
Efficacy of Individualized Sensory-Based mHealth Interventions to Improve Distress Coping in Healthcare Professionals: A Multi-Arm Parallel-Group Randomized Controlled Trial

Abstract
:1. Introduction
- Scientifically validate a sensor-based mHealth intervention for distress coping in the healthcare setting.
- Compare the efficacy of different individualization levels of mHealth interventions by a multi-arm study design.
- Combine components of physical activity and relaxation techniques in an mHealth application using a multimodal intervention approach to improve distress coping among healthcare professionals.
- Measure multiple clinically relevant stress and physical activity-related outcomes during the intervention and adapt the content of the intervention based on these measures.
- Enable unrestricted implementation within the daily work routine of healthcare professionals by means of a mobile and low-threshold intervention.
2. Materials and Methods
2.1. Trial Design
2.2. Participants
2.3. Interventions
2.4. Outcomes
3. Results
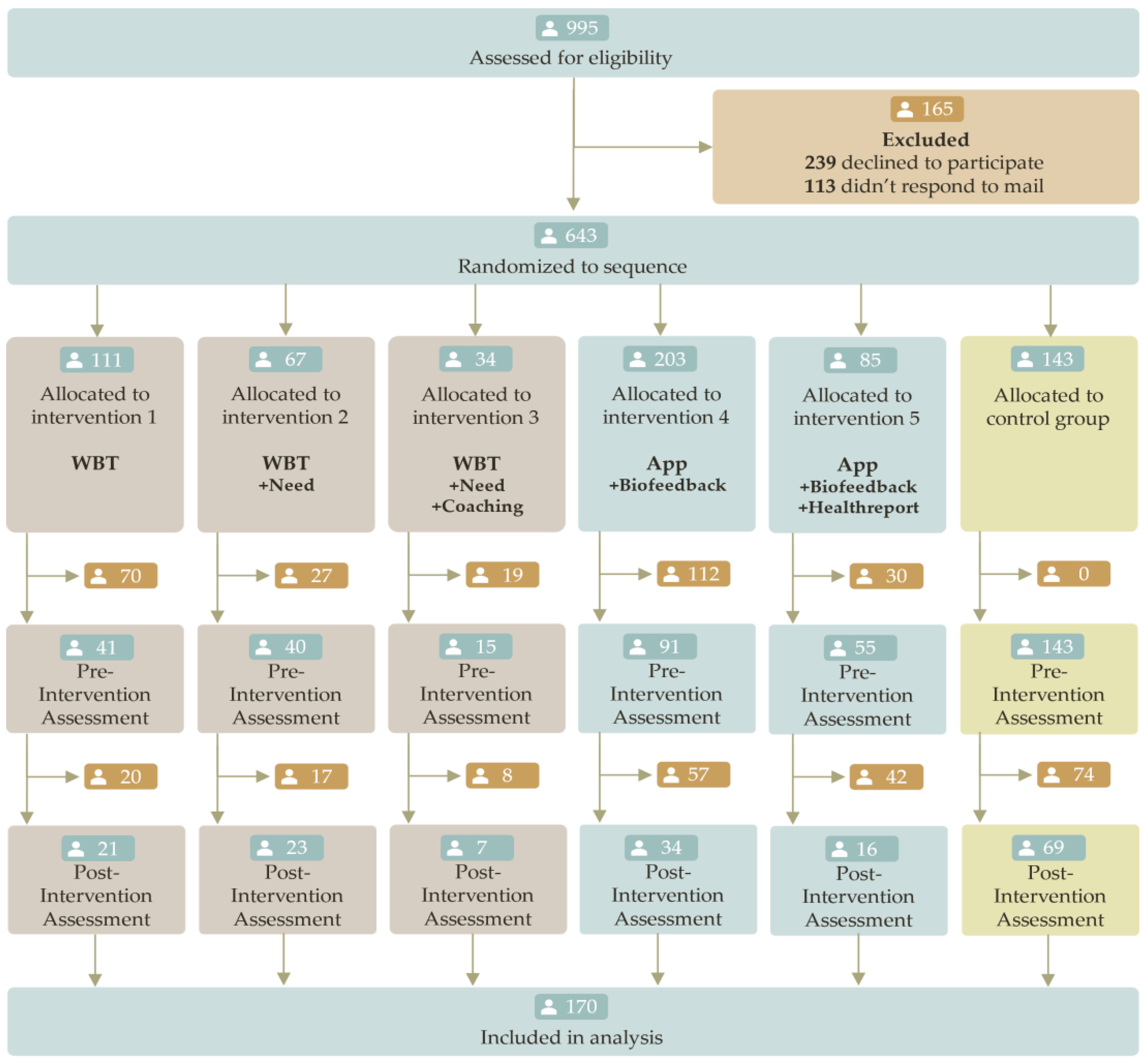
3.1. Flow-Chart
3.2. Baseline Data and Main Analysis
4. Discussion
4.1. Strengths and Limitations
4.2. Future Research
4.3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dragano, N. Arbeitsstress als Risikofaktor für kardiovaskuläre Erkrankungen. Aktuelle Kardiol. 2018, 7, 368–372. [Google Scholar] [CrossRef]
- Järvelin-Pasanen, S.; Sinikallio, S.; Tarvainen, M.P. Heart rate variability and occupational stress-systematic review. Ind. Health 2018, 56, 500–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, J.; Bogossian, F.; Ahern, K. Stress and coping in Australian nurses: A systematic review. Int. Nurs. Rev. 2010, 57, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Halpin, Y.; Terry, L.M.; Curzio, J. A longitudinal, mixed methods investigation of newly qualified nurses’ workplace stressors and stress experiences during transition. J. Adv. Nurs. 2017, 73, 2577–2586. [Google Scholar] [CrossRef] [PubMed]
- Couarraze, S.; Delamarre, L.; Marhar, F.; Quach, B.; Jiao, J.; Avilés Dorlhiac, R.; Saadaoui, F.; Liu, A.S.-I.; Dubuis, B.; Antunes, S.; et al. The major worldwide stress of healthcare professionals during the first wave of the COVID-19 pandemic—The international COVISTRESS survey. PLoS ONE 2021, 16, e0257840. [Google Scholar] [CrossRef] [PubMed]
- Hasselhorn, H.M.; Conway, P.M.; Widerszal-Bazyl, M.; Simon, M.; Tackenberg, P.; Schmidt, S.; Camerino, D.; Müller, B.H.; NEXT study group. Contribution of job strain to nurses’ consideration of leaving the profession—Results from the longitudinal European nurses’ early exit study. Scand. J. Work. Environ. Health 2008, 34, 75–82. [Google Scholar]
- Heinen, M.M.; van Achterberg, T.; Schwendimann, R.; Zander, B.; Matthews, A.; Kózka, M.; Ensio, A.; Sjetne, I.S.; Moreno Casbas, T.; Ball, J.; et al. Nurses’ intention to leave their profession: A cross sectional observational study in 10 European countries. Int. J. Nurs. Stud. 2013, 50, 174–184. [Google Scholar] [CrossRef] [PubMed]
- Schwinger, A.; Klauber, J.; Kuhlmey, A.; Jacobs, K.; Greß, S. Pflege-Report 2019; Springer Nature: Erscheinungsort nicht ermittelbar, Germany, 2020; ISBN 9783662589342. [Google Scholar]
- McVicar, A. Workplace stress in nursing: A literature review. J. Adv. Nurs. 2003, 44, 633–642. [Google Scholar] [CrossRef]
- Moustaka, Ε.; Constantinidis, T. Sources and effects of Work-related stress in nursing. Health Sci. J. 2010, 4, 210–2016. [Google Scholar]
- Stults-Kolehmainen, M.A.; Sinha, R. The effects of stress on physical activity and exercise. Sport. Med. 2014, 44, 81–121. [Google Scholar] [CrossRef] [Green Version]
- van Schalkwijk, F.J.; Blessinga, A.N.; Willemen, A.M.; van der Werf, Y.D.; Schuengel, C. Social support moderates the effects of stress on sleep in adolescents. J. Sleep Res. 2015, 24, 407–413. [Google Scholar] [CrossRef] [Green Version]
- Schneider, D.; Winter, V.; Schreyögg, J. Job demands, job resources, and behavior in times of sickness: An analysis across German nursing homes. Health Care Manag. Rev. 2018, 43, 338–347. [Google Scholar] [CrossRef] [PubMed]
- Gu, B.; Tan, Q.; Zhao, S. The association between occupational stress and psychosomatic wellbeing among Chinese nurses: A cross-sectional survey. Medicine 2019, 98, e15836. [Google Scholar] [CrossRef]
- Dong, H.; Zhang, Q.; Sun, Z.; Sang, F.; Xu, Y. Sleep disturbances among Chinese clinical nurses in general hospitals and its influencing factors. BMC Psychiatry 2017, 17, 241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richardson, S.; Shaffer, J.A.; Falzon, L.; Krupka, D.; Davidson, K.W.; Edmondson, D. Meta-analysis of perceived stress and its association with incident coronary heart disease. Am. J. Cardiol. 2012, 110, 1711–1716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yaribeygi, H.; Panahi, Y.; Sahraei, H.; Johnston, T.P.; Sahebkar, A. The impact of stress on body function: A review. EXCLI J. 2017, 16, 1057–1072. [Google Scholar] [CrossRef] [PubMed]
- Clark, M.M.; Warren, B.A.; Hagen, P.T.; Johnson, B.D.; Jenkins, S.M.; Werneburg, B.L.; Olsen, K.D. Stress level, health behaviors, and quality of life in employees joining a wellness center. Am. J. Health Promot. 2011, 26, 21–25. [Google Scholar] [CrossRef]
- Rabbani, M.; Haque, M.M.; Das Dipal, D.; Zarif, M.I.I.; Iqbal, A.; Akhter, S.; Parveen, S.; Rasel, M.; Soron, T.R.; Bansal, N.; et al. A Mobile Health Application for Monitoring Children with Autism Spectrum Disorder. In AI Applications for Disease Diagnosis and Treatment; El Ouazzani, R., Fattah, M., Benamar, N., Eds.; IGI Global: Hershey, PA, USA, 2022; pp. 40–65. ISBN 9781668423042. [Google Scholar]
- Vrijkotte, T.G.; van Doornen, L.J.; de Geus, E.J. Effects of work stress on ambulatory blood pressure, heart rate, and heart rate variability. Hypertension 2000, 35, 880–886. [Google Scholar] [CrossRef]
- Borchini, R.; Veronesi, G.; Bonzini, M.; Gianfagna, F.; Dashi, O.; Ferrario, M.M. Heart Rate Variability Frequency Domain Alterations among Healthy Nurses Exposed to Prolonged Work Stress. Int. J. Environ. Res. Public Health 2018, 15, 113. [Google Scholar] [CrossRef] [Green Version]
- Chandola, T.; Britton, A.; Brunner, E.; Hemingway, H.; Malik, M.; Kumari, M.; Badrick, E.; Kivimaki, M.; Marmot, M. Work stress and coronary heart disease: What are the mechanisms? Eur. Heart J. 2008, 29, 640–648. [Google Scholar] [CrossRef] [Green Version]
- da Estrela, C.; McGrath, J.; Booij, L.; Gouin, J.-P. Heart Rate Variability, Sleep Quality, and Depression in the Context of Chronic Stress. Ann. Behav. Med. 2021, 55, 155–164. [Google Scholar] [CrossRef]
- Kim, H.-G.; Cheon, E.-J.; Bai, D.-S.; Lee, Y.H.; Koo, B.-H. Stress and Heart Rate Variability: A Meta-Analysis and Review of the Literature. Psychiatry Investig. 2018, 15, 235–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delaney, J.P.; Brodie, D.A. Effects of short-term psychological stress on the time and frequency domains of heart-rate variability. Percept. Mot. Skills 2000, 91, 515–524. [Google Scholar] [CrossRef]
- Filaire, E.; Portier, H.; Massart, A.; Ramat, L.; Teixeira, A. Effect of lecturing to 200 students on heart rate variability and alpha-amylase activity. Eur. J. Appl. Physiol. 2010, 108, 1035–1043. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.G.; Koh, S.B.; Cha, B.S.; Park, J.K.; Woo, J.M.; Chang, S.J. Association between job stress on heart rate variability and metabolic syndrome in shipyard male workers. Yonsei Med. J. 2004, 45, 838–846. [Google Scholar] [CrossRef] [Green Version]
- Uusitalo, A.; Mets, T.; Martinmäki, K.; Mauno, S.; Kinnunen, U.; Rusko, H. Heart rate variability related to effort at work. Appl. Ergon. 2011, 42, 830–838. [Google Scholar] [CrossRef]
- Antelmi, I.; de Paula, R.S.; Shinzato, A.R.; Peres, C.A.; Mansur, A.J.; Grupi, C.J. Influence of age, gender, body mass index, and functional capacity on heart rate variability in a cohort of subjects without heart disease. Am. J. Cardiol. 2004, 93, 381–385. [Google Scholar] [CrossRef] [PubMed]
- Voss, A.; Schroeder, R.; Heitmann, A.; Peters, A.; Perz, S. Short-term heart rate variability—Influence of gender and age in healthy subjects. PLoS ONE 2015, 10, e0118308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molfino, A.; Fiorentini, A.; Tubani, L.; Martuscelli, M.; Rossi Fanelli, F.; Laviano, A. Body mass index is related to autonomic nervous system activity as measured by heart rate variability. Eur. J. Clin. Nutr. 2009, 63, 1263–1265. [Google Scholar] [CrossRef] [Green Version]
- Felber Dietrich, D.; Schindler, C.; Schwartz, J.; Barthélémy, J.-C.; Tschopp, J.-M.; Roche, F.; von Eckardstein, A.; Brändli, O.; Leuenberger, P.; Gold, D.R.; et al. Heart rate variability in an ageing population and its association with lifestyle and cardiovascular risk factors: Results of the SAPALDIA study. Europace 2006, 8, 521–529. [Google Scholar] [CrossRef]
- Yi, S.H.; Lee, K.; Shin, D.-G.; Kim, J.S.; Kim, H.-C. Differential association of adiposity measures with heart rate variability measures in Koreans. Yonsei Med. J. 2013, 54, 55–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tonello, L.; Rodrigues, F.B.; Souza, J.W.S.; Campbell, C.S.G.; Leicht, A.S.; Boullosa, D.A. The role of physical activity and heart rate variability for the control of work-related stress. Front. Physiol. 2014, 5, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bakker, A.B.; de Vries, J.D. Job Demands-Resources theory and self-regulation: New explanations and remedies for job burnout. Anxiety Stress Coping 2021, 34, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Yu, F.; Raphael, D.; Mackay, L.; Smith, M.; King, A. Personal and work-related factors associated with nurse resilience: A systematic review. Int. J. Nurs. Stud. 2019, 93, 129–140. [Google Scholar] [CrossRef] [PubMed]
- Thun, S.; Bakker, A.B. Empowering leadership and job crafting: The role of employee optimism. Stress Health 2018, 34, 573–581. [Google Scholar] [CrossRef] [PubMed]
- Broetje, S.; Jenny, G.J.; Bauer, G.F. The Key Job Demands and Resources of Nursing Staff: An Integrative Review of Reviews. Front. Psychol. 2020, 11, 84. [Google Scholar] [CrossRef]
- Chiou, S.-T.; Chiang, J.-H.; Huang, N.; Chien, L.-Y. Health behaviors and participation in health promotion activities among hospital staff: Which occupational group performs better? BMC Health Serv. Res. 2014, 14, 474. [Google Scholar] [CrossRef]
- Gerber, M.; Pühse, U. Review article: Do exercise and fitness protect against stress-induced health complaints? A review of the literature. Scand. J. Public Health 2009, 37, 801–819. [Google Scholar] [CrossRef]
- Khoury, B.; Sharma, M.; Rush, S.E.; Fournier, C. Mindfulness-based stress reduction for healthy individuals: A meta-analysis. J. Psychosom. Res. 2015, 78, 519–528. [Google Scholar] [CrossRef]
- Caldwell, K.; Harrison, M.; Adams, M.; Quin, R.H.; Greeson, J. Developing mindfulness in college students through movement-based courses: Effects on self-regulatory self-efficacy, mood, stress, and sleep quality. J Am. Coll. Health 2010, 58, 433–442. [Google Scholar] [CrossRef] [Green Version]
- Edwards, K.M.; Wilson, K.L.; Sadja, J.; Ziegler, M.G.; Mills, P.J. Effects on blood pressure and autonomic nervous system function of a 12-week exercise or exercise plus DASH-diet intervention in individuals with elevated blood pressure. Acta Physiol. 2011, 203, 343–350. [Google Scholar] [CrossRef] [Green Version]
- Chan, C.B.; Ryan, D.A.J.; Tudor-Locke, C. Health benefits of a pedometer-based physical activity intervention in sedentary workers. Prev. Med. 2004, 39, 1215–1222. [Google Scholar] [CrossRef]
- Tucker, S.; Farrington, M.; Lanningham-Foster, L.M.; Clark, M.K.; Dawson, C.; Quinn, G.J.; Laffoon, T.; Perkhounkova, Y. Worksite Physical Activity Intervention for Ambulatory Clinic Nursing Staff. Workplace Health Saf. 2016, 64, 313–325. [Google Scholar] [CrossRef] [PubMed]
- Rebar, A.L.; Stanton, R.; Geard, D.; Short, C.; Duncan, M.J.; Vandelanotte, C. A meta-meta-analysis of the effect of physical activity on depression and anxiety in non-clinical adult populations. Health Psychol. Rev. 2015, 9, 366–378. [Google Scholar] [CrossRef] [PubMed]
- Bischoff, L.L.; Otto, A.-K.; Hold, C.; Wollesen, B. The effect of physical activity interventions on occupational stress for health personnel: A systematic review. Int. J. Nurs. Stud. 2019, 97, 94–104. [Google Scholar] [CrossRef] [PubMed]
- Kulur, A.B.; Haleagrahara, N.; Adhikary, P.; Jeganathan, P.S. Effect of diaphragmatic breathing on heart rate variability in ischemic heart disease with diabetes. Arq. Bras. Cardiol. 2009, 92, 423–429, 440–447, 457–463. [Google Scholar] [CrossRef] [Green Version]
- Charalambous, A.; Giannakopoulou, M.; Bozas, E.; Paikousis, L. A Randomized Controlled Trial for the Effectiveness of Progressive Muscle Relaxation and Guided Imagery as Anxiety Reducing Interventions in Breast and Prostate Cancer Patients Undergoing Chemotherapy. Evid. Based Complement. Alternat. Med. 2015, 2015, 270876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hofmann, S.G.; Sawyer, A.T.; Witt, A.A.; Oh, D. The effect of mindfulness-based therapy on anxiety and depression: A meta-analytic review. J. Consult. Clin. Psychol. 2010, 78, 169–183. [Google Scholar] [CrossRef]
- Streeter, C.C.; Gerbarg, P.L.; Saper, R.B.; Ciraulo, D.A.; Brown, R.P. Effects of yoga on the autonomic nervous system, gamma-aminobutyric-acid, and allostasis in epilepsy, depression, and post-traumatic stress disorder. Med. Hypotheses 2012, 78, 571–579. [Google Scholar] [CrossRef]
- Davis, D.E.; Choe, E.; Meyers, J.; Wade, N.; Varjas, K.; Gifford, A.; Quinn, A.; Hook, J.N.; van Tongeren, D.R.; Griffin, B.J.; et al. Thankful for the little things: A meta-analysis of gratitude interventions. J. Couns. Psychol. 2016, 63, 20–31. [Google Scholar] [CrossRef]
- Thoma, M.V.; La Marca, R.; Brönnimann, R.; Finkel, L.; Ehlert, U.; Nater, U.M. The effect of music on the human stress response. PLoS ONE 2013, 8, e70156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seo, E.; Kim, S. Effect of Autogenic Training for Stress Response: A Systematic Review and Meta-Analysis. J. Korean Acad. Nurs. 2019, 49, 361–374. [Google Scholar] [CrossRef] [PubMed]
- Babanataj, R.; Mazdarani, S.; Hesamzadeh, A.; Gorji, M.H.; Cherati, J.Y. Resilience training: Effects on occupational stress and resilience of critical care nurses. Int. J. Nurs. Pract. 2019, 25, e12697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lan, H.K.; Subramanian, P.; Rahmat, N.; Kar, P.C. The effects of mindfulness training program on reducing stress and promoting well-being among nurses in critical care units. Aust. J. Adv. Nurs. 2014, 31, 22–31. [Google Scholar]
- Mealer, M.; Conrad, D.; Evans, J.; Jooste, K.; Solyntjes, J.; Rothbaum, B.; Moss, M. Feasibility and acceptability of a resilience training program for intensive care unit nurses. Am. J. Crit. Care 2014, 23, e97–e105. [Google Scholar] [CrossRef] [PubMed]
- Colquhoun, H.L.; Squires, J.E.; Kolehmainen, N.; Fraser, C.; Grimshaw, J.M. Methods for designing interventions to change healthcare professionals’ behaviour: A systematic review. Implement. Sci. 2017, 12, 30. [Google Scholar] [CrossRef] [Green Version]
- McGill, E.; Er, V.; Penney, T.; Egan, M.; White, M.; Meier, P.; Whitehead, M.; Lock, K.; Anderson de Cuevas, R.; Smith, R.; et al. Evaluation of public health interventions from a complex systems perspective: A research methods review. Soc. Sci. Med. 2021, 272, 113697. [Google Scholar] [CrossRef]
- Stanulewicz, N.; Knox, E.; Narayanasamy, M.; Shivji, N.; Khunti, K.; Blake, H. Effectiveness of Lifestyle Health Promotion Interventions for Nurses: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 17, 17. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Flum, M.; Kotejoshyer, R.; Fleishman, J.; Henning, R.; Punnett, L. Workplace Participatory Occupational Health/Health Promotion Program: Facilitators and Barriers Observed in Three Nursing Homes. J. Gerontol. Nurs. 2016, 42, 34–42. [Google Scholar] [CrossRef] [Green Version]
- Jenkins, C.; Smythe, A.; Galant-Miecznikowska, M.; Bentham, P.; Oyebode, J. Overcoming challenges of conducting research in nursing homes. Nurs. Older People 2016, 28, 16–23. [Google Scholar] [CrossRef] [Green Version]
- Schulz, M.; Damkröger, A.; Voltmer, E.; Löwe, B.; Driessen, M.; Ward, M.; Wingenfeld, K. Work-related behaviour and experience pattern in nurses: Impact on physical and mental health. J. Psychiatr. Ment. Health Nurs. 2011, 18, 411–417. [Google Scholar] [CrossRef]
- Alayli-Goebbels, A.F.G.; Dellaert, B.G.C.; Knox, S.A.; Ament, A.J.H.A.; Lakerveld, J.; Bot, S.D.M.; Nijpels, G.; Severens, J.L. Consumer preferences for health and nonhealth outcomes of health promotion: Results from a discrete choice experiment. Value Health 2013, 16, 114–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Keeffe, M.; O’Sullivan, P.; Purtill, H.; Bargary, N.; O’Sullivan, K. Cognitive functional therapy compared with a group-based exercise and education intervention for chronic low back pain: A multicentre randomised controlled trial (RCT). Br. J. Sport. Med. 2020, 54, 782–789. [Google Scholar] [CrossRef] [PubMed]
- Wienert, J.; Kuhlmann, T.; Storm, V.; Reinwand, D.; Lippke, S. Latent user groups of an eHealth physical activity behaviour change intervention for people interested in reducing their cardiovascular risk. Res. Sport. Med. 2019, 27, 34–49. [Google Scholar] [CrossRef] [PubMed]
- Stratton, E.; Lampit, A.; Choi, I.; Calvo, R.A.; Harvey, S.B.; Glozier, N. Effectiveness of eHealth interventions for reducing mental health conditions in employees: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0189904. [Google Scholar] [CrossRef] [Green Version]
- Phillips, E.A.; Gordeev, V.S.; Schreyögg, J. Effectiveness of occupational e-mental health interventions: A systematic review and meta-analysis of randomized controlled trials. Scand. J. Work. Environ. Health 2019, 45, 560–576. [Google Scholar] [CrossRef] [Green Version]
- Champion, L.; Economides, M.; Chandler, C. The efficacy of a brief app-based mindfulness intervention on psychosocial outcomes in healthy adults: A pilot randomised controlled trial. PLoS ONE 2018, 13, e0209482. [Google Scholar] [CrossRef]
- McCloud, T.; Jones, R.; Lewis, G.; Bell, V.; Tsakanikos, E. Effectiveness of a Mobile App Intervention for Anxiety and Depression Symptoms in University Students: Randomized Controlled Trial. JMIR Mhealth Uhealth 2020, 8, e15418. [Google Scholar] [CrossRef]
- Heber, E.; Lehr, D.; Ebert, D.D.; Berking, M.; Riper, H. Web-Based and Mobile Stress Management Intervention for Employees: A Randomized Controlled Trial. J. Med. Internet Res. 2016, 18, e21. [Google Scholar] [CrossRef] [Green Version]
- El Morr, C.; Layal, M. Effectiveness of ICT-based intimate partner violence interventions: A systematic review. BMC Public Health 2020, 20, 1372. [Google Scholar] [CrossRef]
- Rabbani, M.; Haque, M.M.; Dipal, D.D.; Zarif, M.I.I.; Iqbal, A.; Schwichtenberg, A.; Bansal, N.; Soron, T.R.; Ahmed, S.I.; Ahamed, S.I. A data-driven validation of mobile-based care (mCARE) project for children with ASD in LMICs. Smart Health 2022, 26, 100345. [Google Scholar] [CrossRef]
- Brandes, M.; Muellmann, S.; Allweiss, T.; Bauer, U.; Bethmann, A.; Forberger, S.; Frense, J.; Gelius, P.; Pfeifer, K.; Okan, O.; et al. Evidenzbasierung in Primärprävention und Gesundheitsförderung: Methoden und Vorgehensweisen in 5 Forschungsverbünden. Bundesgesundheitsblatt Gesundh. Gesundh. 2021, 64, 581–589. [Google Scholar] [CrossRef]
- Thranberend, T.; Knöppler, K.; Neisecke, T. SPOTLIGHT Gesundheit: Gesundheits-Apps: Bedeutender Hebel für Patient Empowerment—Potenziale Jedoch Bislang Kaum Genutzt. 2016. Available online: https://www.bertelsmann-stiftung.de/fileadmin/files/BSt/Publikationen/GrauePublikationen/SpotGes_Gesundheits-Apps_dt_final_web.pdf (accessed on 16 February 2023).
- Harrer, M.; Adam, S.H.; Fleischmann, R.J.; Baumeister, H.; Auerbach, R.; Bruffaerts, R.; Cuijpers, P.; Kessler, R.C.; Berking, M.; Lehr, D.; et al. Effectiveness of an Internet- and App-Based Intervention for College Students with Elevated Stress: Randomized Controlled Trial. J. Med. Internet Res. 2018, 20, e136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Economides, M.; Martman, J.; Bell, M.J.; Sanderson, B. Improvements in Stress, Affect, and Irritability Following Brief Use of a Mindfulness-based Smartphone App: A Randomized Controlled Trial. Mindfulness 2018, 9, 1584–1593. [Google Scholar] [CrossRef] [Green Version]
- Mönninghoff, A.; Kramer, J.N.; Hess, A.J.; Ismailova, K.; Teepe, G.W.; Tudor Car, L.; Müller-Riemenschneider, F.; Kowatsch, T. Long-term Effectiveness of mHealth Physical Activity Interventions: Systematic Review and Meta-analysis of Randomized Controlled Trials. J. Med. Internet Res. 2021, 23, e26699. [Google Scholar] [CrossRef] [PubMed]
- Calear, A.L.; Christensen, H.; Mackinnon, A.; Griffiths, K.M. Adherence to the MoodGYM program: Outcomes and predictors for an adolescent school-based population. J. Affect. Disord. 2013, 147, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Lustria, M.L.A.; Cortese, J.; Noar, S.M.; Glueckauf, R.L. Computer-tailored health interventions delivered over the Web: Review and analysis of key components. Patient Educ. Couns. 2009, 74, 156–173. [Google Scholar] [CrossRef] [PubMed]
- Lustria, M.L.A.; Noar, S.M.; Cortese, J.; van Stee, S.K.; Glueckauf, R.L.; Lee, J. A meta-analysis of web-delivered tailored health behavior change interventions. J. Health Commun. 2013, 18, 1039–1069. [Google Scholar] [CrossRef]
- Fleischmann, R.J.; Harrer, M.; Zarski, A.-C.; Baumeister, H.; Lehr, D.; Ebert, D.D. Patients’ experiences in a guided Internet- and App-based stress intervention for college students: A qualitative study. Internet Interv. 2018, 12, 130–140. [Google Scholar] [CrossRef]
- Baumann, H.; Fiedler, J.; Wunsch, K.; Woll, A.; Wollesen, B. mHealth Interventions to Reduce Physical Inactivity and Sedentary Behavior in Children and Adolescents: Systematic Review and Meta-analysis of Randomized Controlled Trials. JMIR Mhealth Uhealth 2022, 10, e35920. [Google Scholar] [CrossRef]
- Chen, Y.; Ji, M.; Wu, Y.; Deng, Y.; Wu, F.; Lu, Y. Individualized mobile health interventions for cardiovascular event prevention in patients with coronary heart disease: Study protocol for the iCARE randomized controlled trial. BMC Cardiovasc. Disord. 2021, 21, 340. [Google Scholar] [CrossRef] [PubMed]
- Maron, D.J.; Boden, W.E.; O’Rourke, R.A.; Hartigan, P.M.; Calfas, K.J.; Mancini, G.B.J.; Spertus, J.A.; Dada, M.; Kostuk, W.J.; Knudtson, M.; et al. Intensive multifactorial intervention for stable coronary artery disease: Optimal medical therapy in the COURAGE (Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation) trial. J. Am. Coll. Cardiol. 2010, 55, 1348–1358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, M.; Lee, E. Effectiveness of Mobile Health Application Use to Improve Health Behavior Changes: A Systematic Review of Randomized Controlled Trials. Healthc. Inform. Res. 2018, 24, 207–226. [Google Scholar] [CrossRef] [PubMed]
- Baumann, H.; Heuel, L.; Bischoff, L.L.; Wollesen, B. mHealth interventions to reduce stress in healthcare workers (fitcor): Study protocol for a randomized controlled trial. Trials 2023, 24, 116. [Google Scholar]
- Amagasa, S.; Machida, M.; Fukushima, N.; Kikuchi, H.; Takamiya, T.; Odagiri, Y.; Inoue, S. Is objectively measured light-intensity physical activity associated with health outcomes after adjustment for moderate-to-vigorous physical activity in adults? A systematic review. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 65. [Google Scholar] [CrossRef] [Green Version]
- Hermans, A.N.L.; Gawalko, M.; Dohmen, L.; van der Velden, R.M.J.; Betz, K.; Duncker, D.; Verhaert, D.V.M.; Heidbuchel, H.; Svennberg, E.; Neubeck, L.; et al. Mobile health solutions for atrial fibrillation detection and management: A systematic review. Clin. Res. Cardiol. 2022, 111, 479–491. [Google Scholar] [CrossRef]
- Connor-Smith, J.K.; Flachsbart, C. Relations between personality and coping: A meta-analysis. J. Pers. Soc. Psychol. 2007, 93, 1080–1107. [Google Scholar] [CrossRef] [Green Version]
- Ghaban, W.; Hendley, R. How Different Personalities Benefit from Gamification. Interact. Comput. 2019, 31, 138–153. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomized trials. Ann. Intern. Med. 2010, 152, 726–732. [Google Scholar] [CrossRef] [Green Version]
- Juszczak, E.; Altman, D.G.; Hopewell, S.; Schulz, K. Reporting of Multi-Arm Parallel-Group Randomized Trials: Extension of the CONSORT 2010 Statement. JAMA 2019, 321, 1610–1620. [Google Scholar] [CrossRef] [Green Version]
- Dwan, K.; Li, T.; Altman, D.G.; Elbourne, D. CONSORT 2010 statement: Extension to randomised crossover trials. BMJ 2019, 366, l4378. [Google Scholar] [CrossRef] [Green Version]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Urbaniak, G.C.; Plous, S. Research Randomizer; Version 4.0; Social Psychology Network: Middletown, CT, USA, 2013. [Google Scholar]
- Qudsyi, H.; Kusumaningrum, F.A.; Utami, D.S.; Fahmie, A.; Afsari, N.; Iqbal, M.M.; Stueck, M. Adaptation of AVEM (Arbeitsbezogenes Vehaltens-Und Erlebensmuster) Test to Measure Work-Related Behavior and Experience Patterns. Int. J. Sci. Technol. Res. 2008, 63–69. [Google Scholar]
- fitbase. AusGleich; fitbase: Hamburg, Germany, 2022. [Google Scholar]
- Fuhrhop, S. Textilintegrierte Trockenelektrodensysteme für die Dauerhafte EKG-Ableitung. Ph.D. Thesis, Karlsruher Institut für Technologie, Karlsruhe, Germany, 2012. [Google Scholar]
- Anastasopoulou, P.; Tubic, M.; Schmidt, S.; Neumann, R.; Woll, A.; Härtel, S. Validation and comparison of two methods to assess human energy expenditure during free-living activities. PLoS ONE 2014, 9, e90606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hysenllari, E.; Ottenbacher, J.; McLennan, D. Validation of human activity recognition using a convolutional neural network on accelerometer and gyroscope data. Ger. J. Exerc. Sport. Res. 2022, 52, 248–252. [Google Scholar] [CrossRef]
- Schmitz, C. LimeSurvey; Limesurvey GmbH: Hamburg, Germany, 2003. [Google Scholar]
- Fenzl, M.; Schlegel, C. Herzratenvariabilität—Diagnosemittel für die Gesundheit: Altersbezogene Effektgrössen. Schweiz. Z. Sportmed. Und Sport. 2010, 58, 138–140. [Google Scholar]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M. Sedentary Behavior Research Network (SBRN)—Terminology Consensus Project process and outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 75. [Google Scholar] [CrossRef] [Green Version]
- Wollesen, B.; Menzel, J.; Lex, H.; Mattes, K. The BASE-Program-A Multidimensional Approach for Health Promotion in Companies. Healthcare 2016, 4, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herold, F.; Müller, P.; Gronwald, T.; Müller, N.G. Dose-Response Matters! A Perspective on the Exercise Prescription in Exercise-Cognition Research. Front. Psychol. 2019, 10, 2338. [Google Scholar] [CrossRef] [Green Version]
- Borresen, J.; Lambert, M.I. The quantification of training load, the training response and the effect on performance. Sport. Med. 2009, 39, 779–795. [Google Scholar] [CrossRef]
- Chang, H.E.; Cho, S.-H. Nurses’ steps, distance traveled, and perceived physical demands in a three-shift schedule. Hum. Resour. Health 2022, 20, 72. [Google Scholar] [CrossRef]
- Hazzard, B.; Johnson, K.; Dordunoo, D.; Klein, T.; Russell, B.; Walkowiak, P. Work- and nonwork-related factors associated with PACU nurses’ fatigue. J. Perianesth. Nurs. 2013, 28, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Holtermann, A.; Krause, N.; van der Beek, A.J.; Straker, L. The physical activity paradox: Six reasons why occupational physical activity (OPA) does not confer the cardiovascular health benefits that leisure time physical activity does. Br. J. Sport. Med. 2018, 52, 149–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coenen, P.; Huysmans, M.A.; Holtermann, A.; Krause, N.; van Mechelen, W.; Straker, L.M.; van der Beek, A.J. Do highly physically active workers die early? A systematic review with meta-analysis of data from 193 696 participants. Br. J. Sport. Med. 2018, 52, 1320–1326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bischoff, L.L.; Baumann, H.; Meixner, C.; Nixon, P.; Wollesen, B. App-Tailoring Requirements to Increase Stress Management Competencies Within Families: Cross-sectional Survey Study. J. Med. Internet Res. 2021, 23, e26376. [Google Scholar] [CrossRef]
- Brown, J.; Pope, N.; Bosco, A.M.; Mason, J.; Morgan, A. Issues affecting nurses’ capability to use digital technology at work: An integrative review. J. Clin. Nurs. 2020, 29, 2801–2819. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Intervention | Type | Need | Biofeedback | Coaching | Report |
|---|---|---|---|---|---|---|
| 1 | Web-based digital stress management intervention | Web-based | No | No | No | No |
| 2 | Web-based need-oriented digital stress management intervention | Web-based | Yes | No | No | No |
| 3 | Web-based need-oriented digital stress management intervention with telephone coaching | Web-based | Yes | No | Yes | No |
| 4 | App-based personality specific digital stress management interventions with sensory biofeedback | App-based | No | Yes | No | No |
| 5 | App-based personality specific digital stress management intervention with sensory biofeedback and health report | App-based | No | Yes | No | Yes |
| Focus | Sub Focus | App | WBT | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Healthy Nutrition | Weight Loss | Physical Activity | Spine Gymnastics | Meditation/Mindfulness | Hatha Yoga | Sleep and Stress | Autogenic Training | |||
| Individualization | Direct biofeedback | x | ||||||||
| AVEM patterns | x | |||||||||
| Telephone coaching | (x) | (x) | (x) | (x) | (x) | (x) | (x) | (x) | ||
| Health Report | (x) | (x) | (x) | (x) | (x) | (x) | (x) | (x) | (x) | |
| Need orientation | (x) | (x) | (x) | (x) | (x) | (x) | (x) | (x) | ||
| Stress and relaxation | Problem-focused | x | ||||||||
| Deep breathing | x | x | x | x | x | |||||
| Mindfulness | x | x | x | x | ||||||
| Goal setting | x | x | x | x | x | x | ||||
| Gratitude journal | x | x | x | x | ||||||
| Positive psychology | x | x | x | x | x | |||||
| Autogenic training | x | x | x | x | x | |||||
| Muscle relaxation | x | x | x | |||||||
| Body perception | x | x | x | |||||||
| Stress physiology | x | |||||||||
| Physical activity | Stretching and yoga | x | x | x | ||||||
| Fascia training | x | x | x | |||||||
| Behavior change | x | |||||||||
| Activity habits | x | |||||||||
| Endurance training | x | x | ||||||||
| Anatomy | x | x | x | |||||||
| Spine health | x | |||||||||
| Parameter | Unit | Description [103] |
|---|---|---|
| SDNN | ms | Standard deviation of all RR intervals includes fluctuations over shorter as well as more widely divergent time periods. |
| RMSSD | ms | Square root of the squared mean value of the sum of all differences of successive RRintervals. Marker for selective assessment of efferent vagus activity and parasympathetic influence on the heart. |
| LF/HF ratio | % | Quotient of LF and HF: LF = power density spectrum from >0.04 to 0.15 Hz, percentage LF of the full spectrum. This parameter characterizes the potency of the low frequency components and can be attributed to parasympathetic as well as sympathetic activity; HF = power density spectrum from > 0.15 to 0.4 Hz, percentage HF of the full spectrum, mediated by respiratory-induced modulations of parasympathetic activity. |
| Baevsky | Index | Measure for characterizing recorded ECG signals or RR intervals. Reflects the degree of central control of the heart rhythm and characterizes the activity of the sympathetic part of the autonomic nervous system (VNS). It serves as an indicator of shifts in the balance of the VNS, i.e., changes in the balance between the effects of the sympathetic and parasympathetic nervous systems. |
| Steps | Counts/day | Accelerometer measured number of steps taken per day. |
| MVPA | Min/day | Accelerometer measured time spend in moderate to vigorous physical activity per day. |
| Disrupt | Counts/day | Accelerometer measured inactive period disruption counts. Counting occurs when a >30 min period of inactivity is interrupted with physical activity. This parameter serves as a measure of behavior change. |
| Inactivity | Min/day | Inactivity or sedentary behavior is defined by any waking behavior characterized by an energy expenditure ≤ 1.5 metabolic equivalents of task [METs] while in a sitting, reclining, or lying posture [104]. |
| Pre-Intervention Assessment | Post-Intervention Assessment | MANOVA | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Studyarm | Control | Overall | Studyarm | Control | Overall | Time*Group | ||||||||||||
| 1 | 2 | 3 | 4 | 5 | 1 | 2 | 3 | 4 | 5 | F(1,5) | p | η2p | ||||||
| Gender | ||||||||||||||||||
| male | n | 12 | 4 | 2 | 43 | 21 | 20 | 102 | 7 | 0 | 1 | 3 | 3 | 52 | 66 | |||
| % | 29 | 10 | 13 | 47 | 38 | 14 | 26.5 | 33.3 | 0 | 14.3 | 18.7 | 8.8 | 75.4 | 38.8 | ||||
| female | n | 29 | 36 | 13 | 48 | 34 | 123 | 283 | 14 | 23 | 6 | 13 | 31 | 17 | 104 | |||
| % | 71 | 90 | 87 | 53 | 62 | 86 | 73.5 | 66.6 | 100 | 85.7 | 81.3 | 91.2 | 24.6 | 41.2 | ||||
| Age | x¯ | 42.4 | 40.6 | 39.0 | 40.8 | 41.6 | 42.4 | 41.1 | 45.8 | 40.2 | 42.6 | 42.6 | 44.3 | 40.9 | 42.7 | 0.888 | 0.489 | 0.008 |
| s | 12.1 | 11.2 | 9.8 | 10.6 | 11.5 | 10.2 | 10.9 | 10.6 | 9.5 | 9.3 | 9.7 | 10.7 | 10.5 | 10.0 | ||||
| BMI | x¯ | 26.1 | 27.5 | 24.9 | 26.4 | 27.8 | 26.7 | 26.6 | 25.8 | 29.1 | 26.1 | 28.0 | 26.7 | 26.8 | 27.1 | 0.177 | 0.971 | 0.002 |
| s | 7.1 | 5.3 | 4.6 | 6.6 | 7.0 | 6.0 | 6.1 | 3.9 | 9.0 | 5.0 | 7.4 | 6.3 | 6.1 | 6.3 | ||||
| Steps counts/day | x¯ | 7925 | 8541 | 8535 | 7588 | 6609 | 8074 | 7879 | 6402 | 8720 | 8956 | 8129 | 6876 | 7562 | 7774 | 0.794 | 0.555 | 0.008 |
| s | 4253 | 2827 | 3255 | 3025 | 2716 | 3509 | 3264 | 2745 | 3121 | 4774 | 3726 | 3010 | 3062 | 3406 | ||||
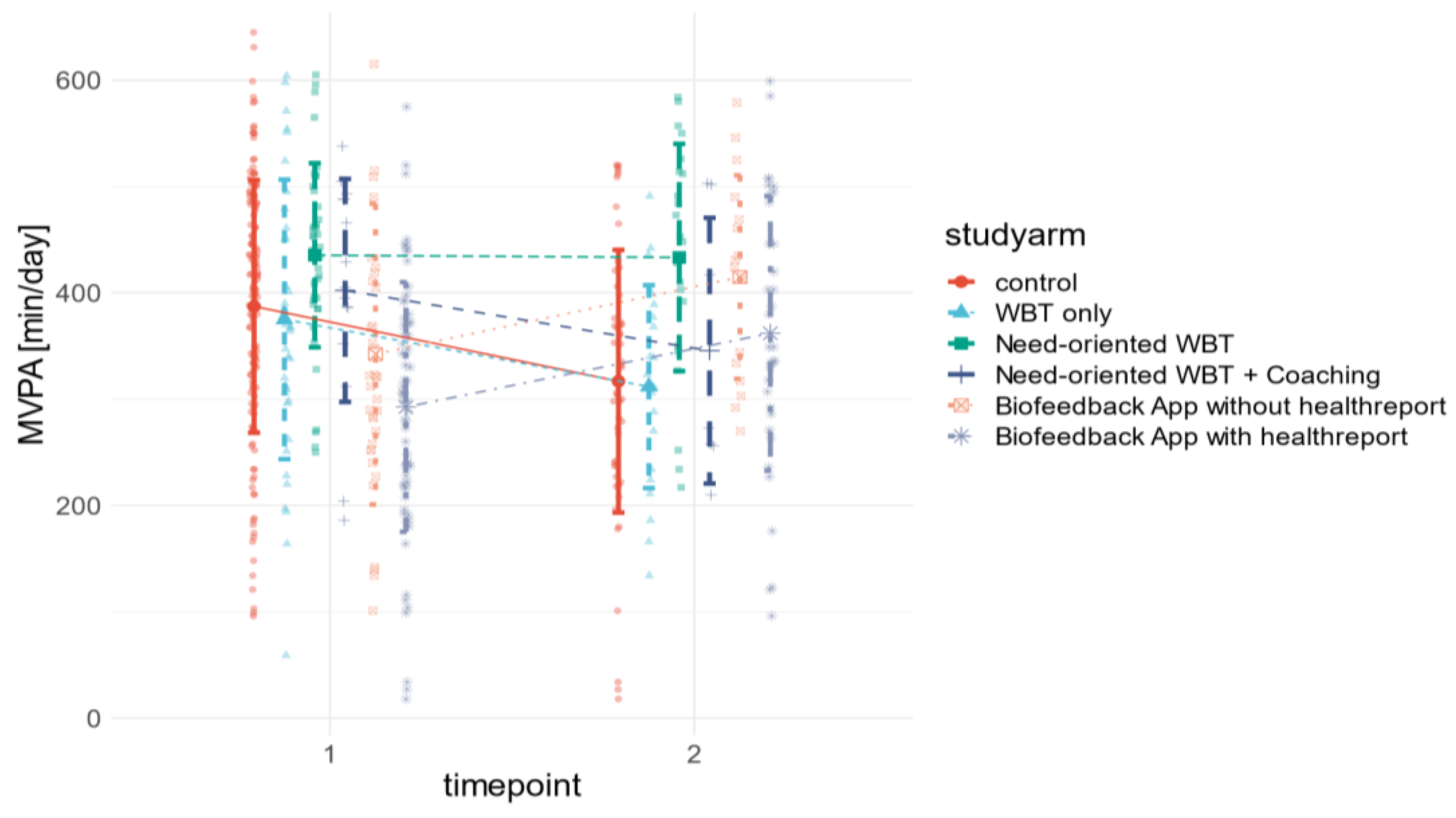
| MVPA min/day | x¯ | 375.0 | 435.4 | 402.3 | 342.4 | 292.6 | 387.2 | 372.5 | 311.8 | 433.3 | 345.6 | 414.8 | 362.0 | 316.8 | 364.0 | 5.826 | <0.001 | 0.057 |
| s | 131.4 | 86.6 | 104.9 | 141.5 | 117.4 | 118.8 | 116.8 | 95.4 | 106.8 | 125.0 | 95.7 | 129.1 | 123.5 | 112.6 | ||||
| Inactivity min/day | x¯ | 287.8 | 213.0 | 227.2 | 182.7 | 231.0 | 254.2 | 232.7 | 358.3 | 183.2 | 284.7 | 192.6 | 280.9 | 226.6 | 254.4 | 2.181 | 0.055 | 0.022 |
| s | 150.3 | 113.5 | 138.5 | 81.1 | 112.4 | 137.5 | 122.2 | 156.1 | 108.3 | 137.0 | 72.1 | 142.7 | 120.2 | 122.7 | ||||
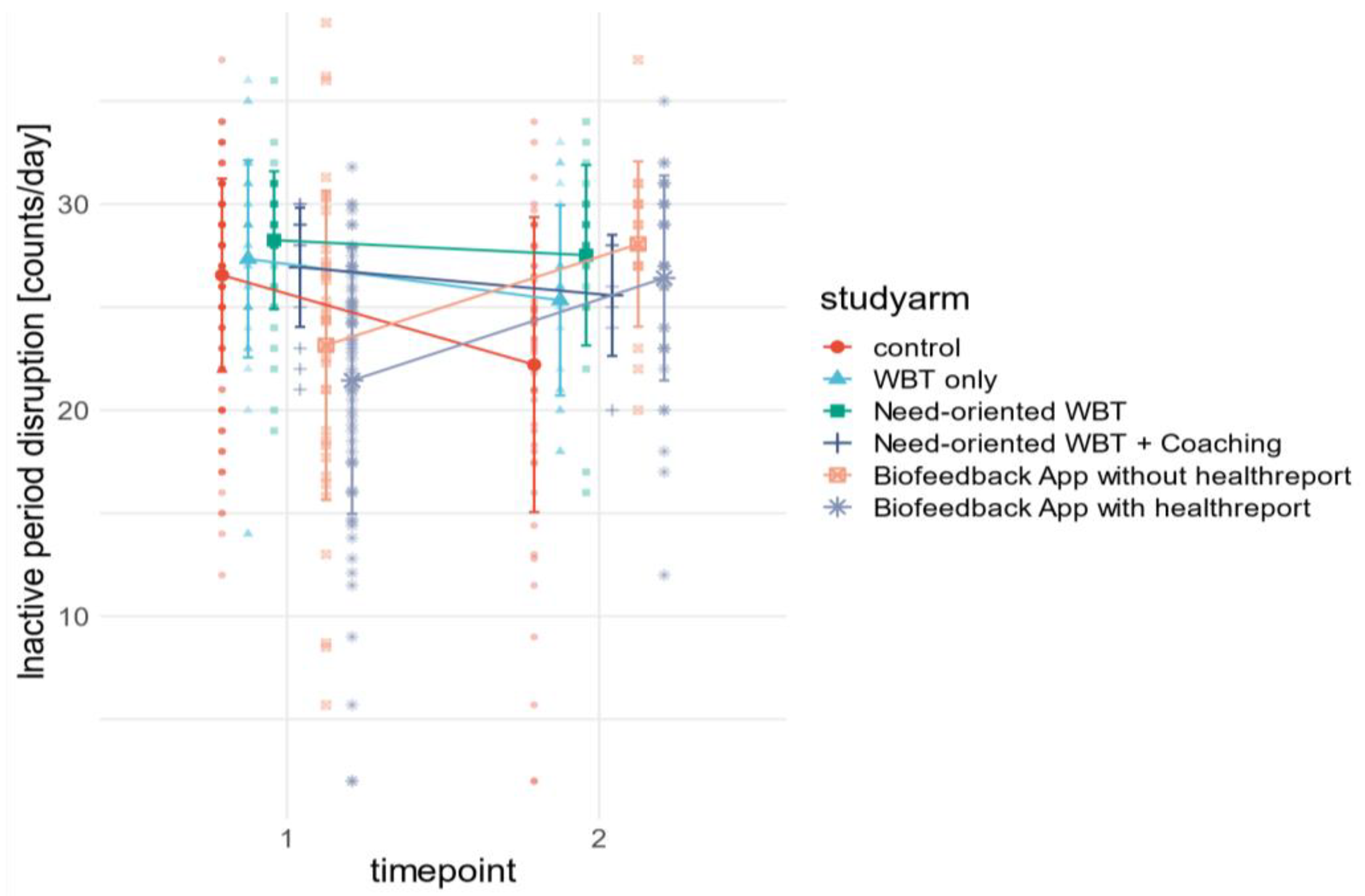
| Disruption counts/day | x¯ | 27.3 | 28.3 | 26.9 | 23.2 | 21.4 | 26.6 | 25.6 | 25.3 | 27.5 | 25.6 | 28.1 | 26.4 | 22.2 | 25.9 | 11.2 | <0.001 | 0.100 |
| s | 4.8 | 3.3 | 2.9 | 7.5 | 6.5 | 4.7 | 4.9 | 4.6 | 4.4 | 2.9 | 4.0 | 5.0 | 7.2 | 4.7 | ||||
| SDNN ms | x¯ | 50.3 | 47.3 | 47.3 | 49.5 | 49.7 | 48.9 | 48.8 | 50.6 | 47.0 | 43.6 | 47.2 | 48.0 | 51.2 | 47.9 | 0.609 | 0.693 | 0.006 |
| s | 11.0 | 11.3 | 12.8 | 9.3 | 12.5 | 11.4 | 11.4 | 11.0 | 10.9 | 10.3 | 10.9 | 12.2 | 12.0 | 11.2 | ||||
| RMSSD ms | x¯ | 28.4 | 28.5 | 27.4 | 28.3 | 29.3 | 27.9 | 28.3 | 28.6 | 27.3 | 27.0 | 26.1 | 27.6 | 29.9 | 27.7 | 0.697 | 0.626 | 0.007 |
| s | 7.5 | 10.6 | 9.0 | 7.4 | 9.8 | 8.7 | 8.8 | 7.7 | 9.0 | 9.6 | 7.3 | 9.2 | 9.8 | 8.8 | ||||
| LFHF % | x¯ | 5.1 | 4.9 | 5.1 | 5.7 | 4.8 | 5.0 | 5.1 | 4.6 | 5.2 | 4.4 | 6.1 | 4.7 | 4.9 | 5.0 | 0.214 | 0.956 | 0.002 |
| s | 2.3 | 2.6 | 3.7 | 3.8 | 2.5 | 3.1 | 3.0 | 2.1 | 2.5 | 2.4 | 5.9 | 2.6 | 2.9 | 3.1 | ||||
| Baevsky Index | x¯ | 241.3 | 279.0 | 283.1 | 268.0 | 270.5 | 263.9 | 267.6 | 225.4 | 289.3 | 307.4 | 258.6 | 282.4 | 248.5 | 268.6 | 0.196 | 0.964 | 0.002 |
| s | 96.3 | 127.5 | 159.0 | 119.0 | 171.2 | 144.9 | 136.3 | 81.6 | 192.9 | 154.1 | 106.2 | 154.5 | 134.5 | 137.3 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baumann, H.; Heuel, L.; Bischoff, L.L.; Wollesen, B. Efficacy of Individualized Sensory-Based mHealth Interventions to Improve Distress Coping in Healthcare Professionals: A Multi-Arm Parallel-Group Randomized Controlled Trial. Sensors 2023, 23, 2322. https://doi.org/10.3390/s23042322
Baumann H, Heuel L, Bischoff LL, Wollesen B. Efficacy of Individualized Sensory-Based mHealth Interventions to Improve Distress Coping in Healthcare Professionals: A Multi-Arm Parallel-Group Randomized Controlled Trial. Sensors. 2023; 23(4):2322. https://doi.org/10.3390/s23042322
Chicago/Turabian StyleBaumann, Hannes, Luis Heuel, Laura Louise Bischoff, and Bettina Wollesen. 2023. "Efficacy of Individualized Sensory-Based mHealth Interventions to Improve Distress Coping in Healthcare Professionals: A Multi-Arm Parallel-Group Randomized Controlled Trial" Sensors 23, no. 4: 2322. https://doi.org/10.3390/s23042322
APA StyleBaumann, H., Heuel, L., Bischoff, L. L., & Wollesen, B. (2023). Efficacy of Individualized Sensory-Based mHealth Interventions to Improve Distress Coping in Healthcare Professionals: A Multi-Arm Parallel-Group Randomized Controlled Trial. Sensors, 23(4), 2322. https://doi.org/10.3390/s23042322