Inhibitory Effects of Diclofenac on Steroid Glucuronidation In Vivo Do Not Affect Hair-Based Doping Tests for Stanozolol

 , ,
, ,  ,
,  and
and
Abstract
:1. Introduction
Aims and Research Hypotheses
- H1: increase the circulating concentration of stanozolol and 3′-hydroxystanozolol (blood);
- H2: decrease the concentration of 3′-hydroxystanozolol in urine;
- H3: increase the concentration of stanozolol and 3′-hydroxystanozolol in hair; and
- H4: whilst the concentrations of stanozolol and 3′-hydroxystanozolol in hair are expected to gradually decrease after ceasing stanolozol treatment, both stanozolol and 3′-hydroxystanozolol in hair will remain detectable for the same period after the treatment cycle.
2. Results
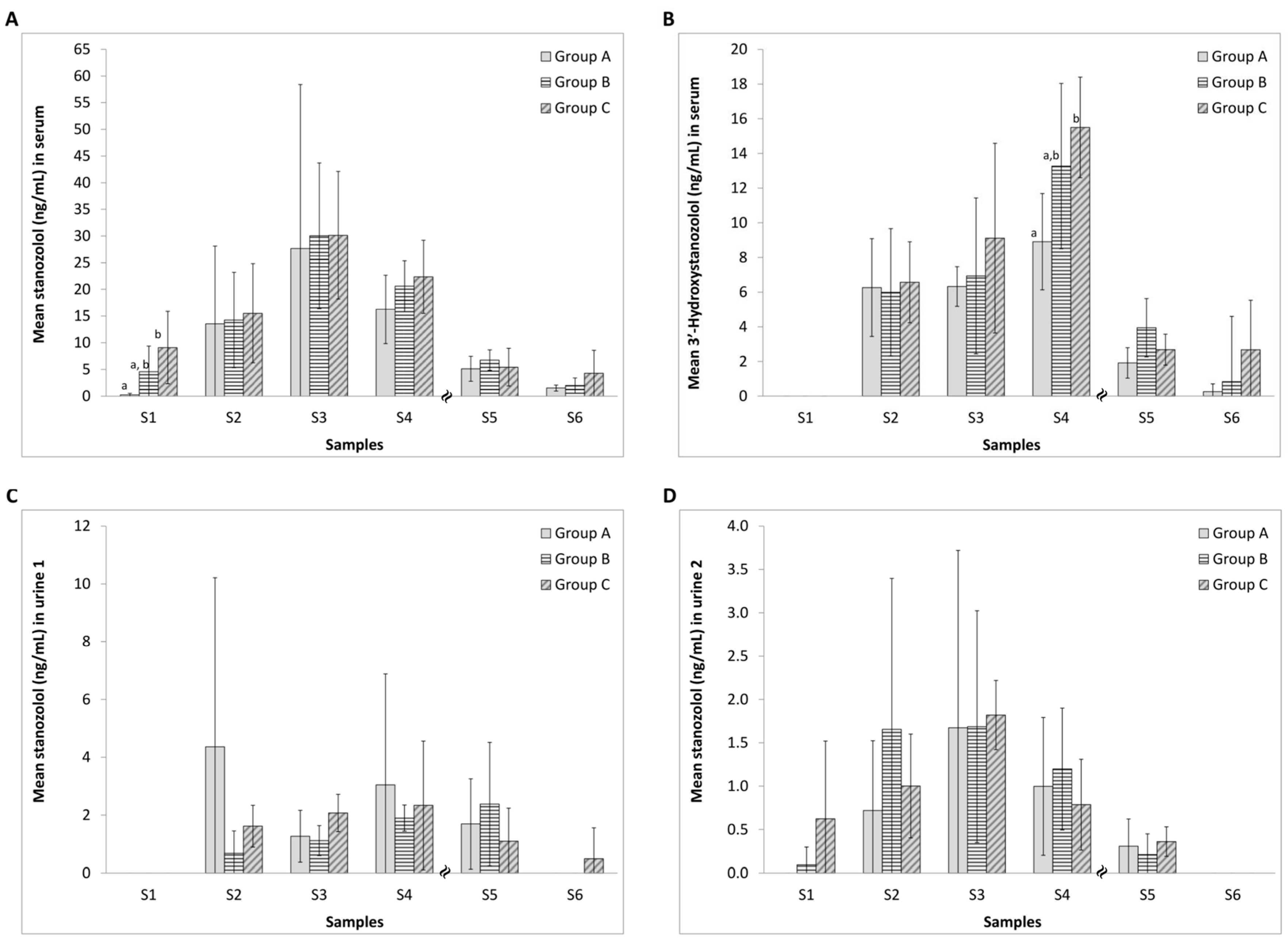
2.1. Effect of Diclofenac on the Serum Concentration of Stanozolol and 3′-Hydroxystanozolol
2.2. Effect of Diclofenac on the Urinary Excretion of Stanozolol and 3′-Hydroxystanozolol
2.3. Effect of Diclofenac on the Incorporation of Stanozolol and 3′-Hydroxystanozolol in Hair
2.4. Relationship between Levels of Stanozolol and 3′-Hydroxystanozolol in Hair, Urine and Blood
3. Discussion
3.1. Effect of Diclofenac on Stanozolol Distribution
3.1.1. H1: Increase the Circulating Concentration of Stanozolol and 3′-Hydroxystanozolol (Blood)
3.1.2. H2: Decrease the Concentration of 3′-Hydroxystanozolol in Urine
3.1.3. H3: Increase the Concentration of Stanozolol and 3′-Hydroxystanozolol in Hair
3.1.4. H4: Whilst the Concentrations of Stanozolol and 3′-Hydroxystanozolol in Hair are Expected to Gradually Decrease after Ceasing Stanolozol Treatment, Both Stanozolol and 3-Hydroxystanozolol in Hair Will Remain Detectable for up to Three Weeks
3.2. Implications of the Results and Future Perspectives
4. Materials and Methods
4.1. Chemicals and Reagents
4.2. Animals
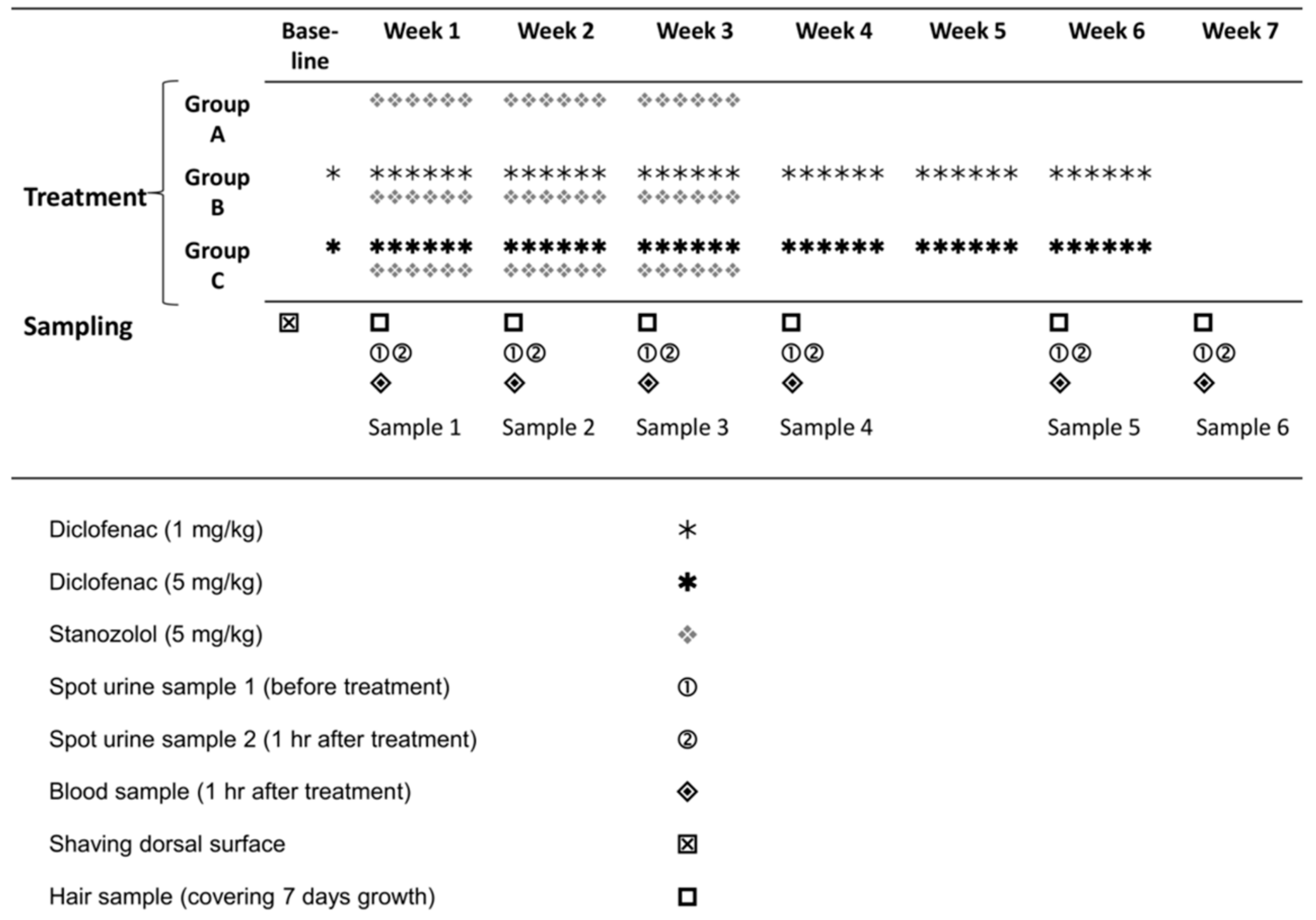
4.3. Administration of Diclofenac and Stanozolol
4.4. Sample Collection
4.5. Sample Preparation
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Turgeon, D.; Carrier, J.S.; Chouinard, S.; Belanger, A. Glucuronidation activity of the UGT2B17 enzyme toward xenobiotics. Drug Metab. Dispos. 2003, 31, 670–676. [Google Scholar] [CrossRef] [PubMed]
- Belanger, A.; Pelletier, G.; Labrie, F.; Barbier, O.; Chouinard, S. Inactivation of androgens by UDP-glucuronosyltransferase enzymes in humans. Trends Endocrinol. Metabol. 2003, 14, 473–479. [Google Scholar] [CrossRef]
- Hum, D.W.; Bélanger, A.; Lévesque, E.; Barbier, O.; Beaulieu, M.; Albert, C.; Vallée, M.; Guillemette, C.; Tchernof, A.; Turgeon, D.; et al. Characterization of UDP-glucuronosyltransferases active on steroid hormones. J. Steroid Biochem. Mol. Biol. 1999, 69, 413–423. [Google Scholar] [CrossRef]
- You, L. Steroid hormone biotransformation and xenobiotic induction of hepatic steroid metabolizing enzymes. Chem. Biol. Interact. 2004, 147, 233–246. [Google Scholar] [CrossRef] [PubMed]
- Schulze, J.J.; Lundmark, J.; Garle, M.; Skilving, I.; Ekström, L.; Rane, A. Doping test results dependent on genotype of uridine diphospho-glucuronosyl transferase 2B17, the major enzyme for testosterone glucuronidation. J. Clin. Endocrinol. Metabol. 2008, 93, 2500–2506. [Google Scholar] [CrossRef] [PubMed]
- Deshmukh, N.; Petróczi, A.; Barker, J.; Szekely, A.; Hussain, I.; Naughton, D.P. Potentially harmful advantage to athletes: A putative connection between UGT2B17 gene deletion polymorphism and renal disorders with prolonged use of anabolic androgenic steroids. Subst. Abuse Treat. Prev. Policy 2010, 5, 7. [Google Scholar] [CrossRef] [PubMed]
- Skarberg, K.; Nyberg, F.; Engstrom, I. Multisubstance use as a feature of addiction to anabolic-androgenic steroids. Eur. Addict. Res. 2009, 15, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Warden, S.J. Prophylactic misuse and recommended use of non-steroidal anti-inflammatory drugs by athletes. Br. J. Sports Med. 2009, 43, 548–549. [Google Scholar] [CrossRef] [PubMed]
- Warden, S.J. Prophylactic use of NSAIDs by athletes: A risk/benefit assessment. Phys. Sportsmed. 2010, 38, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Tsitsimpikou, C.; Tsiokanos, A.; Tsarouhas, K.; Schamasch, P.; Fitch, K.D.; Valasiadis, D.; Jamurtas, A. Medication use by athletes at the Athens 2004 Summer Olympic Games. Clin. J. Sport Med. 2009, 19, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.H.S.; Johnson, K.; Pipe, A.L. The use of dietary supplements and medications by Canadian athletes at the Atlanta and Sydney Olympic Games. Clin. J. Sport Med. 2006, 16, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Van Thuyne, W.; Delbeke, F.T. Declared use of medication in sports. Clin. J. Sport Med. 2008, 18, 143–147. [Google Scholar] [CrossRef] [PubMed]
- Sten, T.; Finel, M.; Ask, B.; Rane, A.; Ekström, L. Non-steroidal anti-inflammatory drugs interact with testosterone glucuronidation. Steroids 2009, 74, 971–977. [Google Scholar] [CrossRef] [PubMed]
- Jenkinson, C.; Petróczi, A.; Barker, J.; Naughton, D.P. Dietary green and white teas suppress UDP-glucuronosyltransferase UGT2B17 mediated testosterone glucuronidation. Steroids 2012, 77, 691–695. [Google Scholar] [CrossRef] [PubMed]
- Jenkinson, C.; Petróczi, A.; Naughton, D.P. Red wine and components flavonoids inhibit UGT2B17 in vitro. Nutr. J. 2012, 11, 67. [Google Scholar] [CrossRef] [PubMed]
- Lundmark, J.; Gårevik, N.; Thörngren, J.-O.; Garle, M.; Ekström, L.; Rane, A.; Schulze, J.J. Non-steroidal anti-inflammatory drugs do not influence the urinary testosterone/epitestosterone glucuronide ratio. Front. Endocrinol. 2013, 4, 51. [Google Scholar] [CrossRef] [PubMed]
- Kintz, P.; Cirimele, V.; Sachs, H.; Jeanneau, T.; Ludes, B. Testing for anabolic steroids in hair from two bodybuilders. Forensic Sci. Int. 1999, 101, 209–216. [Google Scholar] [CrossRef]
- Graham, M.R.; Davies, B.; Grace, F.M.; Kicman, A.; Baker, J.S. Anabolic steroid use: Patterns of use and detection of doping. Sports Med. 2008, 38, 505–525. [Google Scholar] [CrossRef] [PubMed]
- WADA (2014) Technical Document—TD2014MRPL. Available online: https://wada-main-prod.s3.amazonaws.com/resources/files/WADA-TD2014MRPL-v1-Minimum-Required-Performance-Levels-EN.pdf (accessed on 27 April 2017).
- Tudela, E.; Deventer, K.; van Eenoo, P. Sensitive detection of 3′-hydroxy-stanozolol glucuronide by liquid chromatography-tandem mass spectrometry. J. Chromatogr. A 2013, 1292, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Cirimele, V.; Kintz, P.; Ludes, B. Testing of the anabolic stanozolol in human hair by gas chromatography-negative ion chemical ionization mass spectrometry. J. Chromatogr. B 2000, 740, 265–271. [Google Scholar] [CrossRef]
- Shen, M.; Xiang, P.; Yan, H.; Shen, B.; Wang, M. Analysis of anabolic steroids in hair: Time courses in guinea pigs. Steroids 2009, 74, 773–778. [Google Scholar] [CrossRef] [PubMed]
- Council Directive 86/609/EEC of 24 November 1986 on the Approximation of Laws, Regulations and Administrative Provisions of the Member States Regarding the Protection of Animals Used for Experimental and Other Scientific Purposes. Available online: http://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=CELEX:31986L0609:EN:NOT (accessed on 27 April 2017).
- De Almeida Chuffa, L.G.; de Souza, R.B.; Frei, F.; de Fátima Paccola Mesquita, S.; Camargo, I.C. Nandrolone decanoate and physical effort: Histological and morphometrical assessment in adult rat uterus. Anat. Rec. 2011, 294, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Breuer, M.E.; McGinnis, M.Y.; Lumia, A.R.; Possidente, B.P. Aggression in male rats receiving anabolic androgenic steroids: Effects of social and environmental provocation. Horm. Behav. 2001, 40, 409–418. [Google Scholar] [CrossRef] [PubMed]
- Matrisciano, F.; Modafferi, A.M.; Togna, G.I.; Barone, Y.; Pinna, G.; Nicoletti, F.; Scaccianoce, S. Repeated anabolic androgenic steroid treatment causes antidepressant-reversible alterations of the hypothalamic-pituitary-adrenal axis, BDNF levels and behavior. Neuropharmacology 2010, 58, 1078–1084. [Google Scholar] [CrossRef] [PubMed]
- Pieretti, S.; Mastriota, M.; Tucci, P.; Battaglia, G.; Trabace, L.; Nicoletti, F.; Scaccianoce, S. Brain nerve growth factor unbalance induced by anabolic androgenic steroids in rat. Med. Sci. Sports Exerc. 2012, 45, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Deshmukh, N.I.K.; Zachar, G.; Petróczi, A.; Székely, A.D.; Barker, J.; Naughton, D.P. Determination of stanozolol and 3′-hydroxystanozolol in rat hair, urine and serum using liquid chromatography tandem mass spectrometry. Chem. Cent. J. 2012, 6, 162. [Google Scholar] [CrossRef] [PubMed]
- Levine, T.R.; Hullett, C.R. Eta squared, partial eta squared, and misreporting of effect size in communication research. Hum. Commun. Res. 2002, 28, 612–625. [Google Scholar] [CrossRef]
- Morris, S.B.; DeShon, R.P. Combining effect size estimates in meta-analysis with repeated measures and independent-groups designs. Psychol. Methods 2002, 7, 105–125. [Google Scholar] [CrossRef] [PubMed]
- Hotaj, M.; Xu, G. A visitor’s guide to effect sizes—Statistical Significance Versus Practical (Clinical) Importance of Research Findings. Adv. Health Sci. Educ. 2004, 9, 241–249. [Google Scholar]
- Nakagawa, S.; Cuthill, I.C. Effect size, confidence interval and statistical significance: A practical guide for biologists. Biol. Rev. 2007, 82, 591–605. [Google Scholar] [CrossRef] [PubMed]
Sample Availability: Samples of the compounds are not available from the authors. |




{kind=link}
{kind=link}
{kind=link}
| Stanozolol Treatment | Post Stanozolol Treatment | |||||
|---|---|---|---|---|---|---|
| Weeks 1 & 2 | Week 3 | Week 4 | Week 5 | Week 6 | ||
| Hair Stanozolol | ||||||
| Urine 1ST | - | S2 (−) ** | S3 (−) *** | |||
| Urine 2ST | - | S3 (−) * | ||||
| Serum ST | - | S1 (+) ** | S2 (+) * | S3 (+) * | S4 (+) * | |
| Group A | Hair 3′-Hydroxystanozolol | |||||
| Urine 1HST | - | S2 (−) * | S3 (−) *** | |||
| Urine 2HST | - | |||||
| Serum HST | - | S2 (−) * | S3 (+) * | S4 (+) * | ||
| Hair Stanozolol | ||||||
| Urine 1ST | - | S2 (+) *** | S4 (−) * | |||
| Urine 2ST | - | S2 (−) ** | S3 (−) * | |||
| Serum ST | - | S1 (−) *** | S3 (−) * | S4 (−) ** | ||
| Group B | Hair 3′-Hydroxystanozolol | |||||
| Urine 1HST | - | S3 (+) *** | ||||
| Urine 2HST | - | |||||
| Serum HST | - | S2 (+) *** | S3 (-) * | S4 (+) *** | ||
| Hair Stanozolol | ||||||
| Urine 1ST | - | S2 (−) * | S3 (+) *** | S4 (−) ** | ||
| Urine 2ST | - | S2 (−) * | S3 (+) * | |||
| Serum ST | - | S1 (−) * | S2 (+) *** | S3 (+) *** | S4 (−) ** | |
| Group C | Hair 3′-Hydroxystanozolol | |||||
| Urine 1HST | - | S3 (+) *** | ||||
| Urine 2HST | - | |||||
| Serum HST | - | S2 (−) * | S3 (+) ** | S4 (−) * | ||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zachár, G.; Deshmukh, N.I.K.; Petróczi, A.; Székely, A.D.; Shah, I.; Barker, J.; Naughton, D.P. Inhibitory Effects of Diclofenac on Steroid Glucuronidation In Vivo Do Not Affect Hair-Based Doping Tests for Stanozolol. Molecules 2017, 22, 976. https://doi.org/10.3390/molecules22060976
Zachár G, Deshmukh NIK, Petróczi A, Székely AD, Shah I, Barker J, Naughton DP. Inhibitory Effects of Diclofenac on Steroid Glucuronidation In Vivo Do Not Affect Hair-Based Doping Tests for Stanozolol. Molecules. 2017; 22(6):976. https://doi.org/10.3390/molecules22060976
Chicago/Turabian StyleZachár, Gergely, Naved I.K. Deshmukh, Andrea Petróczi, Andrea D. Székely, Iltaf Shah, James Barker, and Declan P. Naughton. 2017. "Inhibitory Effects of Diclofenac on Steroid Glucuronidation In Vivo Do Not Affect Hair-Based Doping Tests for Stanozolol" Molecules 22, no. 6: 976. https://doi.org/10.3390/molecules22060976
APA StyleZachár, G., Deshmukh, N. I. K., Petróczi, A., Székely, A. D., Shah, I., Barker, J., & Naughton, D. P. (2017). Inhibitory Effects of Diclofenac on Steroid Glucuronidation In Vivo Do Not Affect Hair-Based Doping Tests for Stanozolol. Molecules, 22(6), 976. https://doi.org/10.3390/molecules22060976