2.6. Discussion
PVRL is a potentially fatal malignant disease and accurate diagnosis is of critical importance for prompt and appropriate intervention. The gold standard for PVRL diagnosis is detection of lymphoma cells in the retina and/or vitreous. Additionally, clinical manifestations and examinations are important for the diagnosis of PVRL. This study suggests that the molecular analysis of IgH and TCR gene rearrangements using microdissection and PCR technique has the highest sensitivity, specificity, predictive value, and efficiency for the diagnosis of PVRL, when compared with morphological identification of atypical lymphoid cells or IL-10 to IL-6 ratio analysis. Moreover, detection of IgH or TCR gene rearrangements in the microdissected atypical lymphoid cells greatly facilitates the diagnosis and classification of PVRL. The molecular analysis correlates well with the clinical diagnosis of PVRL and can be used as reliable biomarkers for the diagnosis and classification of PVRL.
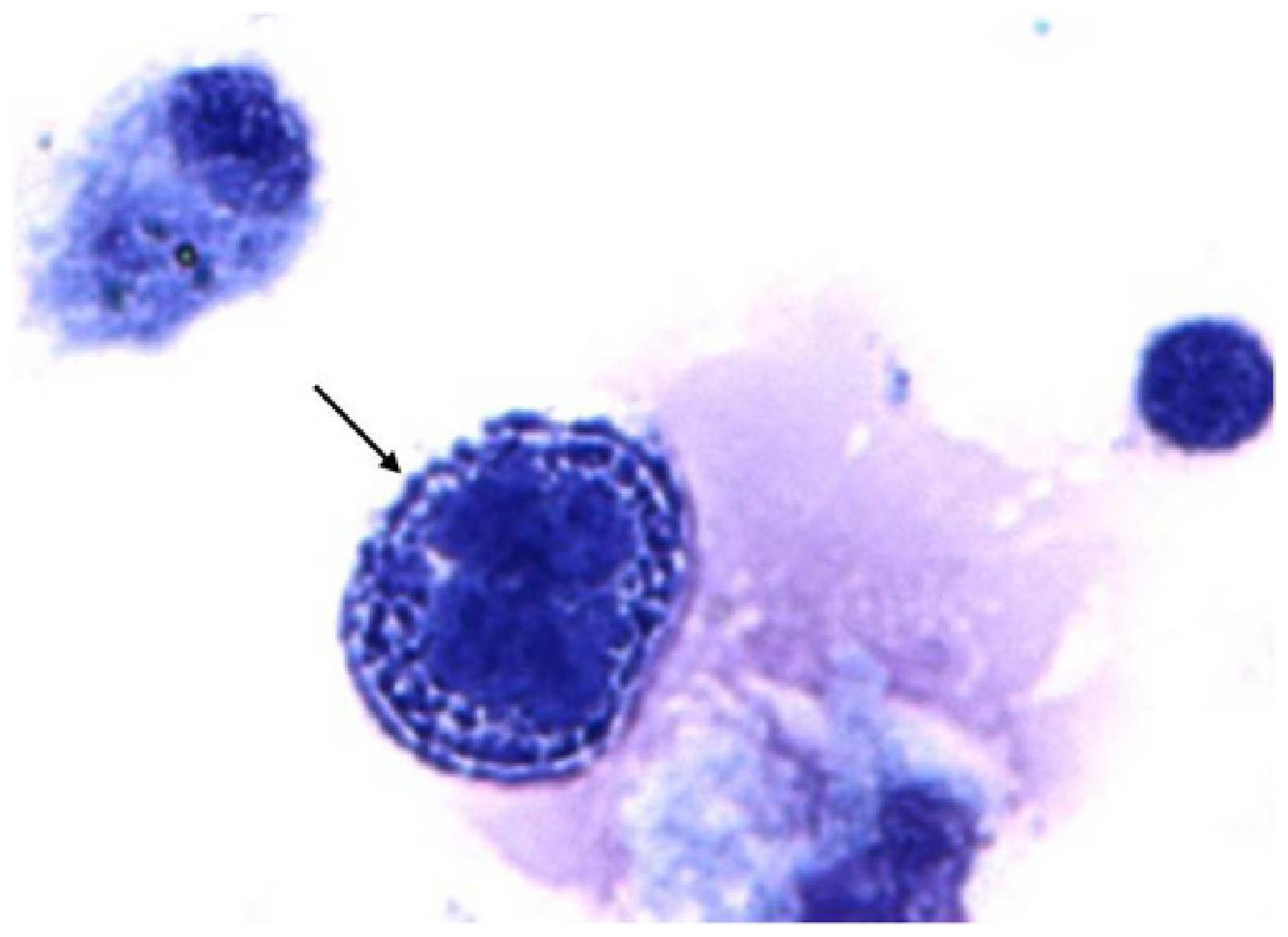
PVRL usually masquerades as uveitis; thus, identification of lymphoma cells in the eye is required for the diagnosis of PVRL. Typical lymphoma cells are characterized by large nuclei, prominent nucleoli, and scanty basophilic cytoplasm [
27,
28]. These atypical lymphoid cells are 2–4 times the size of normal, naive lymphocytes and may have irregular nuclear contours, a fine to coarse chromatin pattern and scanty basophilic cytoplasm [
29]. Although PVRL cells have characteristic features, they are very fragile and easily degenerate in the specimen and even in the eye [
8,
12]. If the specimen is not promptly transported and/or carefully processed, most PVRL cells will show degeneration or may even become necrotic. In this study, 12% of the specimens did not have identifiable cells due to poor morphology, resulting in no diagnosis based on cytology alone.
Although cytological analysis is critical for identifying tumor cells in PVRL, further classification of the cell origin of lymphoma cells must rely on immunophenotyping using techniques such as immunohistochemistry or flow cytometry. Immunohistochemistry staining of the B cell marker (e.g., CD19, CD20, lambda, and kappa) and T cell marker (e.g., CD3) help differentiate the monoclonality of lymphoma cells. Other studies have reported that flow cytometric immunophenotyping is a useful alternative to conventional diagnostic techniques. It refines cytological diagnosis and helps in the classification of ocular lymphoma [
30,
31]. However, flow cytometric immunophenotyping requires relatively larger quantities of material and ocular specimens are often limited to very small amounts [
31]. Thus, the paucity and fragility of the lymphoma cells in the eye restrict the application of immunophenotyping analysis for PVRL diagnosis and classification.
PVRL cells show monoclonal rearrangement of
IgH genes in B-cell lymphoma and
TCR genes in T-cell lymphoma. This feature favors the molecular diagnosis and classification of lymphoma using microdissection to procure the atypical lymphoid cells and PCR to detect gene rearrangements in these cells. The antigen-binding sites of IgH and TCR molecules are encoded by sets of gene regions that include variable (V), diversity (D), and jointing (J) gene regions. The variable region undergoes gene rearrangements that increase the diversity of the immune receptor repertoire [
17,
32]. Among them,
CDR3 in the V(D)J region of the
IgH gene and
TCR gamma in
TCR gene are regarded as the most common sites of gene arrangement [
5,
8,
16,
17]. Because lymphoma usually derives from a single B or T cell, the tumor cell has the features of monoclonality. Thus, gene rearrangements of
IgH and
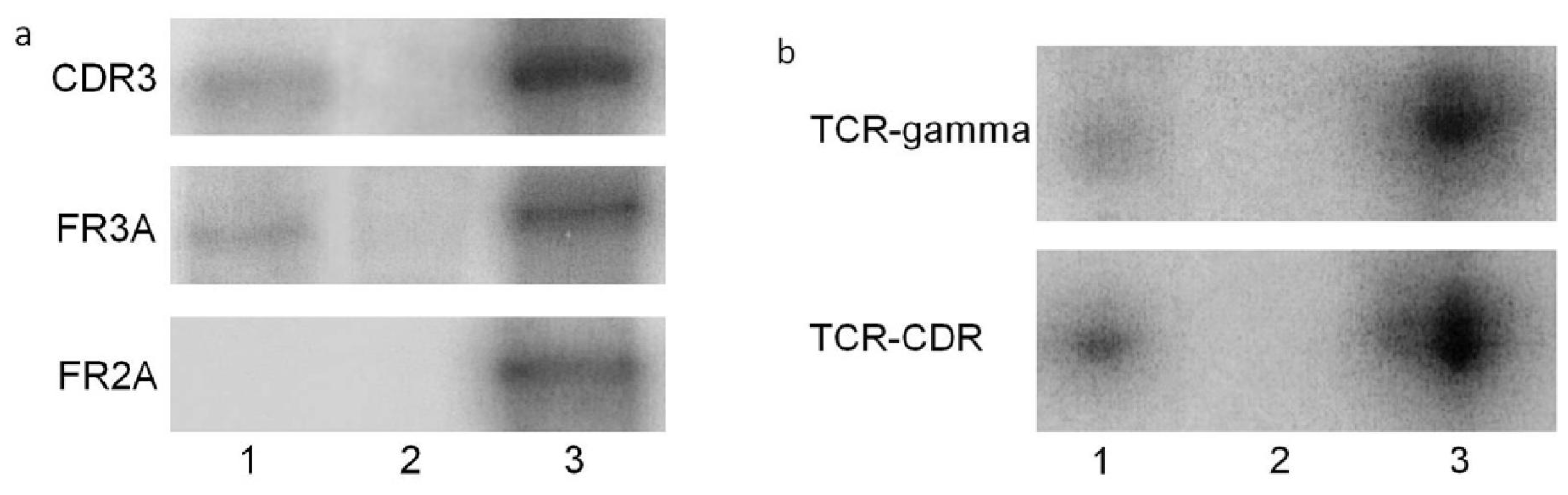
TCR in lymphoma cells serve as reliable biomarkers for the diagnosis and classification of PVRL. In this study, 114 cases of B-cell lymphoma are identified by molecular analysis using primers
FR2A,
FR3A, and/or
CDR3 that cover the
CDR3 region of the
IgH gene in B-cell lymphoma. Five cases of T-cell PVRL are confirmed by the positive
TCR gene arrangement using primer
TCR-gamma and/or
TCR-CDR3 in T-cell PVRL. Only one uveitis case showed
IgH gene rearrangement in the
CDR3 region. No atypical lymphoid cells were found and a proinflammatory cytokine profile was measured in this specimen; therefore, the molecular data alone could not support a diagnosis of lymphoid neoplasm for this patient. The patient responded to anti-inflammatory therapy eventually. Though rare, molecular analysis could yield false positive results.
Because PVRL cells often admix with many reactive lymphocytes and necrotic cells, microdissection of at least 15 atypical lymphoid cells in individual specimens likely guarantees the purity of the cell source for PCR, which greatly improves the accuracy of PVRL diagnosis via molecular analysis. By using microdissection and PCR, the sensitivity and specificity was nearly 100% in patients with PVRL in our study. In comparison, others reported molecular diagnosis rates of approximately 60% [
33,
34] and specificity around 0.64 in smaller case series [
35]. In those molecular studies, however, microdissection was not performed.
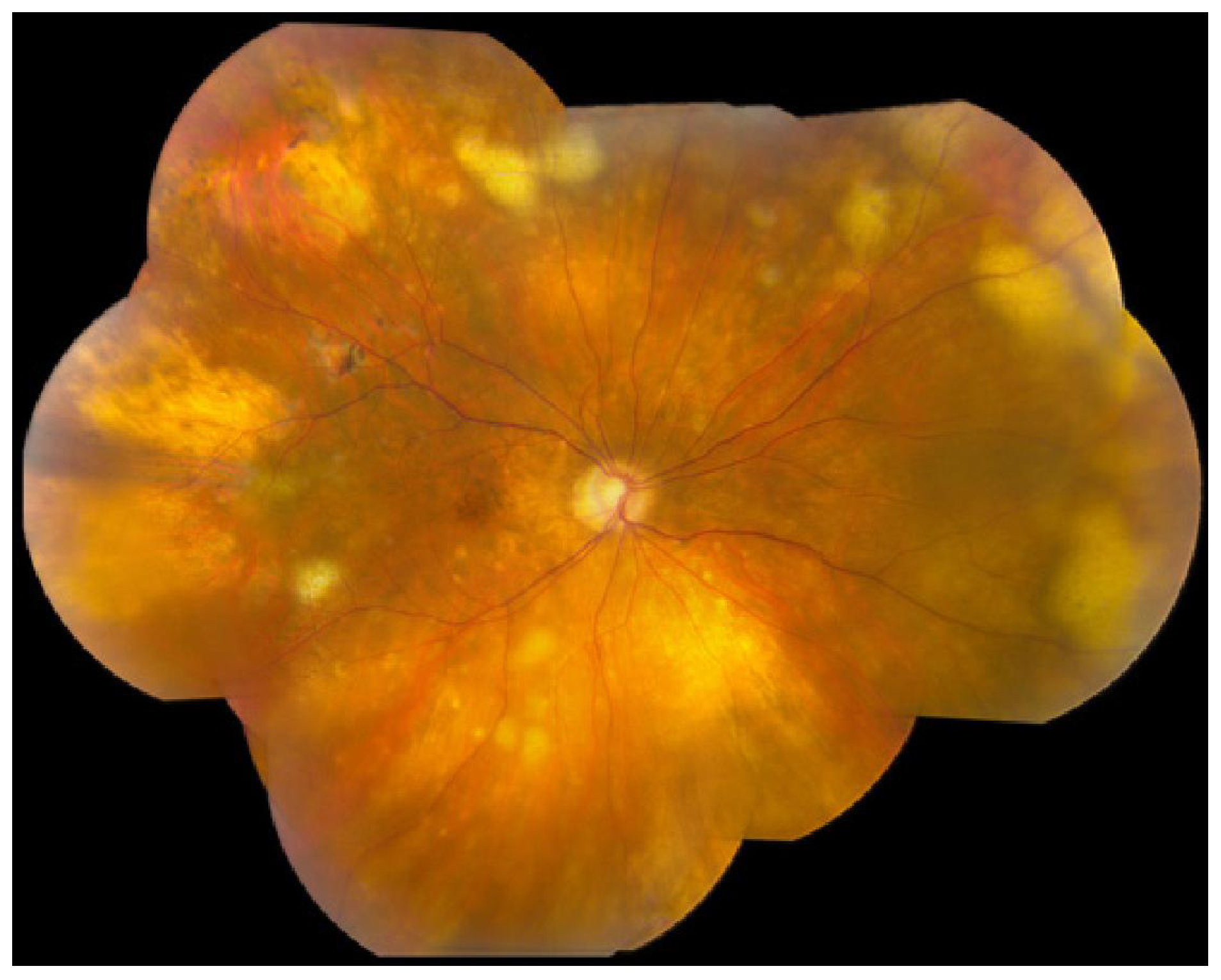
Vitreous biopsy remains the mainstay of PVRL diagnosis. Clinically, vitreous fluids are obtained by vitreous aspiration or pars plana vitrectomy. Our results showed that the majority of submitted specimens (77%) were vitreous samples. Vitreous and aqueous fluids often have sparsely distributed tumor cells admixed with many reactive lymphocytes and debris, which make it difficult for pathologists to differentiate tumor cells from inflammatory cellular contents. Moreover, lymphoma cells tend to have poor morphology due to prior corticosteroid treatment, mechanical damage during vitrectomy and/or prolonged processing procedure [
11,
36,
37]. All of these reasons make PVRL diagnosis challenging. Aqueous is anatomically farther away from the lymphoma lesions than the vitreous simply because PVRL presents in the vitreous and retina. Although fewer PVRL cells are present in the aqueous than in the vitreous, lymphoma cells were found in 2 of the 4 PVRL cases with aqueous specimens. Of the same 4 PVRL cases, 3 had elevated IL-10 levels, which facilitated the final diagnosis of PVRL. Cassoux
et al. also reported that cytokine measurements of the aqueous could be used as a good screening method for PVRL diagnosis [
24]. Other intraocular specimens, such as retina/chorioretina and subretinal fluids, are usually chosen when PVRL cells are absent in the vitreous samples [
38–
41]. In general, PVRL cells are easier to detect in the retina and subretinal space, where they initially reside.
An IL-10 to IL-6 ratio greater than 1 in ocular fluid is highly suggestive of PVRL [
26]. However, IL-10 secretion is affected by not only activated and malignant B cells, but also by other cells, such as Th1 and Th2 cells [
42,
43], and by many other factors, such as IL-12 levels [
44]. In our study, 3 uveitic specimens (2 vitreous and 1 aqueous) showed elevated vitreous IL-10 levels and an IL-10 to IL-6 ratio greater than 1. Akpek
et al. [
45] also reported that the IL-10 to IL-6 ratio was greater than 1 in 8 of 13 patients with non-neoplastic uveitis. In contrast, 7 (11.7%) PVRL cases showed a vitreous IL-10 to IL-6 ratio less than 1 in our study. Three of these were of T-cell origin and the low IL-10 level was compatible with the diagnosis of T-cell lymphoma [
21]. Low IL-10 to IL-6 levels in B-cell lymphomas have also been reported in other studies [
45,
46]. This change may occur in patients who were in the early stage of lymphoma or in patients who have been previously treated with corticosteroids or immunosuppressive agents that influence the cytokine profile. Although an IL-10 to IL-6 ratio greater than 1 in the vitreous is suggestive of PVRL, this ratio cannot be used as the sole biomarker for PVRL diagnosis. However, cytokine analysis showed higher sensitivity and negative predicative value in this study, suggesting that it may serve as a useful adjunctive tool for screening patients suspected of PVRL.





{kind=link}
{kind=link}
{kind=link}