
Application of Entropy-Based Features to Predict Defibrillation Outcome in Cardiac Arrest

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection and Labeling
2.2. Classical Shock Outcome Predictors
2.3. Shock Outcome Predictors Based on Entropy Measures
2.3.1. Regularity-Based Entropies
2.3.2. Predictability-Based Entropies
2.4. Study of Optimal Parameters to Compute Entropy Measures
2.5. Statistical Analysis
3. Results
3.1. Optimal Parameters to Compute Entropy Measures
3.2. Classical versus Entropy-Based Predictors
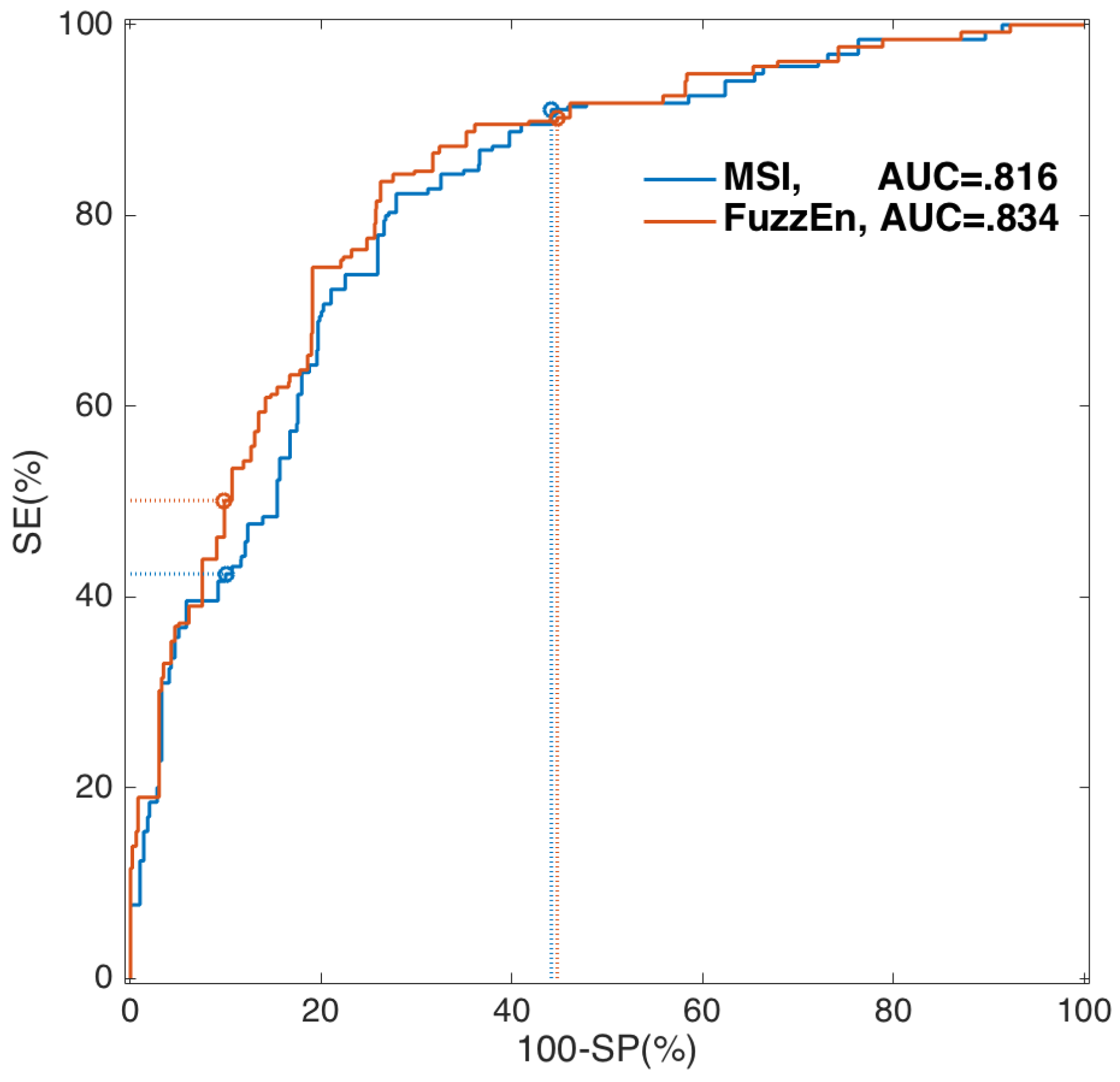
3.3. Optimal Single-Predictor Classifier
4. Discussion and Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Berdowski, J.; Berg, R.A.; Tijssen, J.G.P.; Koster, R.W. Global incidences of out-of-hospital cardiac arrest and survival rates: Systematic review of 67 prospective studies. Resuscitation 2010, 81, 1479–1487. [Google Scholar] [CrossRef] [PubMed]
- Rubart, M.; Zipes, D.P. Mechanisms of sudden cardiac death. J. Clin. Investig. 2005, 115, 2305–2315. [Google Scholar] [CrossRef] [PubMed]
- Zoll, P.M. Resuscitation of the heart in ventricular standstill by external electric stimulation. New Engl. J. Med. 1952, 247, 768–771. [Google Scholar] [CrossRef] [PubMed]
- Perkins, G.D.; Handley, A.J.; Koster, R.W.; Castrén, M.; Smyth, M.A.; Olasveengen, T.; Monsieurs, K.G.; Raffay, V.; Gräsner, J.T.; Wenzel, V.; et al. European Resuscitation Council Guidelines for Resuscitation 2015: Section 2. Adult basic life support and automated external defibrillation. Resuscitation 2015, 95, 81–99. [Google Scholar] [CrossRef] [PubMed]
- Kleinman, M.E.; Brennan, E.E.; Goldberger, Z.D.; Swor, R.A.; Terry, M.; Bobrow, B.J.; Gazmuri, R.J.; Travers, A.H.; Rea, T. Part 5: Adult Basic Life Support and Cardiopulmonary Resuscitation Quality: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2015, 132, S414–S435. [Google Scholar] [CrossRef] [PubMed]
- Rudikoff, M.T.; Maughan, W.L.; Effron, M.; Freund, P.; Weisfeldt, M.L. Mechanisms of blood flow during cardiopulmonary resuscitation. Circulation 1980, 61, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Monsieurs, K.G.; Nolan, J.P.; Bossaert, L.L.; Greif, R.; Maconochie, I.K.; Nikolaou, N.I.; Perkins, G.D.; Soar, J.; Truhlář, A.; Wyllie, J.; et al. European Resuscitation Council Guidelines for Resuscitation 2015: Section 1. Executive summary. Resuscitation 2015, 95, 1–80. [Google Scholar] [CrossRef] [PubMed]
- Neumar, R.W.; Shuster, M.; Callaway, C.W.; Gent, L.M.; Atkins, D.L.; Bhanji, F.; Brooks, S.C.; de Caen, A.R.; Donnino, M.W.; Ferrer, J.M.E.; et al. Part 1: Executive Summary: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2015, 132, S315–S367. [Google Scholar] [CrossRef] [PubMed]
- Ruiz de Gauna, S.; Irusta, U.; Ruiz, J.; Ayala, U.; Aramendi, E.; Eftestøl, T. Rhythm analysis during cardiopulmonary resuscitation: past, present, and future. Biomed. Res. Int. 2014, 2014, 386010. [Google Scholar] [CrossRef] [PubMed]
- Irusta, U.; Ruiz, J.; Aramendi, E.; Ruiz de Gauna, S.; Ayala, U.; Alonso, E. A high-temporal resolution algorithm to discriminate shockable from nonshockable rhythms in adults and children. Resuscitation 2012, 83, 1090–1097. [Google Scholar] [CrossRef] [PubMed]
- Eftestol, T.; Sunde, K.; Ole Aase, S.; Husoy, J.H.; Steen, P.A. Predicting outcome of defibrillation by spectral characterization and nonparametric classification of ventricular fibrillation in patients with out-of-hospital cardiac arrest. Circulation 2000, 102, 1523–1529. [Google Scholar] [CrossRef] [PubMed]
- Ristagno, G.; Mauri, T.; Cesana, G.; Li, Y.; Finzi, A.; Fumagalli, F.; Rossi, G.; Grieco, N.; Migliori, M.; Andreassi, A.; et al. Amplitude spectrum area to guide defibrillation: A validation on 1617 patients with ventricular fibrillation. Circulation 2015, 131, 478–487. [Google Scholar] [CrossRef] [PubMed]
- Xie, J.; Weil, M.H.; Sun, S.; Tang, W.; Sato, Y.; Jin, X.; Bisera, J. High-energy defibrillation increases the severity of postresuscitation myocardial dysfunction. Circulation 1997, 96, 683–688. [Google Scholar] [CrossRef] [PubMed]
- Cheskes, S.; Schmicker, R.H.; Christenson, J.; Salcido, D.D.; Rea, T.; Powell, J.; Edelson, D.P.; Sell, R.; May, S.; Menegazzi, J.J.; et al. Perishock pause: An independent predictor of survival from out-of-hospital shockable cardiac arrest. Circulation 2011, 124, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Weisfeldt, M.L.; Becker, L.B. Resuscitation after cardiac arrest: A 3-phase time-sensitive model. JAMA 2002, 288, 3035–3038. [Google Scholar] [CrossRef] [PubMed]
- Reed, M.J.; Clegg, G.R.; Robertson, C.E. Analysing the ventricular fibrillation waveform. Resuscitation 2003, 57, 11–20. [Google Scholar] [CrossRef]
- Callaway, C.W.; Menegazzi, J.J. Waveform analysis of ventricular fibrillation to predict defibrillation. Curr. Opin. Crit. Care 2005, 11, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Salcido, D.D.; Menegazzi, J.J.; Suffoletto, B.P.; Logue, E.S.; Sherman, L.D. Association of intramyocardial high energy phosphate concentrations with quantitative measures of the ventricular fibrillation electrocardiogram waveform. Resuscitation 2009, 80, 946–950. [Google Scholar] [CrossRef] [PubMed]
- Weaver, W.D.; Cobb, L.A.; Dennis, D.; Ray, R.; Hallstrom, A.P.; Copass, M.K. Amplitude of ventricular fibrillation waveform and outcome after cardiac arrest. Ann. Intern. Med. 1985, 102, 53–55. [Google Scholar] [CrossRef] [PubMed]
- Callaway, C.W.; Sherman, L.D.; Scheatzle, M.D.; Menegazzi, J.J. Scaling structure of electrocardiographic waveform during prolonged ventricular fibrillation in swine. Pacing Clin. Electrophysiol. 2000, 23, 180–191. [Google Scholar] [CrossRef] [PubMed]
- Sherman, L.D.; Rea, T.D.; Waters, J.D.; Menegazzi, J.J.; Callaway, C.W. Logarithm of the absolute correlations of the ECG waveform estimates duration of ventricular fibrillation and predicts successful defibrillation. Resuscitation 2008, 78, 346–354. [Google Scholar] [CrossRef] [PubMed]
- Dzwonczyk, R.; Brown, C.G.; Werman, H.A. The median frequency of the ECG during ventricular fibrillation: Its use in an algorithm for estimating the duration of cardiac arrest. IEEE Trans. Biomed. Eng. 1990, 37, 640–646. [Google Scholar] [CrossRef] [PubMed]
- Neurauter, A.; Eftestøl, T.; Kramer-Johansen, J.; Abella, B.S.; Sunde, K.; Wenzel, V.; Lindner, K.H.; Eilevstjønn, J.; Myklebust, H.; Steen, P.A.; et al. Prediction of countershock success using single features from multiple ventricular fibrillation frequency bands and feature combinations using neural networks. Resuscitation 2007, 73, 253–263. [Google Scholar] [CrossRef] [PubMed]
- Endoh, H.; Hida, S.; Oohashi, S.; Hayashi, Y.; Kinoshita, H.; Honda, T. Prompt prediction of successful defibrillation from 1-s ventricular fibrillation waveform in patients with out-of-hospital sudden cardiac arrest. J. Anesth. 2011, 25, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Firoozabadi, R.; Nakagawa, M.; Helfenbein, E.D.; Babaeizadeh, S. Predicting defibrillation success in sudden cardiac arrest patients. J. Electrocardiol. 2013, 46, 473–479. [Google Scholar] [CrossRef] [PubMed]
- He, M.; Gong, Y.; Li, Y.; Mauri, T.; Fumagalli, F.; Bozzola, M.; Cesana, G.; Latini, R.; Pesenti, A.; Ristagno, G. Combining multiple ECG features does not improve prediction of defibrillation outcome compared to single features in a large population of out-of-hospital cardiac arrests. Crit. Care 2015, 19. [Google Scholar] [CrossRef] [PubMed]
- Marn-Pernat, A.; Weil, M.H.; Tang, W.; Pernat, A.; Bisera, J. Optimizing timing of ventricular defibrillation. Crit. Care Med. 2001, 29, 2360–2365. [Google Scholar] [CrossRef] [PubMed]
- Sherman, L.D.; Callaway, C.W.; Menegazzi, J.J. Ventricular fibrillation exhibits dynamical properties and self-similarity. Resuscitation 2000, 47, 163–173. [Google Scholar] [CrossRef]
- Lin, L.Y.; Lo, M.T.; Ko, P.C.I.; Lin, C.; Chiang, W.C.; Liu, Y.B.; Hu, K.; Lin, J.L.; Chen, W.J.; Ma, M.H.M. Detrended fluctuation analysis predicts successful defibrillation for out-of-hospital ventricular fibrillation cardiac arrest. Resuscitation 2010, 81, 297–301. [Google Scholar] [CrossRef] [PubMed]
- Gong, Y.; Lu, Y.; Zhang, L.; Zhang, H.; Li, Y. Predict Defibrillation Outcome Using Stepping Increment of Poincaree Plot for Out-of-Hospital Ventricular Fibrillation Cardiac Arrest. Biomed. Res. Int. 2015, 2015, 493472. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Zhuang, J.; Yu, W.; Wang, Z. Measuring complexity using FuzzyEn, ApEn, and SampEn. Med. Eng. Phys. 2009, 31, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Liu, C.; Li, K.; Zheng, D.; Liu, C.; Hou, Y. Assessing the complexity of short-term heartbeat interval series by distribution entropy. Med. Biol. Eng. Comput. 2015, 53, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Borowska, M. Entropy-based algorithms in the analysis of biomedical signals. Stud. Log. Gramm. Rhetor. 2015, 43, 21–32. [Google Scholar] [CrossRef]
- Faust, O.; Bairy, M.G. Nonlinear analysis of physiological signals: A review. J. Mech. Med. Biol. 2012, 12, 124005. [Google Scholar] [CrossRef]
- Ibarguren, K.; Unanue, J.M.; Alonso, D.; Vaqueriza, I.; Irusta, U.; Aramendi, E.; Chicote, B. Difference in survival from pre-hospital cardiac arrest between cities and villages in the Basque Autonomous Community. Resuscitation 2015, 96. [Google Scholar] [CrossRef]
- Higuchi, T. Approach to an irregular time series on the basis of the fractal theory. Physica D 1988, 31, 277–283. [Google Scholar] [CrossRef]
- Sherman, L.D.; Flagg, A.; Callaway, C.W.; Menegazzi, J.J.; Hsieh, M. Angular velocity: A new method to improve prediction of ventricular fibrillation duration. Resuscitation 2004, 60, 79–90. [Google Scholar] [CrossRef] [PubMed]
- Pincus, S.M. Approximate entropy as a measure of system complexity. Proc. Natl. Acad. Sci. USA 1991, 88, 2297–2301. [Google Scholar] [CrossRef] [PubMed]
- Amigó, J.M.; Keller, K.; Unakafova, V.A. Ordinal symbolic analysis and its application to biomedical recordings. Philos. Trans. A Math. Phys. Eng. Sci. 2015, 373. [Google Scholar] [CrossRef] [PubMed]
- Richman, J.S.; Moorman, J.R. Physiological time-series analysis using approximate entropy and sample entropy. Am. J. Physiol. Heart Circ. Physiol. 2000, 278, H2039–H2049. [Google Scholar] [PubMed]
- Chen, W.; Wang, Z.; Xie, H.; Yu, W. Characterization of surface EMG signal based on fuzzy entropy. IEEE. Trans. Neural Syst. Rehabil. Eng. 2007, 15, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Bandt, C.; Pompe, B. Permutation entropy: A natural complexity measure for time series. Phys. Rev. Lett. 2002, 88, 174102. [Google Scholar] [CrossRef] [PubMed]
- Porta, A.; Guzzetti, S.; Montano, N.; Furlan, R.; Pagani, M.; Malliani, A.; Cerutti, S. Entropy, entropy rate, and pattern classification as tools to typify complexity in short heart period variability series. IEEE Trans. Biomed. Eng. 2001, 48, 1282–1291. [Google Scholar] [CrossRef] [PubMed]
- Lu, S.; Chen, X.; Kanters, J.K.; Solomon, I.C.; Chon, K.H. Automatic selection of the threshold value R for approximate entropy. IEEE. Trans. Biomed. Eng. 2008, 55, 1966–1972. [Google Scholar] [PubMed]
- Alcaraz, R.; Abásolo, D.; Hornero, R.; Rieta, J.J. Optimal parameters study for sample entropy-based atrial fibrillation organization analysis. Comput. Methods Programs Biomed. 2010, 99, 124–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, A.; Saini, B.S.; Singh, D. An alternative approach to approximate entropy threshold value (r) selection: Application to heart rate variability and systolic blood pressure variability under postural challenge. Med. Biol. Eng. Comput. 2016, 54, 723–732. [Google Scholar] [CrossRef] [PubMed]
- Zanin, M.; Zunino, L.; Rosso, O.A.; Papo, D. Permutation Entropy and Its Main Biomedical and Econophysics Applications: A Review. Entropy 2012, 14, 1553–1577. [Google Scholar] [CrossRef]
- Porta, A.; Baselli, G.; Liberati, D.; Montano, N.; Cogliati, C.; Gnecchi-Ruscone, T.; Malliani, A.; Cerutti, S. Measuring regularity by means of a corrected conditional entropy in sympathetic outflow. Biol. Cybern. 1998, 78, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Zou, K.H.; O’Malley, A.J.; Mauri, L. Receiver-operating characteristic analysis for evaluating diagnostic tests and predictive models. Circulation 2007, 115, 654–657. [Google Scholar] [CrossRef] [PubMed]
- Ben-Hur, A.; Weston, J. A user’s guide to support vector machines. Methods Mol. Biol. 2010, 609, 223–239. [Google Scholar] [PubMed]
- Khandoker, A.H.; Gubbi, J.; Palaniswami, M. Automated scoring of obstructive sleep apnea and hypopnea events using short-term electrocardiogram recordings. IEEE Trans. Inform. Technol. Biomed. 2009, 13, 1057–1067. [Google Scholar] [CrossRef] [PubMed]
- Lillo-Castellano, J.M.; Mora-Jiménez, I.; Santiago-Mozos, R.; Chavarría-Asso, F.; Cano-González, A.; García-Alberola, A.; Rojo-Álvarez, J.L. Symmetrical compression distance for arrhythmia discrimination in cloud-based big-data services. IEEE J. Biomed. Health Inform. 2015, 19, 1253–1263. [Google Scholar] [CrossRef] [PubMed]
- Musicant, D.R.; Kumar, V.; Ozgur, A. Optimizing F-Measure with Support Vector Machines. In Proceedings of the FLAIRS Conference, St. Augustine, FL, USA, 12–14 May 2003; pp. 356–360.
- Sokolova, M.; Japkowicz, N.; Szpakowicz, S. Beyond accuracy, F-score and ROC: A family of discriminant measures for performance evaluation. In AI 2006: Advances in Artificial Intelligence; Springer: Berlin/Heidelberg, Germany, 2006; pp. 1015–1021. [Google Scholar]
- Xiao-Feng, L.; Yue, W. Fine-grained permutation entropy as a measure of natural complexity for time series. Chin. Phys. B 2009, 18. [Google Scholar] [CrossRef]
- Fadlallah, B.; Chen, B.; Keil, A.; Príncipe, J. Weighted-permutation entropy: A complexity measure for time series incorporating amplitude information. Phys. Rev. E 2013, 87, 022911. [Google Scholar] [CrossRef] [PubMed]
- Howe, A.; Escalona, O.J.; di Maio, R.; Massot, B.; Cromie, N.A.; Darragh, K.M.; Adgey, J.; McEneaney, D.J. A support vector machine for predicting defibrillation outcomes from waveform metrics. Resuscitation 2014, 85, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Shandilya, S.; Ward, K.; Kurz, M.; Najarian, K. Non-linear dynamical signal characterization for prediction of defibrillation success through machine learning. BMC Med. Inform. Decis. Mak. 2012, 12. [Google Scholar] [CrossRef] [PubMed]
- He, M.; Lu, Y.; Zhang, L.; Zhang, H.; Gong, Y.; Li, Y. Combining Amplitude Spectrum Area with Previous Shock Information Using Neural Networks Improves Prediction Performance of Defibrillation Outcome for Subsequent Shocks in Out-Of-Hospital Cardiac Arrest Patients. PLoS ONE 2016, 11, e0149115. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Bisera, J.; Tang, W. Signal integral for optimizing the timing of defibrillation. Resuscitation 2013, 84, 1704–1707. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Measure | Optimal Input Parameters |
|---|---|
| ApEn | and V |
| SampEn | and V |
| FuzzEn | and V |
| PerEn | |
| ConEn | and 10 |
| MConEn | and V |
| Predictor | AUC | SE (%) a | SP (%) b |
|---|---|---|---|
| PPA | 0.804 | 41.2 | 50.6 |
| MdS | 0.815 | 41.9 | 56.3 |
| AMSA | 0.806 | 43.9 | 52.3 |
| MSI | 0.816 | 42.4 | 55.9 |
| ScE | 0.778 | 36.5 | 43.4 |
| LAC | 0.726 | 25.9 | 34.2 |
| ApEn | 0.813 | 42.7 | 53.5 |
| SampEn | 0.813 | 40.4 | 53.5 |
| FuzzEn | 0.834 | 50.1 | 55.2 |
| PerEn | 0.550 | 13.1 | 12.8 |
| ConEn | 0.636 | 15.5 | 19.4 |
| MConEn | 0.820 | 46.7 | 55.4 |
| Predictor | BER | SE (%) | SP (%) | PPV (%) | NPV (%) |
|---|---|---|---|---|---|
| PPA | 0.247 | 80.4 | 70.2 | 48.0 | 91.2 |
| MdS | 0.239 | 79.4 | 72.8 | 50.0 | 91.2 |
| AMSA | 0.267 | 74.8 | 71.8 | 47.6 | 89.2 |
| MSI | 0.238 | 80.4 | 72.1 | 49.7 | 91.5 |
| ScE | 0.273 | 83.2 | 62.2 | 43.0 | 91.5 |
| LAC | 0.330 | 75.7 | 58.3 | 38.4 | 87.5 |
| ApEn | 0.220 | 81.3 | 74.7 | 52.4 | 92.1 |
| SampEn | 0.218 | 81.3 | 75.0 | 52.7 | 92.1 |
| FuzzEn | 0.214 | 80.4 | 76.9 | 54.4 | 92.0 |
| PerEn | 0.475 | 37.4 | 67.6 | 28.4 | 75.9 |
| ConEn | 0.436 | 43.0 | 69.9 | 32.9 | 78.1 |
| MConEn | 0.230 | 85.0 | 68.9 | 48.4 | 93.1 |
| Threshold | SE (%) | SP (%) | PPV (%) | NPV (%) |
|---|---|---|---|---|
| Defibrillation Failure | ||||
| 98.5 | 21.1 | 39.4 | 96.3 | |
| 95.6 | 34.7 | 43.2 | 93.9 | |
| 90.3 | 55.2 | 51.2 | 91.6 | |
| Defibrillation Success | ||||
| 19.0 | 98.8 | 89.2 | 70.1 | |
| 36.9 | 95.3 | 80.4 | 74.4 | |
| 50.1 | 90.2 | 72.6 | 77.7 | |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chicote, B.; Irusta, U.; Alcaraz, R.; Rieta, J.J.; Aramendi, E.; Isasi, I.; Alonso, D.; Ibarguren, K. Application of Entropy-Based Features to Predict Defibrillation Outcome in Cardiac Arrest. Entropy 2016, 18, 313. https://doi.org/10.3390/e18090313
Chicote B, Irusta U, Alcaraz R, Rieta JJ, Aramendi E, Isasi I, Alonso D, Ibarguren K. Application of Entropy-Based Features to Predict Defibrillation Outcome in Cardiac Arrest. Entropy. 2016; 18(9):313. https://doi.org/10.3390/e18090313
Chicago/Turabian StyleChicote, Beatriz, Unai Irusta, Raúl Alcaraz, José Joaquín Rieta, Elisabete Aramendi, Iraia Isasi, Daniel Alonso, and Karlos Ibarguren. 2016. "Application of Entropy-Based Features to Predict Defibrillation Outcome in Cardiac Arrest" Entropy 18, no. 9: 313. https://doi.org/10.3390/e18090313