Molecular MRI of Atherosclerosis

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction


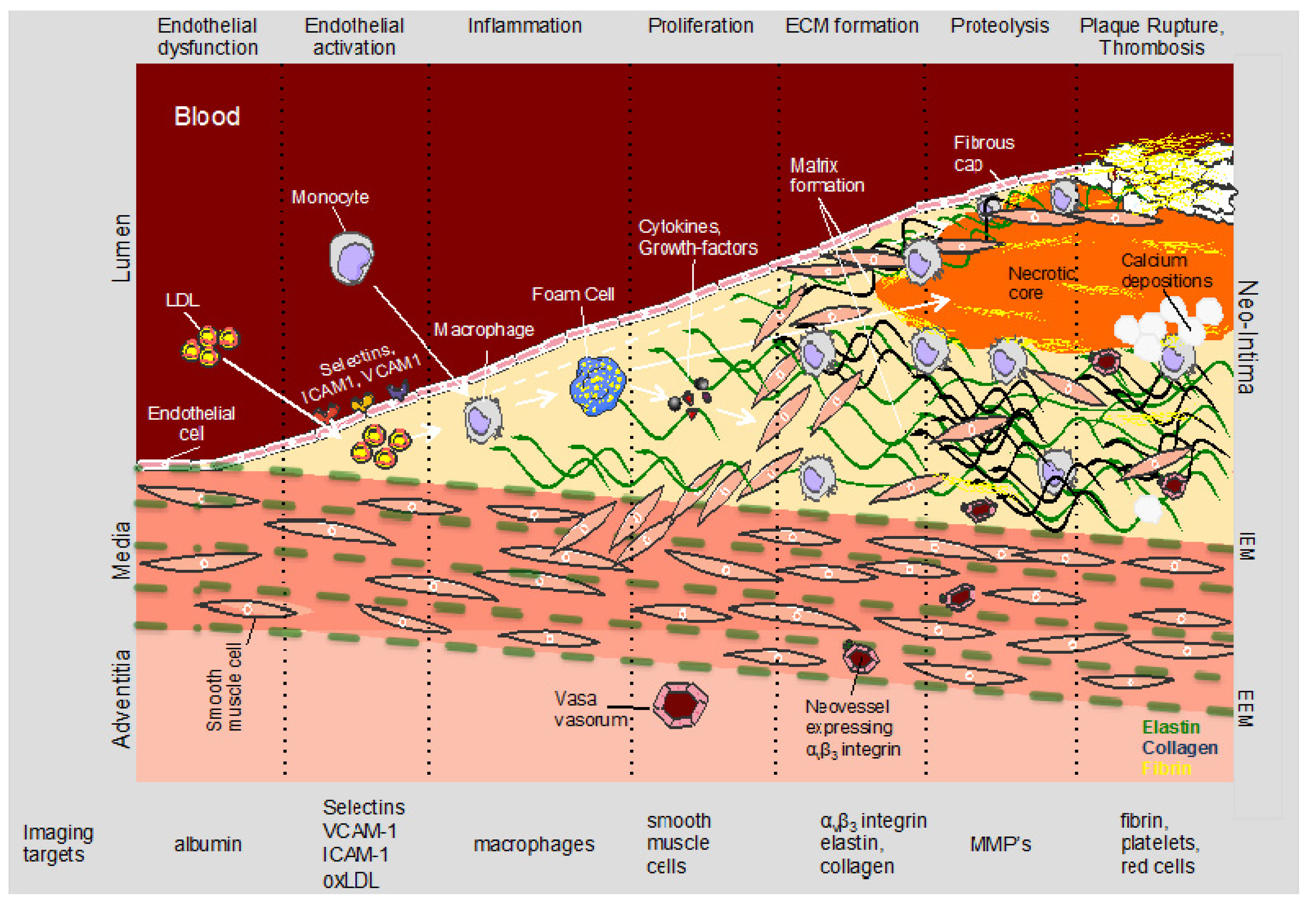
2. Pathophysiology of Atherosclerosis and Molecular Targets
2.1. Endothelial Dysfunction
2.2. Inflammation
2.3. Vascular Remodeling
2.4. Neovascularization and Intraplaque Hemorrhage
2.5. Proteolytic Enzymes
2.6. Fibrin
3. Molecular Imaging Agents
3.1. Probe Detection by MR
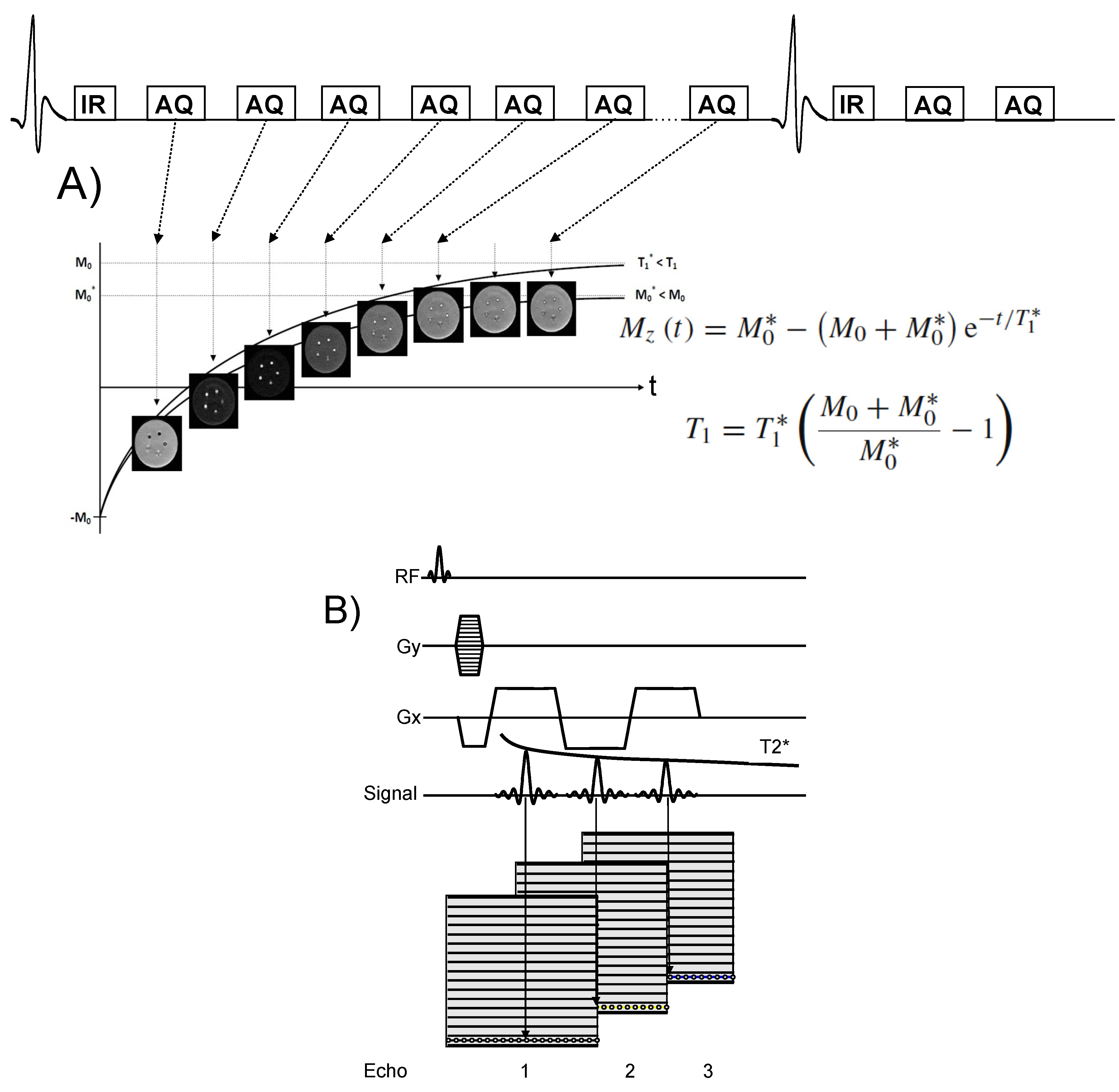
3.2. T1 and T2* Mapping
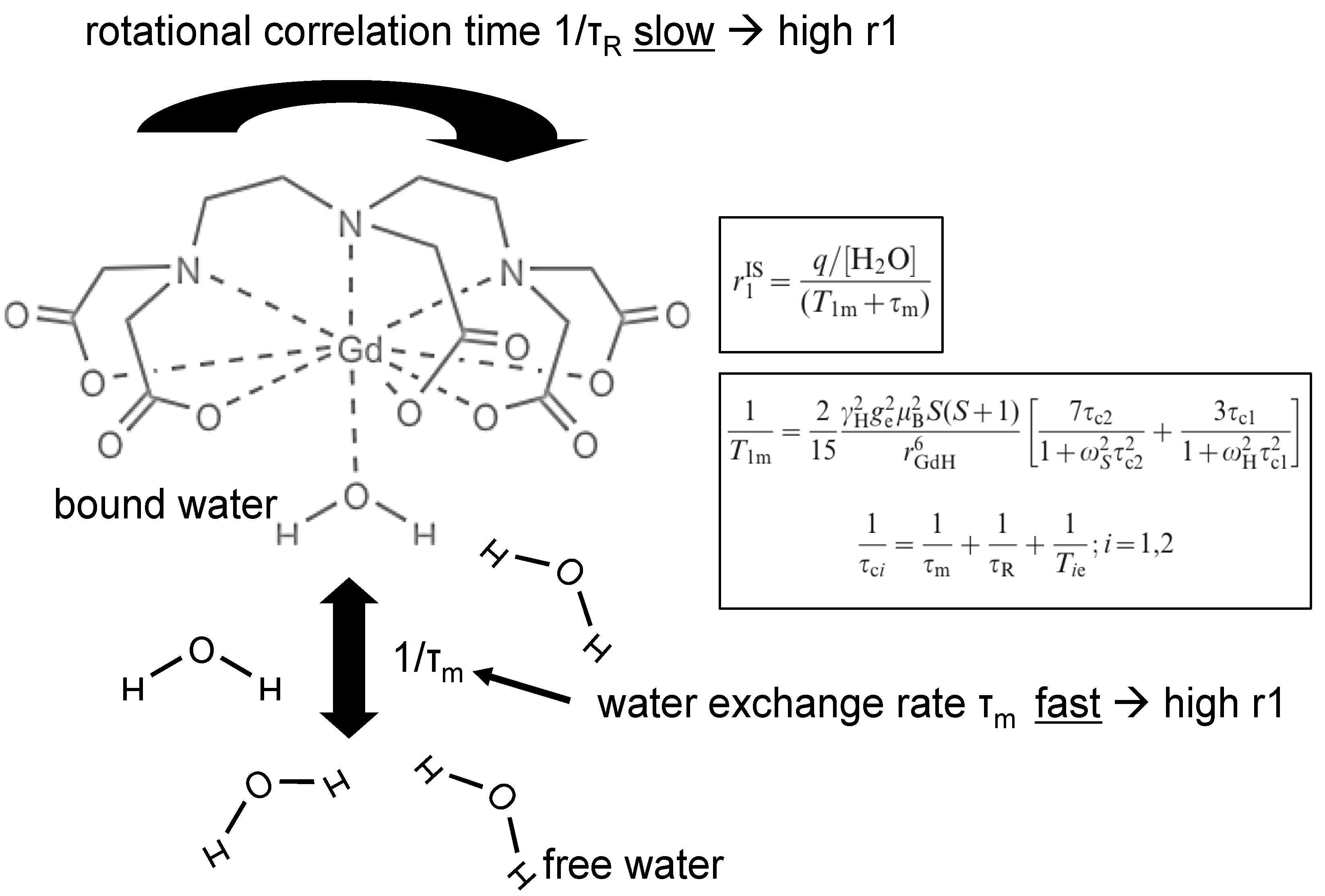
3.3. T1 Contrast Agents


3.4. T2/T2* Contrast Agents

3.5. Mechanism of Targeting
3.5.1. Passive Targeting
3.5.2. Active Targeting
4. Molecular Imaging Applications
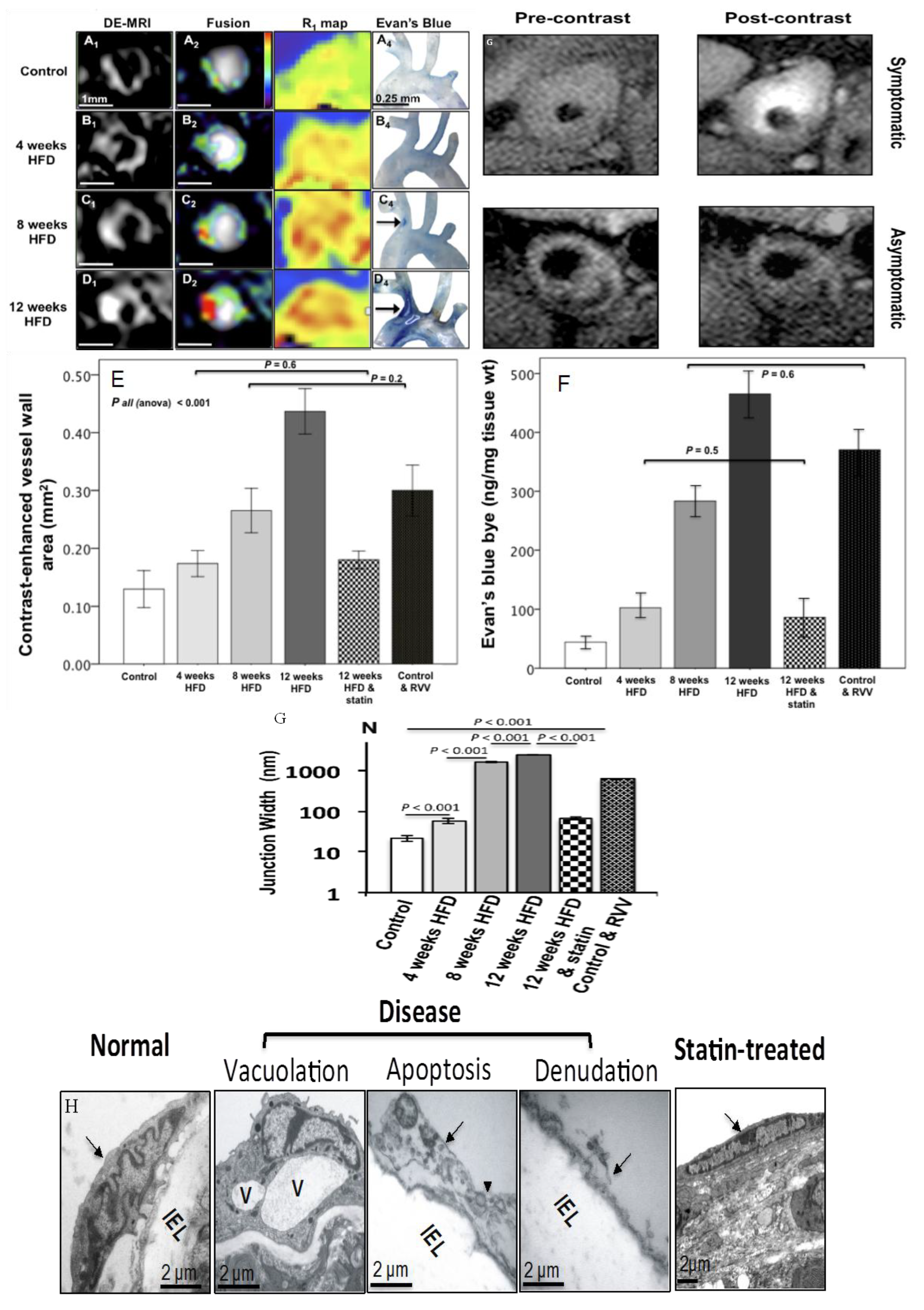
4.1. Endothelial Dysfunction and Activation


4.2. Macrophages

4.3. Extracellular Matrix

4.4. Intraplaque Hemorrhage and Thrombus
4.5. Neovascularization
4.6. Proteolytic Enzymes

4.7. Fibrin

4.8. Lipids
5. Limitations
6. Conclusions
Acknowledgments
Conflicts of Interest
References
- Rosamond, W.; Flegal, K.; Furie, K.; Go, A.; Greenlund, K.; Haase, N.; Hailpern, S.M.; Ho, M.; Howard, V.; Kissela, B.; et al. Heart disease and stroke statistics–2008 update: A report from the american heart association statistics committee and stroke statistics subcommittee. Circulation 2008, 117, e25–e146. [Google Scholar] [CrossRef]
- Lloyd-Jones, D.; Adams, R.; Carnethon, M.; De Simone, G.; Ferguson, T.B.; Flegal, K.; Ford, E.; Furie, K.; Go, A.; Greenlund, K.; et al. Heart disease and stroke statistics–2009 update: A report from the american heart association statistics committee and stroke statistics subcommittee. Circulation 2009, 119, 480–486. [Google Scholar] [CrossRef]
- Virmani, R.; Burke, A.P.; Farb, A.; Kolodgie, F.D. Pathology of the vulnerable plaque. J. Am. Coll. Cardiol. 2006, 47, C13–C18. [Google Scholar] [CrossRef]
- Falk, E. Pathogenesis of atherosclerosis. J. Am. Coll. Cardiol. 2006, 47, C7–C12. [Google Scholar] [CrossRef]
- Narula, J.; Strauss, H.W. The popcorn plaques. Nat. Med. 2007, 13, 532–534. [Google Scholar] [CrossRef]
- Kubo, T.; Imanishi, T.; Takarada, S.; Kuroi, A.; Ueno, S.; Yamano, T.; Tanimoto, T.; Matsuo, Y.; Masho, T.; Kitabata, H.; et al. Assessment of culprit lesion morphology in acute myocardial infarction: Ability of optical coherence tomography compared with intravascular ultrasound and coronary angioscopy. J. Am. Coll. Cardiol. 2007, 50, 933–939. [Google Scholar] [CrossRef]
- Schoenhagen, P.; Ziada, K.M.; Kapadia, S.R.; Crowe, T.D.; Nissen, S.E.; Tuzcu, E.M. Extent and direction of arterial remodeling in stable versus unstable coronary syndromes: An intravascular ultrasound study. Circulation 2000, 101, 598–603. [Google Scholar] [CrossRef]
- Pundziute, G.; Schuijf, J.D.; Jukema, J.W.; Boersma, E.; Scholte, A.J.; Kroft, L.J.; van der Wall, E.E.; Bax, J.J. Noninvasive assessment of plaque characteristics with multislice computed tomography coronary angiography in symptomatic diabetic patients. Diabetes Care 2007, 30, 1113–1119. [Google Scholar] [CrossRef]
- Yeon, S.B.; Sabir, A.; Clouse, M.; Martinezclark, P.O.; Peters, D.C.; Hauser, T.H.; Gibson, C.M.; Nezafat, R.; Maintz, D.; Manning, W.J.; et al. Delayed-enhancement cardiovascular magnetic resonance coronary artery wall imaging: Comparison with multislice computed tomography and quantitative coronary angiography. J. Am. Coll. Cardiol. 2007, 50, 441–447. [Google Scholar] [CrossRef]
- Maintz, D.; Ozgun, M.; Hoffmeier, A.; Fischbach, R.; Kim, W.Y.; Stuber, M.; Manning, W.J.; Heindel, W.; Botnar, R.M. Selective coronary artery plaque visualization and differentiation by contrast-enhanced inversion prepared mri. Eur. Heart J. 2006, 27, 1732–1736. [Google Scholar] [CrossRef]
- Fayad, Z.A.; Fuster, V.; Fallon, J.T.; Jayasundera, T.; Worthley, S.G.; Helft, G.; Aguinaldo, J.G.; Badimon, J.J.; Sharma, S.K. Noninvasive in vivo human coronary artery lumen and wall imaging using black-blood magnetic resonance imaging. Circulation 2000, 102, 506–510. [Google Scholar] [CrossRef]
- Kim, W.Y.; Stuber, M.; Bornert, P.; Kissinger, K.V.; Manning, W.J.; Botnar, R.M. Three-dimensional black-blood cardiac magnetic resonance coronary vessel wall imaging detects positive arterial remodeling in patients with nonsignificant coronary artery disease. Circulation 2002, 106, 296–299. [Google Scholar] [CrossRef]
- Johnson, G.A.; Benveniste, H.; Black, R.D.; Hedlund, L.W.; Maronpot, R.R.; Smith, B.R. Histology by magnetic resonance microscopy. Magn. Reson. Quart. 1993, 9, 1–30. [Google Scholar]
- Hays, A.G.; Hirsch, G.A.; Kelle, S.; Gerstenblith, G.; Weiss, R.G.; Stuber, M. Noninvasive visualization of coronary artery endothelial function in healthy subjects and in patients with coronary artery disease. J. Am. Coll. Cardiol. 2010, 56, 1657–1665. [Google Scholar] [CrossRef]
- Hays, A.G.; Kelle, S.; Hirsch, G.A.; Soleimanifard, S.; Yu, J.; Agarwal, H.K.; Gerstenblith, G.; Schar, M.; Stuber, M.; Weiss, R.G. Regional coronary endothelial function is closely related to local early coronary atherosclerosis in patients with mild coronary artery disease: Pilot study. Circ. Cardiovasc. Imaging 2012, 5, 341–348. [Google Scholar] [CrossRef]
- Phinikaridou, A.; Andia, M.E.; Protti, A.; Indermuehle, A.; Shah, A.; Smith, A.; Warley, A.; Botnar, R.M. Noninvasive magnetic resonance imaging evaluation of endothelial permeability in murine atherosclerosis using an albumin-binding contrast agent. Circulation 2012, 126, 707–719. [Google Scholar] [CrossRef]
- Ross, R. Atherosclerosis—An inflammatory disease. N. Engl. J. Med. 1999, 340, 115–126. [Google Scholar] [CrossRef]
- Libby, P.; Ridker, P.M.; Maseri, A. Inflammation and atherosclerosis. Circulation 2002, 105, 1135–1143. [Google Scholar] [CrossRef]
- Falk, E. Why do plaques rupture? Circulation 1992, 86, II30–II42. [Google Scholar]
- Falk, E.; Shah, P.K.; Fuster, V. Coronary plaque disruption. Circulation 1995, 92, 657–671. [Google Scholar] [CrossRef]
- Welt, F.G.; Rogers, C. Inflammation and restenosis in the stent era. Arterioscler. Thromb. Vasc. Biol. 2002, 22, 1769–1776. [Google Scholar] [CrossRef]
- Jeremias, A.; Spies, C.; Herity, N.A.; Pomerantsev, E.; Yock, P.G.; Fitzgerald, P.J.; Yeung, A.C. Coronary artery compliance and adaptive vessel remodelling in patients with stable and unstable coronary artery disease. Heart 2000, 84, 314–319. [Google Scholar] [CrossRef]
- Katsuda, S.; Kaji, T. Atherosclerosis and extracellular matrix. J. Atheroscler. Thromb. 2003, 10, 267–274. [Google Scholar] [CrossRef]
- Rekhter, M.D. Collagen synthesis in atherosclerosis: Too much and not enough. Cardiovasc. Res. 1999, 41, 376–384. [Google Scholar] [CrossRef]
- Krettek, A.; Sukhova, G.K.; Libby, P. Elastogenesis in human arterial disease: A role for macrophages in disordered elastin synthesis. Arterioscler. Thromb. Vasc. Biol. 2003, 23, 582–587. [Google Scholar] [CrossRef]
- Strauss, B.H.; Chisholm, R.J.; Keeley, F.W.; Gotlieb, A.I.; Logan, R.A.; Armstrong, P.W. Extracellular matrix remodeling after balloon angioplasty injury in a rabbit model of restenosis. Circ. Res. 1994, 75, 650–658. [Google Scholar] [CrossRef]
- Brasselet, C.; Durand, E.; Addad, F.; Al Haj Zen, A.; Smeets, M.B.; Laurent-Maquin, D.; Bouthors, S.; Bellon, G.; de Kleijn, D.; Godeau, G.; et al. Collagen and elastin cross-linking: A mechanism of constrictive remodeling after arterial injury. Am. J. Physiol. Heart Circ. Physiol. 2005, 289, H2228–H2233. [Google Scholar] [CrossRef]
- Stone, G.W.; Maehara, A.; Lansky, A.J.; de Bruyne, B.; Cristea, E.; Mintz, G.S.; Mehran, R.; McPherson, J.; Farhat, N.; Marso, S.P.; et al. A prospective natural-history study of coronary atherosclerosis. N. Engl. J. Med. 2011, 364, 226–235. [Google Scholar] [CrossRef]
- Calvert, P.A.; Obaid, D.R.; O'Sullivan, M.; Shapiro, L.M.; McNab, D.; Densem, C.G.; Schofield, P.M.; Braganza, D.; Clarke, S.C.; Ray, K.K.; et al. Association between ivus findings and adverse outcomes in patients with coronary artery disease: The viva (vh-ivus in vulnerable atherosclerosis) study. J. Am. Coll. Cardiol. Img. 2011, 4, 894–901. [Google Scholar] [CrossRef]
- Motoyama, S.; Sarai, M.; Harigaya, H.; Anno, H.; Inoue, K.; Hara, T.; Naruse, H.; Ishii, J.; Hishida, H.; Wong, N.D.; et al. Computed tomographic angiography characteristics of atherosclerotic plaques subsequently resulting in acute coronary syndrome. J. Am. Coll. Cardiol. 2009, 54, 49–57. [Google Scholar] [CrossRef]
- Sluimer, J.C.; Kolodgie, F.D.; Bijnens, A.P.; Maxfield, K.; Pacheco, E.; Kutys, B.; Duimel, H.; Frederik, P.M.; van Hinsbergh, V.W.; Virmani, R.; et al. Thin-walled microvessels in human coronary atherosclerotic plaques show incomplete endothelial junctions relevance of compromised structural integrity for intraplaque microvascular leakage. J. Am. Coll. Cardiol. 2009, 53, 1517–1527. [Google Scholar] [CrossRef]
- Lee, R.T.; Schoen, F.J.; Loree, H.M.; Lark, M.W.; Libby, P. Circumferential stress and matrix metalloproteinase 1 in human coronary atherosclerosis. Implications for plaque rupture. Arterioscler. Thromb. Vasc. Biol. 1996, 16, 1070–1073. [Google Scholar] [CrossRef]
- Hansson, G.K.; Robertson, A.K.; Soderberg-Naucler, C. Inflammation and atherosclerosis. Annu. Rev. Pathol. 2006, 1, 297–329. [Google Scholar] [CrossRef]
- Kolodgie, F.D.; Gold, H.K.; Burke, A.P.; Fowler, D.R.; Kruth, H.S.; Weber, D.K.; Farb, A.; Guerrero, L.J.; Hayase, M.; Kutys, R.; et al. Intraplaque hemorrhage and progression of coronary atheroma. N. Engl. J. Med. 2003, 349, 2316–2325. [Google Scholar] [CrossRef]
- Tavora, F.; Cresswell, N.; Li, L.; Ripple, M.; Burke, A. Immunolocalisation of fibrin in coronary atherosclerosis: Implications for necrotic core development. Pathology 2010, 42, 15–22. [Google Scholar] [CrossRef]
- Gossl, M.; Versari, D.; Mannheim, D.; Ritman, E.L.; Lerman, L.O.; Lerman, A. Increased spatial vasa vasorum density in the proximal lad in hypercholesterolemia—implications for vulnerable plaque-development. Atherosclerosis 2007, 192, 246–252. [Google Scholar] [CrossRef]
- Cheruvu, P.K.; Finn, A.V.; Gardner, C.; Caplan, J.; Goldstein, J.; Stone, G.W.; Virmani, R.; Muller, J.E. Frequency and distribution of thin-cap fibroatheroma and ruptured plaques in human coronary arteries: A pathologic study. J. Am. Coll. Cardiol. 2007, 50, 940–949. [Google Scholar] [CrossRef]
- Virmani, R.; Kolodgie, F.D.; Burke, A.P.; Finn, A.V.; Gold, H.K.; Tulenko, T.N.; Wrenn, S.P.; Narula, J. Atherosclerotic plaque progression and vulnerability to rupture: Angiogenesis as a source of intraplaque hemorrhage. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 2054–2061. [Google Scholar] [CrossRef]
- Dollery, C.M.; Libby, P. Atherosclerosis and proteinase activation. Cardiovasc. Res. 2006, 69, 625–635. [Google Scholar] [CrossRef]
- Newby, A.C. Metalloproteinase expression in monocytes and macrophages and its relationship to atherosclerotic plaque instability. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 2108–2114. [Google Scholar] [CrossRef]
- Re, G.; Azzimondi, G.; Lanzarini, C.; Bassein, L.; Vaona, I.; Guarnieri, C. Plasma lipoperoxidative markers in ischaemic stroke suggest brain embolism. Eur. J. Emerg. Med. 1997, 4, 5–9. [Google Scholar]
- Brennan, M.L.; Penn, M.S.; Van Lente, F.; Nambi, V.; Shishehbor, M.H.; Aviles, R.J.; Goormastic, M.; Pepoy, M.L.; McErlean, E.S.; Topol, E.J.; et al. Prognostic value of myeloperoxidase in patients with chest pain. N. Engl. J. Med. 2003, 349, 1595–1604. [Google Scholar] [CrossRef]
- Sugiyama, S.; Okada, Y.; Sukhova, G.K.; Virmani, R.; Heinecke, J.W.; Libby, P. Macrophage myeloperoxidase regulation by granulocyte macrophage colony-stimulating factor in human atherosclerosis and implications in acute coronary syndromes. Am. J. Pathol. 2001, 158, 879–891. [Google Scholar] [CrossRef]
- Xiao, Q.; Danton, M.J.; Witte, D.P.; Kowala, M.C.; Valentine, M.T.; Degen, J.L. Fibrinogen deficiency is compatible with the development of atherosclerosis in mice. J. Clin Invest. 1998, 101, 1184–1194. [Google Scholar] [CrossRef]
- Bini, A.; Fenoglio, J.J., Jr.; Mesa-Tejada, R.; Kudryk, B.; Kaplan, K.L. Identification and distribution of fibrinogen, fibrin, and fibrin(ogen) degradation products in atheroscleros. Use of monoclonal antibodies. Arteriosclerosis 1989, 9, 109–121. [Google Scholar] [CrossRef]
- Sirol, M.; Itskovich, V.V.; Mani, V.; Aguinaldo, J.G.; Fallon, J.T.; Misselwitz, B.; Weinmann, H.J.; Fuster, V.; Toussaint, J.F.; Fayad, Z.A. Lipid-rich atherosclerotic plaques detected by gadofluorine-enhanced in vivo magnetic resonance imaging. Circulation 2004, 109, 2890–2896. [Google Scholar] [CrossRef]
- Weinmann, H.J.; Brasch, R.C.; Press, W.R.; Wesbey, G.E. Characteristics of gadolinium-dtpa complex: A potential nmr contrast agent. Am. J. Roentgenol 1984, 142, 619–624. [Google Scholar] [CrossRef]
- Laniado, M.; Weinmann, H.J.; Schorner, W.; Felix, R.; Speck, U. First use of gddtpa/dimeglumine in man. Physiol. Chem. Phys. Med. NMR 1984, 16, 157–165. [Google Scholar]
- Caravan, P.; Ellison, J.J.; McMurry, T.J.; Lauffer, R.B. Gadolinium(iii) chelates as mri contrast agents: Structure, dynamics, and applications. Chem. Rev. 1999, 99, 2293–2352. [Google Scholar] [CrossRef]
- Weissleder, R.; Elizondo, G.; Wittenberg, J.; Rabito, C.A.; Bengele, H.H.; Josephson, L. Ultrasmall superparamagnetic iron oxide: Characterization of a new class of contrast agents for mr imaging. Radiology 1990, 175, 489–493. [Google Scholar]
- Blume, U.; Orbell, J.; Waltham, M.; Smith, A.; Razavi, R.; Schaeffter, T. 3D T(1)-mapping for the characterization of deep vein thrombosis. Magn. Reson. Mater. Phys. Biol. Med. 2009, 22, 375–383. [Google Scholar] [CrossRef]
- Deoni, S.C.; Rutt, B.K.; Peters, T.M. Rapid combined t1 and t2 mapping using gradient recalled acquisition in the steady state. Magn. Reson. Med. 2003, 49, 515–526. [Google Scholar] [CrossRef]
- Bach-Gansmo, T. Ferrimagnetic susceptibility contrast agents. Acta Radiol. Suppl. 1993, 387, 1–30. [Google Scholar]
- Nivorozhkin, A.L.; Kolodziej, A.F.; Caravan, P.; Greenfield, M.T.; Lauffer, R.B.; McMurry, T.J. Enzyme-activated gd(3+) magnetic resonance imaging contrast agents with a prominent receptor-induced magnetization enhancement. Angew. Chem. Int. Ed. Engl. 2001, 40, 2903–2906. [Google Scholar] [CrossRef]
- Caravan, P. Strategies for increasing the sensitivity of gadolinium based mri contrast agents. Chem. Soc. Rev. 2006, 35, 512–523. [Google Scholar] [CrossRef]
- Solomon, I. Relaxation processes in a system of 2 spins. Phys. Rev. 1955, 99, 559–565. [Google Scholar] [CrossRef]
- Caravan, P.; Farrar, C.T.; Frullano, L.; Uppal, R. Influence of molecular parameters and increasing magnetic field strength on relaxivity of gadolinium- and manganese-based t(1) contrast agents. Contrast. Media. Mol. Imaging 2009, 4, 89–100. [Google Scholar] [CrossRef]
- Ferrucci, J.T.; Stark, D.D. Iron oxide-enhanced mr imaging of the liver and spleen: Review of the first 5 years. Am. J. Roentgenol. 1990, 155, 943–950. [Google Scholar] [CrossRef]
- Small, W.C.; Nelson, R.C.; Bernardino, M.E. Dual contrast enhancement of both t1- and t2-weighted sequences using ultrasmall superparamagnetic iron oxide. Magn. Reson. Imaging 1993, 11, 645–654. [Google Scholar] [CrossRef]
- Taupitz, M.; Wagner, S.; Schnorr, J.; Kravec, I.; Pilgrimm, H.; Bergmann-Fritsch, H.; Hamm, B. Phase i clinical evaluation of citrate-coated monocrystalline very small superparamagnetic iron oxide particles as a new contrast medium for magnetic resonance imaging. Invest. Radiol 2004, 39, 394–405. [Google Scholar] [CrossRef]
- von Bary, C.; Preissel, A.; Wagner, S.; Makowski, M.; Schachoff, S.; Keithahn, A.; Spuentrup, E.; Schoemig, A.; Robinson, S.; Lazewatsky, J.; et al. 211 MRI of coronary vessel wall injury in a swine model of coronary intervention using an eletrostatically stabilized vsop nanoparticle. J. Cardiovasc. Magn. Resonance 2008, 10 (Suppl. 1), A72. [Google Scholar] [CrossRef]
- Choudhury, R.P.; Fuster, V.; Fayad, Z.A. Molecular, cellular and functional imaging of atherothrombosis. Nat. Rev. Drug Discov. 2004, 3, 913–925. [Google Scholar] [CrossRef]
- Pouliquen, D.; Le Jeune, J.J.; Perdrisot, R.; Ermias, A.; Jallet, P. Iron oxide nanoparticles for use as an mri contrast agent: Pharmacokinetics and metabolism. Magn. Reson. Imaging 1991, 9, 275–283. [Google Scholar] [CrossRef]
- Schmitz, S.A.; Coupland, S.E.; Gust, R.; Winterhalter, S.; Wagner, S.; Kresse, M.; Semmler, W.; Wolf, K.J. Superparamagnetic iron oxide-enhanced mri of atherosclerotic plaques in watanabe hereditable hyperlipidemic rabbits. Invest. Radiol. 2000, 35, 460–471. [Google Scholar] [CrossRef]
- Taupitz, M.; Schnorr, J.; Abramjuk, C.; Wagner, S.; Pilgrimm, H.; Hunigen, H.; Hamm, B. New generation of monomer-stabilized very small superparamagnetic iron oxide particles (vsop) as contrast medium for mr angiography: Preclinical results in rats and rabbits. J. Magn. Reson. Imaging 2000, 12, 905–911. [Google Scholar] [CrossRef]
- Ruehm, S.G.; Corot, C.; Vogt, P.; Kolb, S.; Debatin, J.F. Magnetic resonance imaging of atherosclerotic plaque with ultrasmall superparamagnetic particles of iron oxide in hyperlipidemic rabbits. Circulation 2001, 103, 415–422. [Google Scholar] [CrossRef]
- Kooi, M.E.; Cappendijk, V.C.; Cleutjens, K.B.; Kessels, A.G.; Kitslaar, P.J.; Borgers, M.; Frederik, P.M.; Daemen, M.J.; van Engelshoven, J.M. Accumulation of ultrasmall superparamagnetic particles of iron oxide in human atherosclerotic plaques can be detected by in vivo magnetic resonance imaging. Circulation 2003, 107, 2453–2458. [Google Scholar] [CrossRef]
- Pirko, I.; Johnson, A.; Ciric, B.; Gamez, J.; Macura, S.I.; Pease, L.R.; Rodriguez, M. In vivo magnetic resonance imaging of immune cells in the central nervous system with superparamagnetic antibodies. Faseb J. 2004, 18, 179–182. [Google Scholar]
- Yuan, C.; Kerwin, W.S.; Ferguson, M.S.; Polissar, N.; Zhang, S.; Cai, J.; Hatsukami, T.S. Contrast-enhanced high resolution mri for atherosclerotic carotid artery tissue characterization. J. Magn. Reson. Imaging 2002, 15, 62–67. [Google Scholar] [CrossRef]
- Kramer, C.M.; Cerilli, L.A.; Hagspiel, K.; DiMaria, J.M.; Epstein, F.H.; Kern, J.A. Magnetic resonance imaging identifies the fibrous cap in atherosclerotic abdominal aortic aneurysm. Circulation 2004, 109, 1016–1021. [Google Scholar] [CrossRef]
- Weinmann, H.J.; Ebert, W.; Misselwitz, B.; Schmitt-Willich, H. Tissue-specific mr contrast agents. Eur J. Radiol. 2003, 46, 33–44. [Google Scholar] [CrossRef]
- Lobbes, M.B.; Heeneman, S.; Passos, V.L.; Welten, R.; Kwee, R.M.; van der Geest, R.J.; Wiethoff, A.J.; Caravan, P.; Misselwitz, B.; Daemen, M.J.; et al. Gadofosveset-enhanced magnetic resonance imaging of human carotid atherosclerotic plaques: A proof-of-concept study. Invest. Radiol. 2010, 45, 275–281. [Google Scholar] [CrossRef]
- Jaffer, F.A.; Nahrendorf, M.; Sosnovik, D.; Kelly, K.A.; Aikawa, E.; Weissleder, R. Cellular imaging of inflammation in atherosclerosis using magnetofluorescent nanomaterials. Mol. Imaging 2006, 5, 85–92. [Google Scholar]
- McAteer, M.A.; Schneider, J.E.; Ali, Z.A.; Warrick, N.; Bursill, C.A.; von zur Muhlen, C.; Greaves, D.R.; Neubauer, S.; Channon, K.M.; Choudhury, R.P. Magnetic resonance imaging of endothelial adhesion molecules in mouse atherosclerosis using dual-targeted microparticles of iron oxide. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 77–83. [Google Scholar]
- Mulder, W.J.; Strijkers, G.J.; Griffioen, A.W.; van Bloois, L.; Molema, G.; Storm, G.; Koning, G.A.; Nicolay, K. A liposomal system for contrast-enhanced magnetic resonance imaging of molecular targets. Bioconjug. Chem. 2004, 15, 799–806. [Google Scholar] [CrossRef]
- Nahrendorf, M.; Jaffer, F.A.; Kelly, K.A.; Sosnovik, D.E.; Aikawa, E.; Libby, P.; Weissleder, R. Noninvasive vascular cell adhesion molecule-1 imaging identifies inflammatory activation of cells in atherosclerosis. Circulation 2006, 114, 1504–1511. [Google Scholar] [CrossRef]
- Mulder, W.J.; Strijkers, G.J.; Briley-Saboe, K.C.; Frias, J.C.; Aguinaldo, J.G.; Vucic, E.; Amirbekian, V.; Tang, C.; Chin, P.T.; Nicolay, K.; et al. Molecular imaging of macrophages in atherosclerotic plaques using bimodal peg-micelles. Magn. Reson. Med. 2007, 58, 1164–1170. [Google Scholar] [CrossRef]
- Amirbekian, V.; Lipinski, M.J.; Briley-Saebo, K.C.; Amirbekian, S.; Aguinaldo, J.G.; Weinreb, D.B.; Vucic, E.; Frias, J.C.; Hyafil, F.; Mani, V.; et al. Detecting and assessing macrophages in vivo to evaluate atherosclerosis noninvasively using molecular mri. Proc. Natl. Acad. Sci. USA 2007, 104, 961–966. [Google Scholar] [CrossRef]
- Korosoglou, G.; Weiss, R.G.; Kedziorek, D.A.; Walczak, P.; Gilson, W.D.; Schar, M.; Sosnovik, D.E.; Kraitchman, D.L.; Boston, R.C.; Bulte, J.W.; et al. Noninvasive detection of macrophage-rich atherosclerotic plaque in hyperlipidemic rabbits using “positive contrast” magnetic resonance imaging. J. Am. Coll. Cardiol. 2008, 52, 483–491. [Google Scholar] [CrossRef]
- Makowski, M.R.; Wiethoff, A.J.; Blume, U.; Cuello, F.; Warley, A.; Jansen, C.H.; Nagel, E.; Razavi, R.; Onthank, D.C.; Cesati, R.R.; et al. Assessment of atherosclerotic plaque burden with an elastin-specific magnetic resonance contrast agent. Nat. Med. 2011, 17, 383–388. [Google Scholar] [CrossRef]
- von Bary, C.; Makowski, M.; Preissel, A.; Keithahn, A.; Warley, A.; Spuentrup, E.; Buecker, A.; Lazewatsky, J.; Cesati, R.; Onthank, D.; et al. Mri of coronary wall remodeling in a swine model of coronary injury using an elastin-binding contrast agent. Circ. Cardiovasc. Imaging 2011, 4, 147–155. [Google Scholar] [CrossRef]
- Sanders, H.M.; Strijkers, G.J.; Mulder, W.J.; Huinink, H.P.; Erich, S.J.; Adan, O.C.; Sommerdijk, N.A.; Merkx, M.; Nicolay, K. Morphology, binding behavior and mr-properties of paramagnetic collagen-binding liposomes. Contrast Media Mol. Imaging 2009, 4, 81–88. [Google Scholar] [CrossRef]
- Klink, A.; Heynens, J.; Herranz, B.; Lobatto, M.E.; Arias, T.; Sanders, H.M.; Strijkers, G.J.; Merkx, M.; Nicolay, K.; Fuster, V.; et al. In vivo characterization of a new abdominal aortic aneurysm mouse model with conventional and molecular magnetic resonance imaging. J. Am. Coll. Cardiol. 2011, 58, 2522–2530. [Google Scholar] [CrossRef]
- Chen, W.; Cormode, D.P.; Vengrenyuk, Y.; Herranz, B.; Feig, J.E.; Klink, A.; Mulder, W.J.; Fisher, E.A.; Fayad, Z.A. Collagen-specific peptide conjugated hdl nanoparticles as mri contrast agent to evaluate compositional changes in atherosclerotic plaque regression. JACC Cardiovasc. Imaging 2013, 6, 373–384. [Google Scholar] [CrossRef]
- Moody, A.R. Magnetic resonance direct thrombus imaging. J. Thromb. Haemost. 2003, 1, 1403–1409. [Google Scholar] [CrossRef]
- Moody, A.R.; Murphy, R.E.; Morgan, P.S.; Martel, A.L.; Delay, G.S.; Allder, S.; MacSweeney, S.T.; Tennant, W.G.; Gladman, J.; Lowe, J.; et al. Characterization of complicated carotid plaque with magnetic resonance direct thrombus imaging in patients with cerebral ischemia. Circulation 2003, 107, 3047–3052. [Google Scholar] [CrossRef]
- Murphy, R.E.; Moody, A.R.; Morgan, P.S.; Martel, A.L.; Delay, G.S.; Allder, S.; MacSweeney, S.T.; Tennant, W.G.; Gladman, J.; Lowe, J.; et al. Prevalence of complicated carotid atheroma as detected by magnetic resonance direct thrombus imaging in patients with suspected carotid artery stenosis and previous acute cerebral ischemia. Circulation 2003, 107, 3053–3058. [Google Scholar] [CrossRef]
- van Beek, E.J.; Wild, J.M.; Fink, C.; Moody, A.R.; Kauczor, H.U.; Oudkerk, M. Mri for the diagnosis of pulmonary embolism. J. Magn. Reson. Imaging 2003, 18, 627–640. [Google Scholar] [CrossRef]
- Toussaint, J.F.; LaMuraglia, G.M.; Southern, J.F.; Fuster, V.; Kantor, H.L. Magnetic resonance images lipid, fibrous, calcified, hemorrhagic, and thrombotic components of human atherosclerosis in vivo. Circulation 1996, 94, 932–938. [Google Scholar] [CrossRef]
- Yuan, C.; Petty, C.; O’Brien, K.D.; Hatsukami, T.S.; Eary, J.F.; Brown, B.G. In vitro and in situ magnetic resonance imaging signal features of atherosclerotic plaque-associated lipids. Arterioscler. Thromb. Vasc. Biol. 1997, 17, 1496–1503. [Google Scholar] [CrossRef]
- Fayad, Z.A.; Fallon, J.T.; Shinnar, M.; Wehrli, S.; Dansky, H.M.; Poon, M.; Badimon, J.J.; Charlton, S.A.; Fisher, E.A.; Breslow, J.L.; et al. Noninvasive in vivo high-resolution magnetic resonance imaging of atherosclerotic lesions in genetically engineered mice. Circulation 1998, 98, 1541–1547. [Google Scholar] [CrossRef]
- Rapoport, S.; Sostman, H.D.; Pope, C.; Camputaro, C.M.; Holcomb, W.; Gore, J.C. Venous clots: Evaluation with mr imaging. Radiology 1987, 162, 527–530. [Google Scholar]
- Moody, A.R.; Morgan, P.S.; Fraser, D.; Hunt, B.J. T1 Reducing Properties of Methaemoglobin: Application to Direct MR Thrombus Imaging. In Proceedings of the ISMRM 8th scientific meeting, Denver, CO, USA, 2000.
- McGuinness, C.L.; Humphries, J.; Waltham, M.; Burnand, K.G.; Collins, M.; Smith, A. Recruitment of labelled monocytes by experimental venous thrombi. Thromb. Haemost. 2001, 85, 1018–1024. [Google Scholar]
- Modarai, B.; Burnand, K.G.; Humphries, J.; Waltham, M.; Smith, A. The role of neovascularisation in the resolution of venous thrombus. Thromb. Haemost. 2005, 93, 801–809. [Google Scholar]
- Fraser, D.G.W.; Moody, A.R.; Morgan, P.S.; Martel, A.L.; Davidson, I. Diagnosis of lower-limb deep venous thrombosis: A prospective blinded study of magnetic resonance direct thrombus imaging. Ann. Intern. Med. 2002, 136, 89–98. [Google Scholar]
- Moody, A.R. Direct imaging of deep-vein thrombosis with magnetic resonance imaging. Lancet 1997, 350, 1073–1073. [Google Scholar] [CrossRef]
- Kelly, J.; Hunt, B.J.; Moody, A. Magnetic resonance direct thrombus imaging: A novel technique for imaging venous thromboemboli. Thromb. Haemost. 2003, 89, 773–782. [Google Scholar]
- Moody, A.R.; Pollock, J.G.; O’Connor, A.R.; Bagnall, M. Lower-limb deep venous thrombosis: Direct mr imaging of the thrombus. Radiology 1998, 209, 349–355. [Google Scholar]
- Schmitz, S.A.; O'Regan, D.P.; Gibson, D.; Cunningham, C.; Fitzpatrick, J.; Allsop, J.; Larkman, D.J.; Hajnal, J.V. Magnetic resonance direct thrombus imaging at 3 t field strength in patients with lower limb deep vein thrombosis: A feasibility study. Clin. Radiol. 2006, 61, 282–286. [Google Scholar] [CrossRef]
- Saha, P.; Andia, M.E.; Modarai, B.; Blume, U.; Humphries, J.; Patel, A.S.; Phinikaridou, A.; Evans, C.E.; Mattock, K.; Grover, S.P.; et al. Magnetic resonance t1 relaxation time of venous thrombus is determined by iron processing and predicts susceptibility to lysis. Circulation 2013, 128, 729–736. [Google Scholar] [CrossRef]
- Griffioen, A.W.; Molema, G. Angiogenesis: Potentials for pharmacologic intervention in the treatment of cancer, cardiovascular diseases, and chronic inflammation. Pharmacol. Rev. 2000, 52, 237–268. [Google Scholar]
- Purushothaman, K.R.; Sanz, J.; Zias, E.; Fuster, V.; Moreno, P.R. Atherosclerosis neovascularization and imaging. Curr. Mol. Med. 2006, 6, 549–556. [Google Scholar] [CrossRef]
- Libby, P. Inflammation in atherosclerosis. Nature 2002, 420, 868–874. [Google Scholar] [CrossRef]
- Winter, P.M.; Neubauer, A.M.; Caruthers, S.D.; Harris, T.D.; Robertson, J.D.; Williams, T.A.; Schmieder, A.H.; Hu, G.; Allen, J.S.; Lacy, E.K.; et al. Endothelial alpha(v)beta3 integrin-targeted fumagillin nanoparticles inhibit angiogenesis in atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 2006, 26, 2103–2109. [Google Scholar] [CrossRef]
- Cai, K.; Caruthers, S.D.; Huang, W.; Williams, T.A.; Zhang, H.; Wickline, S.A.; Lanza, G.M.; Winter, P.M. Mr molecular imaging of aortic angiogenesis. JACC Cardiovasc. Imaging 2010, 3, 824–832. [Google Scholar] [CrossRef]
- Kerwin, W.S.; O’Brien, K.D.; Ferguson, M.S.; Polissar, N.; Hatsukami, T.S.; Yuan, C. Inflammation in carotid atherosclerotic plaque: A dynamic contrast-enhanced mr imaging study. Radiology 2006, 241, 459–468. [Google Scholar] [CrossRef]
- Lancelot, E.; Amirbekian, V.; Brigger, I.; Raynaud, J.S.; Ballet, S.; David, C.; Rousseaux, O.; Le Greneur, S.; Port, M.; Lijnen, H.R.; et al. Evaluation of matrix metalloproteinases in atherosclerosis using a novel noninvasive imaging approach. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 425–432. [Google Scholar] [CrossRef]
- Hyafil, F.; Vucic, E.; Cornily, J.C.; Sharma, R.; Amirbekian, V.; Blackwell, F.; Lancelot, E.; Corot, C.; Fuster, V.; Galis, Z.S.; et al. Monitoring of arterial wall remodelling in atherosclerotic rabbits with a magnetic resonance imaging contrast agent binding to matrix metalloproteinases. Eur. Heart J. 2011, 32, 1561–1571. [Google Scholar] [CrossRef]
- Ronald, J.A.; Chen, J.W.; Chen, Y.; Hamilton, A.M.; Rodriguez, E.; Reynolds, F.; Hegele, R.A.; Rogers, K.A.; Querol, M.; Bogdanov, A.; et al. Enzyme-sensitive magnetic resonance imaging targeting myeloperoxidase identifies active inflammation in experimental rabbit atherosclerotic plaques. Circulation 2009, 120, 592–599. [Google Scholar] [CrossRef]
- Yu, X.; Song, S.K.; Chen, J.; Scott, M.J.; Fuhrhop, R.J.; Hall, C.S.; Gaffney, P.J.; Wickline, S.A.; Lanza, G.M. High-resolution mri characterization of human thrombus using a novel fibrin-targeted paramagnetic nanoparticle contrast agent. Magn. Reson. Med. 2000, 44, 867–872. [Google Scholar] [CrossRef]
- Flacke, S.; Fischer, S.; Scott, M.J.; Fuhrhop, R.J.; Allen, J.S.; McLean, M.; Winter, P.; Sicard, G.A.; Gaffney, P.J.; Wickline, S.A.; et al. Novel mri contrast agent for molecular imaging of fibrin: Implications for detecting vulnerable plaques. Circulation 2001, 104, 1280–1285. [Google Scholar] [CrossRef]
- Botnar, R.M.; Perez, A.S.; Witte, S.; Wiethoff, A.J.; Laredo, J.; Hamilton, J.; Quist, W.; Parsons, E.C., Jr.; Vaidya, A.; Kolodziej, A.; et al. In vivo molecular imaging of acute and subacute thrombosis using a fibrin-binding magnetic resonance imaging contrast agent. Circulation 2004, 109, 2023–2029. [Google Scholar] [CrossRef]
- Botnar, R.M.; Buecker, A.; Wiethoff, A.J.; Parsons, E.C., Jr.; Katoh, M.; Katsimaglis, G.; Weisskoff, R.M.; Lauffer, R.B.; Graham, P.B.; Gunther, R.W.; et al. In vivo magnetic resonance imaging of coronary thrombosis using a fibrin-binding molecular magnetic resonance contrast agent. Circulation 2004, 110, 1463–1466. [Google Scholar] [CrossRef]
- Spuentrup, E.; Buecker, A.; Katoh, M.; Wiethoff, A.J.; Parsons, E.C., Jr.; Botnar, R.M.; Weisskoff, R.M.; Graham, P.B.; Manning, W.J.; Gunther, R.W. Molecular magnetic resonance imaging of coronary thrombosis and pulmonary emboli with a novel fibrin-targeted contrast agent. Circulation 2005, 111, 1377–1382. [Google Scholar] [CrossRef]
- Makowski, M.R.; Forbes, S.C.; Blume, U.; Warley, A.; Jansen, C.H.; Schuster, A.; Wiethoff, A.J.; Botnar, R.M. In vivo assessment of intraplaque and endothelial fibrin in apoe(-/-) mice by molecular mri. Atherosclerosis 2012, 222, 43–49. [Google Scholar] [CrossRef]
- Spuentrup, E.; Botnar, R.M.; Wiethoff, A.; Ibrahim, T.; Sebastin, K.; Katho, M.; Oezgun, M.; Nagel, E.; Vymazal, J.; Graham, P.; et al. Mr imaging of thrombi using ep-2104r, a fibrin specific contrast agent: Initial results in patients. European Radiol. 2008, 18, 1995–2005. [Google Scholar] [CrossRef]
- Sirol, M.; Moreno, P.; Purushothaman, K.; Vucic, E.; Amirbekian, V.; Weinmann, H.; Muntner, P.; Fuster, V.; Fayad, Z. Increased neovascularization in advanced lipid-rich atherosclerotic lesions detected by gadofluorine-m-enhanced mri: Implications for plaque vulnerability. Circ. Cardiovasc. Imaging 2009, 2, 391–396. [Google Scholar] [CrossRef]
- Frias, J.C.; Williams, K.J.; Fisher, E.A.; Fayad, Z.A. Recombinant hdl-like nanoparticles: A specific contrast agent for mri of atherosclerotic plaques. J. Am. Chem. Soc. 2004, 126, 16316–16317. [Google Scholar] [CrossRef]
- Chen, W.; Vucic, E.; Leupold, E.; Mulder, W.J.; Cormode, D.P.; Briley-Saebo, K.C.; Barazza, A.; Fisher, E.A.; Dathe, M.; Fayad, Z.A. Incorporation of an apoe-derived lipopeptide in high-density lipoprotein mri contrast agents for enhanced imaging of macrophages in atherosclerosis. Contrast Media Mol. Imaging 2008, 3, 233–242. [Google Scholar]
- Winter, P.M.; Morawski, A.M.; Caruthers, S.D.; Fuhrhop, R.W.; Zhang, H.; Williams, T.A.; Allen, J.S.; Lacy, E.K.; Robertson, J.D.; Lanza, G.M.; et al. Molecular imaging of angiogenesis in early-stage atherosclerosis with alpha(v)beta3-integrin-targeted nanoparticles. Circulation 2003, 108, 2270–2274. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Phinikaridou, A.; Andia, M.E.; Lacerda, S.; Lorrio, S.; Makowski, M.R.; Botnar, R.M. Molecular MRI of Atherosclerosis. Molecules 2013, 18, 14042-14069. https://doi.org/10.3390/molecules181114042
Phinikaridou A, Andia ME, Lacerda S, Lorrio S, Makowski MR, Botnar RM. Molecular MRI of Atherosclerosis. Molecules. 2013; 18(11):14042-14069. https://doi.org/10.3390/molecules181114042
Chicago/Turabian StylePhinikaridou, Alkystis, Marcelo E. Andia, Sara Lacerda, Silvia Lorrio, Marcus R. Makowski, and René M. Botnar. 2013. "Molecular MRI of Atherosclerosis" Molecules 18, no. 11: 14042-14069. https://doi.org/10.3390/molecules181114042