
Evaluation of Cortical Bone Microdamage and Primary Stability of Orthodontic Miniscrew Using a Human Bone Analogue

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Specimens
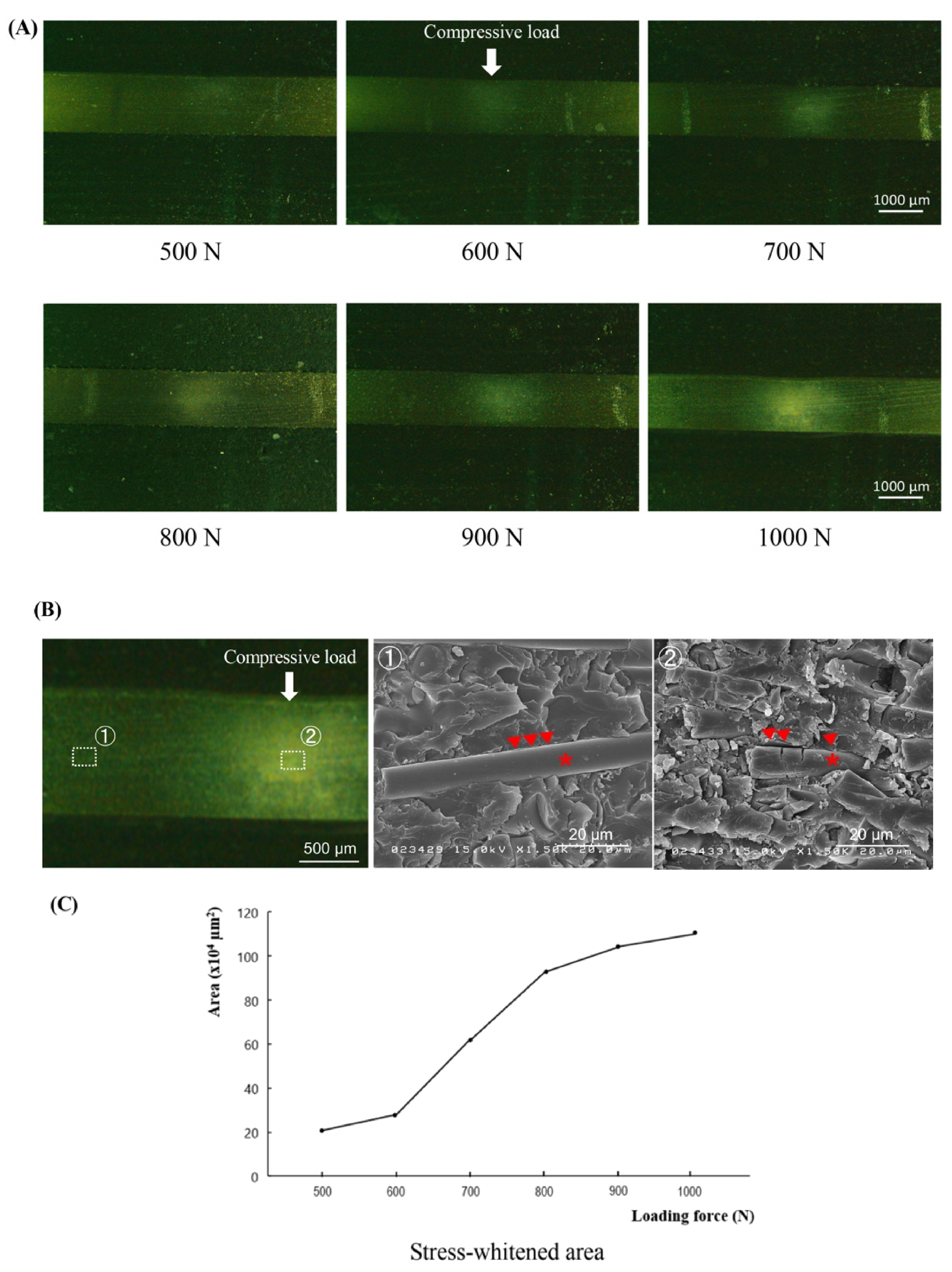
2.2. Indentation Tests
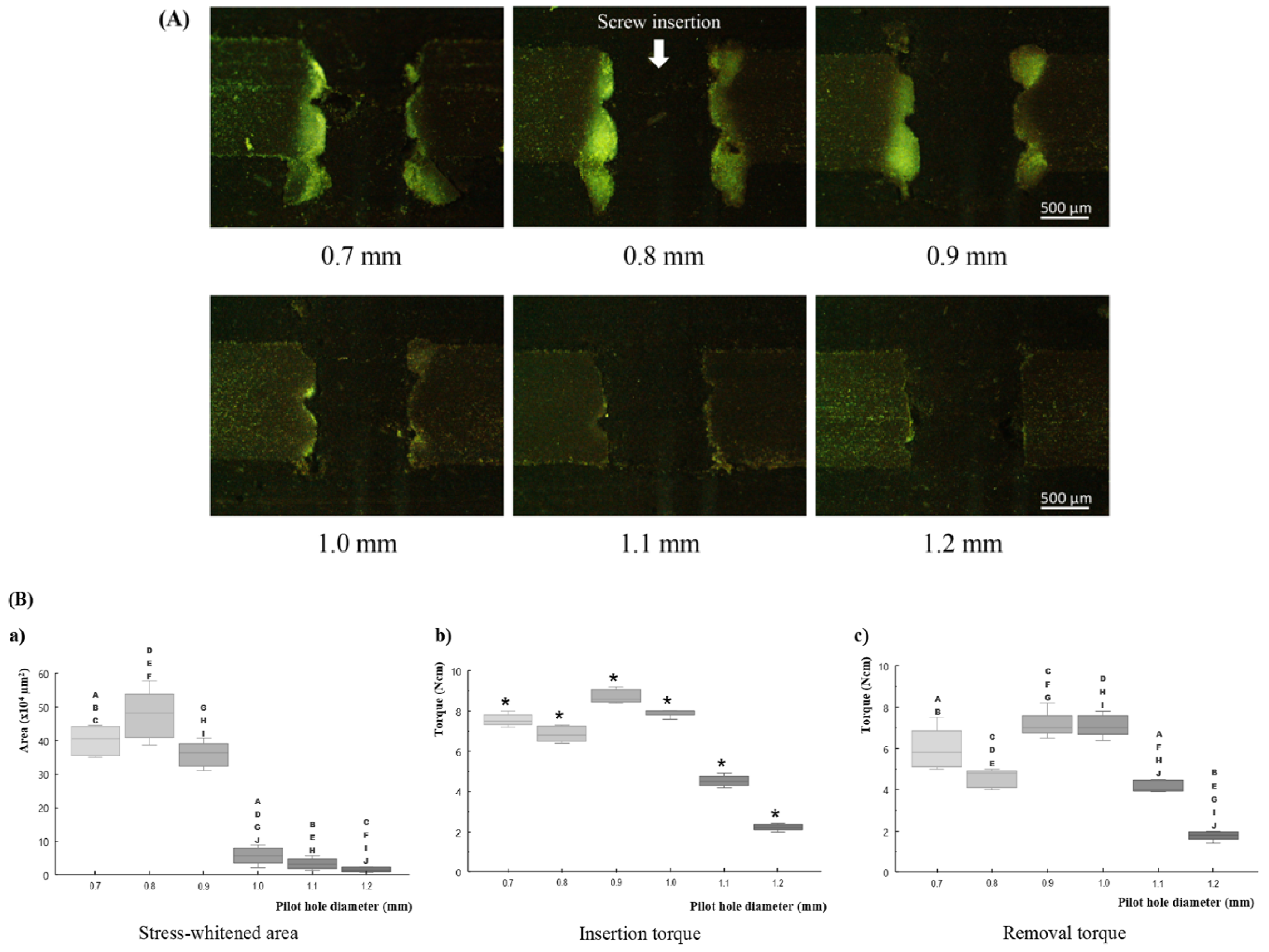
2.3. Miniscrew Insertion Tests
2.4. Statistical Analysis
3. Results
3.1. Indentation Tests
3.2. Miniscrew Insertion Tests
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

References
- Kim, K.B. Temporary Skeletal Anchorage Devices: A Guide to Design and Evidence-Based Solution; Springer: Berlin/Heidelberg, Germany, 2014. [Google Scholar]
- Bornstein, M.M.; Harnisch, H.; Lussi, A.; Buser, D. Clinical performance of wide-body implants with a sandblasted and acid-etched (SLA) surface: Results of a 3-year follow-up study in a referral clinic. Int. J. Oral Maxillofac. Implant. 2007, 22, 631–638. [Google Scholar]
- Chen, Y.; Kyung, H.M.; Zhao, W.T.; Yu, W.J. Critical factors for the success of orthodontic mini-implants: A systematic review. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Khayat, P.G.; Milliez, S.N. Prospective clinical evaluation of 835 multithreaded tapered screw-vent implants: Results after two years of functional loading. J. Oral Implantol. 2007, 33, 225–231. [Google Scholar] [CrossRef]
- Nguyen, M.V.; Codrington, J.; Fletcher, L.; Dreyer, C.W.; Sampson, W.J. The influence of miniscrew insertion torque. Eur. J. Orthod. 2018, 40, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Yadav, S.; Upadhyay, M.; Liu, S.; Roberts, E.; Neace, W.P.; Nanda, R. Microdamage of the cortical bone during mini-implant insertion with self-drilling and self-tapping techniques: A randomized controlled trial. Am. J. Orthod. Dentofac. Orthop. 2012, 141, 538–546. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.S.; Cruz-Marroquin, E.; Sun, J.; Stewart, K.T.; Allen, M.R. Orthodontic mini-implant diameter does not affect in-situ linear microcrack generation in the mandible or the maxilla. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 768–773. [Google Scholar] [CrossRef] [PubMed]
- Shank, S.B.; Beck, F.M.; D’Atri, A.M.; Huja, S.S. Bone damage associated with orthodontic placement of miniscrew implants in an animal model. Am. J. Orthod. Dentofac. Orthop. 2012, 141, 412–418. [Google Scholar] [CrossRef] [PubMed]
- Sowden, D.; Schmitz, J.P. AO self-drilling and self-tapping screws in rat calvarial bone: An ultrastructural study of the implant interface. J. Oral Maxillofac. Surg. 2002, 60, 294–299, discussion 300. [Google Scholar] [CrossRef]
- Taing-Watson, E.; Katona, T.R.; Stewart, K.T.; Ghoneima, A.; Chu, G.T.; Kyung, H.M.; Liu, S.S. Microdamage generation by tapered and cylindrical mini-screw implants after pilot drilling. Angle Orthod. 2015, 85, 859–867. [Google Scholar] [CrossRef] [Green Version]
- Florvaag, B.; Kneuertz, P.; Lazar, F.; Koebke, J.; Zoller, J.E.; Braumann, B.; Mischkowski, R.A. Biomechanical properties of orthodontic miniscrews. An in-vitro study. J. Orofac. Orthop. 2010, 71, 53–67. [Google Scholar] [CrossRef]
- Uemura, M.; Motoyoshi, M.; Yano, S.; Sakaguchi, M.; Igarashi, Y.; Shimizu, N. Orthodontic mini-implant stability and the ratio of pilot hole implant diameter. Eur. J. Orthod. 2012, 34, 52–56. [Google Scholar] [CrossRef] [Green Version]
- Wilmes, B.; Rademacher, C.; Olthoff, G.; Drescher, D. Parameters affecting primary stability of orthodontic mini-implants. J. Orofac. Orthop. 2006, 67, 162–174. [Google Scholar] [CrossRef]
- Nguyen, M.V.; Codrington, J.; Fletcher, L.; Dreyer, C.W.; Sampson, W.J. Influence of cortical bone thickness on miniscrew microcrack formation. Am. J. Orthod. Dentofac. Orthop. 2017, 152, 301–311. [Google Scholar] [CrossRef]
- Jin, J.; Kim, G.T.; Kwon, J.S.; Choi, S.H. Effects of intrabony length and cortical bone density on the primary stability of orthodontic miniscrews. Materials 2020, 13, 5615. [Google Scholar] [CrossRef]
- Kang, S.Y.; Yu, J.M.; Kim, H.S.; Lee, J.S.; Yeon, C.M.; Park, K.S.; Choi, S.H.; Lee, S.Y. Influence of orthodontic anchor screw anchorage method on the stability of artificial bone: An in vitro study. Materials 2020, 13, 3205. [Google Scholar] [CrossRef] [PubMed]
- Russell, W.M.S.; Burch, R.L. The Principles of Humane Experimental Technique; Methuen: London, UK, 1959. [Google Scholar]
- Cheng, S.; Feng, P.; Li, Z.; Du, J. Mechanical behavior of cylindrical GFRP chimney liners subjected to axial tension. Compos. Part B Eng. 2019, 177, 107411. [Google Scholar] [CrossRef]
- Feldmann, A.; Schweizer, M.; Stucki, S.; Nolte, L. Experimental evaluation of cortical bone substitute materials for tool development, surgical training and drill bit wear investigations. Med. Eng. Phys. 2019, 66, 107–112. [Google Scholar] [CrossRef]
- Bayarchimeg, D.; Namgoong, H.; Kim, B.K.; Kim, M.D.; Kim, S.; Kim, T.I.; Seol, Y.J.; Lee, Y.M.; Ku, Y.; Rhyu, I.; et al. Evaluation of the correlation between insertion torque and primary stability of dental implants using a block bone test. J. Periodontal. Implant Sci. 2013, 43, 30–36. [Google Scholar] [CrossRef] [Green Version]
- Ahn, S.J.; Leesungbok, R.; Lee, S.W.; Heo, Y.K.; Kang, K.L. Differences in implant stability associated with various methods of preparation of the implant bed: An in vitro study. J. Prosthet. Dent. 2012, 107, 366–372. [Google Scholar] [CrossRef]
- Pithon, M.M.; Nojima, M.G.; Nojima, L.I. In vitro evaluation of insertion and removal torques of orthodontic mini-implants. Int. J. Oral Maxillofac. Surg. 2011, 40, 80–85. [Google Scholar] [CrossRef]
- Sakin, Ç.; Aylikci, Ö. Techniques to measure miniscrew implant stability. J. Orthod. Res. 2013, 1, 5–10. [Google Scholar] [CrossRef]
- Gerde, E.; Marder, M. Friction and fracture. Nature 2001, 413, 285–288. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Ye, T.; Deng, L.; Shao, J.; Qi, J.; Zhou, Q.; Wei, L.; Qiu, S. Repair of microdamage in osteonal cortical bone adjacent to bone screw. PLoS ONE 2014, 9, e89343. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Density (g/mL) | 1.7 |
| Ultimate tensile strength (MPa) | 90.0 |
| Modulus of elasticity (GPa) | 12.4 |
| Compressive yield strength (MPa) | 120.0 |
| Compressive modulus (GPa) | 7.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Teekavanich, C.; Uezono, M.; Takakuda, K.; Ogasawara, T.; Techalertpaisarn, P.; Moriyama, K. Evaluation of Cortical Bone Microdamage and Primary Stability of Orthodontic Miniscrew Using a Human Bone Analogue. Materials 2021, 14, 1825. https://doi.org/10.3390/ma14081825
Teekavanich C, Uezono M, Takakuda K, Ogasawara T, Techalertpaisarn P, Moriyama K. Evaluation of Cortical Bone Microdamage and Primary Stability of Orthodontic Miniscrew Using a Human Bone Analogue. Materials. 2021; 14(8):1825. https://doi.org/10.3390/ma14081825
Chicago/Turabian StyleTeekavanich, Chutimont, Masayoshi Uezono, Kazuo Takakuda, Takeshi Ogasawara, Paiboon Techalertpaisarn, and Keiji Moriyama. 2021. "Evaluation of Cortical Bone Microdamage and Primary Stability of Orthodontic Miniscrew Using a Human Bone Analogue" Materials 14, no. 8: 1825. https://doi.org/10.3390/ma14081825