Neurological Manifestations of Neuropathy and Ataxia in Celiac Disease: A Systematic Review

 , ,
, , 
Abstract
:1. Introduction
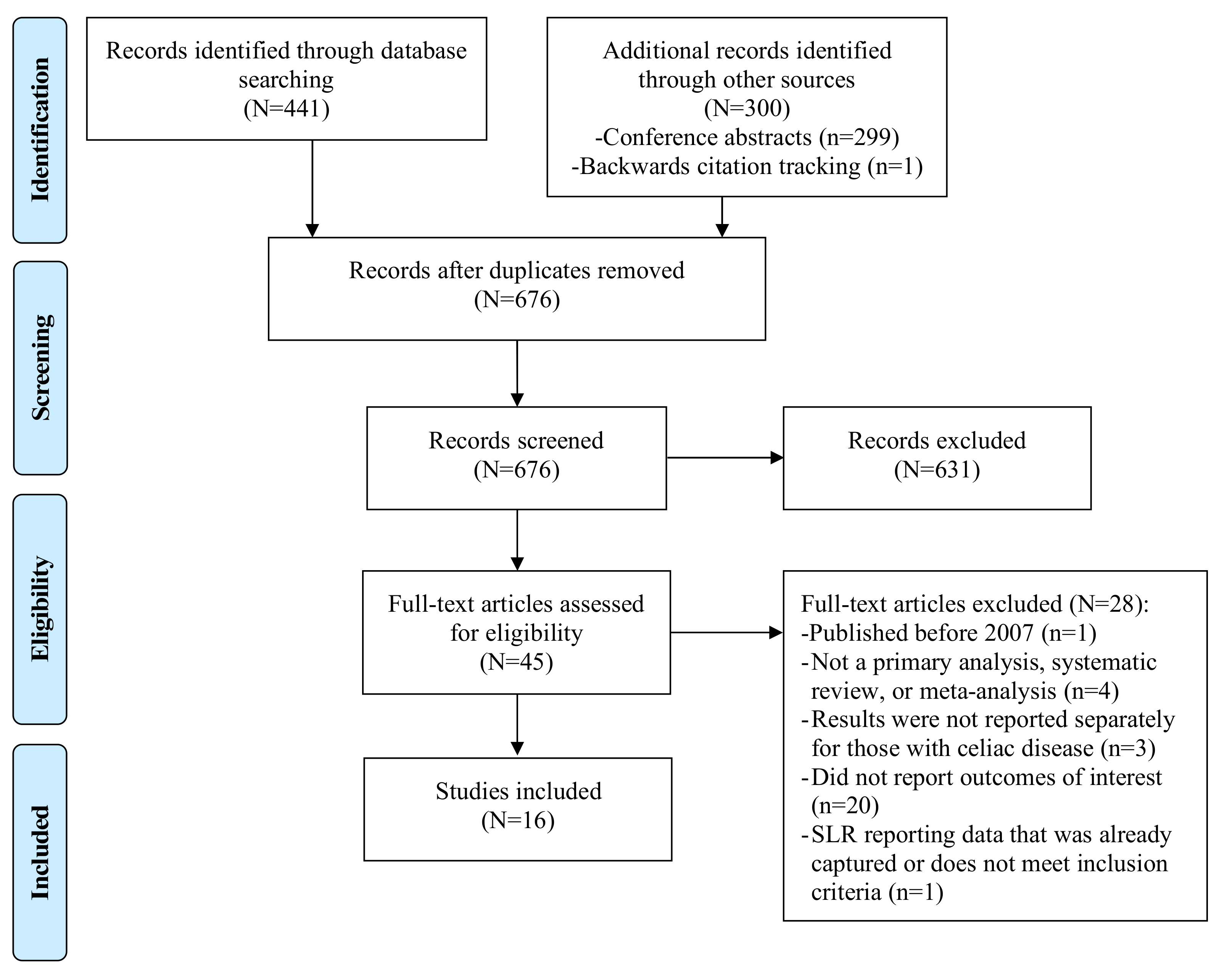
2. Materials and Methods
3. Results
3.1. Gluten Neuropathy
3.2. Gluten Ataxia
3.3. Quality Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rubio-Tapia, A.; Hill, I.D.; Kelly, C.P.; Calderwood, A.H.; Murray, J.A. ACG clinical guidelines: Diagnosis and management of celiac disease. Am. J. Gastroenterol. 2013, 108, 656–676. [Google Scholar] [CrossRef] [PubMed]
- Tonutti, E.; Bizzaro, N. Diagnosis and classification of celiac disease and gluten sensitivity. Autoimmun. Rev. 2014, 13, 472–476. [Google Scholar] [CrossRef]
- Ludvigsson, J.F.; Leffler, D.A.; Bai, J.C.; Biagi, F.; Fasano, A.; Green, P.H.; Hadjivassiliou, M.; Kaukinen, K.; Kelly, C.P.; Leonard, J.N.; et al. The Oslo definitions for coeliac disease and related terms. Gut 2013, 62, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Green, P.H.; Lebwohl, B.; Greywoode, R. Celiac disease. J. Allergy Clin. Immunol. 2015, 135, 1099–1106. [Google Scholar] [CrossRef] [PubMed]
- Reilly, N.R.; Green, P.H. Epidemiology and clinical presentations of celiac disease. Semin. Immunopathol. 2012, 34, 473–478. [Google Scholar] [CrossRef]
- Roma, E.; Panayiotou, J.; Karantana, H.; Constantinidou, C.; Siakavellas, S.I.; Krini, M.; Syriopoulou, V.P.; Bamias, G. Changing pattern in the clinical presentation of pediatric celiac disease: A 30-year study. Digestion 2009, 80, 185–191. [Google Scholar] [CrossRef]
- Ludvigsson, J.F.; Rubio-Tapia, A.; van Dyke, C.T.; Melton, L.J., 3rd; Zinsmeister, A.R.; Lahr, B.D.; Murray, J.A. Increasing incidence of celiac disease in a North American population. Am. J. Gastroenterol. 2013, 108, 818–824. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, V.; Kurppa, K.; Huhtala, H.; Collin, P.; Maki, M.; Kaukinen, K. Factors associated with long diagnostic delay in celiac disease. Scand. J. Gastroenterol. 2014, 49, 1304–1310. [Google Scholar] [CrossRef]
- Leffler, D.A.; Green, P.H.; Fasano, A. Extraintestinal manifestations of coeliac disease. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 561–571. [Google Scholar] [CrossRef] [PubMed]
- Hadjivassiliou, M.; Rao, D.G.; Grinewald, R.A.; Aeschlimann, D.P.; Sarrigiannis, P.G.; Hoggard, N.; Aeschlimann, P.; Mooney, P.D.; Sanders, D.S. Neurological Dysfunction in Coeliac Disease and Non-Coeliac Gluten Sensitivity. Am. J. Gastroenterol. 2016, 111, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Hadjivassiliou, M.; Sanders, D.S.; Grunewald, R.A.; Woodroofe, N.; Boscolo, S.; Aeschlimann, D. Gluten sensitivity: From gut to brain. Lancet Neurol. 2010, 9, 318–330. [Google Scholar] [CrossRef]
- Hadjivassiliou, M.; Kandler, R.H.; Chattopadhyay, A.K.; Davies-Jones, A.G.; Jarratt, J.A.; Sanders, D.S.; Sharrack, B.; Grunewald, R.A. Dietary treatment of gluten neuropathy. Muscle Nerve 2006, 34, 762–766. [Google Scholar] [CrossRef] [PubMed]
- Hadjivassiliou, M.; Williamson, C.A.; Woodroofe, N. The immunology of gluten sensitivity: Beyond the gut. Trends Immunol. 2004, 25, 578–582. [Google Scholar] [CrossRef] [PubMed]
- Rampertab, S.D.; Pooran, N.; Brar, P.; Singh, P.; Green, P.H. Trends in the presentation of celiac disease. Am. J. Med. 2006, 119, 355.e9–355.e14. [Google Scholar] [CrossRef] [PubMed]
- Green, P.H. The many faces of celiac disease: Clinical presentation of celiac disease in the adult population. Gastroenterology 2005, 128, S74–S78. [Google Scholar] [CrossRef] [PubMed]
- Lionetti, E.; Catassi, C. The role of environmental factors in the development of celiac disease: What is new? Diseases 2015, 3, 282–293. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Oxford Centre for Evidence-Based Medicine—Levels of Evidence. March 2009. Available online: http://www.cebm.net/blog/2009/06/11/oxford-centre-evidence-based-medicine-levels-evidence-march-2009/ (accessed on 16 January 2018).
- Briani, C.; Doria, A.; Ruggero, S.; Toffanin, E.; Luca, M.; Albergoni, M.P.; Odorico, A.D.; Grassivaro, F.; Lucchetta, M.; Lazzari, F.D.; et al. Antibodies to muscle and ganglionic acetylcholine receptors (AchR) in celiac disease. Autoimmunity 2008, 41, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Briani, C.; Zara, G.; Alaedini, A.; Grassivaro, F.; Ruggero, S.; Toffanin, E.; Albergoni, M.P.; Luca, M.; Giometto, B.; Ermani, M.; et al. Neurological complications of celiac disease and autoimmune mechanisms: A prospective study. J. Neuroimmunol. 2008, 195, 171–175. [Google Scholar] [CrossRef]
- Burk, K.; Farecki, M.L.; Lamprecht, G.; Roth, G.; Decker, P.; Weller, M.; Rammensee, H.G.; Oertel, W. Neurological symptoms in patients with biopsy proven celiac disease. Mov. Disord. 2009, 24, 2358–2362. [Google Scholar] [CrossRef]
- Cakir, D.; Tosun, A.; Polat, M.; Celebisoy, N.; Gokben, S.; Aydogdu, S.; Yagci, R.V.; Tekgul, H. Subclinical neurological abnormalities in children with celiac disease receiving a gluten-free diet. J. Pediatr. Gastroenterol. Nutr. 2007, 45, 366–369. [Google Scholar] [CrossRef]
- Diaconu, G.; Burlea, M.; Grigore, I.; Anton, D.T.; Trandafir, L.M. Celiac disease with neurologic manifestations in children. Revista Medico-Chirurgicala A Societatii de Medici si Naturalisti din Iasi 2014, 117, 88–94. [Google Scholar]
- Isikay, S.; Isikay, N.; Kocamaz, H.; Hizli, S. Peripheral neuropathy electrophysiological screening in children with celiac disease. Arq. Gastroenterol. 2015, 52, 134–138. [Google Scholar] [CrossRef]
- Jericho, H.; Sansotta, N.; Guandalini, S. Extraintestinal Manifestations of Celiac Disease: Effectiveness of the Gluten-Free Diet. J. Pediatr. Gastroenterol. Nutr. 2017, 65, 75–79. [Google Scholar] [CrossRef]
- Ludvigsson, J.F.; Olsson, T.; Ekbom, A.; Montgomery, S.M. A population-based study of coeliac disease, neurodegenerative and neuroinflammatory diseases. Aliment. Pharmacol. Ther. 2007, 25, 1317–1327. [Google Scholar] [CrossRef]
- Mukherjee, R.; Egbuna, I.; Brar, P.; Hernandez, L.; McMahon, D.J.; Shane, E.J.; Bhagat, G.; Green, P.H. Celiac disease: Similar presentations in the elderly and young adults. Dig. Dis. Sci. 2010, 55, 3147–3153. [Google Scholar] [CrossRef]
- Ruggieri, M.; Incorpora, G.; Polizzi, A.; Parano, E.; Spina, M.; Pavone, P. Low prevalence of neurologic and psychiatric manifestations in children with gluten sensitivity. J. Pediatr. 2008, 152, 244–249. [Google Scholar] [CrossRef]
- Shen, T.C.; Lebwohl, B.; Verma, H.; Kumta, N.; Tennyson, C.; Lewis, S.; Scherl, E.; Swaminath, A.; Capiak, K.M.; DiGiacomo, D.; et al. Peripheral neuropathic symptoms in celiac disease and inflammatory bowel disease. J. Clin. Neuromuscul. Dis. 2012, 13, 137–145. [Google Scholar] [CrossRef]
- Thawani, S.P.; Brannagan, T.H., 3rd; Lebwohl, B.; Green, P.H.; Ludvigsson, J.F. Risk of Neuropathy Among 28,232 Patients with Biopsy-Verified Celiac Disease. JAMA Neurol. 2015, 72, 806–811. [Google Scholar] [CrossRef]
- Hadjivassiliou, M.; Grunewald, R.A.; Sanders, D.S.; Shanmugarajah, P.; Hoggard, N. Effect of gluten-free diet on cerebellar MR spectroscopy in gluten ataxia. Neurology 2017, 89, 705–709. [Google Scholar] [CrossRef]
- Sangal, K.; Camhi, S.; Lima, R.; Kenyon, V.; Fasano, A.; Leonard, M. Prevalence of neurological symptoms in children with gluten related disorders. J. Pediatr. Gastroenterol. Nutr. 2017, 65, S328–S329. [Google Scholar] [CrossRef]
- Thawani, S.; Brannagan, T.H., 3rd; Lebwohl, B.; Mollazadegan, K.; Green, P.H.R.; Ludvigsson, J.F. Type 1 Diabetes, Celiac Disease, and Neuropathy-A Nationwide Cohort Study. J. Clin. Neuromuscul. Dis. 2017, 19, 12–18. [Google Scholar] [CrossRef]
- Hanewinckel, R.; Drenthen, J.; van Oijen, M.; Hofman, A.; van Doorn, P.A.; Ikram, M.A. Prevalence of polyneuropathy in the general middle-aged and elderly population. Neurology 2016, 87, 1892–1898. [Google Scholar] [CrossRef]
- Chin, R.L.; Sander, H.W.; Brannagan, T.H.; Green, P.H.; Hays, A.P.; Alaedini, A.; Latov, N. Celiac neuropathy. Neurology 2003, 60, 1581–1585. [Google Scholar] [CrossRef]
- Luostarinen, L.; Himanen, S.L.; Luostarinen, M.; Collin, P.; Pirttila, T. Neuromuscular and sensory disturbances in patients with well treated coeliac disease. J. Neurol. Neurosurg. Psychiatry 2003, 74, 490–494. [Google Scholar] [CrossRef]
- Muzaimi, M.B.; Thomas, J.; Palmer-Smith, S.; Rosser, L.; Harper, P.S.; Wiles, C.M.; Ravine, D.; Robertson, N.P. Population based study of late onset cerebellar ataxia in south east Wales. J. Neurol. Neurosurg. Psychiatry 2004, 75, 1129–1134. [Google Scholar] [CrossRef]
- Hadjivassiliou, M. Immune-mediated acquired ataxias. Handb. Clin. Neurol. 2012, 103, 189–199. [Google Scholar] [CrossRef]
- Hadjivassiliou, M.; Boscolo, S.; Tongiorgi, E.; Grunewald, R.A.; Sharrack, B.; Sanders, D.S.; Woodroofe, N.; Davies-Jones, G.A. Cerebellar ataxia as a possible organ-specific autoimmune disease. Mov. Disord. 2008, 23, 1370–1377. [Google Scholar] [CrossRef]
- Abele, M.; Burk, K.; Schols, L.; Schwartz, S.; Besenthal, I.; Dichgans, J.; Zuhlke, C.; Riess, O.; Klockgether, T. The aetiology of sporadic adult-onset ataxia. Brain 2002, 125, 961–968. [Google Scholar] [CrossRef]
- Abele, M.; Schols, L.; Schwartz, S.; Klockgether, T. Prevalence of antigliadin antibodies in ataxia patients. Neurology 2003, 60, 1674–1675. [Google Scholar] [CrossRef]
- Burk, K.; Bosch, S.; Muller, C.A.; Melms, A.; Zuhlke, C.; Stern, M.; Besenthal, I.; Skalej, M.; Ruck, P.; Ferber, S.; et al. Sporadic cerebellar ataxia associated with gluten sensitivity. Brain 2001, 124, 1013–1019. [Google Scholar] [CrossRef]
- Bushara, K.O.; Goebel, S.U.; Shill, H.; Goldfarb, L.G.; Hallett, M. Gluten sensitivity in sporadic and hereditary cerebellar ataxia. Ann. Neurol. 2001, 49, 540–543. [Google Scholar] [CrossRef]
- Hadjivassiliou, M.; Grunewald, R.; Sharrack, B.; Sanders, D.; Lobo, A.; Williamson, C.; Woodroofe, N.; Wood, N.; Davies-Jones, A. Gluten ataxia in perspective: Epidemiology, genetic susceptibility and clinical characteristics. Brain 2003, 126, 685–691. [Google Scholar] [CrossRef]
- Ihara, M.; Makino, F.; Sawada, H.; Mezaki, T.; Mizutani, K.; Nakase, H.; Matsui, M.; Tomimoto, H.; Shimohama, S. Gluten sensitivity in Japanese patients with adult-onset cerebellar ataxia. Intern. Med. 2006, 45, 135–140. [Google Scholar] [CrossRef]
- Luostarinen, L.K.; Collin, P.O.; Peraaho, M.J.; Maki, M.J.; Pirttila, T.A. Coeliac disease in patients with cerebellar ataxia of unknown origin. Ann. Med. 2001, 33, 445–449. [Google Scholar] [CrossRef]
- Pellecchia, M.T.; Scala, R.; Filla, A.; De Michele, G.; Ciacci, C.; Barone, P. Idiopathic cerebellar ataxia associated with celiac disease: Lack of distinctive neurological features. J. Neurol. Neurosurg. Psychiatry 1999, 66, 32–35. [Google Scholar] [CrossRef]
- Anheim, M.; Degos, B.; Echaniz-Laguna, A.; Fleury, M.; Grucker, M.; Tranchant, C. Ataxia associated with gluten sensitivity, myth or reality? Rev. Neurol. 2006, 162, 214–221. [Google Scholar] [CrossRef]
- Hadjivassiliou, M.; Grünewald, R.; Sanders, D.; Zis, P.; Croall, I.; Shanmugarajah, P.; Sarrigiannis, P.; Trott, N.; Wild, G.; Hoggard, N. The Significance of Low Titre Antigliadin Antibodies in the Diagnosis of Gluten Ataxia. Nutrients 2018, 10, 1444. [Google Scholar] [CrossRef]
- Hadjivassiliou, M.; Grunewald, R.A.; Kandler, R.H.; Chattopadhyay, A.K.; Jarratt, J.A.; Sanders, D.S.; Sharrack, B.; Wharton, S.B.; Davies-Jones, G.A. Neuropathy associated with gluten sensitivity. J. Neurol. Neurosurg. Psychiatry 2006, 77, 1262–1266. [Google Scholar] [CrossRef]
- Zis, P.; Sarrigiannis, P.G.; Rao, D.G.; Hadjivassiliou, M. Gluten neuropathy: Prevalence of neuropathic pain and the role of gluten-free diet. J. Neurol. 2018, 265, 2231–2236. [Google Scholar] [CrossRef]
- Vinagre-Aragon, A.; Zis, P.; Grunewald, R.A.; Hadjivassiliou, M. Movement Disorders Related to Gluten Sensitivity: A Systematic Review. Nutrients 2018, 10, 34. [Google Scholar] [CrossRef]
- Hadjivassiliou, M.; Gibson, A.; Davies-Jones, G.A.; Lobo, A.J.; Stephenson, T.J.; Milford-Ward, A. Does cryptic gluten sensitivity play a part in neurological illness? Lancet 1996, 347, 369–371. [Google Scholar] [CrossRef]


{kind=link}
| Search No. | Search Terms | Search Results (28 August 2018) |
|---|---|---|
| 1 | celiac*[tiab] OR coeliac*[tiab] OR celiac disease[MeSH] | 31,137 |
| 2 | ((coeliac OR celiac) AND (trunk* OR axis OR node*)) OR “coeliac artery” OR “celiac artery” | 7348 |
| 3 | #1 NOT #2 | 25,521 |
| 4 | (cerebellar ataxia[MeSH] OR “cerebellar ataxia”[tiab] OR ((cerebellum* OR cerebellar) AND ataxi*) OR “gluten ataxia” OR “gluten-sensitive ataxia”) | 17,238 |
| 5 | neuropathy[tiab] OR neuropathies[tiab] OR neuropathic[tiab] | 88,749 |
| 6 | #3 AND #4 | 141 |
| 7 | #3 AND #5 | 213 |
| 8 | #6 OR #7 | 309 |
| 9 | case reports[pt] | 1,893,340 |
| 10 | #8 NOT #9 | 238 |
| 11 | mice OR mouse OR murine OR rodent* | 1,754,334 |
| 12 | #10 NOT #11 | 227 |
| 13 | review[pt] NOT (systematic OR Cochrane OR meta-analy*) | 2,162,485 |
| 14 | #12 NOT #13 | 160 |
| 15 | #14; Filter: published 2007 or later | 99 |
| 16 | #15; Filter: abstract | 96 |
| Level | Differential Diagnosis/Symptom Prevalence Study |
| 1a | Systematic review (with homogeneity) of prospective cohort studies |
| 1b | Prospective cohort study with good follow-up |
| 1c | All or none case-series |
| 2a | Systematic review (with homogeneity) of 2b and better studies |
| 2b | Retrospective cohort study, or poor follow-up |
| 2c | Ecological studies |
| 3a | Systematic review (with homogeneity) of 3b and better studies |
| 3b | Non-consecutive cohort study, or very limited population |
| 4 | Case-series or superseded reference standards |
| 5 | Expert opinion without explicit critical appraisal, or based on physiology, bench research or “first principles” |
| Grade | Levels of Individual Studies |
| A | Consistent level 1 studies |
| B | Consistent level 2 or 3 studies or extrapolations from level 1 studies |
| C | Level 4 studies or extrapolations from level 2 or 3 studies |
| D | Level 5 evidence or troublingly inconsistent or inconclusive studies of any level |
| Author (year) | Study Design | Country | Population | Neurological Complication |
|---|---|---|---|---|
| Briani and Doria et al. (2008) [19] | Prospective, single-center, cross-sectional | Italy | Patients with CD | Neuropathy |
| Briani and Zara et al. (2008) [20] | Prospective, single-center, cross-sectional | Italy | Unselected, consecutive patients with CD treated at the University of Padova | Ataxia, neuropathy |
| Burk et al. (2013) [21] | Prospective, single-center, cross-sectional | Germany | Patients with CD on a GFD recruited from advertisements in the official journal of the German Celiac Society or personal contact | Ataxia |
| Cakir et al. (2007)[22] | Prospective, multi-center, cross-sectional | Turkey | Children with CD treated at the outpatient follow-up program of celiac patients in the pediatric gastroenterology and nutrition division of Ege University Hospital from 1998–2002 | Ataxia, neuropathy |
| Diaconu et al. (2013) [23] | Prospective, single-center, cross-sectional | Romania | Children (2–18 years) diagnosed with CD from 2000–2010 | Ataxia |
| Hadjivassiliou et al. (2016) [10] | Retrospective, single-center, cohort | UK | Patients with CD and neurological manifestations presenting to the Neuroscience Department at Royal Hallamshire Hospital from 1994–2014 | Ataxia, neuropathy |
| Hadjivassiliou et al. (2017) [31] | Prospective, single-center, observational case series | UK | Patients diagnosed with gluten ataxia at the Sheffield Ataxia Centre | Ataxia |
| Isikay et al. (2015) [24] | Prospective, single-center, cross-sectional, case-control | Turkey | Asymptomatic children with CD diagnosed at a pediatric gastroenterology outpatient clinic from September 2012–August 2014 | Ataxia, neuropathy |
| Jericho et al. (2017) [25] | Retrospective, single-center, chart review | US | Patients with CD registered at the University of Chicago Celiac Center clinic from January 2002–October 2014 | Ataxia, neuropathy |
| Ludvigsson et al. (2007) [26] | Retrospective, multi-center, database | Sweden | Patients in the Swedish national inpatient register with a hospital-based discharge diagnosis of CD from 1964–2003 | Ataxia, neuropathy |
| Mukherjee et al. (2010) [27] | Retrospective, single-center, database | US | Patients with CD from a prospectively generated database at a university-based referral center | Neuropathy |
| Ruggieri et al. (2008) [28] | Prospective, single-center, cross-sectional | Italy | Children with CD and neurological dysfunction evaluated at the gluten sensitivity clinic at the Department of Pediatrics at the University of Catania from January 1991–December 2004 | Ataxia, neuropathy |
| Sangal et al. (2017) [32] | Retrospective, single-center, medical record review | Not reported | Children with and without gluten-related disorders between July 2013 and May 2016 | Ataxia, neuropathy |
| Shen et al. (2012) [29] | Questionnaire-based, multi-center, cross-sectional, case-control | US | Patients with CD recruited from the Celiac Disease Center at Columbia University and support groups in New York and California | Neuropathy |
| Thawani et al. (2015) [30] | Retrospective, multi-center | Sweden | Patients with CD from one of Sweden’s pathology departments from June 1969–February 2008 | Neuropathy |
| Thawani et al. (2017) [33] | Retrospective, nationwide registry | Sweden | Patients diagnosed with T1DM between 1964 and 2009, with and without CD (based on biopsies between 1969 and 2008) in the Swedish National Patient Register | Neuropathy |
| Study Identifier | Oxford Level of Evidence |
|---|---|
| Briani and Doria et al. (2008) [19] | 2c. Ecological study * |
| Briani and Zara et al. (2008) [20] | 1b. Prospective cohort study |
| Burk et al. (2013) [21] | 2c. Ecological study * |
| Cakir et al. (2007) [22] | 2c. Ecological study * |
| Diaconu et al. (2013) [23] | 2c. Ecological study * |
| Hadjivassiliou et al. (2016) [10] | 2b. Retrospective cohort study |
| Hadjivassiliou et al. (2017) [31] | 4. Case-series or superseded reference standards |
| Isikay et al. (2015) [24] | 2c. Ecological study * |
| Jericho et al. (2017) [25] | 2b. Retrospective cohort study |
| Ludvigsson et al. (2007) [26] | 2b. Retrospective cohort study |
| Mukherjee et al. (2010) [27] | 2b. Retrospective cohort study |
| Ruggieri et al. (2008) [28] | 2c. Ecological study * |
| Sangal et al. (2017) [32] | 2b. Retrospective cohort study |
| Shen et al. (2012) [29] | 2c. Ecological study * |
| Thawani et al. (2015) [30] | 2b. Retrospective cohort study |
| Thawani et al. (2017) [33] | 2b. Retrospective cohort study |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mearns, E.S.; Taylor, A.; Thomas Craig, K.J.; Puglielli, S.; Cichewicz, A.B.; Leffler, D.A.; Sanders, D.S.; Lebwohl, B.; Hadjivassiliou, M. Neurological Manifestations of Neuropathy and Ataxia in Celiac Disease: A Systematic Review. Nutrients 2019, 11, 380. https://doi.org/10.3390/nu11020380
Mearns ES, Taylor A, Thomas Craig KJ, Puglielli S, Cichewicz AB, Leffler DA, Sanders DS, Lebwohl B, Hadjivassiliou M. Neurological Manifestations of Neuropathy and Ataxia in Celiac Disease: A Systematic Review. Nutrients. 2019; 11(2):380. https://doi.org/10.3390/nu11020380
Chicago/Turabian StyleMearns, Elizabeth S., Aliki Taylor, Kelly J. Thomas Craig, Stefanie Puglielli, Allie B. Cichewicz, Daniel A. Leffler, David S. Sanders, Benjamin Lebwohl, and Marios Hadjivassiliou. 2019. "Neurological Manifestations of Neuropathy and Ataxia in Celiac Disease: A Systematic Review" Nutrients 11, no. 2: 380. https://doi.org/10.3390/nu11020380
APA StyleMearns, E. S., Taylor, A., Thomas Craig, K. J., Puglielli, S., Cichewicz, A. B., Leffler, D. A., Sanders, D. S., Lebwohl, B., & Hadjivassiliou, M. (2019). Neurological Manifestations of Neuropathy and Ataxia in Celiac Disease: A Systematic Review. Nutrients, 11(2), 380. https://doi.org/10.3390/nu11020380