
COVID-19 Vaccine Acceptance, Hesitancy, and Resistancy among University Students in France


Abstract
:1. Introduction
2. Methods
2.1. Study Design and Settings
2.2. Questionnaire
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. World Health Organization COVID-19 Dashboard. Available online: https://covid19.who.int/ (accessed on 28 April 2021).
- European Medicines Agency. COVID-19 Vaccines. Available online: https://www.ema.europa.eu/en/human-regulatory/overview/public-health-threats/coronavirus-disease-covid-19/treatments-vaccines/covid-19-vaccines (accessed on 25 March 2021).
- Harrison, E.A.; Wu, J.W. Vaccine confidence in the time of COVID-19. Eur. J. Epidemiol. 2020, 35, 325–330. [Google Scholar] [CrossRef] [Green Version]
- Ministère Des Solidarités et de la Santé. Available online: https://solidarites-sante.gouv.fr/grands-dossiers/vaccin-covid-19/publics-prioritaires-vaccin-covid-19 (accessed on 25 March 2021).
- Chou, R.; Dana, T.; Buckley, D.I.; Selph, S.; Fu, R.; Totten, A.M. Epidemiology of and Risk Factors for Coronavirus Infection in Health Care Workers. Ann. Intern. Med. 2020, 173, 120–136. [Google Scholar] [CrossRef]
- Han, D.; Li, R.; Han, Y.; Zhang, R.; Li, J. COVID-19: Insight into the asymptomatic SARS-COV-2 infection and transmission. Int. J. Biol. Sci. 2020, 15, 2803–2811. [Google Scholar] [CrossRef] [PubMed]
- Guilamo-Ramos, V.; Benzekri, A.; Thimm-Kaiser, M.; Hidalgo, A.; Perlman, D.C. Reconsidering Assumptions of Adolescent and Young Adult Severe Acute Respiratory Syndrome Coronavirus 2 Transmission Dynamics. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.; Peng, F.; Xu, B.; Zhao, J.; Liu, H.; Peng, J.; Li, Q.; Jiang, C.; Zhou, Y.; Liu, S.; et al. 2020 Risk factors of critical and mortal COVID-19 cases: A systematic literature review and meta-analysis. J. Infect. 2020, 8, e16–e25. [Google Scholar] [CrossRef]
- Figliozzi, S.; Masci, P.G.; Ahmadi, N.; Tondi, L.; Koutli, E.; Aimo, A.; Stamatelopoulos, K.; Dimopoulos, M.-A.; Caforio, A.L.P.; Georgiopoulos, G. Predictors of adverse prognosis in COVID-19: A systematic review and meta-analysis. Eur. J. Clin. Investig. 2020, 10, e13362. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.; Weintz, C.; Pace, J.; Indana, D.; Linka, K.; Kuhl, E. Are college campuses superspreaders? A data-driven modeling study. Comput. Methods Biomech. Biomed. Eng. 2021, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.; Tu, P.; Beitsch, L.M. Confidence and Receptivity for COVID-19 Vaccines: A Rapid Systematic Review. Vaccines 2021, 9, 16. [Google Scholar] [CrossRef]
- Global Attitudes on a COVID-19 Vaccine. Ipsos Survey for The World Economic Forum. Available online: https://www.ipsos.com/en-ro/global-attitudes-covid-19-vaccine-january-2021 (accessed on 25 March 2021).
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Böhm, R. Beyond confidence: Development of a measure assessing the 5C psychological antecedents of vaccination. PLoS ONE 2018, 13, e0208601. [Google Scholar] [CrossRef] [Green Version]
- Lane, S.; MacDonald, N.E.; Marti, M.; Dumolard, L. Vaccine hesitancy around the globe: Analysis of three years of WHO/UNICEF Joint Reporting Form data-2015–2017. Vaccine 2018, 36, 3861–3867. [Google Scholar] [CrossRef] [PubMed]
- Dubé, E.; Laberge, C.; Guay, M.; Bramadat, P.; Roy, R.; Bettinger, J. Vaccine hesitancy: An overview. Hum. Vaccines Immunother. 2013, 8, 1763–1773. [Google Scholar] [CrossRef] [PubMed]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef] [PubMed]
- Detoc, M.; Bruel, S.; Frappe, P.; Tardy, B.; Botelho-Nevers, E.; Gagneux-Brunon, A. Intention to participate in a COVID-19 vaccine clinical trial and to get vaccinated against COVID-19 in France during the pandemic. Vaccine 2020, 38, 7002–7006. [Google Scholar] [CrossRef]
- Kreps, S.; Prasad, S.; Brownstein, J.; Hswen, Y.; Garibaldi, B.; Zhang, B.; Kriner, D. Factors Associated with US Adults’ Likelihood of Accepting COVID-19 Vaccination. JAMA Netw. Open 2020, 10, e2025594. [Google Scholar] [CrossRef]
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Negl. Trop. Dis. 2020, 14, e0008961. [Google Scholar] [CrossRef]
- Suresh, P.S.; Thejaswini, V.; Rajan, T. Factors associated with 2009 pandemic influenza A (H1N1) vaccination acceptance among university students from India during the post-pandemic phase. BMC Infect. Dis. 2011, 11, 205. [Google Scholar] [CrossRef] [Green Version]
- Barello, S.; Nania, T.; Dellafiore, F.; Graffigna, G.; Caruso, R. ‘Vaccine hesitancy’ among university students in Italy during the COVID-19 pandemic. Eur. J. Epidemiol. 2020, 35, 781–783. [Google Scholar] [CrossRef]
- Saied, S.; Saied, E.; Kabbash, I.; Abdo, S.A.E.-F. Vaccine Hesitancy: Beliefs and Barriers Associated with COVID-19 Vaccination among Egyptian Medical Students. Med. Virol. 2021, 93, 4280–4291. [Google Scholar] [CrossRef]
- Lucia, V.C.; Kelekar, A.; Afonso, N.M. COVID-19 vaccine hesitancy among medical students. J. Public Health 2020, 230. [Google Scholar] [CrossRef]
- Montagni, I.; Ouazzani-Touhami, K.; Mebarki, A.; Texier, N.; Schück, S.; Tzourio, C.; The Confins Group. Acceptance of a Covid-19 vaccine is associated with ability to detect fake news and health literacy. J. Public Health 2021. [Google Scholar] [CrossRef]
- Grech, V.; Gauci, C. WITHDRAWN: Vaccine hesitancy in the University of Malta Faculties of Health Sciences, Dentistry and Medicine vis-à-vis influenza and novel COVID-19 vaccination. Early Hum. Dev. 2020, 105258. [Google Scholar] [CrossRef]
- Verger, P.; Fressard, L.; Collange, F.; Gautier, A.; Jestin, C.; Launay, O.; Raude, J.; Pulcini, C.; Peretti-Watel, P. Vaccine Hesitancy Among General Practitioners and Its Determinants During Controversies: A National Cross-sectional Survey in France. EBioMedicine 2015, 2, 891–897. [Google Scholar] [CrossRef] [Green Version]
- Lepiller, Q.; Bouiller, K.; Slekovec, C.; Millot, D.; Mazué, N.; Pourchet, V.; Balice, R.; Garrien-Maire, F.; Simon, E.; Wintenberger, V.; et al. Perceptions of French healthcare students of vaccines and the impact of conducting an intervention in health promotion. Vaccine 2020, 38, 6794–6799. [Google Scholar] [CrossRef]
- Kernéis, S.; Jacquet, C.; Bannay, A.; May, T.; Launay, O.; Verger, P. Pulcini On behalf of the EDUVAC Study Group Vaccine Education of Medical Students: A Nationwide Cross-sectional Survey. Am. J. Prev. Med. 2017, 3, e97–e104. [Google Scholar] [CrossRef] [PubMed]
- Van Bavel, J.; Baicker, K.; Boggio, P.; Capraro, V.; Cichocka, A.; Cikara, M.; Crockett, M.; Crum, A.; Douglas, K.; Druckman, J.; et al. Using social and behavioural science to support COVID-19 pandemic response. Nat. Hum. Behav. 2020, 5, 460–471. [Google Scholar] [CrossRef]
- Karlsson, L.C.; Lewandowsky, S.; Antfolk, J.; Salo, P.; Lindfelt, M.; Oksanen, T.; Kivimäki, M.; Soveri, A. The association between vaccination confidence, vaccination behavior, and willingness to recommend vaccines among Finnish healthcare workers. PLoS ONE 2019, 14, e0224330. [Google Scholar] [CrossRef]
- Vulpe, S.-N.; Rughiniş, C. Social amplification of risk and “probable vaccine damage”: A typology of vaccination beliefs in 28 European countries. Vaccine 2021, 39, 1508–1515. [Google Scholar] [CrossRef] [PubMed]
- Kreps, S.; Dasgupta, N.; Brownstein, J.; Hswen, Y.; Kriner, D. Public attitudes toward COVID-19 vaccination: The role of vaccine attributes, incentives, and misinformationPublic attitudes toward COVID-19 vaccination: The role of vaccine attributes, incentives, and misinformation. npj Vaccines 2021, 6, 73. [Google Scholar] [CrossRef]
- Palamenghi, L.; Barello, S.; Boccia, S.; Graffigna, G. Mistrust in biomedical research and vaccine hesitancy: The forefront challenge in the battle against COVID-19 in Italy. Eur. J. Epidemiol. 2020, 35, 785–788. [Google Scholar] [CrossRef] [PubMed]
- Latkin, C.A.; Dayton, L.; Yi, G.; Colon, B.; Kong, X. Mask usage, social distancing, racial, and gender correlates of COVID-19 vaccine intentions among adults in the US. PLoS ONE 2021, 16, e0246970. [Google Scholar] [CrossRef] [PubMed]
- Korhonen, T.; Neveu, A.; Armengaud, A.; Six, C.; Danis, K.; Malfait, P. Low measles vaccination coverage among medical residents in Marseille, France: Reasons for non-vaccination. Eur. J. Public Health 2013, 3, 512–517. [Google Scholar]
- Viswanath, K.; Bekalu, M.; Dhawan, D.; Pinnamaneni, R.; Lang, J.; McLoud, R. Individual and social determinants of COVID-19 vaccine uptake. BMC Public Health 2021, 21, 818. [Google Scholar] [CrossRef]
- Schwarzinger, M.; Watson, V.; Arwidson, P.; Alla, F.; Luchini, S. COVID-19 vaccine hesitancy in a representative working-age population in France: A survey experiment based on vaccine characteristics. Lancet Public Health 2021, 6, e210–e221. [Google Scholar] [CrossRef]
- Rodas, J.R.; Lau, C.H.; Zhang, Z.Z.; Griffiths, S.M.; Luk, W.C.; Kim, J.H. Exploring predictors influencing intended and actual acceptability of the A/H1N1 pandemic vaccine: A cohort study of university students in Hong Kong. Public Health 2012, 126, 1007–1012. [Google Scholar] [CrossRef]
- Karafillakis, E.; Dinca, I.; Apfel, F.; Cecconi, S.; Wűrz, A.; Takacs, J.; Suk, J.; Celentano, L.P.; Kramarz, P.; Larson, H.J. Vaccine hesitancy among healthcare workers in Europe: A qualitative study. Vaccine 2016, 34, 5013–5020. [Google Scholar] [CrossRef] [PubMed]
- Smith, N.; Graham, T. Mapping the anti-vaccination movement on Facebook. Inf. Commun. Soc. 2019, 22, 1310–1327. [Google Scholar] [CrossRef]
- Germani, F.; Biller-Andorno, N. The anti-vaccination infodemic on social media: A behavioral analysis. PLoS ONE 2021, 16, e0247642. [Google Scholar] [CrossRef]
- Edwards, B.; Biddle, N.; Gray, M.; Sollis, K. COVID-19 vaccine hesitancy and resistance: Correlates in a nationally representative longitudinal survey of the Australian population. PLoS ONE 2021, 16, e0248892. [Google Scholar] [CrossRef]
- Johnson, D.K.; Mello, E.J.; Walker, T.D.; Hood, S.J.; Jensen, J.L.; Poole, B.D. Combating Vaccine Hesitancy with Vaccine-Preventable Disease Familiarization: An Interview and Curriculum Intervention for College Students. Vaccines 2019, 7, 39. [Google Scholar] [CrossRef] [Green Version]
- Paterson, P.; Meurice, F.; Stanberry, L.R.; Glismann, S.; Rosenthal, S.L.; Larson, H.J. Vaccine hesitancy and healthcare providers. Vaccine 2016, 34, 6700–6706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marco-Franco, J.M.; Pita-Barros, P.; Vivas-Orts, D.; González-de-Julián, S.; Vivas-Consuelo, D. COVID-19, Fake News, and Vaccines: Should Regulation Be Implemented? Int. J. Environ. Res. Public Health 2021, 18, 744. [Google Scholar] [CrossRef] [PubMed]
- Montagni, I.; Mabchour, I.; Tzourio, C. Gamification is an innovative and promising option to consider when designing vaccination-related interventions addressed to the general public and young people in particular, especially for those who are hesitant about vaccination. JMIR Serious Games 2020, 2, e16983. [Google Scholar] [CrossRef] [PubMed]
- Université de Rouen Normandie. Available online: https://www.univ-rouen.fr/ (accessed on 22 April 2021).
- French, J.; Deshpande, S.; Evans, W.; Obregon, R. Key Guidelines in Developing a Pre-Emptive COVID-19 Vaccination Uptake Promotion Strategy. Int. J. Environ. Res. Public Health 2020, 17, 5893. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Behavioral Considerations for Acceptance and Uptake of COVID-19 Vaccines: WHO Technical Advisory Group on Behavioral Insights and Sciences for Health, Meeting Report, 15 October 2020; World Health Organization: Geneva, Switzerland, 2020; Available online: https://apps.who.int/iris/handle/10665/337335 (accessed on 5 April 2021).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Item | Questions | Proposed Answers |
|---|---|---|
| Conventional vaccination (excluding COVID-19) | ||
| Are you confident in the efficacy of the vaccines? | Scale from 0 to 10: 0 “not at all confident” to 10 “very confident” | |
| Are you confident in the security of the vaccines? | Scale from 0 to 10: 0 “not at all confident” to 10 ”very confident” | |
| Do you think that getting vaccinated is useful for your health? | Scale from 0 to 10:0 “not at all useful” to 10 “very useful” | |
| How would you rate your level of knowledge about vaccination? | Scale from 0 to 10: 0 “I know nothing at all” to 10 “I know a lot” | |
| COVID-19 infection | ||
| Have you been infected with COVID-19? | Yes or no | |
| Has a relative been hospitalised or died from COVID-19 | Yes or no | |
| COVID-19 vaccination | ||
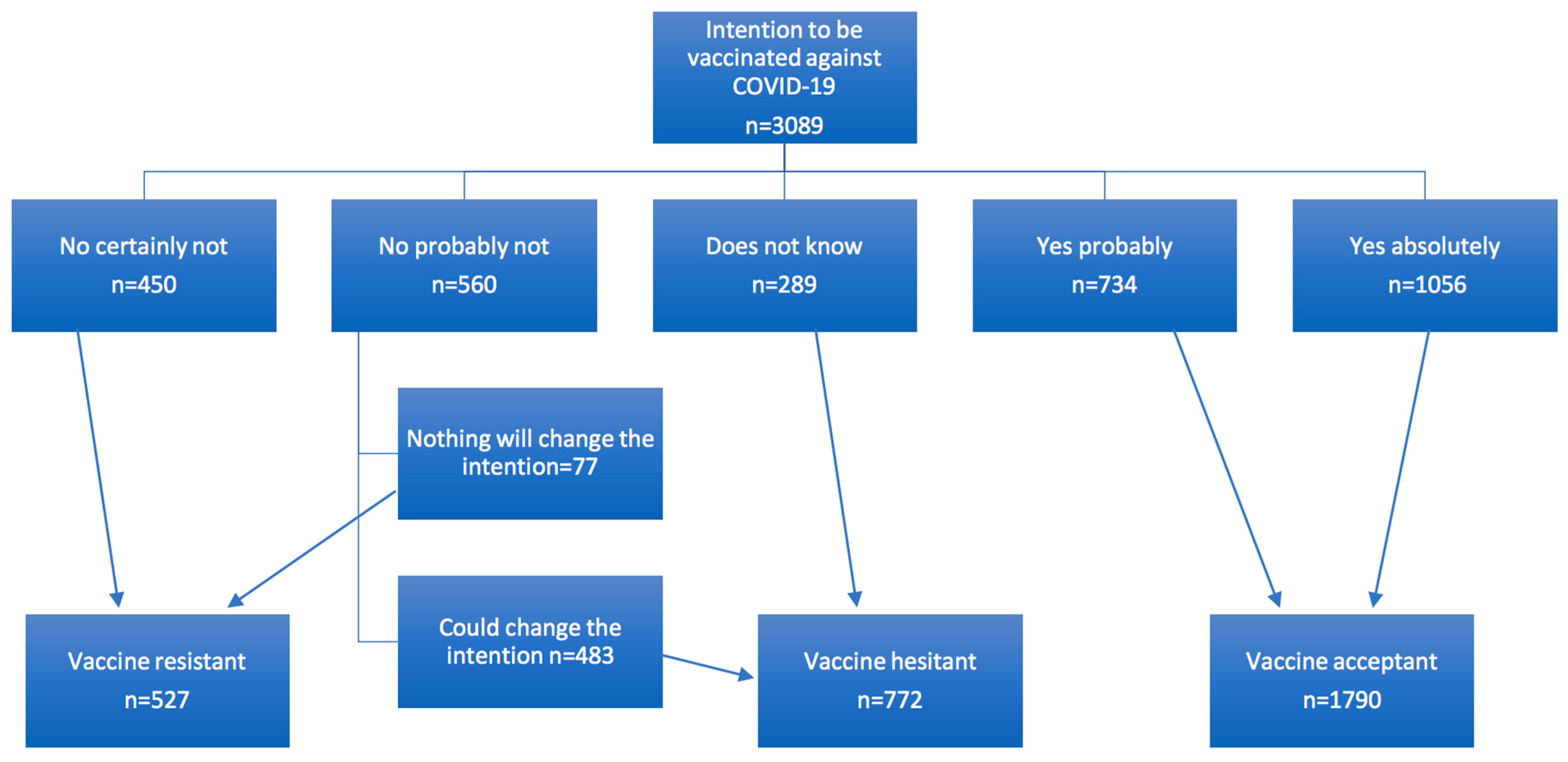
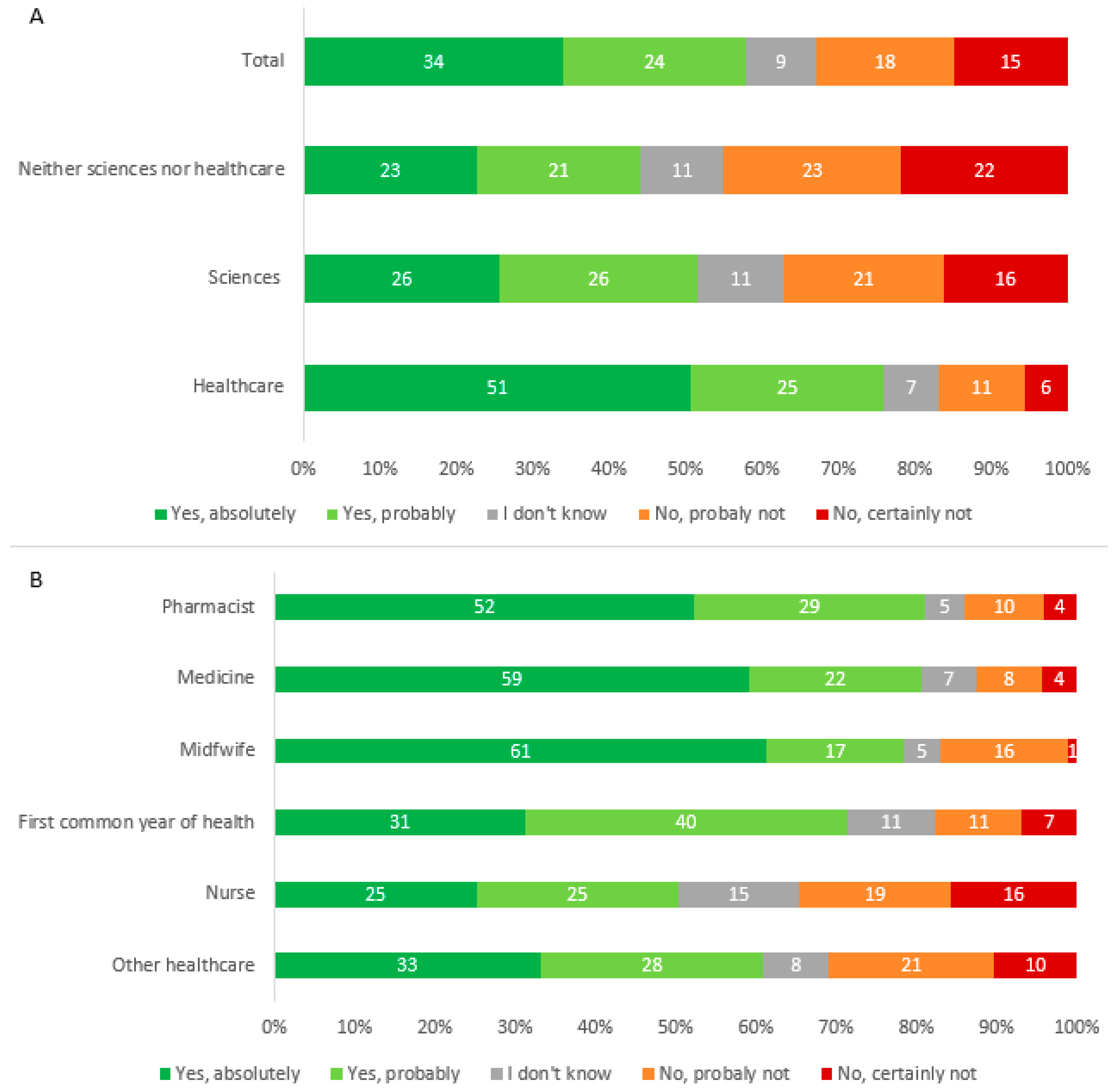
| Do you intend to be vaccinated against COVID-19 (when it is possible for you to do so)? | «Yes, absolutely”; “Yes, probably”; “No, probably not“; “No, certainly not”; and “I don’t know“ | |
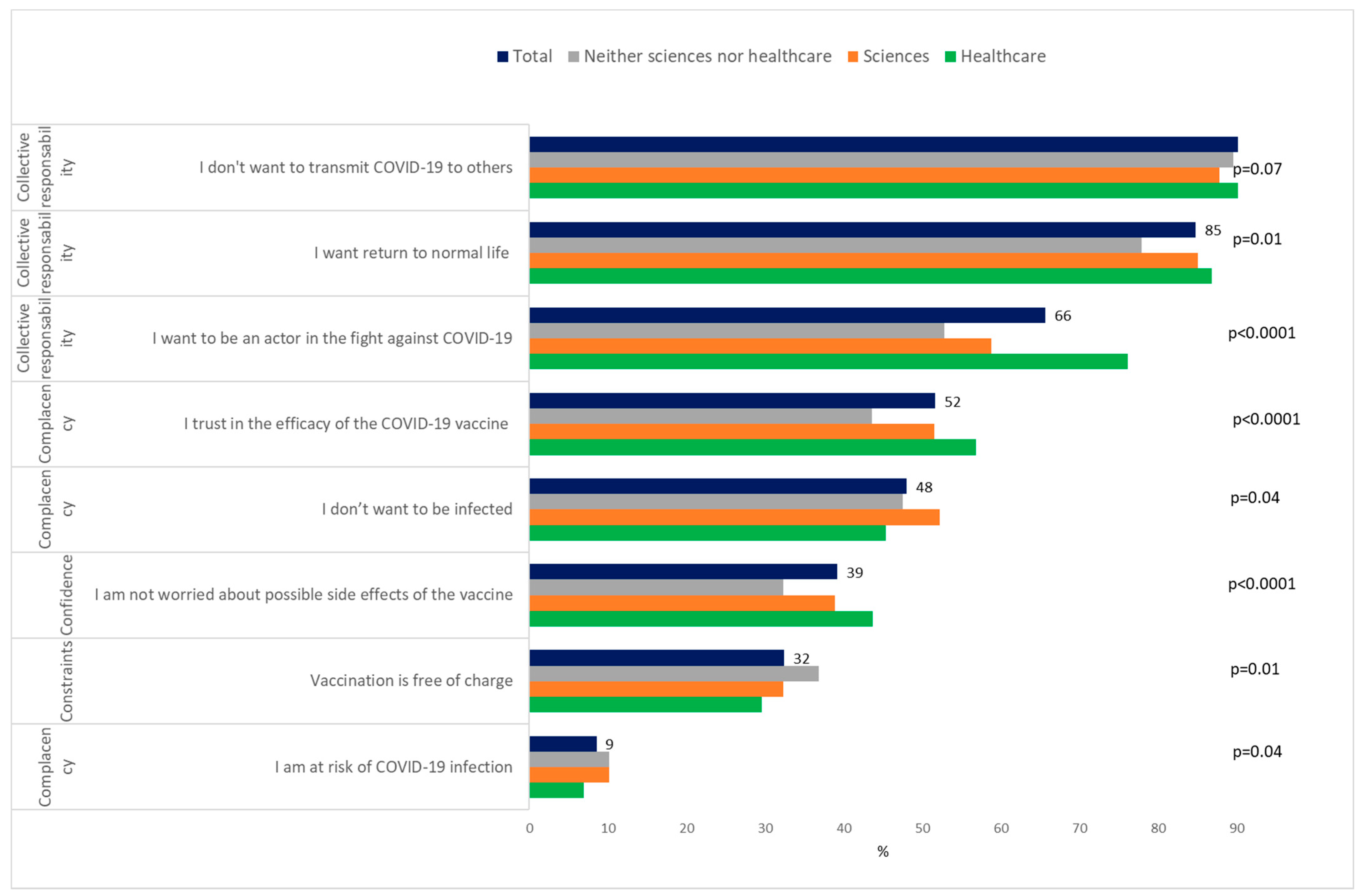
| Motivations of vaccination | I am at risk of COVID-19 infection” I don’t want to be infected, I don′t want to transmit COVID-19 to others I trust in the efficacy of the COVID-9 vaccine I am not worried about possible side effects of the COVID-19 vaccine I want to be an actor in the fight against COVID-19 I want return to normal life as soon as possible The vaccination is free of charge | Yes or no |
| Reasons of hesitation | I am not at risk of sever COVID-19 infection I′m not really scared of being infected by COVID-19 I prefer to wait until I have more experience with these new vaccines I doubt the efficacy of the vaccine I am afraid of mild side effects (e.g., fever, pain at the injection site) of the vaccine I fear serious side effects (e.g., hospitalisation, serious illness) of the vaccine The media (e.g., TV, radio) have dissuaded me from getting vaccinated I don’t trust pharmaceutical companies I don’t trust public authority Social networks (e.g., Facebook, Twitter) have dissuaded me from getting vaccinated I don’t really understand how the vaccine works The design of the COVID-19 vaccines seems to me to be too fast I prefer to protect myself with barrier gestures (e.g., wearing a mask, using hydroalcoholic solution) | Yes or no |
| Opportunities to change decision | A protection rate of 100% (or almost 100%) A protection rate of at least 80% A duration of immunity of at least 1 year French or European origin of the vaccine A low risk of serious side effects Free vaccine Only one injection (no booster required) A vaccination proposal from my doctor People around me (friends, family, etc.) being vaccinated Encouragement of vaccination by influential personalities/persons in social networks Nothing, I won′t change my decision | Yes or no |
| Variables | COVID-19 Vaccine Acceptance N = 1790 | COVID-19 Vaccine Hesitancy N = 772 | COVID-19 Vaccine Resistancy N = 527 | Total N = 3089 | p |
|---|---|---|---|---|---|
| Age mean (SD) | 20.5 | 20.1 | 20.1 | 20.3 | <0.0001 |
| Women (%) | 67.3 | 78.8 | 74.8 | 71.4 | <0.0001 |
| Years of study | <0.0001 | ||||
| 1 (%) | 26.0 | 41.1 | 40.2 | 32.2 | |
| 2 and 3 (%) | 44.8 | 42.2 | 44.8 | 44.1 | |
| 4 and more (%) | 29.2 | 16.7 | 15.0 | 23.7 | |
| Courses of study Healthcare (%) | 50.8 | 26.7 | 15.6 | 38.8 | <0.0001 |
| Sciences (%) | 16.9 | 22.2 | 21.6 | 19.0 | |
| Neither Science nor Healthcare (%) | 32.3 | 51.2 | 62.8 | 42.2 | |
| COVID-19 | |||||
| Have been Infected (%) | 17.8 | 15.7 | 19.0 | 17.4 | 0.26 |
| Have a Relative been Hospitalized or Died (%) | 15.9 | 16.3 | 16.7 | 16.1 | 0.90 |
| Knowledge | |||||
| Conventional Vaccination Mean (SD) | 6.5 (2.1) | 5.1 (2.3) | 4.8 (2.5) | 5.9 (2.3) | <0.0001 |
| COVID-19 Vaccination Mean (SD) | 5.5 (2.4) | 4.1 (2.3) | 4.4 (2.6) | 4.9 (2.5) | <0.0001 |
| Confidence about Conventional Vaccination | |||||
| Efficacy Mean (SD) | 8.9 (1.3) | 7.2 (2.1) | 5.8 (2.9) | 8.0 (2.3) | <0.0001 |
| Security Mean (SD) | 8.8 (1.4) | 6.8 (2.2) | 5.4 (2.8) | 7.7 (2.3) | <0.0001 |
| Variables | COVID-19 Vaccine Hesitancy ** AOR 95% CI | p | COVID-19 Vaccine Resistancy ** AOR 95% CI | p |
|---|---|---|---|---|
| Age | 1.08 (1.01–1.16) | 0.02 | 1.08 (1.00–1.17) | 0.04 |
| Women | 2.09 (1.69–2.57) | <0.0001 | 1.72 (1.37–2.18) | <0.0001 |
| Years of study | ||||
| 1 | 3.08 (2.13–4.44) | <0.0001 | 3.00 (1.96–4.59) | <0.0001 |
| 2 and 3 | 1.63 (1.22–2.17) | 0.001 | 1.74 (1.25–2.45) | 0.001 |
| 4 and more | Ref | Ref | ||
| Courses of study Healthcare | Ref | Ref | ||
| Sciences | 2.79 (2.17–3.58) | <0.0001 | 4.50 (3.27–6.19) | <0.0001 |
| Neither sciences nor healthcare | 2.92 (2.39–3.59) | <0.0001 | 6.08 (4.65–7.96) | <0.0001 |
| Knowledge | ||||
| Conventional Vaccination | 0.81 (0.78–0.85) | <0.0001 | 0.81 (0.77–0.85) | <0.0001 |
| COVID-19 Vaccination | 0.84 (0.81–0.87) | <0.0001 | 0.90 (0.86–0.94) | <0.0001 |
| Confidence about Conventional Vaccination | ||||
| Efficacy | 0.61 (0.58–0.65) | <0.0001 | 0.50 (0.47–0.53) | <0.0001 |
| Security | 0.57 (0.54–0.60) | <0.0001 | 0.46 (0.43–0.49) | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tavolacci, M.P.; Dechelotte, P.; Ladner, J. COVID-19 Vaccine Acceptance, Hesitancy, and Resistancy among University Students in France. Vaccines 2021, 9, 654. https://doi.org/10.3390/vaccines9060654
Tavolacci MP, Dechelotte P, Ladner J. COVID-19 Vaccine Acceptance, Hesitancy, and Resistancy among University Students in France. Vaccines. 2021; 9(6):654. https://doi.org/10.3390/vaccines9060654
Chicago/Turabian StyleTavolacci, Marie Pierre, Pierre Dechelotte, and Joel Ladner. 2021. "COVID-19 Vaccine Acceptance, Hesitancy, and Resistancy among University Students in France" Vaccines 9, no. 6: 654. https://doi.org/10.3390/vaccines9060654