Nonselective Blocking of the Sympathetic Nervous System Decreases Detrusor Overactivity in Spontaneously Hypertensive Rats

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results and Discussion
2.1. Results
2.1.1. Body and Bladder Weights, Normalized Ratios between Them, and Systemic Blood Pressure
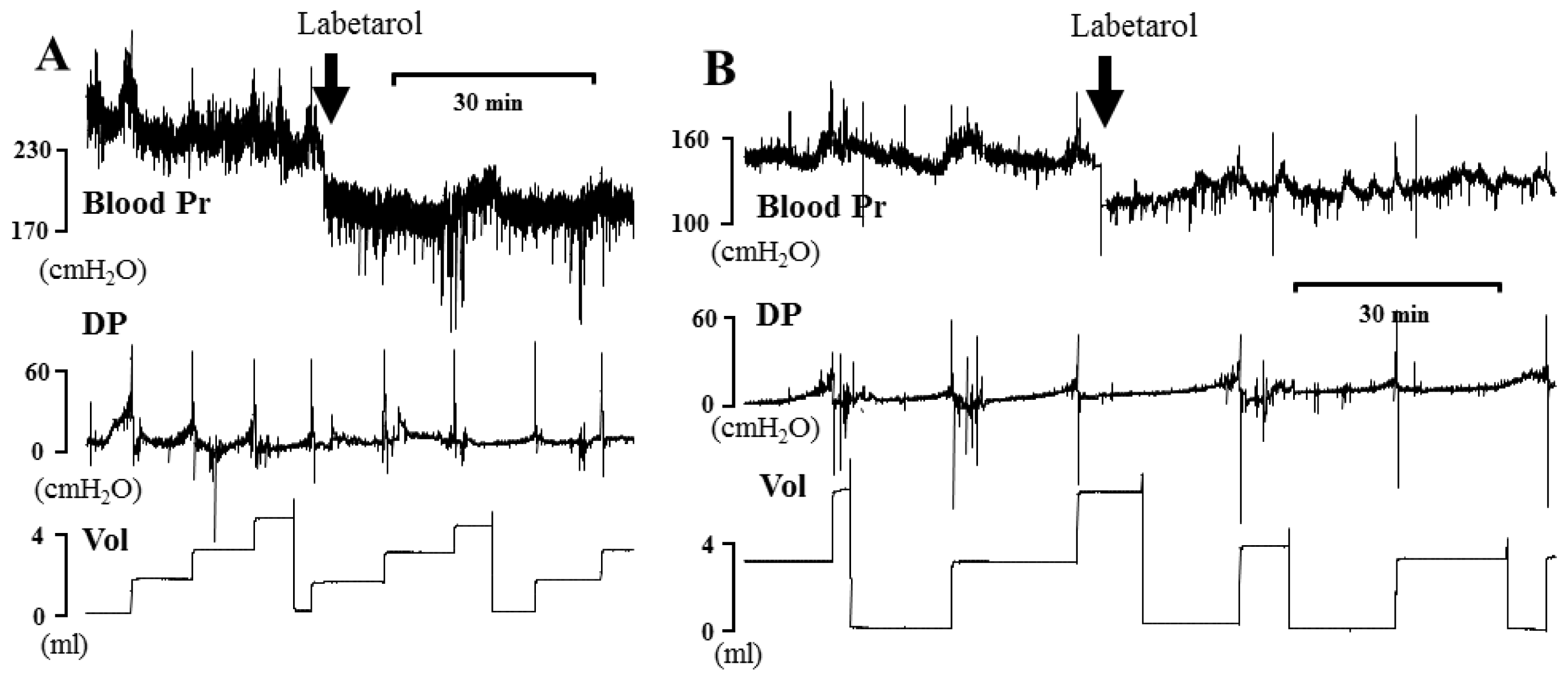
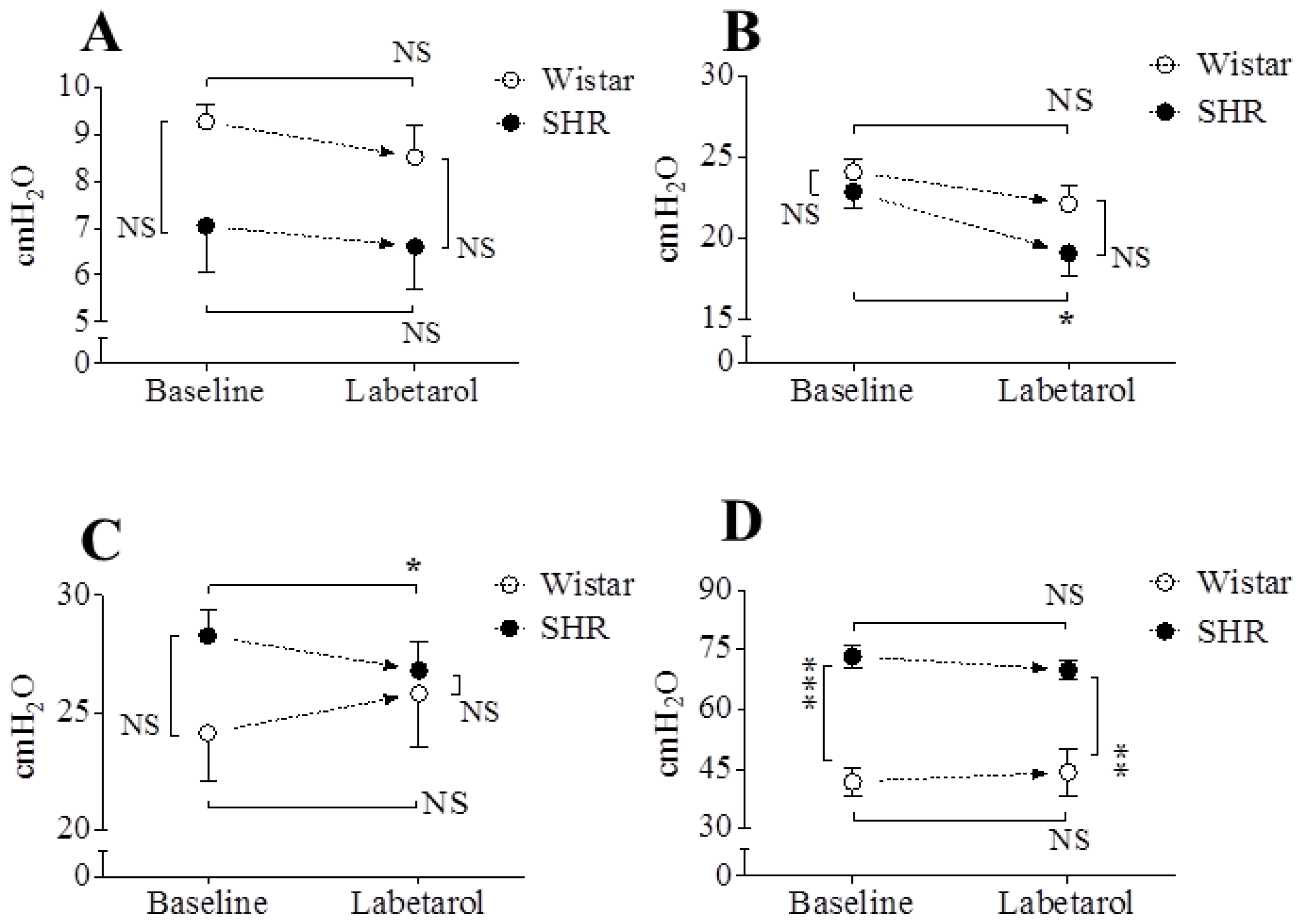
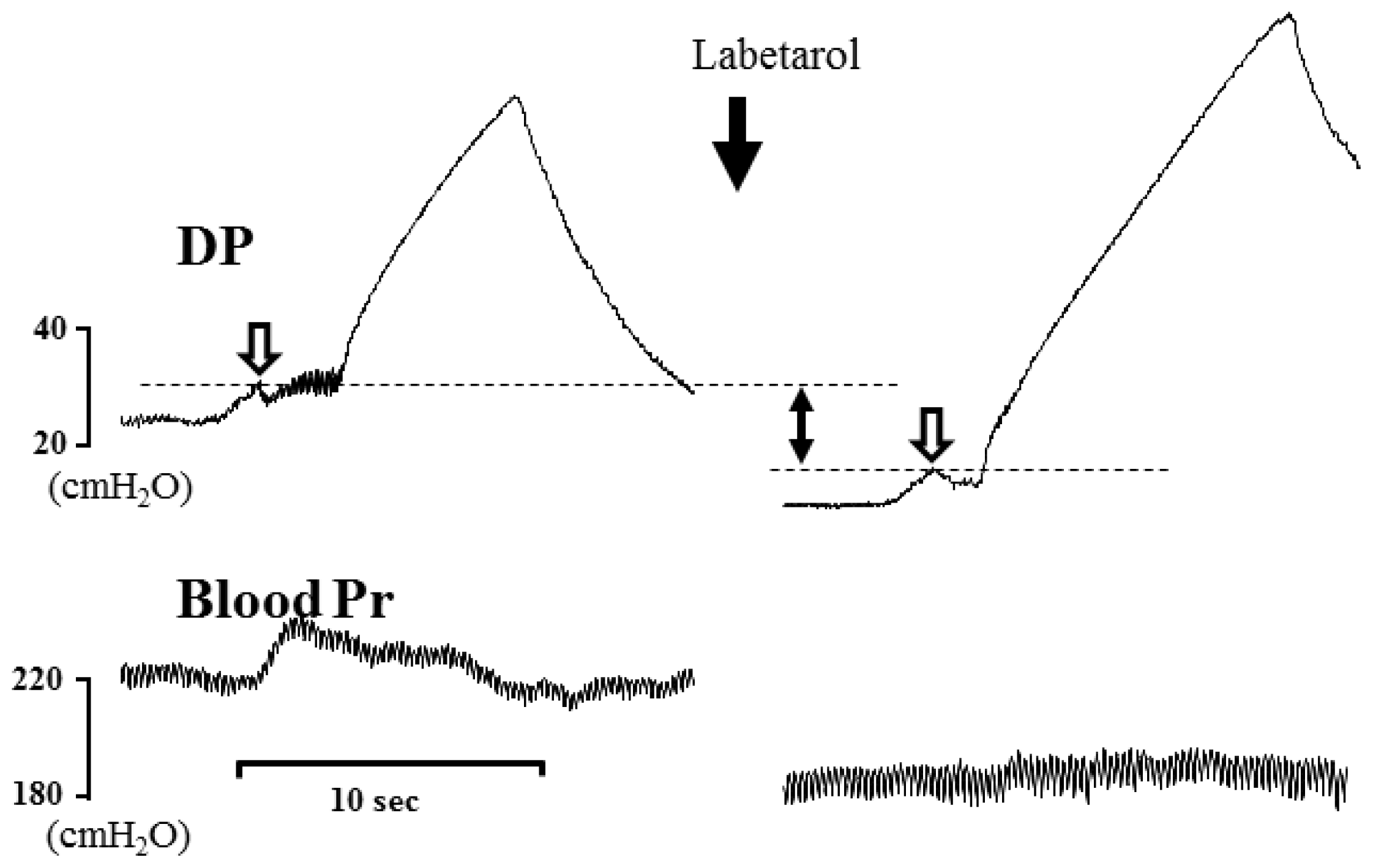
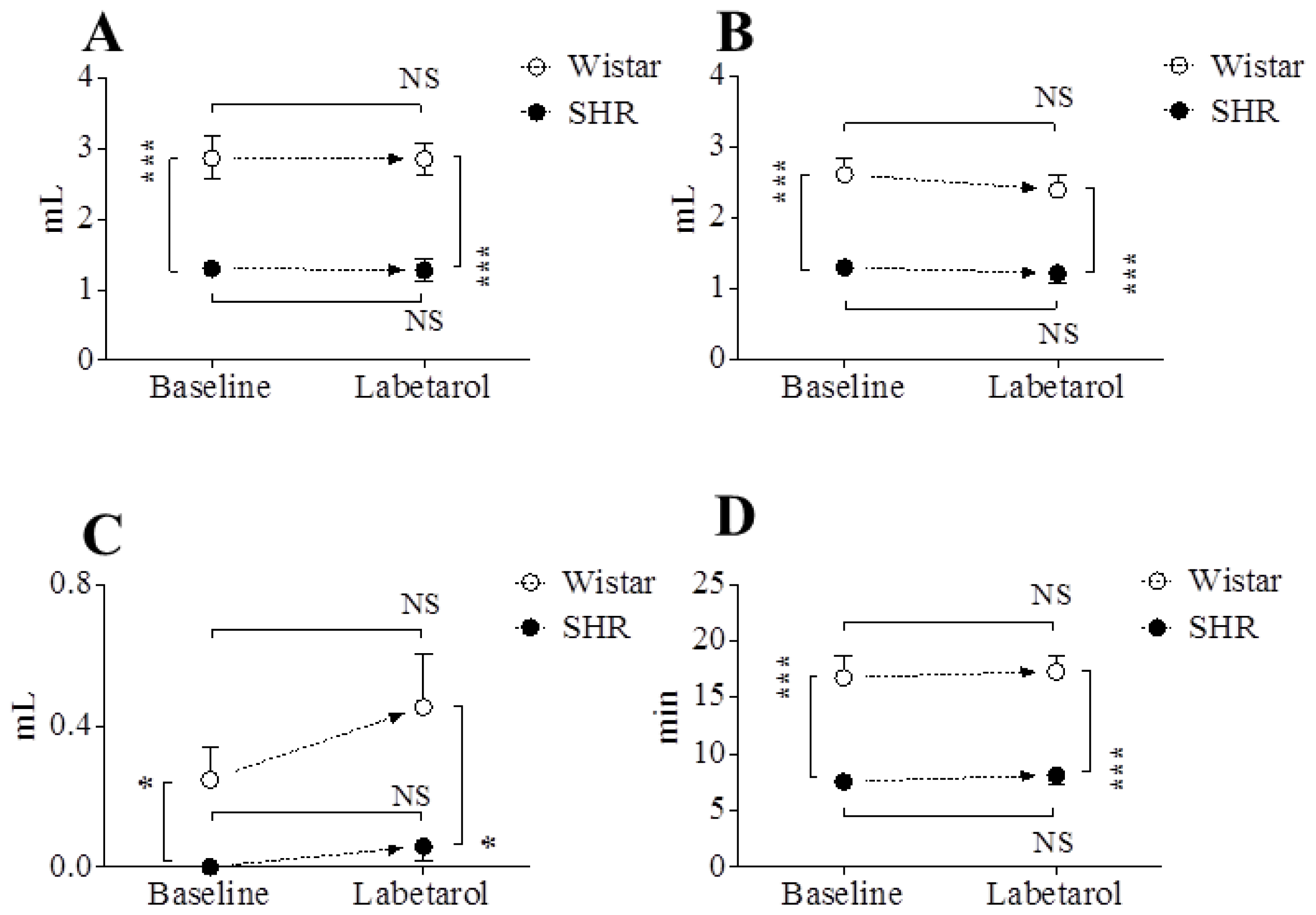
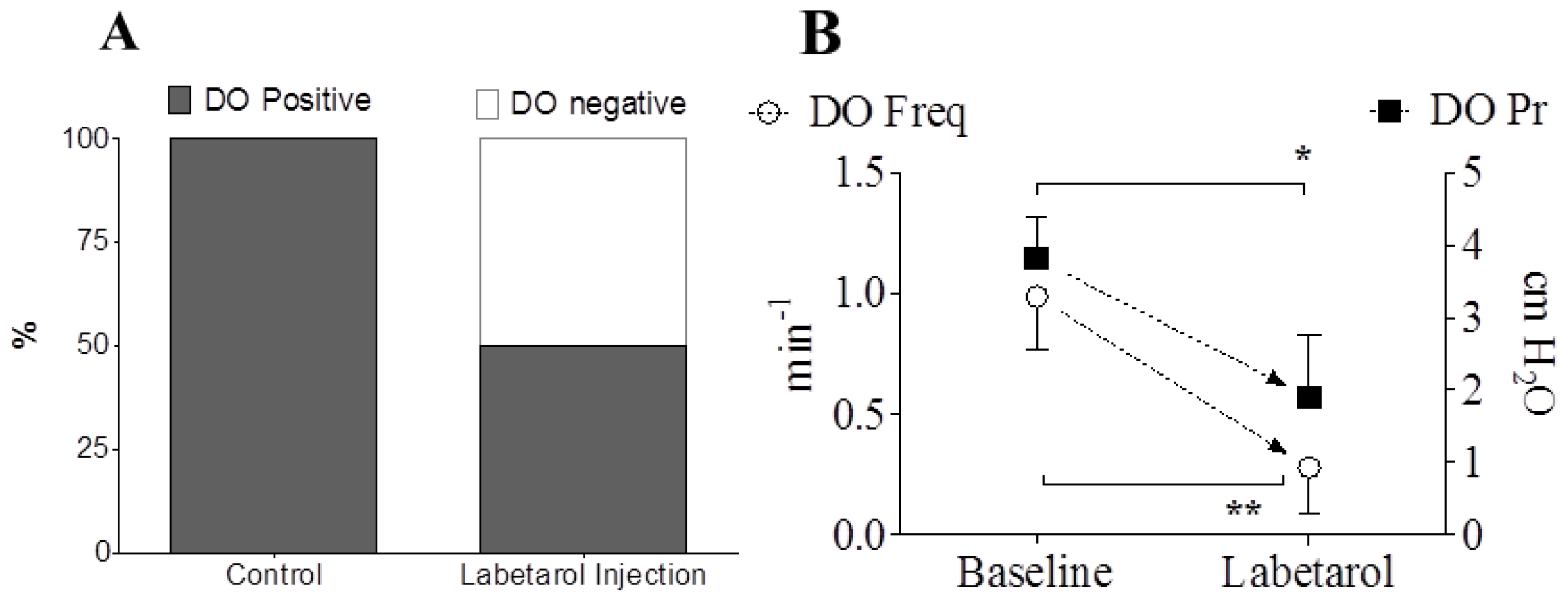
2.1.2. Cystometric Parameters before and after the Intraarterial Injection of Labetalol
2.2. Discussion
3. Experimental Section
3.1. Animals
3.2. Surgical Procedures
3.3. In Vivo Cystometric Investigations and Analysis
- Pressure- and volume-related parameters derived from detrusor pressure: Basal pressure (BP; the lowest bladder pressure during filling), FP (bladder pressure at the time of start of flow of urine from the urethra), threshold pressure (TP; bladder pressure immediately before micturition), maximum pressure (MP; maximum bladder pressure during the micturition cycle), micturition volume (MV; volume of expelled urine), residual volume (RV; remaining urine after voiding), bladder capacity (BC; MV + RV), and micturition interval (MI; intervals between micturition contractions).
- DO-related parameters during the filling phase: Time of filling phase (interval from the initiation of infusion through the tube and the point immediately before the initiation of micturition), frequency of abdominal straining per minute, frequency of DO per minute, and increased amplitude from base to peak of DO spike as IVP. These frequencies were calculated on the basis of the time of filling phase.
3.4. Statistical Analyses
4. Conclusions
Acknowledgments
- Conflict of Interest We have no potential conflict of interest relevant to this article.
References
- Abrams, P.; Cardozo, L.; Fall, M.; Griffiths, D.; Rosier, P.; Ulmsten, U.; van Kerrebroeck, P.; Victor, A.; Wein, A. The standardisation of terminology of lower urinary tract function: report from the Standardisation Sub-committee of the International Continence Society. Neurourol. Urodyn 2002, 21, 167–178. [Google Scholar]
- Al Ghazo, M.A.; Ghalayini, I.F.; Al Azab, R.; Hani, O.B.; Matani, Y.S.; Haddad, Y. Urodynamic detrusor overactivity in patients with overactive bladder symptoms. Int. Neurourol. J 2011, 15, 48–54. [Google Scholar]
- Milsom, I.; Abrams, P.; Cardozo, L.; Roberts, R.G.; Thuroff, J.; Wein, A.J. How widespread are the symptoms of an overactive bladder and how are they managed? A population-based prevalence study. BJU Int 2001, 87, 760–766. [Google Scholar]
- Stewart, W.F.; van Rooyen, J.B.; Cundiff, G.W.; Abrams, P.; Herzog, A.R.; Corey, R.; Hunt, T.L.; Wein, A.J. Prevalence and burden of overactive bladder in the United States. World J. Urol 2003, 20, 327–336. [Google Scholar]
- Hashim, H.; Abrams, P. Overactive bladder: An update. Curr. Opin. Urol 2007, 17, 231–236. [Google Scholar]
- Andersson, K.E.; Arner, A. Urinary bladder contraction and relaxation: Physiology and pathophysiology. Physiol. Rev 2004, 84, 935–986. [Google Scholar]
- Kollai, M.; Koizumi, K. Cardiovascular reflexes and interrelationships between sympathetic and parasympathetic activity. J. Auton. Nerv. Syst 1981, 4, 135–148. [Google Scholar]
- Choi, J.B.; Kim, Y.B.; Kim, B.T.; Kim, Y.S. Analysis of heart rate variability in female patients with overactive bladder. Urology 2005, 65, 1109–1112. [Google Scholar]
- Blanc, F.; Pichot, V.; Roche, F.; Barthelemy, J.C.; Tostain, J. Activity of the autonomous nervous system measured based on the variability of heart rate in female urinary incontinence. Prog. Urol 2001, 11, 492–497. [Google Scholar]
- Yoo, E.S.; Kim, B.S.; Kim, D.Y.; Oh, S.J.; Kim, J.C. The impact of overactive bladder on health-related quality of life, sexual life and psychological health in Korea. Int. Neurourol. J 2011, 15, 143–151. [Google Scholar]
- Kim, J.C.; Joo, K.J.; Kim, J.T.; Choi, J.B.; Cho, D.S.; Won, Y.Y. Alteration of autonomic function in female urinary incontinence. Int. Neurourol. J 2010, 14, 232–237. [Google Scholar]
- De Groat, W.C. Integrative control of the lower urinary tract: Preclinical perspective. Br. J. Pharmacol 2006, 147, S25–S40. [Google Scholar]
- McVary, K.T.; Rademaker, A.; Lloyd, G.L.; Gann, P. Autonomic nervous system overactivity in men with lower urinary tract symptoms secondary to benign prostatic hyperplasia. J. Urol 2005, 174, 1327–1433. [Google Scholar]
- Hendley, E.D.; Ohlsson, W.G. Two new inbred rat strains derived from SHR: WKHA, hyperactive, and WKHT, hypertensive, rats. Am. J. Physiol 1991, 261, H583–H589. [Google Scholar]
- Cloutier, F.; Ongali, B.; Deschamps, K.; Brouillette, J.; Neugebauer, W.; Couture, R. Upregulation of tachykinin NK-1 and NK-3 receptor binding sites in the spinal cord of spontaneously hypertensive rat: Impact on the autonomic control of blood pressure. Br. J. Pharmacol 2006, 148, 25–38. [Google Scholar]
- Norman, R.A., Jr; Dzielak, D.J. Spontaneous hypertension is primarily the result of sympathetic overactivity and immunologic dysfunction. Proc. Soc. Exp. Biol. Med 1986, 182, 448–453. [Google Scholar]
- Lee, T.; Andersson, K.E.; Streng, T.; Hedlund, P. Simultaneous registration of intraabdominal and intravesical pressures during cystometry in conscious rats—Effects of bladder outlet obstruction and intravesical PGE2. Neurourol. Urodyn 2008, 27, 88–95. [Google Scholar]
- Hubeaux, K.; Deffieux, X.; Ismael, S.S.; Raibaut, P.; Amarenco, G. Autonomic nervous system activity during bladder filling assessed by heart rate variability analysis in women with idiopathic overactive bladder syndrome or stress urinary incontinence. J. Urol 2007, 178, 2483–2487. [Google Scholar]
- Jin, L.H.; Park, C.S.; Shin, H.Y.; Yoon, S.M.; Lee, T. Dissimilar effects of tolterodine on detrusor overactivity in awake rats with chemical cystitis and partial bladder outlet obstruction. Int. Neurourol. J 2011, 15, 120–126. [Google Scholar]
- Clemow, D.B.; Spitsbergen, J.M.; McCarty, R.; Steers, W.D.; Tuttle, J.B. Altered NGF regulation may link a genetic predisposition for hypertension with hyperactive voiding. J. Urol 1999, 161, 1372–1377. [Google Scholar]
- Zweifach, B.W.; Kovalcheck, S.; de Lano, F.; Chen, P. Micropressure-flow relationships in a skeletal muscle of spontaneously hypertensive rats. Hypertension 1981, 3, 601–614. [Google Scholar]
- Jin, L.H.; Shin, H.Y.; Yoon, S.H.; Seong, D.H.; Park, C.S.; Lee, T.; Yoon, S.M. Time-related changes in detrusor overactivity in awake rats with spinal cord injury observed by simultaneous registrations of intravesical and intraabdominal pressures. Int. Neurourol. J 2011, 15, 19–24. [Google Scholar]
- Andersson, K.E. Antimuscarinic mechanisms and the overactive detrusor: An update. Eur. Urol 2011, 59, 377–386. [Google Scholar]






© 2012 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Kim, K.-H.; Jin, L.-H.; Choo, G.-Y.; Lee, H.-J.; Choi, B.-H.; Kwak, J.; Yoon, S.-M.; Park, C.-S.; Lee, T. Nonselective Blocking of the Sympathetic Nervous System Decreases Detrusor Overactivity in Spontaneously Hypertensive Rats. Int. J. Mol. Sci. 2012, 13, 5048-5059. https://doi.org/10.3390/ijms13045048
Kim K-H, Jin L-H, Choo G-Y, Lee H-J, Choi B-H, Kwak J, Yoon S-M, Park C-S, Lee T. Nonselective Blocking of the Sympathetic Nervous System Decreases Detrusor Overactivity in Spontaneously Hypertensive Rats. International Journal of Molecular Sciences. 2012; 13(4):5048-5059. https://doi.org/10.3390/ijms13045048
Chicago/Turabian StyleKim, Khae-Hawn, Long-Hu Jin, Gwoan-Youb Choo, Hun-Jae Lee, Bo-Hwa Choi, Jiyeon Kwak, Sang-Min Yoon, Chang-Shin Park, and Tack Lee. 2012. "Nonselective Blocking of the Sympathetic Nervous System Decreases Detrusor Overactivity in Spontaneously Hypertensive Rats" International Journal of Molecular Sciences 13, no. 4: 5048-5059. https://doi.org/10.3390/ijms13045048
APA StyleKim, K.-H., Jin, L.-H., Choo, G.-Y., Lee, H.-J., Choi, B.-H., Kwak, J., Yoon, S.-M., Park, C.-S., & Lee, T. (2012). Nonselective Blocking of the Sympathetic Nervous System Decreases Detrusor Overactivity in Spontaneously Hypertensive Rats. International Journal of Molecular Sciences, 13(4), 5048-5059. https://doi.org/10.3390/ijms13045048