Combined Effects of Cyclooxygenase-1 and Cyclooxygenase-2 Selective Inhibitors on Ovarian Carcinoma in Vivo

Abstract
:1. Introduction
2. Results and Discussion
2.1. Inhibition of Ovarian Cancer Growth
2.2. Synergistic Effects of SC-560 and Celecoxib on Ovarian Cancer Growth
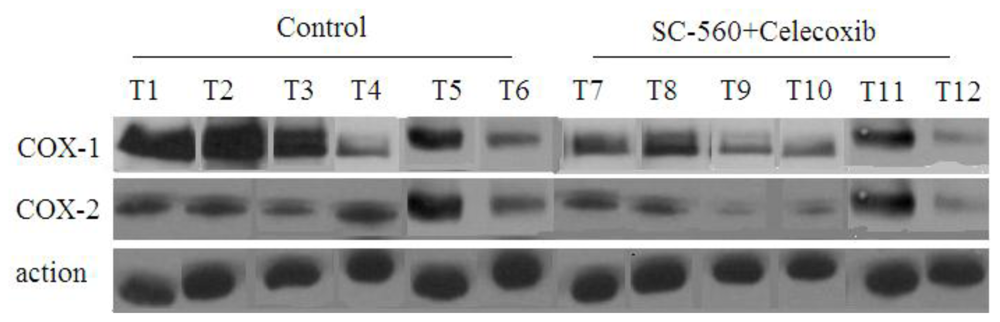
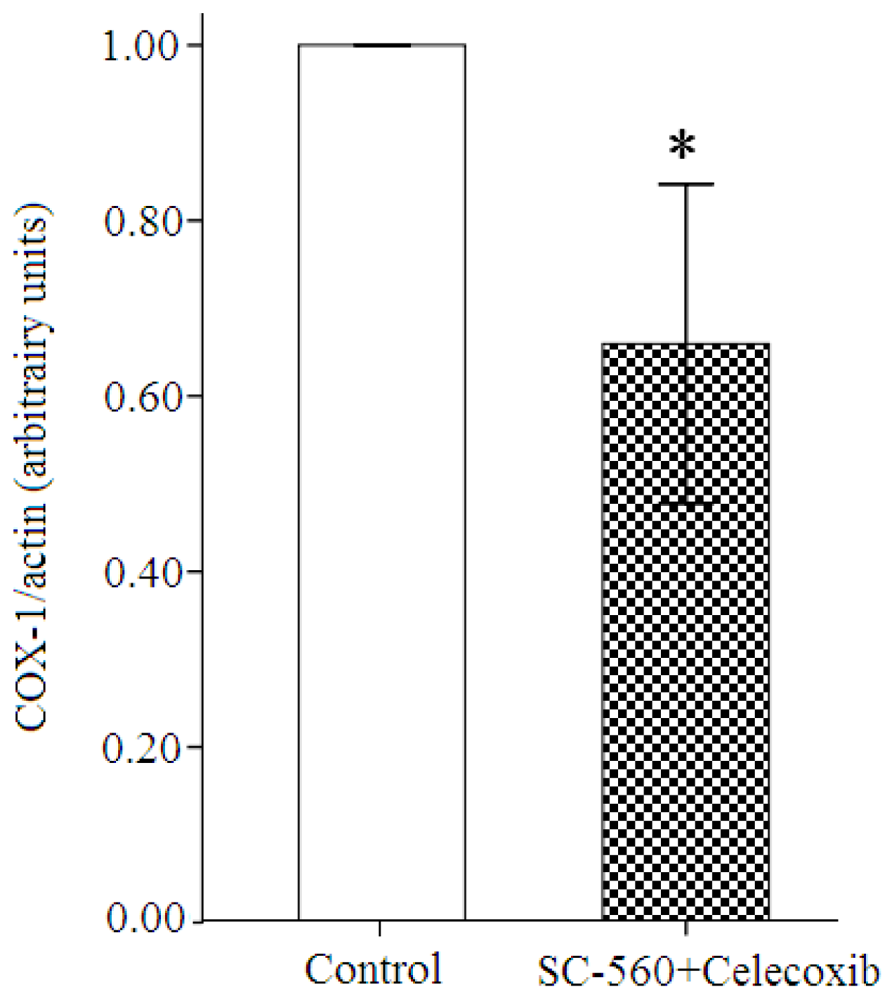
2.3. COX Expression in Ovarian Carcinoma Cells
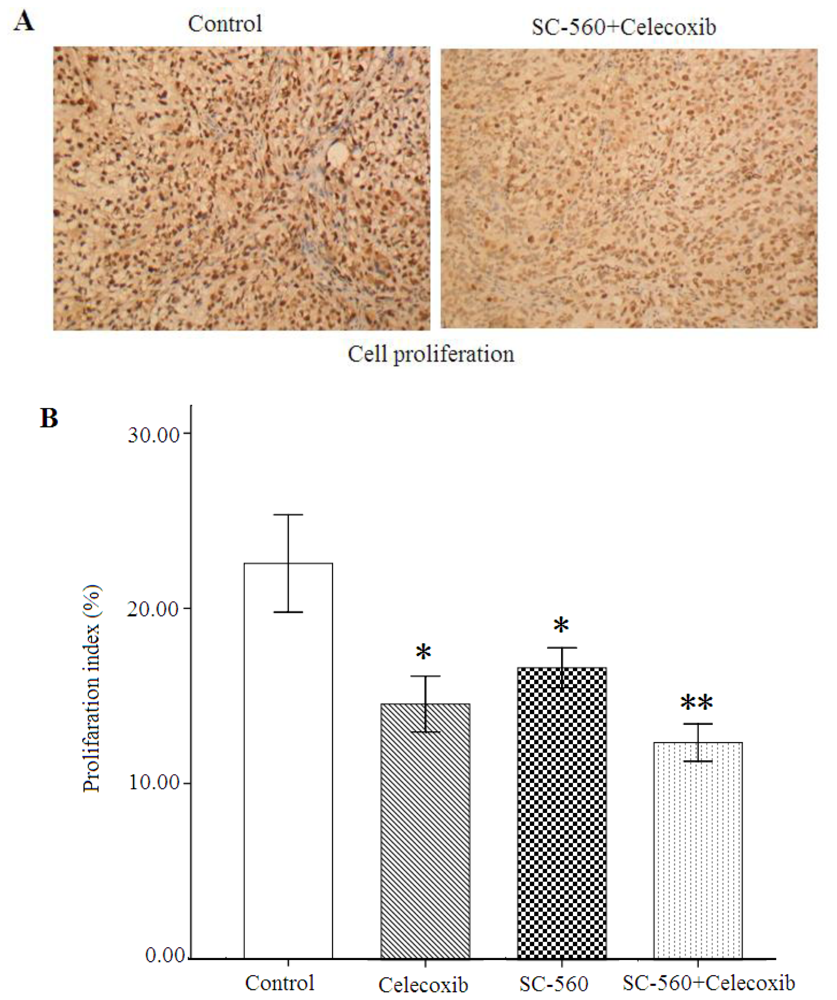
2.4. Cell Proliferation
2.5. Cell Apoptosis
2.6. Discussion
3. Experimental Section
3.1. Human Ovarian Tumors in Nude Mice
3.2. Western Blot Analysis
3.3. Immunohistochemistry
3.4. TUNEL Assay
3.5. Statistical Analyses
4. Conclusions
Acknowledgements
References
- Ozols, RF. Recurrent ovarian cancer: evidence-based treatment. J. Clin. Oncol 2002, 20, 1161–1163. [Google Scholar]
- Dannenberg, AJ; Subbaramaiah, K. Targeting cyclooxygenase-2 in human neoplasia: rationale and promise. Cancer Cell 2003, 4, 431–436. [Google Scholar]
- Gupta, RA; Dubois, RN. Colorectal cancer prevention and treatment by inhibition of cyclooxygenase-2. Nat. Rev Cancer 2001, 1, 11–21. [Google Scholar]
- Smith, WL; Garavito, RM; DeWitt, DL. Prostaglandin endoperoxide H synthases (cyclooxygenases)-1 and -2. J. Biol. Chem 1996, 271, 33157–33160. [Google Scholar]
- Li, JY; Wang, XZ; Chen, FL; Yu, JP; Luo, HS. Nimesulide inhibits proliferation via induction of apoptosis and cell cycle arrest in human gastric adenocarcinoma cell line. World J. Gastroenterol 2003, 9, 915–920. [Google Scholar]
- Li, W; Zhang, HH; Xu, RJ; Zhuo, GC; Hu, YQ; Li, J. Effects of a selective cyclooxygenase-2 inhibitor, nimesulide, on the growth of ovarian carcinoma in vivo. Med. Oncol 2008, 25, 172–177. [Google Scholar]
- Vane, JR; Bakhle, YS; Botting, RM. Cyclooxygenases 1 and 2. Annu. Rev. Pharmacol. Toxicol 1998, 38, 97–120. [Google Scholar]
- Half, E; Tang, XM; Gwyn, K; Sahin, A; Wathen, K; Sinicrope, FA. Cyclooxygenase-2 expression in human breast cancers and adjacent ductal carcinoma in situ. Cancer Res 2002, 62, 1676–1681. [Google Scholar]
- Quidville, V; Segond, N; Tebbi, A; Cohen, R; Jullienne, A; Lepoivre, M; Lausson, S. Anti-tumoral effect of a celecoxib low dose on a model of human medullary thyroid cancer in nude mice. Thyroid 2009, 19, 613–621. [Google Scholar]
- Denkert, C; Köbel, M; Pest, S; Koch, I; Berger, S; Schwabe, M; Siegert, A; Reles, A; Klosterhalfen, B; Hauptmann, S. Expression of cyclooxygenase 2 is an independent prognostic factor in human ovarian carcinoma. Am. J. Pathol 2002, 160, 893–903. [Google Scholar]
- Erkinheimo, TL; Lassus, H; Finne, P; van Rees, BP; Leminen, A; Ylikorkala, O; Haglund, C; Butzow, R; Ristimäki, A. Elevated cyclooxygenase-2 expression is associated with altered expression of p53 and SMAD4, amplification of HER-2/neu, and poor outcome in serous ovarian carcinoma. Clin. Cancer Res 2004, 10, 538–545. [Google Scholar]
- Ferrandina, G; Lauriola, L; Zannoni, GF; Fagotti, A; Fanfani, F; Legge, F; Maggiano, N; Gessi, M; Mancuso, S; Ranelletti, FO; Scambia, G. Increased cyclooxygenase-2 (COX-2) expression is associated with chemotherapy resistance and outcome in ovarian cancer patients. Ann. Oncol 2002, 13, 1205–1211. [Google Scholar]
- Fukutake, M; Nakatsugi, S; Isoi, T; Takahashi, M; Ohta, T; Mamiya, S; Taniguchi, Y; Sato, H; Fukuda, K; Sugimura, T; Wakabayashi, K. Suppressive effects of nimesulide, a selective inhibitor of cyclooxygenase-2, on azoxymethane-induced colon carcinogenesis in mice. Carcinogenesis 1998, 19, 1939–1942. [Google Scholar]
- Kawamori, T; Rao, CV; Seibert, K; Reddy, BS. Chemopreventive activity of celecoxib, a specific cyclooxygenase-2 inhibitor, against colon carcinogenesis. Cancer Res 1998, 58, 409–412. [Google Scholar]
- Daikoku, T; Wang, D; Tranguch, S; Morrow, JD; Orsulic, S; DuBois, RN; Dey, SK. Cyclooxygenase-1 is a potential target for prevention and treatment of ovarian epithelial cancer. Cancer Res 2005, 65, 3735–3744. [Google Scholar]
- Gupta, RA; Tejada, LV; Tong, BJ; Das, SK; Morrow, JD; Dey, SK; DuBois, RN. Cyclooxygenase-1 is overexpressed and promotes angiogenic growth factor production in ovarian cancer. Cancer Res 2003, 63, 906–911. [Google Scholar]
- Cramer, DW; Harlow, BL; Titus-Ernstoff, L; Bohlke, K; Welch, WR; Greenberg, ER. Over-the-counter analgesics and risk of ovarian cancer. Lancet 1998, 351, 104–107. [Google Scholar]
- Harris, RE; Kasbari, S; Farrar, WB. Prospective study of nonsteroidal anti-inflammatory drugs and breast cancer. Oncol. Rep 1999, 6, 71–73. [Google Scholar]
- Reese, J; Zhao, X; Ma, WG; Brown, N; Maziasz, TJ; Dey, SK. Comparative analysis of pharmacologic and/or genetic disruption of cyclooxygenase-1 and cyclooxygenase-2 function in female reproduction in mice. Endocrinology 2001, 142, 3198–3206. [Google Scholar]
- Li, W; Xu, RJ; Lin, ZY; Zhuo, GC; Zhang, HH. Effects of a cyclooxygenase-1-selective inhibitor in a mouse model of ovarian cancer, administered alone or in combination with ibuprofen, a nonselective cyclooxygenase inhibitor. Med. Oncol 2009, 26, 170–177. [Google Scholar]
- Rao, CV; Indranie, C; Simi, B; Manning, PT; Connor, JR; Reddy, BS. Chemopreventive properties of a selective inducible nitric oxide synthase inhibitor in colon carcinogenesis, administered alone or in combination with celecoxib, a selective cyclooxygenase-2 inhibitor. Cancer Res 2002, 62, 165–170. [Google Scholar]
- Zhao, S; Cai, J; Bian, H; Gui, L; Zhao, F. Synergistic inhibition effect of tumor growth by using celecoxib in combination with oxaliplatin. Cancer Invest 2009, 27, 636–640. [Google Scholar]
- Kundu, N; Fulton, AM. Selective cyclooxygenase (COX)-1 or COX-2 inhibitors control metastatic disease in a murine model of breast cancer. Cancer Res 2002, 62, 2343–2346. [Google Scholar]
- Daikoku, T; Tranguch, S; Trofimova, IN; Dinulescu, DM; Jacks, T; Nikitin, AY; Connolly, DC; Dey, SK. Cyclooxygenase-1 is overexpressed in multiple genetically engineered mouse models of epithelial ovarian cancer. Cancer Res 2006, 66, 2527–2531. [Google Scholar]
- Yao, M; Zhou, W; Sangha, S; Albert, A; Chang, AJ; Liu, TC; Wolfe, MM. Effects of nonselective cyclooxygenase inhibition with low-dose ibuprofen on tumor growth, angiogenesis, metastasis, and survival in a mouse model of colorectal cancer. Clin. Cancer Res 2005, 11, 1618–1628. [Google Scholar]
- Li, S; Miner, K; Fannin, R; Carl, BJ; Davis, BJ. Cyclooxygenase-1 and 2 in normal and malignant human ovarian epithelium. Gynecol. Oncol 2004, 92, 622–627. [Google Scholar]
- Leahy, KM; Ornberg, RL; Wang, Y; Zweifel, BS; Koki, AT; Masferrer, JL. Cyclooxygenase-2 inhibition by celecoxib reduces proliferation and induces apoptosis in angiogenic endothelial cells in vivo. Cancer Res 2002, 62, 625–631. [Google Scholar]
- Bottone, FG, Jr; Martinez, JM; Alston-Mills, B; Eling, TE. Gene modulation by Cox-1 and Cox-2 specific inhibitors in human colorectal carcinoma cancer cells. Carcinogenesis 2004, 25, 349–357. [Google Scholar]
- Grosch, S; Tegeder, I; Niederberger, E; Bräutigam, L; Geisslinger, G. COX-2 independent induction of cell cycle arrest and apoptosis in colon cancer cells by the selective COX-2 inhibitor celecoxib. FASEB J 2001, 15, 2742–2744. [Google Scholar]
- Zhu, J; Song, X; Lin, HP; Young, DC; Yan, S; Marquez, VE; Chen, CS. Using cyclooxygenase-2 inhibitors as molecular platforms to develop a new class of apoptosis-inducing agents. J. Natl. Cancer Inst 2002, 94, 1745–1757. [Google Scholar]
- Kirtikara, K; Morham, SG; Raghow, R; Laulederkind, SJ; Kanekura, T; Goorha, S; Ballou, LR. Compensatory prostaglandin E2 biosynthesis in cyclooxygenase 1 or 2 null cells. J. Exp. Med 1998, 187, 517–523. [Google Scholar]
- Hales, DB; Zhuge, Y; Lagman, JA; Ansenberger, K; Mahon, C; Barua, A; Luborsky, JL; Bahr, JM. Cyclooxygenases expression and distribution in the normal ovary and their role in ovarian cancer in the domestic hen (Gallus domesticus). Endocrine 2008, 33, 235–244. [Google Scholar]
- Urick, ME; Johnson, PA. Cyclooxygenase 1 and 2 mRNA and protein expression in the Gallus domesticus model of ovarian cancer. Gynecol. Oncol 2006, 103, 673–678. [Google Scholar]
- Li, W; Ji, ZL; Zhuo, GC; Xu, RJ; Wang, J; Jiang, HR. Effects of a selective cyclooxygenase- 1 inhibitor in SKOV-3 ovarian carcinoma xenograft-bearing mice. Med. Oncol 2010, 27, 98–104. [Google Scholar]
- Dore, M; Cote, LC; Mitchell, A; Sirois, J. Expression of prostaglandin G/H synthase type 1, but not type 2, in human ovarian adenocarcinomas. J. Histochem. Cytochem 1998, 46, 77–84. [Google Scholar]
- Tsujii, M; Kawano, S; Tsuji, S; Sawaoka, H; Hori, M; DuBois, RN. Cyclooxygenase regulates angiogenesis induced by colon cancer cells. Cell 1998, 93, 705–716. [Google Scholar]
- Narko, K; Ristimäki, A; MacPhee, M; Smith, E; Haudenschild, CC; Hla, T. Tumorigenic transformation of immortalized ECV endothelial cells by cyclooxygenase-1 overexpression. J. Biol. Chem 1997, 272, 21455–21460. [Google Scholar]
- Williams, CS; Watson, AJ; Sheng, H; Helou, R; Shao, J; DuBois, RN. Celecoxib prevents tumor growth in vivo without toxicity to normal gut: lack of correlation between in vitro and in vivo models. Cancer Res 2000, 60, 6045–6051. [Google Scholar]
- Gerdes, J; Lemke, H; Baisch, H; Wacker, HH; Schwab, U; Stein, H. Cell cycle analysis of a cell proliferationassociated human nuclear antigen defined by the monoclonal antibody Ki-67. J. Immunol 1984, 133, 1710–1715. [Google Scholar]
- Del Vecchio, MT; Leoncini, L; Buerki, K; Kraft, R; Megha, T; Barbini, P; Tosi, P; Cottier, H. Diffuse controcytic and/or centroblastic malignant non-Hodgkins lymphomas: comparison of mitotic and pyknotic (apoptotic) indices. Int. J Cancer 1991, 47, 38–43. [Google Scholar]
- Kitamura, T; Itoh, M; Noda, T; Matsuura, M; Wakabayashi, K. Combined effects of cyclooxygenase-1 and cyclooxygenase-2 selective inhibitors on intestinal tumorigenesis in adenomatous polyposis coli gene knockout mice. Int. J Cancer 2004, 109, 576–580. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Day b | Fractional Tumor Volume (FTV) Relative to Untreated Controls a | ||||
|---|---|---|---|---|---|
| SC-560 | Celecoxib | Combination Treatment | Ratio of Expected TV/Observed FTV d | ||
| Expected c | Observed | ||||
| 17 | 1.027 | 0.923 | 0.948 | 0.807 | 1.175 |
| 21 | 0.988 | 0.880 | 0.869 | 0.704 | 1.234 |
| 24 | 1.036 | 0.949 | 0.983 | 0.700 | 1.404 |
© 2011 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Li, W.; Wang, J.; Jiang, H.-R.; Xu, X.-L.; Zhang, J.; Liu, M.-L.; Zhai, L.-Y. Combined Effects of Cyclooxygenase-1 and Cyclooxygenase-2 Selective Inhibitors on Ovarian Carcinoma in Vivo. Int. J. Mol. Sci. 2011, 12, 668-681. https://doi.org/10.3390/ijms12010668
Li W, Wang J, Jiang H-R, Xu X-L, Zhang J, Liu M-L, Zhai L-Y. Combined Effects of Cyclooxygenase-1 and Cyclooxygenase-2 Selective Inhibitors on Ovarian Carcinoma in Vivo. International Journal of Molecular Sciences. 2011; 12(1):668-681. https://doi.org/10.3390/ijms12010668
Chicago/Turabian StyleLi, Wei, Jie Wang, Hong-Ru Jiang, Xiao-Li Xu, Jun Zhang, Mei-Lin Liu, and Ling-Yun Zhai. 2011. "Combined Effects of Cyclooxygenase-1 and Cyclooxygenase-2 Selective Inhibitors on Ovarian Carcinoma in Vivo" International Journal of Molecular Sciences 12, no. 1: 668-681. https://doi.org/10.3390/ijms12010668