaxillary approach for resection of giant infratemporal fossa schwannoma with intracranial extension: Operative video and technical nuances. Neurosurg. Focus Video 2020, 2, V16. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
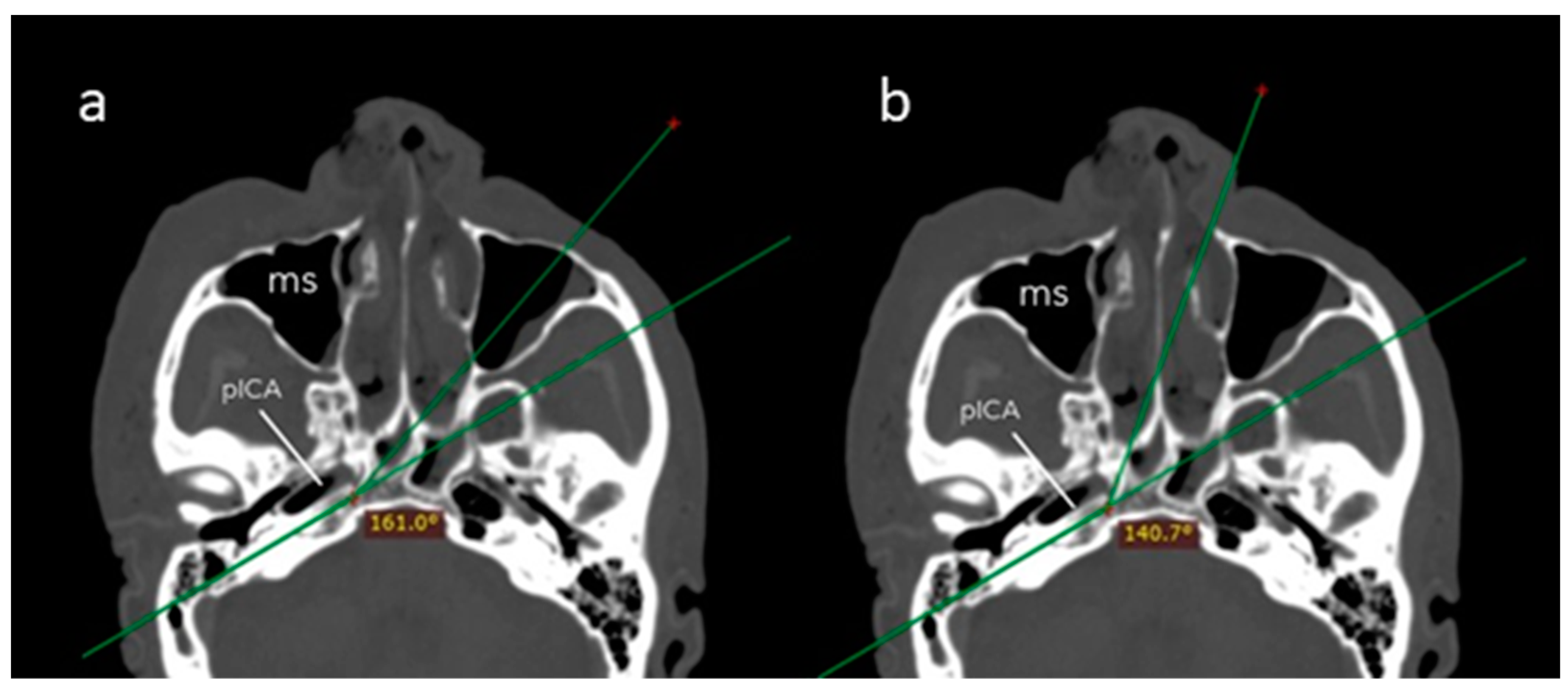
| Transmaxillary Corridor (Mean ± SD) | Endonasal Corridor (Mean ± SD) | p Value | |
|---|---|---|---|
| Angle of attack (°) | 161.1 (8.6) | 140.6 (5.7) | 0.001 |
| Surgical field depth (mm) | 74.3 (4.0) | 88.0 (5.8) | 0.001 |
| Petrous drilling depth (mm) | 17.2 (4.0) | 11.0 (3.3) | 0.008 |
| Surgical Exposure | Surgical Maneuverability | |||
|---|---|---|---|---|
| 0° Optics | 30° Optics | Straight Instruments | Angled Instruments | |
| Transmaxillary corridor | 2 | 2 | 2 | 2 |
| Endonasal corridor | 1 | 2 | 1 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Donofrio, C.A.; Corrivetti, F.; Riccio, L.; Corvino, S.; Dallan, I.; Fioravanti, A.; de Notaris, M. Combined Endoscopic Endonasal Transclival and Contralateral Transmaxillary Approach to the Petrous Apex and the Petroclival Synchondrosis: Working “Around the Corner” of the Internal Carotid Artery—Quantitative Anatomical Study and Clinical Applications. J. Clin. Med. 2024, 13, 2713. https://doi.org/10.3390/jcm13092713
Donofrio CA, Corrivetti F, Riccio L, Corvino S, Dallan I, Fioravanti A, de Notaris M. Combined Endoscopic Endonasal Transclival and Contralateral Transmaxillary Approach to the Petrous Apex and the Petroclival Synchondrosis: Working “Around the Corner” of the Internal Carotid Artery—Quantitative Anatomical Study and Clinical Applications. Journal of Clinical Medicine. 2024; 13(9):2713. https://doi.org/10.3390/jcm13092713
Chicago/Turabian StyleDonofrio, Carmine Antonio, Francesco Corrivetti, Lucia Riccio, Sergio Corvino, Iacopo Dallan, Antonio Fioravanti, and Matteo de Notaris. 2024. "Combined Endoscopic Endonasal Transclival and Contralateral Transmaxillary Approach to the Petrous Apex and the Petroclival Synchondrosis: Working “Around the Corner” of the Internal Carotid Artery—Quantitative Anatomical Study and Clinical Applications" Journal of Clinical Medicine 13, no. 9: 2713. https://doi.org/10.3390/jcm13092713