Dietary Patterns in Secondary Prevention of Heart Failure: A Systematic Review

Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Study Selection
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Assessment of Bias Risk and Study Quality
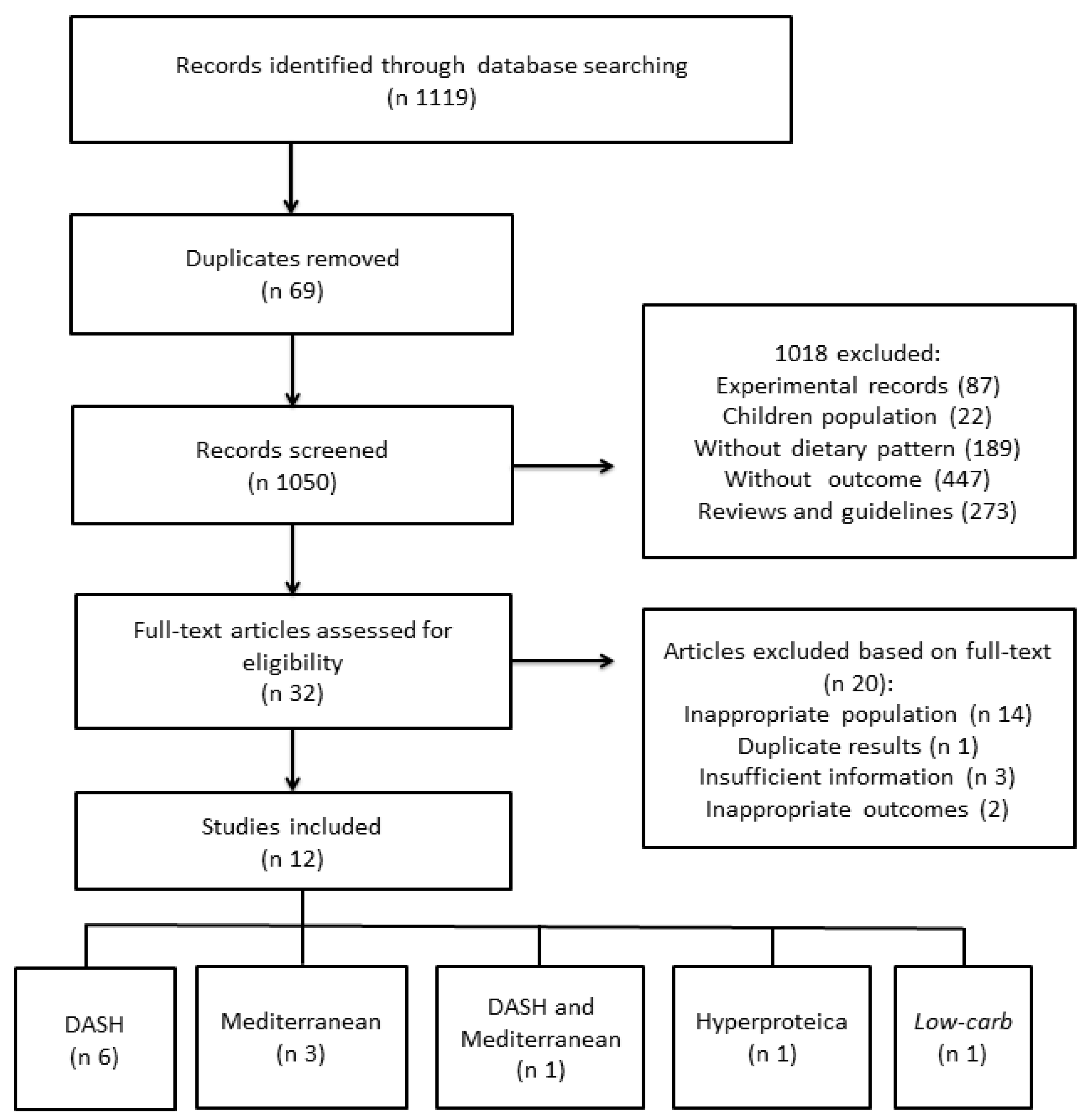
3. Results
3.1. Descriptions of Studies
3.2. Quality and Publication Bias Assessment
3.3. DASH
3.4. Mediterranean
3.5. Low-Carb
3.6. Hyperproteic
4. Discussion
Limitations
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Study | SD | RSG | AC | Blinding of Research | Blinding of PP | Blinding of OA | LE | Do They Describe Confounders in an Adjusted Analysis? | Do You Assess the Balance between the Groups at the Start of the Study? |
|---|---|---|---|---|---|---|---|---|---|
| Rifai et al. [25] | RCT | Low risk | Unclear risk | High risk | High risk | High risk | Unclear risk | NA | NA |
| Silver * [17] | RCT | Unclear risk | Unclear risk | Unclear risk | Unclear risk | Unclear risk | Unclear risk | NA | NA |
| Vittos et al. * [21] | Cohort | NA | NA | NA | NA | NA | NA | Unclear risk | Low risk |
| Hummel et al., (2012) [23] | Cohort | NA | NA | NA | NA | NA | NA | Unclear risk | Low risk |
| Hummel et al., (2013) [24] | Cohort | NA | NA | NA | NA | NA | NA | Unclear risk | Low risk |
| Hummel et al., (2014) * [20] | Cohort | NA | NA | NA | NA | NA | NA | Low risk | Unclear risk |
| Chrysohoou et al., (2009a) * [18] | Cross-sectional study | NA | NA | NA | NA | NA | NA | Low risk | Unclear risk |
| Chrysohoou et al. (2009b) * [19] | Cross-sectional study | NA | NA | NA | NA | NA | NA | Low risk | Unclear risk |
| Chrysohoou et al., (2012) [26] | Cross-sectional study | NA | NA | NA | NA | NA | NA | Low risk | Low risk |
| Levitan et al. [22] | Cohort | NA | NA | NA | NA | NA | NA | Low risk | Low risk |
| Gonzales et al. * [16] | RCT | Unclear risk | Unclear risk | Unclear risk | Unclear risk | Unclear risk | Unclear risk | NA | NA |
| Evangelista et al. [27] | RCT | Unclear risk | Unclear risk | Unclear risk | Unclear risk | Unclear risk | Unclear risk | NA | NA |
| Study | SD | Population (N) | Age (years) | Intervention | Control/Comparison | Duration of Intervention | Outcomes |
|---|---|---|---|---|---|---|---|
| Rifai et al., 2015 [25] | RCT | Patients with chronic HF (48) | Intervention: 60 ± 11 Comparison: 64 ± 12 | DASH | General HF dietary recommendations | 3 months | Functional capacity 6-min walk test (m): Baseline: DASH = 254 ± 119 Comparison = 202 ± 77 p = 0.158 After 3 months: DASH = 292 ± 124 Comparison = 197 ±81 p = 0.018 Quality of life (MLHFQ index) Baseline: DASH = 29 ± 20 Comparison = 38 ± 4 p = 0.056 After 3 months: DASH = 21 ± 15 Comparison = 39 ± 22 p = 0.006 |
| Silver, 2014 * [17] | RCT | Patients with chronic HF (40) | 40 to 84 | DASH | UD | 30 days | Functional capacity 6-min walk test (m): Baseline: DASH = 255 After 30 days: DASH = 292 p < 0.05 Cardiac function (∆ units): After 30 days: DASH = > 4 p < 0.05 |
| Vittos et al., 2013 * [21] | Cohort | Hypertensive patients with compensated HFpEF (17) + healthy controls (10) | NR | DASH | DASH | 21 days | Oxidative stress MPO activity (UI/L): Baseline: Intervention: 303.04 ± 18.7 Control: 248.0 ± 21.3 After 21 days: Intervention: 282.1 ± 14.9 p < 0.05 BP (mmHg): Intervention group Systolic Baseline: 158 After 21 days: 140 p <0.05 Diastolic Baseline: 81 After 21 days: 75 p < 0.05 |
| Hummel et al., 2012 [23] | Cohort | Hypertensive patients with compensated HFpEF (13) | 72 ± 10 | DASH | NA | 21 days | Functional capacity 6-min walk test (m): Baseline: 313 ± 86 After 21 days: 337 ± 91 p = 0.006 BP (mmHg): Clinic Systolic: Baseline: 155 ± 29 After 21 days: 138± 22 p = 0.02 Clinic Diastolic: Baseline: 79 ± 15 After 21 days: 72 ± 8 p = 0.04 24-h ambulatory systolic: Baseline: 130 ± 4 After 21 days: 123 ± 4 p = 0.02 24-h ambulatory diastolic: Baseline: 67 ± 3 After 21 days: 62 ± 3 p = 0.02 Oxidative stress Urinary F2-isoprostanes (pmol/mmol de Cr): Baseline: 209 After 21 days: 144 p = 0.02 |
| Hummel et al., 2013 [24] | Cohort | Hypertensive patients with compensated HFpEF (13) | 72 ± 10 | DASH | NA | 21 days | Cardiac function Arterial elastance (mmHg/mL): Baseline: 2.0 ± 0.4 After 21 days: 1.7 ± 0.4 p = 0.007 Ventricular-atrial coupling: Baseline: 1.5 ± 0.3 After 21 days: 1.7 ± 0.4 p = 0.04 Viscoelastic/relaxation flexibility (beats/min): Baseline: 24.3 ± 5.3 After 21 days: 22.7 ± 8.1 p = 0.03 Chamber stiffness (s-1): Baseline: 252 ± 115 After 21 days: 170 ± 37 p = 0.03 |
| Hummel et al., 2014 * [20] | Cohort | Hypertensive patients with compensated HFpEF (12) | NR | DASH | NA | 21 days | Oxidative stress F2-isoprostanes:Cr (pg/Mg): Baseline: 6.0 ± 2.5 After 21 days: 4.3 ± 1.4 p = 0.04 Aldosterone:Cr (pg/mg) Baseline: 6.7 ± 2.6 After 21 days: 14.2 ± 7.3 p = 0.009 Na:Cr (mg Na/mg Cr) Baseline: 59 ± 79 After 21 days: 30 ± 20 p = 0.01 ∆MBG:Cr × ∆Na:Cr β = 23.8 p < 0.001 ∆MBG:Cr × ∆F2-isoprostanes:Cr β = 1.1 p = 0.06 |
| Chrysohoou et al., 2009a * [18] | Cross-sectional study | Patients with chronic HF (218) | M: 63 ± 13 W: 65 ± 13 | Mediterranean diet | NA | NA | Cardiac function Wave speed: Smv = 0.62 ± 0.08, p = 0.001 Stv = 0.25 ± 0.09, p = 0.07 LVEF = 0.58 ± 0.30, p = 0.05 LAEF = 2.20 ± 0.67, p = 0.001 Emv = 0.69 ± 0.17, p = 0.001 Amv = 0.42 ± 0.20, p = 0.03 |
| Chrysohoou et al., 2009b * [19] | Cross-sectional study | Patients with chronic HF (106) | 65 ± 14 | Mediterranean diet | NA | NA | Inflammatory cytokines: IL-6 = r = −0.56 ± 0.168 p = 0.004 TNF-a = r = −0.599 ± 0.281 p = 0.047 Cytokines x Quality of life: R = −0.52 ± 0.25, p = 0.040 |
| Chrysohoou et al., 2012 [26] | Cross-sectional study | Patients with systolic HF (372) | M: 64 ± 13 W: 63 ± 13 | Mediterranean diet | NA | NA | Cardiac function Before the adjusted analysis: log Smv: R = 0.154, p = 0.009 LAEF: R = 0.133, p = 0.041 Log E/AR = −0.24, p = 0.001 Log Emv/Amv: R = −0.133, p = 0.041 E/AxMDS: b =−0.225 ± 0.092, β = −0.782, p = 0.04 |
| Levitan et al., 2013 [22] | Cohort | Postmenopausal women with HF (3.215) | 50 to 79 | Mediterranean and DASH diets | NA | 4.6 years | Mortality Mortality rate per 100 person-years 1: Mediterranean diet Q1 (lower adherence): 10.1 Q4 (higher adherence): 8.0 HR 0.85 (IC 95% 0.70–1.02) p = 0.08 DASH diet Q1: 10.0 Q4: 8.8 HR 0.84 (IC 95% 0.70–1.00) p = 0.01 |
| Gonzales et al., 2015 * [16] | RCT | Patients with stable chronic HF (123) | NR | Low-carb diet + exercise (group A) (n = 18):40% CHO, 40% LIP, 20% PTN Low-carb diet (group B) (n = 45):40% CHO, 40% LIP, 20%PTN | UD+ exercise (group C) (n = 21): 50% CHO, 30% LIP, 20%PTN UD (group D) (n = 39): 50% CHO, 30% LIP, 20% PTN | 2 months | Functional capacity 6-min walk test (m): Group A: Baseline: 270.37 ± 11.39 After 2 months: 301.78 ± 7.02 p = 0.08 Group B: Baseline: 345.77 ± 22.32 After 2 months: 370.07 ± 26.15 p = 0.05 BP diastolic: Group A: Baseline: 71.5 ± 2.98 After 2 months: 62.5 ± 1.70 p = 0.03 Group C: Baseline: 71.76 ± 2.31 After 2 months: 64.69 ± 1.9 p = 0.04 |
| Evangelista et al., 2009 [27] | RCT | Ambulatory patients with HF, DM2 (untreated with insulin), overweight (BMI ≥ 27) and not eligible for transplantation (14) | 58.8 ± 9.7 | Hyperproteic and hypocaloric diet (HP) (n = 5): 40% CHO, 30% PTN, 30% LIP Normoproteic and hypocaloric (NP) (n = 5): 55% CHO, 15% PTN, 30% LIP | UD (n = 4) | 12 weeks | Functional capacity 6-min walk test (m): HP: 87.5± 21.0 NP: −3.7± 21.0 UD: −42.2 ± 23.5 p = 0.01 VO2 max máximo (mL/kg/min): HP: 3.1 ± 1.0 NP: −0.3 ± 1.0 UD: −0.3 ± 1.1 p = 0.003 Quality of life (MLHFQ index): MLHFQ general HP: −20.1 ± 9.5 NP: −12.2 ± 4.3 UD: −5.1 ± 3.9 p = 0.046 |
References
- McMurray, J.J.; Adamopoulos, S.; Anker, S.D.; Auricchio, A.; Böhm, M.; Dickstein, K.; Falk, V.; Filippatos, G.; Fonseca, C.; Gomez-Sanchez, M.A. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2012, 33, 1787–1847. [Google Scholar] [PubMed] [Green Version]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.; Coats, A.J.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, C.J.; Wu, C.; Jones, M.; Kato, T.S.; Dam, T.T.; Givens, R.C.; Templeton, D.L.; Maurer, M.S.; Naka, Y.; Takayama, H.; et al. Reduced handgrip strength as a marker of frailty predicts clinical outcomes in patients with heart failure undergoing ventricular assist device placement. J. Card. Fail. 2014, 20, 310–315. [Google Scholar] [CrossRef] [PubMed]
- Lloyd-Jones, D.M.; Larson, M.G.; Leip, E.P.; Beiser, A.; D’Agostino, R.B.; Kannel, W.B. Lifetime risk for developing congestive heart failure: The Framingham Heart Study. Circulation 2002, 106, 3068–3072. [Google Scholar] [CrossRef] [PubMed]
- Nichols, G.A.; Gullion, C.M.; Koro, C.E.; Ephross, S.A.; Brown, J.B. The incidence of congestive heart failure in type 2 diabetes: An update. Diabetes Care 2004, 27, 1879–1884. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Ogden, L.G.; Bazzano, L.A.; Vupputuri, S.; Loria, C.; Whelton, P.K. Risk factors for congestive heart failure in US men and women: NHANES I epidemiologic follow-up study. Arch. Intern. Med. 2001, 161, 996–1002. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, S.; Chen, S.; Hong, L.; Sun, K.; Gong, E.; Li, C. Effect of Mobile Health Interventions on the Secondary Prevention of Cardiovascular Disease: Systematic Review and Meta-analysis. Can. J. Cardiol. 2017, 33, 219–231. [Google Scholar] [CrossRef] [PubMed]
- Labrunée, M.; Pathak, A.; Loscos, M.; Coudeyre, E.; Casillas, J.M.; Gremeaux, V. Therapeutic education in cardiovascular diseases: State of the art and perspectives. Ann. Phys. Rehabil. Med. 2012, 55, 322–341. [Google Scholar] [CrossRef] [PubMed]
- Prince, M.J.; Wu, F.; Guo, Y.; Robledo, L.M.G.; O’Donnell, M.; Sullivan, R.; Yusuf, S. The burden of disease in older people and implications for health policy and practice. Lancet 2015, 385, 549–562. [Google Scholar] [CrossRef]
- González-Salvado, V.; Barcala-Furelos, R.; Neiro-Rey, C.; Varela-Casal, C.; Peña-Gil, C.; Ruano-Raviña, A. Cardiac rehabilitation: The missing link to close the chain of survival? Resuscitation 2017, 113, e7–e8. [Google Scholar] [CrossRef] [PubMed]
- Mitter, S.S.; Yancy, C.W. Contemporary Approaches to Patients with Heart Failure. Cardiol. Clin. 2017, 35, 261–271. [Google Scholar] [CrossRef] [PubMed]
- d’Almeida, K.S.M.; Spillere, S.R.; Zuchinali, P.; Souza, G.C. Mediterranean Diet and Other Dietary Patterns in Primary Prevention of Heart Failure and Changes in Cardiac Function Markers: A Systematic Review. Nutrients 2018, 10, 58. [Google Scholar] [CrossRef] [PubMed]
- Sciatti, E.; Lombardi, C.; Ravera, A.; Vizzardi, E.; Bonadei, I.; Carubelli, V.; Gorga, E.; Metra, M. Nutritional Deficiency in Patients with Heart Failure. Nutrients 2016, 8, 442. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Grren, S. Cochrane Handbook for Systematic Reviews of Interventions, version 5.1; John Wiley & Sons Ltd.: Chichester, UK, 2011. [Google Scholar]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzalez, D.G.; Orea, A.; Castillo, L.; Vaquero, N.; Lozada, M.; Bernal, M.F.; Lozano, O.; Kauffman, E. The effect of low-carbohydrate diet and exercise on clinical status in chronic stable heart failure patients. Eur. J. Heart Fail. 2015, 17, 108. [Google Scholar]
- Silver, M.A. Is the DASH diet optimal for heart failure patients? Time for a randomized trial. Eur. J. Heart Fail. 2014, 16, 162. [Google Scholar]
- Chrysohoou, C.; Metallinos, G.; Aggelopoulos, P.; Kastorini, C.; Athanasopoulou, S.; Pitsavos, C.; Panagiotakos, D.B.; Stefanadis, C. Long-term adherence to the traditional Mediterranean diet is associated with improved biventricular systolic function, in chronic heart failure patients. Eur. J. Heart Fail. 2009, 120, 739. [Google Scholar]
- Chrysohoou, C.; Kotrogiannis, I.; Vasiliadou, C.; Kastorini, C.; Aggelopoulos, P.; Metallinos, G.; Athanasopoulou, S.; Pitsavos, C.; Stefanadis, C. The role of Mediterranean diet on subclinical inflammation and quality of life in patients with newly diagnosed systolic heart failure (The Hellenic heart failure study). Eur. Heart J. 2009, 30, 1032. [Google Scholar]
- Hummel, S.L.; Marolt, C.; Healy, A.; Tang, W.W.; Weder, A.B.; Fedorova, O.V.; Bagrov, A.Y.; Kennedy, D.J. Cardiotonic Steroids and Sodium Excretion in Heart Failure with Preserved Ejection Fraction. J. Card. Fail. 2014, 20, S79–S80. [Google Scholar] [CrossRef]
- Vittos, O.; Halici, F.; Toana, B.; Marta, D.; Vittos, A.; Moldoveanu, E. Myeloperoxidase activity and sodium restricted diet in heart failure patients with preserved ejection fraction. Eur. J. Heart Fail. 2013, 15, S352. [Google Scholar]
- Levitan, E.B.; Lewis, C.E.; Tinker, L.F.; Eaton, C.B.; Ahmed, A.; Manson, J.E.; Snetselaar, L.G.; Martin, L.W.; Trevisan, M.; Howard, B.V.; et al. Mediterranean and DASH diet scores and mortality in women with heart failure: The Women’s Health Initiative. Circ. Heart Fail. 2013, 6, 1116–1123. [Google Scholar] [CrossRef] [PubMed]
- Hummel, S.L.; Seymour, E.M.; Brook, R.D.; Kolias, T.J.; Sheth, S.S.; Rosenblum, H.R.; Wells, J.M.; Weder, A.B. Low-Sodium DASH Diet Reduces Blood Pressure, Arterial Stiffness and Oxidative Stress in Hypertensive HFPEF. Hypertension 2012, 60, 1200–1206. [Google Scholar] [CrossRef] [PubMed]
- Hummel, S.L.; Seymour, E.M.; Brook, R.D.; Sheth, S.S.; Ghosh, E.; Zhu, S.; Weder, A.B.; Kovács, S.J.; Kolias, T.J. Low-Sodium DASH Diet Improves Diastolic Function and Ventricular-Arterial Coupling in Hypertensive Heart Failure with Preserved Ejection Fraction. Circ. Heart Fail. 2013, 6, 1165–1171. [Google Scholar] [CrossRef] [PubMed]
- Rifai, L.; Pisano, C.; Hayden, J.; Sulo, S.; Silver, M.A. Impact of the DASH diet on endothelial function, exercise capacity and quality of life in patients with heart failure. Bayl. Univ. Med. Cent. Proc. 2015, 28, 151–156. [Google Scholar] [CrossRef]
- Chrysohoou, C.; Pitsavos, C.; Metallinos, G.; Antoniou, C.; Oikonomou, E.; Kotroyiannis, I.; Tsantilas, A.; Tsitsinakis, G.; Tousoulis, D.; Panagiotakos, D.B.; et al. Cross-sectional relationship of Mediterranean type diet to diastolic heart function in chronic heart failure patients. Heart Vessels 2012, 27, 576–584. [Google Scholar] [CrossRef] [PubMed]
- Evangelista, L.S.; Heber, D.; Li, Z.; Bowerman, S.; Hamilton, M.A.; Fonarow, G.C. Reduced body weight and adiposity with a high-protein diet improves functional status, lipid profiles, glycemic control and quality of life in patients with heart failure: A feasibility study. J. Cardiovasc. Nurs. 2009, 24, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Folsom, A.R.; Parker, E.D.; Harnack, L.J. Degree of concordance with DASH diet guidelines and incidence of hypertension and fatal cardiovascular disease. Am. J. Hypertens. 2007, 20, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Panagiotakos, D.B.; Pitsavos, C.; Stefanadis, C. Dietary patterns: A mediterranean diet score and its relation to clinical and biological markers of cardiovascular disease risk. Nutr. Metab. Cardiovasc. Dis. 2006, 16, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Salehi-Abargouei, A.; Maghsoudi, Z.; Shirani, F.; Azadbakht, L. Effects of Dietary Approaches to Stop Hypertension (DASH)-style diet on fatal or nonfatal cardiovascular diseases—Incidence: A systematic review and meta-analysis on observational prospective studies. Nutrition 2013, 29, 611–618. [Google Scholar] [CrossRef] [PubMed]
- Siervo, M.; Lara, J.; Chowdhury, S.; Ashor, A.; Oggioni, C.; Mathers, J.C. Effects of the Dietary Approach to Stop Hypertension (DASH) diet on cardiovascular risk factors: A systematic review and meta-analysis. Br. J. Nutr. 2015, 113, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Eilat-Adar, S.; Sinai, T.; Yosefy, C.; Henkin, Y. Nutritional recommendations for cardiovascular disease prevention. Nutrients 2013, 5, 3646–3683. [Google Scholar] [CrossRef] [PubMed]
- Struijk, E.A.; May, A.M.; Wezenbeek, N.L.; Fransen, H.P.; Soedamah-Muthu, S.S.; Geelen, A.; Boer, J.M.; van der Schouw, Y.T.; Bueno-de-Mesquita, H.B.; Beulens, J.W. Adherence to dietary guidelines and cardiovascular disease risk in the EPIC-NL cohort. Int. J. Cardiol. 2014, 176, 354–359. [Google Scholar] [CrossRef] [PubMed]
- Saneei, P.; Salehi-Abargouei, A.; Esmaillzadeh, A.; Azadbakht, L. Influence of Dietary Approaches to Stop Hypertension (DASH) diet on blood pressure: A systematic review and meta-analysis on randomized controlled trials. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 1253–1261. [Google Scholar] [CrossRef] [PubMed]
- Aaron, K.J.; Sanders, P.W. Role of dietary salt and potassium intake in cardiovascular health and disease: A review of the evidence. Mayo Clin. Proc. 2013, 88, 987–995. [Google Scholar] [CrossRef] [PubMed]
- d’El-Rei, J.; Cunha, A.R.; Trindade, M.; Neves, M.F. Beneficial effects of dietary nitrate on endothelial function and blood pressure levels. Int. J. Hypertens. 2016, 2016, 6791519. [Google Scholar] [CrossRef] [PubMed]
- Vongpatanasin, W.; Peri-Okonny, P.; Velasco, A.; Arbique, D.; Wang, Z.; Ravikumar, P.; Adams-Huet, B.; Moe, O.W.; Pak, C.Y. Effects of Potassium Magnesium Citrate Supplementation on 24-Hour Ambulatory Blood Pressure and Oxidative Stress Marker in Prehypertensive and Hypertensive Subjects. Am. J. Cardiol. 2016, 118, 849–853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopes, H.F.; Martin, K.L.; Nashar, K.; Morrow, J.D.; Goodfriend, T.L.; Egan, B.M. DASH diet lowers blood pressure and lipid-induced oxidative stress in obesity. Hypertension 2003, 41, 422–430. [Google Scholar] [CrossRef] [PubMed]
- Asemi, Z.; Samimi, M.; Tabassi, Z.; Shakeri, H.; Sabihi, S.S.; Esmaillzadeh, A. Effects of DASH diet on lipid profiles and biomarkers of oxidative stress in overweight and obese women with polycystic ovary syndrome: A randomized clinical trial. Nutrition 2014, 30, 1287–1293. [Google Scholar] [CrossRef] [PubMed]
- Puchau, B.; Zulet, M.A.; de Echavarri, A.G.; Hermsdorff, H.H.; Martinez, J.A. Dietary total antioxidant capacity is negatively associated with some metabolic syndrome features in healthy young adults. Nutrition 2010, 26, 534–541. [Google Scholar] [CrossRef] [PubMed]
- Gates, P.E.; Tanaka, H.; Hiatt, W.R.; Seals, D.R. Dietary sodium restriction rapidly improves large elastic artery compliance in older adults with systolic hypertension. Hypertension 2004, 44, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Jablonski, K.L.; Racine, M.L.; Geolfos, C.J.; Gates, P.E.; Chonchol, M.; McQueen, S.M.B.; Seals, D.R. Dietary sodium restriction reverses vascular endothelial dysfunction in middle-aged/older adults with moderately elevated systolic blood pressure. J. Am. Coll. Cardiol. 2013, 61, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Rostagno, C.; Gensini, G.F. Six minute walk test: A simple and useful test to evaluate functional capacity in patients with heart failure. Intern. Emerg. Med. 2008, 3, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Szlachcic, J.; Massie, B.M.; Kramer, B.L.; Topic, N.; Tubau, J. Correlates and prognostic implication of exercise capacity in chronic congestive heart failure. Am. J. Cardiol. 1985, 55, 1037–1042. [Google Scholar] [CrossRef]
- Mackenbach, J.D.; Burgoine, T.; Lakerveld, J.; Forouhi, N.G.; Griffin, S.J.; Wareham, N.J.; Monsivais, P. Accessibility and Affordability of Supermarkets: Associations with the DASH Diet. Am. J. Prev. Med. 2017, 53, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.M.M.; Fung, T.T.; Steck, S.E.; Zhang, J.; Hazlett, L.J.; Han, K.; Lee, S.H.; Merchant, A.T. Diet Quality and Mortality Risk in Metabolically Obese Normal-Weight Adults. Mayo Clin. Proc. 2016, 91, 1372–1383. [Google Scholar] [CrossRef] [PubMed]
- Stefler, D.; Malyutina, S.; Kubinova, R.; Pajak, A.; Peasey, A.; Pikhart, H.; Brunner, E.J.; Bobak, M. Mediterranean diet and mortality in eastern Europeans: Results from the HAPIEE study. Eur. J. Nutr. 2017, 56, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Tong, T.Y.; Wareham, N.J.; Khaw, K.T.; Imamura, F.; Forouhi, N.G. Prospective association of the Mediterranean diet with cardiovascular disease incidence and mortality and its population impact in a non-Mediterranean population: The EPIC-Norfolk study. BMC Med. 2016, 14, 135. [Google Scholar] [CrossRef] [PubMed]
- Bonaccio, M.; Di Castelnuovo, A.; Costanzo, S.; Persichillo, M.; De Curtis, A.; Donati, M.B.; De Gaetano, G.; Iacoviello, L.; MOLI-SANI Study Investigators. Adherence to the traditional Mediterranean diet and mortality in subjects with diabetes. Prospective results from the MOLI-SANI study. Eur. J. Prev. Cardiol. 2016, 23, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Limongi, F.; Noale, M.; Gesmundo, A.; Crepaldi, G.; Maggi, S. Adherence to the Mediterranean Diet and all-cause mortality risk in an elderly Italian population: Data from the ILSA study. J. Nutr. Health Aging 2017, 21, 505–513. [Google Scholar] [CrossRef] [PubMed]
- Mohammadifard, N.; Talaei, M.; Sadeghi, M.; Oveisegharan, S.; Golshahi, J.; Esmaillzadeh, A.; Sarrafzadegan, N. Dietary patterns and mortality from cardiovascular disease: Isfahan Cohort Study. Eur. J. Clin. Nutr. 2017, 71, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Veronese, N.; Stubbs, B.; Noale, M.; Solmi, M.; Luchini, C.; Maggi, S. Adherence to the Mediterranean diet is associated with better quality of life: Data from the Osteoarthritis Initiative. Am. J. Clin. Nutr. 2016, 104, 1403–1409. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, P.H.; Ruano, C.; De Irala, J.; Ruiz-Canela, M.; Martinez-Gonzalez, M.A.; Sánchez-Villegas, A. Adherence to the Mediterranean diet and quality of life in the SUN Project. Eur. J. Clin. Nutr. 2012, 66, 360–368. [Google Scholar] [CrossRef] [PubMed]
- Bonaccio, M.; Di Castelnuovo, A.; Bonanni, A.; Costanzo, S.; De Lucia, F.; Pounis, G.; Zito, F.; Donati, M.B.; De Gaetano, G.; Iacoviello, L. Adherence to a Mediterranean diet is associated with a better health-related quality of life: A possible role of high dietary antioxidant contente. BMJ Open 2013, 3, e003003. [Google Scholar] [CrossRef] [PubMed]
- Butler, T. Dietary management of heart failure: Room for improvement? Br. J. Nutr. 2016, 115, 1202–1217. [Google Scholar] [CrossRef] [PubMed]
- Levitan, E.B.; Ahmed, A.; Arnett, D.K.; Polak, J.F.; Hundley, W.G.; Bluemke, D.A.; Heckbert, S.R.; Jacobs, D.R., Jr.; Nettleton, J.A. Mediterranean diet score and left ventricular structure and function: The multi-ethnic study of atherosclerosis. Am. J. Clin. Nutr. 2016, 104, 595–602. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Luna, R.; Muñoz-Hernandez, R.; Miranda, M.L.; Costa, A.F.; Jimenez-Jimenez, L.; Vallejo-Vaz, A.J.; Muriana, F.J.; Villar, J.; Stiefel, P. Olive oil polyphenols decrease blood pressure and improve endothelial function in young women with mild hypertension. Am. J. Hypertens. 2012, 25, 1299–1304. [Google Scholar] [CrossRef] [PubMed]
- Cardeno, A.; Sanchez-Hidalgo, M.; Alarcon-de-la-Lastra, C. An Up-date of Olive Oil Phenols in Inflammation and Cancer: Molecular Mechanisms and Clinical Implications. Curr. Med. Chem. 2013, 20, 4758–4776. [Google Scholar] [CrossRef] [PubMed]
- Sacks, F.M.; Bray, G.A.; Carey, V.J.; Smith, S.R.; Ryan, D.H.; Anton, S.D.; McManus, K.; Champagne, C.M.; Bishop, L.M.; Laranjo, N.; et al. Comparison of weight-loss diets with different compositions of fat, protein and carbohydrates. N. Engl. J. Med. 2009, 360, 859–873. [Google Scholar] [CrossRef] [PubMed]
- Naude, C.E.; Schoonees, A.; Senekal, M.; Young, T.; Garner, P.; Volmink, J. Low carbohydrate versus isoenergetic balanced diets for reducing weight and cardiovascular risk: A systematic review and meta-analysis. PLoS ONE 2014, 9, e100652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bradley, U.; Spence, M.; Courtney, C.H.; McKinley, M.C.; Ennis, C.N.; McCance, D.R.; McEneny, J.; Bell, P.M.; Young, I.S.; Hunter, S.J. Low-fat versus low-carbohydrate weight reduction diets: Effects on weight loss, insulin resistance and cardiovascular risk: A randomized control trial. Diabetes 2009, 58, 2741–2748. [Google Scholar] [CrossRef] [PubMed]
- Browning, J.D.; Baker, J.A.; Rogers, T.; Davis, J.; Satapati, S.; Burgess, S.C. Short-term weight loss and hepatic triglyceride reduction: Evidence of a metabolic advantage with dietary carbohydrate restriction. Am. J. Clin. Nutr. 2011, 93, 1048–1052. [Google Scholar] [CrossRef] [PubMed]
- El Ghoch, M.; Calugi, S.; Dalle Grave, R. The Effects of Low-Carbohydrate Diets on Psychosocial Outcomes in Obesity/Overweight: A Systematic Review of Randomized, Controlled Studies. Nutrients 2016, 8, 402. [Google Scholar] [CrossRef] [PubMed]
- Hu, T.; Bazzano, L.A. The low-carbohydrate diet and cardiovascular risk factors: Evidence from epidemiologic studies. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 337–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paoli, A.; Rubini, A.; Volek, J.S.; Grimaldi, K.A. Beyond weight loss: A review of the therapeutic uses of very-low-carbohydrate (ketogenic) diets. Eur. J. Clin. Nutr. 2013, 67, 789–796. [Google Scholar] [CrossRef] [PubMed]
- Roul, G.; Moulichon, M.E.; Bareiss, P.; Gries, P.; Sacrez, J.; Germain, P.H.; Mossard, J.M.; Sacrez, A. Exercise peak VO2 determination in chronic heart failure: Is it still of value? Eur. Heart J. 1994, 15, 495–502. [Google Scholar] [CrossRef] [PubMed]

© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dos Reis Padilha, G.; Sanches Machado d’Almeida, K.; Ronchi Spillere, S.; Corrêa Souza, G. Dietary Patterns in Secondary Prevention of Heart Failure: A Systematic Review. Nutrients 2018, 10, 828. https://doi.org/10.3390/nu10070828
Dos Reis Padilha G, Sanches Machado d’Almeida K, Ronchi Spillere S, Corrêa Souza G. Dietary Patterns in Secondary Prevention of Heart Failure: A Systematic Review. Nutrients. 2018; 10(7):828. https://doi.org/10.3390/nu10070828
Chicago/Turabian StyleDos Reis Padilha, Gabriela, Karina Sanches Machado d’Almeida, Stefanny Ronchi Spillere, and Gabriela Corrêa Souza. 2018. "Dietary Patterns in Secondary Prevention of Heart Failure: A Systematic Review" Nutrients 10, no. 7: 828. https://doi.org/10.3390/nu10070828
APA StyleDos Reis Padilha, G., Sanches Machado d’Almeida, K., Ronchi Spillere, S., & Corrêa Souza, G. (2018). Dietary Patterns in Secondary Prevention of Heart Failure: A Systematic Review. Nutrients, 10(7), 828. https://doi.org/10.3390/nu10070828