One-Seventh of Patients with COVID-19 Had Olfactory and Gustatory Abnormalities as Their Initial Symptoms: A Systematic Review and Meta-Analysis

 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Literature Search
2.2. Study Selection and Data Extraction
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- WHO. Coronavirus Disease (Covid-19) Outbreak Situation. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 1 July 2020).
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (covid-19): A review. JAMA 2020. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.-M.; Tan, T.-W.; Ho, T.-C.; Chen, C.-C.; Su, T.-H.; Lin, C.-Y. Covid-19: Taiwan’s epidemiological characteristics and public and hospital responses. PeerJ 2020, 8, e9360. [Google Scholar] [CrossRef] [PubMed]
- Chiu, N.-C.; Chi, H.; Tai, Y.-L.; Peng, C.-C.; Tseng, C.-Y.; Chen, C.-C.; Tan, B.F.; Lin, C.Y. Impact of wearing masks, hand hygiene, and social distancing on influenza, enterovirus, and all-cause pneumonia during the coronavirus pandemic: Retrospective national epidemiological surveillance study. J. Med. Internet. Res. 2020, 22, e21257. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (covid-19) outbreak in china: Summary of a report of 72314 cases from the Chinese center for disease control and prevention. JAMA 2020. [Google Scholar] [CrossRef]
- Lee, P.I.; Hsueh, P.R. Emerging threats from zoonotic coronaviruses-from sars and mers to 2019-ncov. J. Microbiol. Immunol. Infect. 2020, 53, 365–367. [Google Scholar] [CrossRef]
- Luers, J.C.; Rokohl, A.C.; Loreck, N.; Wawer Matos, P.A.; Augustin, M.; Dewald, F.; Klein, F.; Lehmann, C.; Heindl, L.M. Olfactory and gustatory dysfunction in coronavirus disease 19 (covid-19). Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Mao, L.; Jin, H.; Wang, M.; Hu, Y.; Chen, S.; He, Q.; Chang, J.; Hong, C.; Zhou, Y.; Wang, D.; et al. Neurologic manifestations of hospitalized patients with coronavirus disease 2019 in wuhan, china. JAMA Neurol. 2020, 77, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (prisma-p) 2015: Elaboration and explanation. BMJ 2015, 350, g7647. [Google Scholar] [CrossRef] [Green Version]
- Chi, H.; Chiu, N.-C.; Tai, Y.-L.; Chang, H.-Y.; Lin, C.-H.; Sung, Y.-H.; Tseng, C.-Y.T.; Liu, L.Y.-M.; Lin, C.-Y. Clinical features of neonates born to mothers with coronavirus disease-2019: A systematic review of 105 neonates. J. Microbiol. Immunol. Infect. 2020. [Google Scholar] [CrossRef]
- Aggarwal, S.; Garcia-Telles, N.; Aggarwal, G.; Lavie, C.; Lippi, G.; Henry, B.M. Clinical features, laboratory characteristics, and outcomes of patients hospitalized with coronavirus disease 2019 (covid-19): Early report from the united states. Diagnosis (Berl) 2020, 7, 91–96. [Google Scholar] [CrossRef]
- Beltran-Corbellini, A.; Chico-Garcia, J.L.; Martinez-Poles, J.; Rodriguez-Jorge, F.; Natera-Villalba, E.; Gomez-Corral, J.; Gomez-Lopez, A.; Monreal, E.; Parra-Diaz, P.; Cortes-Cuevas, J.L.; et al. Acute-onset smell and taste disorders in the context of covid-19: A pilot multicenter pcr-based case-control study. Eur. J. Neurol. 2020. [Google Scholar] [CrossRef]
- Giacomelli, A.; Pezzati, L.; Conti, F.; Bernacchia, D.; Siano, M.; Oreni, L.; Rusconi, S.; Gervasoni, C.; Ridolfo, A.L.; Rizzardini, G.; et al. Self-reported olfactory and taste disorders in patients with severe acute respiratory coronavirus 2 infection: A cross-sectional study. Clin. Infect. Dis. 2020, 71, 889–890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lechien, J.R.; Chiesa-Estomba, C.M.; De Siati, D.R.; Horoi, M.; Le Bon, S.D.; Rodriguez, A.; Dequanter, D.; Blecic, S.; El Afia, F.; Distinguin, L.; et al. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (covid-19): A multicenter European study. Eur. Arch. Otorhinolaryngol. 2020, 277, 2251–2261. [Google Scholar] [CrossRef]
- Moein, S.T.; Hashemian, S.M.R.; Mansourafshar, B.; Khorram-Tousi, A.; Tabarsi, P.; Doty, R.L. Smell dysfunction: A biomarker for covid-19. Int. Forum Allergy Rhinol. 2020, 10, 944–950. [Google Scholar] [CrossRef] [PubMed]
- Roland, L.T.; Gurrola, J.G., 2nd; Loftus, P.A.; Cheung, S.W.; Chang, J.L. Smell and taste symptom-based predictive model for covid-19 diagnosis. Int. Forum. Allergy Rhinol. 2020, 10, 832–838. [Google Scholar] [CrossRef]
- Spinato, G.; Fabbris, C.; Polesel, J.; Cazzador, D.; Borsetto, D.; Hopkins, C.; Boscolo-Rizzo, P. Alterations in smell or taste in mildly symptomatic outpatients with sars-cov-2 infection. JAMA 2020, 323, 2089–2090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaira, L.A.; Salzano, G.; Deiana, G.; De Riu, G. Anosmia and ageusia: Common findings in covid-19 patients. Laryngoscope 2020, 130, 1787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yan, C.H.; Faraji, F.; Prajapati, D.P.; Boone, C.E.; DeConde, A.S. Association of chemosensory dysfunction and covid-19 in patients presenting with influenza-like symptoms. Int. Forum Allergy Rhinol. 2020, 10, 806–813. [Google Scholar] [CrossRef] [Green Version]
- Yan, C.H.; Faraji, F.; Prajapati, D.P.; Ostrander, B.T.; DeConde, A.S. Self-reported olfactory loss associates with outpatient clinical course in covid-19. Int. Forum Allergy Rhinol 2020, 10, 821–831. [Google Scholar] [CrossRef] [Green Version]
- Vaira, L.A.; Salzano, G.; Fois, A.G.; Piombino, P.; De Riu, G. Potential pathogenesis of ageusia and anosmia in covid-19 patients. Int Forum Allergy Rhinol 2020. [Google Scholar] [CrossRef]
- Tong, J.Y.; Wong, A.; Zhu, D.; Fastenberg, J.H.; Tham, T. The prevalence of olfactory and gustatory dysfunction in covid-19 patients: A systematic review and meta-analysis. Otolaryngol. Head Neck Surg. 2020, 163, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Hoang, M.P.; Kanjanaumporn, J.; Aeumjaturapat, S.; Chusakul, S.; Seresirikachorn, K.; Snidvongs, K. Olfactory and gustatory dysfunctions in covid-19 patients: A systematic review and meta-analysis. Asian Pac. J. Allergy Immunol. 2020. [Google Scholar] [CrossRef]
- da Costa, K.V.; Carnaúba, A.T.L.; Rocha, K.W.; de Andrade, K.C.L.; Ferreira, S.M.; Menezes, P.D.L. Olfactory and taste disorders in covid-19: A systematic review. Braz. J. Otorhinolaryngol. 2020. [Google Scholar] [CrossRef]
- Vaira, L.A.; Deiana, G.; Fois, A.G.; Pirina, P.; Madeddu, G.; De Vito, A.; Babudieri, S.; Petrocelli, M.; Serra, A.; Bussu, F.; et al. Objective evaluation of anosmia and ageusia in covid-19 patients: Single-center experience on 72 cases. Head Neck 2020, 42, 1252–1258. [Google Scholar] [CrossRef] [PubMed]
- Vaira, L.A.; Hopkins, C.; Salzano, G.; Petrocelli, M.; Melis, A.; Cucurullo, M.; Ferrari, M.; Gagliardini, L.; Pipolo, C.; Deiana, G.; et al. Olfactory and gustatory function impairment in covid-19 patients: Italian objective multicenter-study. Head Neck 2020, 42, 1560–1569. [Google Scholar] [CrossRef]
- Salzano, F.A.; Mora, R.; Penco, S.; Traverso, D.; Gaggero, G.; Salzano, G.; Guastini, L. Nasal tactile sensitivity in allergic rhinitis. Acta Otolaryngol. 2011, 131, 640–644. [Google Scholar] [CrossRef]
- Vaira, L.A.; Salzano, G.; Petrocelli, M.; Deiana, G.; Salzano, F.A.; De Riu, G. Validation of a self-administered olfactory and gustatory test for the remotely evaluation of covid-19 patients in home quarantine. Head Neck 2020, 42, 1570–1576. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study [Ref.] | Country | Study Population | Study Participants, N | Patients with OGA, N (%) | OGA as Initial Presentation, N (%) | Controls, N | Controls with OGA, N (%) |
|---|---|---|---|---|---|---|---|
| Aggarwal [11] | USA | hospitalized patients | 16 | 3 (18.8) | |||
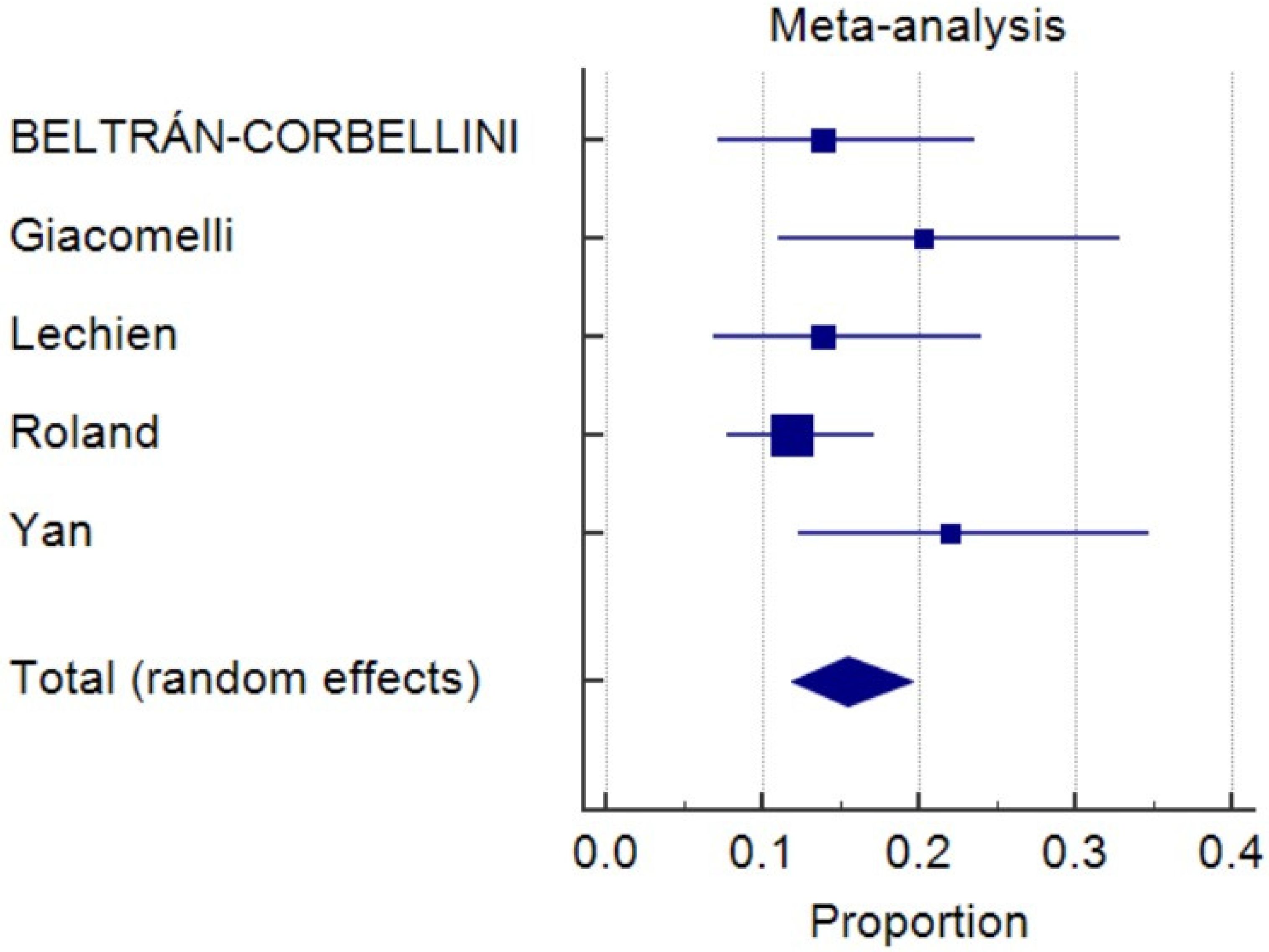
| Beltrán-Corbellini [12] | Spain | hospitalized patients | 79 | 31 (39.2) | 11 (13.9) | 40 | 5 (12.5) |
| Giacomelli [13] | Italy | hospitalized patients | 59 | 20 (33.9) | 12 (20.3) | ||
| Lechien [14] | Belgium, France, Spain, Italy | mild-to-moderate patients | 385 | 362 (94) | |||
| Luers [7] | Germany | not reported | 72 | 54 (75) | 10 (13.9) | ||
| Mao [8] | China | hospitalized patients | 214 | 12 (5.6) | |||
| Moein [15] | Iran | mild, moderate, severe | 60 | 21 (35) | 60 | 11 (18.3) | |
| Roland [16] | USA | hospitalized and outpatients | 145 | 95 (66) | 157 | 42 (26.8) | |
| Spinato [17] | Italy | home patients | 202 | 130 (64.4) | 24 (11.9) | ||
| Vaira [18] | Italy | not reported | 320 | 62 (19.4) | |||
| Yan [19] | USA | hospitalized and outpatients | 59 | 42 (71.2) | 13 (22) | 203 | 35 (17.2) |
| Yan [20] | USA | hospitalized and outpatients | 128 | 75 (58.6) | |||
| Total | 1739 | 907 (48.5) | 70 (15.5) | 460 | 93 (20.2) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chi, H.; Chiu, N.-C.; Peng, C.-C.; Lin, C.-H.; Tai, Y.-L.; Lee, M.-D.; Cheng, Y.-J.; Tan, B.F.; Lin, C.-Y. One-Seventh of Patients with COVID-19 Had Olfactory and Gustatory Abnormalities as Their Initial Symptoms: A Systematic Review and Meta-Analysis. Life 2020, 10, 158. https://doi.org/10.3390/life10090158
Chi H, Chiu N-C, Peng C-C, Lin C-H, Tai Y-L, Lee M-D, Cheng Y-J, Tan BF, Lin C-Y. One-Seventh of Patients with COVID-19 Had Olfactory and Gustatory Abnormalities as Their Initial Symptoms: A Systematic Review and Meta-Analysis. Life. 2020; 10(9):158. https://doi.org/10.3390/life10090158
Chicago/Turabian StyleChi, Hsin, Nan-Chang Chiu, Chun-Chih Peng, Chao-Hsu Lin, Yu-Lin Tai, Ming-Dar Lee, Yu-Jyun Cheng, Boon Fatt Tan, and Chien-Yu Lin. 2020. "One-Seventh of Patients with COVID-19 Had Olfactory and Gustatory Abnormalities as Their Initial Symptoms: A Systematic Review and Meta-Analysis" Life 10, no. 9: 158. https://doi.org/10.3390/life10090158
APA StyleChi, H., Chiu, N.-C., Peng, C.-C., Lin, C.-H., Tai, Y.-L., Lee, M.-D., Cheng, Y.-J., Tan, B. F., & Lin, C.-Y. (2020). One-Seventh of Patients with COVID-19 Had Olfactory and Gustatory Abnormalities as Their Initial Symptoms: A Systematic Review and Meta-Analysis. Life, 10(9), 158. https://doi.org/10.3390/life10090158