
Combined Treatment with Hyaluronic Acid and Mesalamine Protects Rats from Inflammatory Bowel Disease Induced by Intracolonic Administration of Trinitrobenzenesulfonic Acid

Abstract
:1. Introduction
2. Results
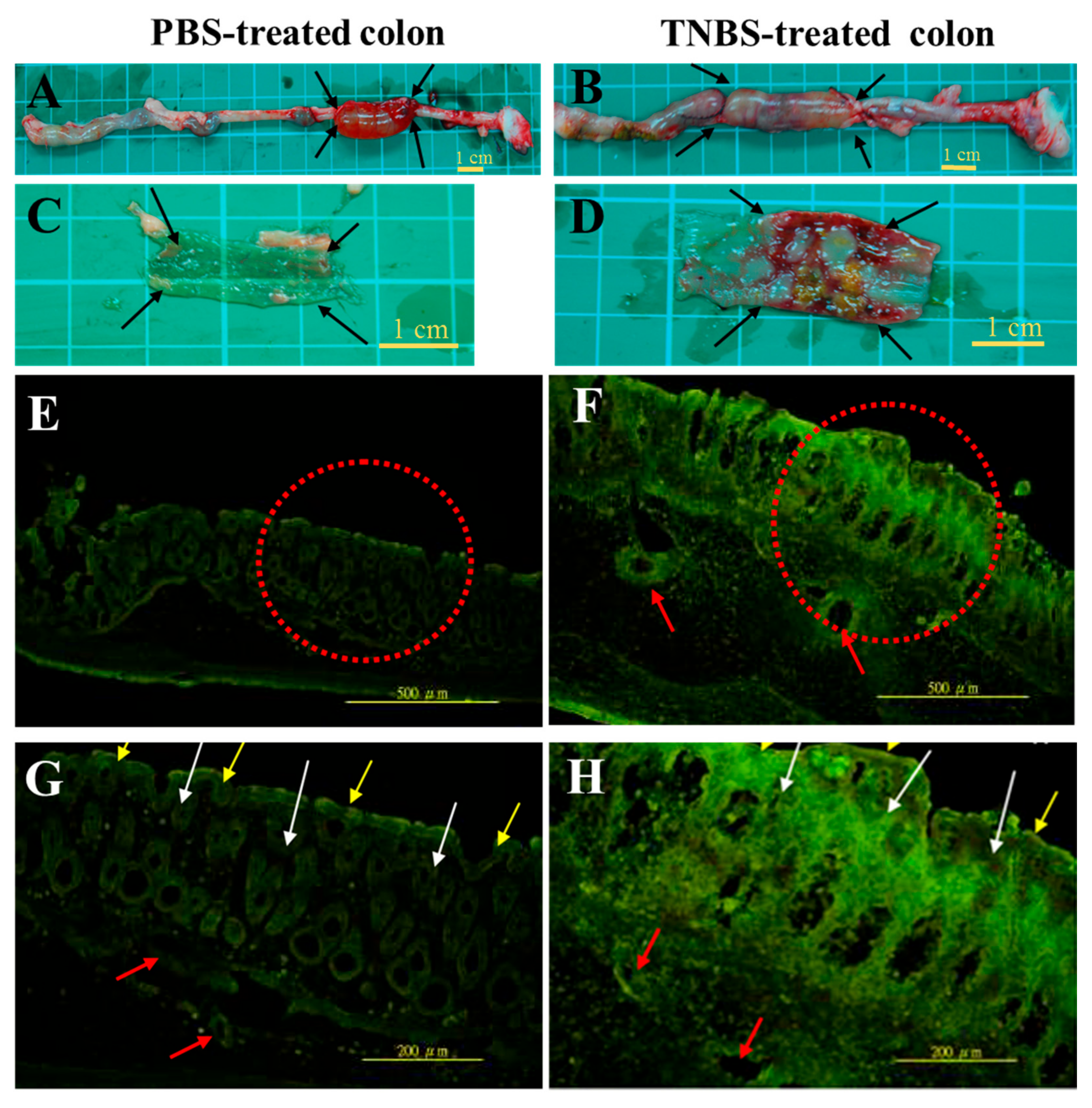
2.1. Ex Vivo Adhesive Properties of FL-Labeled HA Conjugates in the Colon Tissue of Rats
2.2. In Vivo Adhesive Observation of FL-Labeled HA Conjugates on the Colon Epithelia
2.3. Clinical Findings and Macroscopic and Cumulative Microscopic Assessment of Rats with TNBS-Induced Colitis
2.4. Suppression of MPO Activity and TNF-α Gene and COX-2 Protein Expressions after the Combined Treatment with HA and 5-ASA in Rats with TNBS-Induced Colitis
3. Discussion
4. Materials and Methods
4.1. Experimental Reagents
4.2. Preparation of Fluorescent HA Conjugates
4.3. Animal Care
4.4. Ex Vivo Adhesion of FL-Labeled HA Conjugates in Colon Tissue through Observation with an IVIS
4.5. In Vivo Adhesion Observation of HA-FL in the Colon Tissue
4.6. Induction of Colitis and Determination of Clinical Scores of Stool Consistency
4.7. Assessment of the Severity of Colitis
4.8. Histological Assessment of Colitis
4.9. Assessment of MPO Activity
4.10. Analysis of Gene Levels of Proinflammatory Cytokine Expressions in Colon Tissues through Real-Time PCR
4.11. Analysis of COX-2 Protein Expression
4.12. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Strober, W.; Fuss, I.J.; Blumberg, R.S. The immunology of mucosal models of inflammation. Annu. Rev. Immunol. 2002, 20, 495–549. [Google Scholar] [CrossRef] [PubMed]
- Bouma, G.; Strober, W. The immunological and genetic basis of inflammatory bowel disease. Nat. Rev. Immunol. 2003, 3, 521–533. [Google Scholar] [CrossRef] [PubMed]
- Waldner, M.J.; Neurath, M.F. Novel cytokine-targeted therapies and intestinal inflammation. Curr. Opin. Pharmacol. 2009, 9, 702–707. [Google Scholar] [CrossRef] [PubMed]
- Arab, H.H.; Al-Shorbagy, M.Y.; Abdallah, D.M.; Nassar, N.N. Telmisartan attenuates colon inflammation, oxidative perturbations and apoptosis in a rat model of experimental inflammatory bowel disease. PLoS ONE 2014, 9, e97193. [Google Scholar] [CrossRef] [PubMed]
- Kretzmann, N.A.; Fillmann, H.; Mauriz, J.L.; Marroni, C.A.; Marroni, N.; Gonzalez-Gallego, J.; Tunon, M.J. Effects of glutamine on proinflammatory gene expression and activation of nuclear factor kappa b and signal transducers and activators of transcription in tnbs-induced colitis. Inflamm. Bowel Dis. 2008, 14, 1504–1513. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, O.; Petersson, J.; Walden, T.; Ahl, D.; Sandler, S.; Phillipson, M.; Holm, L. Inos-dependent increase in colonic mucus thickness in dss-colitic rats. PLoS ONE 2013, 8, e71843. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Yuan, C.P.; Wang, W.; Yang, Z.Q.; Cui, W.; Mu, L.Z.; Yue, Z.P.; Yin, X.L.; Hu, Z.M.; Liu, J.X. Expression of interleukin 6 in brain and colon of rats with tnbs-induced colitis. World J. Gastroenterol. 2010, 16, 2252–2259. [Google Scholar] [CrossRef] [PubMed]
- James, S.L.; Irving, P.M.; Gearry, R.B.; Gibson, P.R. Management of distal ulcerative colitis: Frequently asked questions analysis. Intern. Med. J. 2008, 38, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Papadakis, K.A.; Targan, S.R. Current theories on the causes of inflammatory bowel disease. Gastroenterol. Clin. N. Am. 1999, 28, 283–296. [Google Scholar] [CrossRef]
- Chidlow, J.H., Jr.; Shukla, D.; Grisham, M.B.; Kevil, C.G. Pathogenic angiogenesis in ibd and experimental colitis: New ideas and therapeutic avenues. Am. J. Physiol. Gastrointest. Liver Physiol. 2007, 293, G5–G18. [Google Scholar] [CrossRef] [PubMed]
- Aslan, M.; Simsek, G.; Dayi, E. The effect of hyaluronic acid-supplemented bone graft in bone healing: Experimental study in rabbits. J. Biomater. Appl. 2006, 20, 209–220. [Google Scholar] [CrossRef] [PubMed]
- Savani, R.C.; Cao, G.; Pooler, P.M.; Zaman, A.; Zhou, Z.; DeLisser, H.M. Differential involvement of the hyaluronan (ha) receptors cd44 and receptor for ha-mediated motility in endothelial cell function and angiogenesis. J. Biol. Chem. 2001, 276, 36770–36778. [Google Scholar] [CrossRef] [PubMed]
- Bourguignon, L.Y.; Gilad, E.; Peyrollier, K.; Brightman, A.; Swanson, R.A. Hyaluronan-cd44 interaction stimulates rac1 signaling and pkn gamma kinase activation leading to cytoskeleton function and cell migration in astrocytes. J. Neurochem. 2007, 101, 1002–1017. [Google Scholar] [CrossRef] [PubMed]
- Wittig, B.M.; Johansson, B.; Zoller, M.; Schwarzler, C.; Gunthert, U. Abrogation of experimental colitis correlates with increased apoptosis in mice deficient for cd44 variant exon 7 (cd44v7). J. Exp. Med. 2000, 191, 2053–2064. [Google Scholar] [CrossRef] [PubMed]
- Wittig, B.M.; Stallmach, A.; Zeitz, M.; Gunthert, U. Functional involvement of cd44 variant 7 in gut immune response. Pathobiol. J. Immunopathol. Mol. Cell. Biol. 2002, 70, 184–189. [Google Scholar] [CrossRef]
- Miyake, K.; Underhill, C.B.; Lesley, J.; Kincade, P.W. Hyaluronate can function as a cell adhesion molecule and cd44 participates in hyaluronate recognition. J. Exp. Med. 1990, 172, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Johnson, P.; Ruffell, B. Cd44 and its role in inflammation and inflammatory diseases. Inflamm. Allergy Drug Targets 2009, 8, 208–220. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.Y.; Abatangelo, G. Functions of hyaluronan in wound repair. Wound Repair Regen. 1999, 7, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Tesar, B.M.; Jiang, D.; Liang, J.; Palmer, S.M.; Noble, P.W.; Goldstein, D.R. The role of hyaluronan degradation products as innate alloimmune agonists. Am. J. Transplant. 2006, 6, 2622–2635. [Google Scholar] [CrossRef] [PubMed]
- West, D.C.; Hampson, I.N.; Arnold, F.; Kumar, S. Angiogenesis induced by degradation products of hyaluronic acid. Science 1985, 228, 1324–1326. [Google Scholar] [CrossRef] [PubMed]
- Necas, J.; Bartosikova, L.; Brauner, P.; Kolar, J. Hyaluronic acid (hyaluronan): A review. Vet. Med. Czech 2008, 53, 15. [Google Scholar]
- Annabi, B.; Thibeault, S.; Moumdjian, R.; Beliveau, R. Hyaluronan cell surface binding is induced by type i collagen and regulated by caveolae in glioma cells. J. Biol. Chem. 2004, 279, 21888–21896. [Google Scholar] [CrossRef] [PubMed]
- Dickinson, L.E.; Ho, C.C.; Wang, G.M.; Stebe, K.J.; Gerecht, S. Functional surfaces for high-resolution analysis of cancer cell interactions on exogenous hyaluronic acid. Biomaterials 2010, 31, 5472–5478. [Google Scholar] [CrossRef] [PubMed]
- Gerdin, B.; Hallgren, R. Localisation of hyaluronan in the human intestinal wall. Gut 1991, 32, 760–762. [Google Scholar] [CrossRef] [PubMed]
- Andre, R.; Wheeler, R.D.; Collins, P.D.; Luheshi, G.N.; Pickering-Brown, S.; Kimber, I.; Rothwell, N.J.; Pinteaux, E. Identification of a truncated il-18r beta mrna: A putative regulator of il-18 expressed in rat brain. J. Neuroimmunol. 2003, 145, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Nau, F., Jr.; Yu, B.; Martin, D.; Nichols, C.D. Serotonin 5-ht2a receptor activation blocks tnf-alpha mediated inflammation in vivo. PLoS ONE 2013, 8, e75426. [Google Scholar] [CrossRef] [PubMed]
- Sandri, G.; Rossi, S.; Ferrari, F.; Bonferoni, M.C.; Zerrouk, N.; Caramella, C. Mucoadhesive and penetration enhancement properties of three grades of hyaluronic acid using porcine buccal and vaginal tissue, caco-2 cell lines, and rat jejunum. J. Pharm. Pharmacol. 2004, 56, 1083–1090. [Google Scholar] [CrossRef] [PubMed]
- Zheng, L.; Riehl, T.E.; Stenson, W.F. Regulation of colonic epithelial repair in mice by toll-like receptors and hyaluronic acid. Gastroenterology 2009, 137, 2041–2051. [Google Scholar] [CrossRef] [PubMed]
- Martinez, F.J.; Safrin, S.; Weycker, D.; Starko, K.M.; Bradford, W.Z.; King, T.E., Jr.; Flaherty, K.R.; Schwartz, D.A.; Noble, P.W.; Raghu, G.; et al. The clinical course of patients with idiopathic pulmonary fibrosis. Ann. Intern. Med. 2005, 142, 963–967. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Jung, J.Y.; Bang, D. The efficacy of topical 0.2% hyaluronic acid gel on recurrent oral ulcers: Comparison between recurrent aphthous ulcers and the oral ulcers of behcet's disease. J. Eur. Acad. Derm. Venereol. JEADV 2008, 22, 590–595. [Google Scholar] [CrossRef] [PubMed]
- Eiserich, J.P.; Hristova, M.; Cross, C.E.; Jones, A.D.; Freeman, B.A.; Halliwell, B.; van der Vliet, A. Formation of nitric oxide-derived inflammatory oxidants by myeloperoxidase in neutrophils. Nature 1998, 391, 393–397. [Google Scholar] [CrossRef] [PubMed]
- Goyal, S.; Arora, S.; Bhatt, T.K.; Das, P.; Sharma, A.; Kumari, S.; Arya, D.S. Modulation of ppar-gamma by telmisartan protects the heart against myocardial infarction in experimental diabetes. Chem.-Biol. Int. 2010, 185, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Goyal, S.N.; Bharti, S.; Bhatia, J.; Nag, T.C.; Ray, R.; Arya, D.S. Telmisartan, a dual arb/partial ppar-gamma agonist, protects myocardium from ischaemic reperfusion injury in experimental diabetes. Diabetes Obes. Metab. 2011, 13, 533–541. [Google Scholar] [CrossRef] [PubMed]
- Roth, A.; Mollenhauer, J.; Wagner, A.; Fuhrmann, R.; Straub, A.; Venbrocks, R.A.; Petrow, P.; Brauer, R.; Schubert, H.; Ozegowski, J.; et al. Intra-articular injections of high-molecular-weight hyaluronic acid have biphasic effects on joint inflammation and destruction in rat antigen-induced arthritis. Arthritis Res. Ther. 2005, 7, R677–R686. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Luo, J.; Chen, X.; Wang, J.; Wang, G.; Li, H.; Xu, Y.; Feng, J.; Tu, H. Expression characteristic and significance of interleukin-6, nuclear factor kappa beta, and bone formation markers in rat models of osteoporosis. Transl. Res. 2008, 152, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Ross, R. Atherosclerosis—An inflammatory disease. N. Engl. J. Med. 1999, 340, 115–126. [Google Scholar] [CrossRef]
- Parameswaran, N.; Patial, S. Tumor necrosis factor-alpha signaling in macrophages. Crit. Rev. Eukaryot. Gene Expr. 2010, 20, 87–103. [Google Scholar] [CrossRef] [PubMed]
- Okayama, M.; Hayashi, S.; Aoi, Y.; Nishio, H.; Kato, S.; Takeuchi, K. Aggravation by selective cox-1 and cox-2 inhibitors of dextran sulfate sodium (dss)-induced colon lesions in rats. Dig. Dis. Sci. 2007, 52, 2095–2103. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, A.; Ancha, H.; Tedesco, D.; Lightfoot, S.; Stewart, C.A.; Harty, R.F. Antioxidant therapy with n-acetylcysteine plus mesalamine accelerates mucosal healing in a rodent model of colitis. Dig. Dis. Sci. 2006, 51, 698–705. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.F.; Maeda, N.; Smithies, O.; Straight, D.L.; Stafford, D.W. A coagulation factor ix-deficient mouse model for human hemophilia b. Blood 1997, 90, 3962–3966. [Google Scholar] [PubMed]
Sample Availability: Samples of the compounds are not available from the authors. |





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Clinical Findings | Macroscopic Lesions | Cumulative Microscopic Injury Scores | ||||||
|---|---|---|---|---|---|---|---|---|---|
| (Induction/Treatment) | No. of Animals | Weight Gain (%) | Stool Lesion Score | Length of Colon (cm) | Weight of Colon (g) | Bowel Wall Thickness (μm) | Inflammatory Area (cm2) | Macroscopic Scores | |
| PBS/PBS | n = 10 | 14.5 ± 1.4 b | 1.0 ± 0 a | 20.4 ± 1.6 a | 2.2 ± 0.2 a | 177.2 ± 19.1 a | 0 ± 0 a | 0 ± 0 a | 0.0 ± 0.0 a |
| TNBS/PBS | n = 16 | 2.4 ± 2.2 a | 2.6 ± 0.1 b | 16.6 ± 1.6 b | 3.2 ± 1.0 b | 599.1 ± 181.3 c | 3.39 ± 0.73 b,c | 1.94 ± 0.39 c | 8.33 ± 0.49 c |
| TNBS/HA | n = 16 | 4.6 ± 1.5 a | 2.0 ± 0.2 c | 16.9 ± 1.7 b | 3.0 ± 1.0 b | 514.6 ± 133.7 b,c | 3.02 ± 0.77 b,c | 1.69 ± 0.36 b | 5.80 ± 0.58 b |
| TNBS/5-ASA | n = 16 | 3.7 ± 1.7 a | 2.5 ± 0.2 b,c | 17.2 ± 1.4 b | 3.5 ± 1.1 b | 581.1 ± 214.7 c | 4.30 ± 0.70 c | 2.19 ± 0.33 b,c | 6.33 ± 0.61 b,c |
| TNBS/HA + 5-ASA | n = 16 | 5.4 ± 1.5 a | 2.0 ± 0.2 c | 16.8 ± 1.2 b | 3.1 ± 0.9 b | 442.9 ± 98.6 b | 2.50 ± 0.63 b | 0.94 ± 0.30 b | 7.27 ± 0.21 c |
| Cytokines | Sequence | Amplicon Length | Reference | |
|---|---|---|---|---|
| TNF-α | Primer | 5′-AAATGGGCTCCCTCTCATCAG TTC-3′ | 110 bp | [25] |
| 5′-TCTGCTTGGTGGTTTGCTACG AC-3′ | ||||
| probe | FAM-CCA GAC CCT CAC ACT CAG-MGB | |||
| IL-1β | Primer | 5′-CACCTCTCAAGCAGAGCA CAG-3′ | 78 bp | [25] |
| 5′-GGGTTCCATGGTGAAGTC AAC-3′ | ||||
| probe | FAM-AGG AAA CAG CAA TGG-MGB | |||
| IL-6 | Primer | 5′-TCCTACCCCAACTTCCAATGC TC-3′ | 78 bp | [25] |
| 5′-TTGGATGGTCTTGGTCCTTAG CC-3′ | ||||
| probe | FAM-AGTT TAG AGT CAC AGA AG-MGB | |||
| β-actin | Primer | 5′-CCTTCCTGTGCATGGAGT CCT-3′ | 202 bp | [40] |
| 5′-GGAGCAATGATCTTGATC TTC-3′ | ||||
| probe | FAM-AGA CCT GTA TGC CAA C-MGB |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiu, C.-T.; Kuo, S.-N.; Hung, S.-W.; Yang, C.-Y. Combined Treatment with Hyaluronic Acid and Mesalamine Protects Rats from Inflammatory Bowel Disease Induced by Intracolonic Administration of Trinitrobenzenesulfonic Acid. Molecules 2017, 22, 904. https://doi.org/10.3390/molecules22060904
Chiu C-T, Kuo S-N, Hung S-W, Yang C-Y. Combined Treatment with Hyaluronic Acid and Mesalamine Protects Rats from Inflammatory Bowel Disease Induced by Intracolonic Administration of Trinitrobenzenesulfonic Acid. Molecules. 2017; 22(6):904. https://doi.org/10.3390/molecules22060904
Chicago/Turabian StyleChiu, Chih-Tung, Sheng-Nan Kuo, Shao-Wen Hung, and Cheng-Yao Yang. 2017. "Combined Treatment with Hyaluronic Acid and Mesalamine Protects Rats from Inflammatory Bowel Disease Induced by Intracolonic Administration of Trinitrobenzenesulfonic Acid" Molecules 22, no. 6: 904. https://doi.org/10.3390/molecules22060904