Analysis of MTHFR and MTRR Gene Polymorphisms in Iranian Ventricular Septal Defect Subjects

Abstract
:1. Introduction
2. Results and Discussion
2.1. Socio-Demographic Characteristics
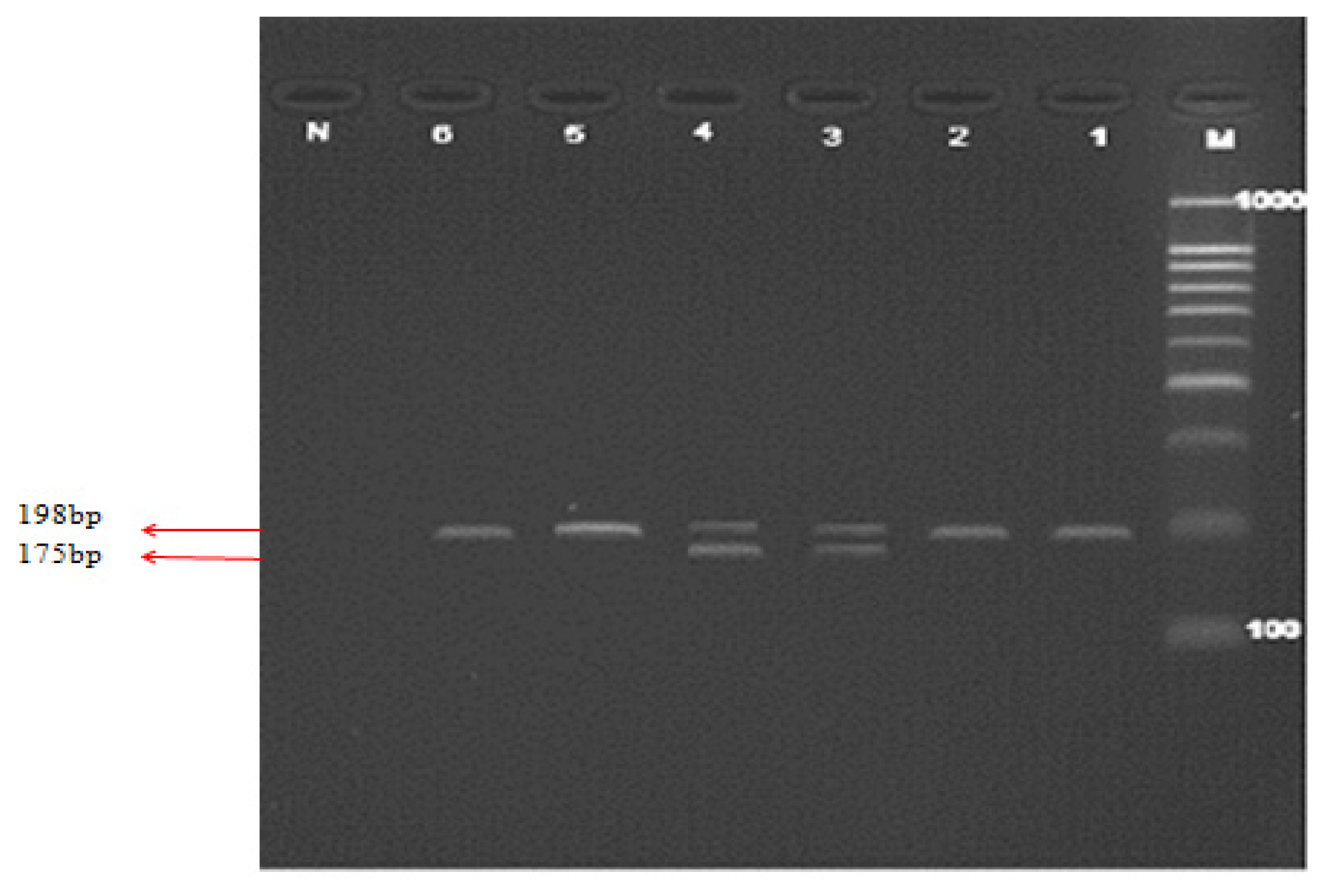
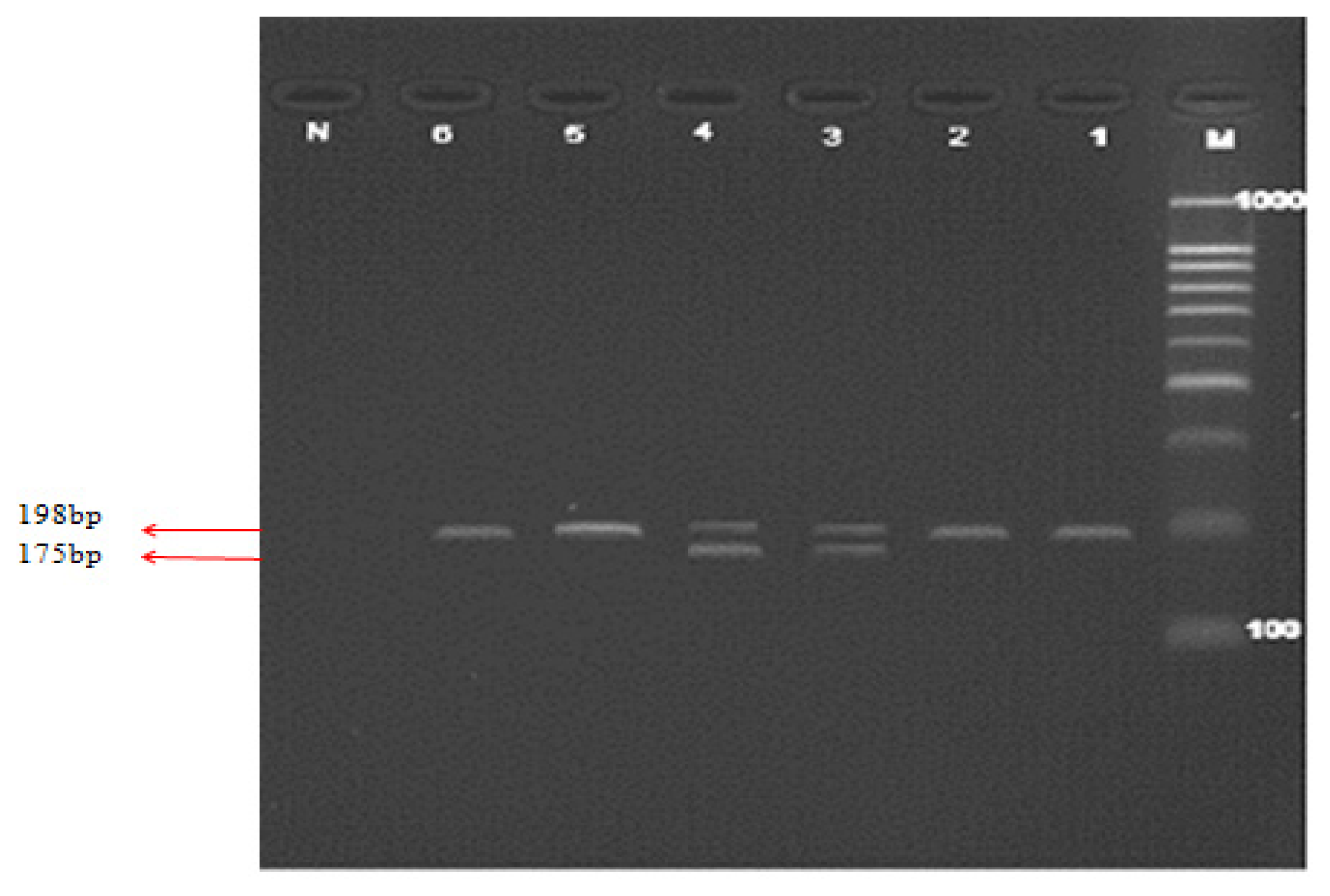
2.2. C677T Polymorphism of MTHFR Gene
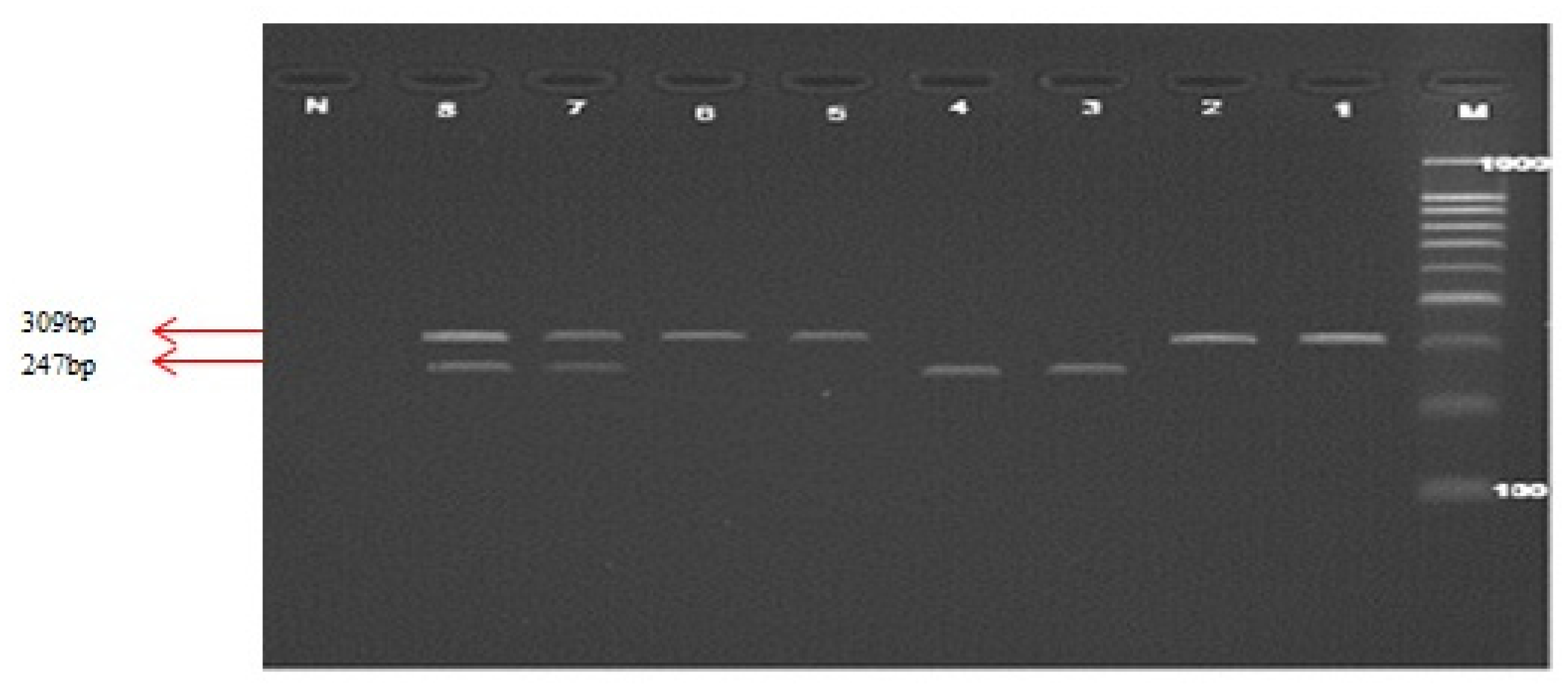
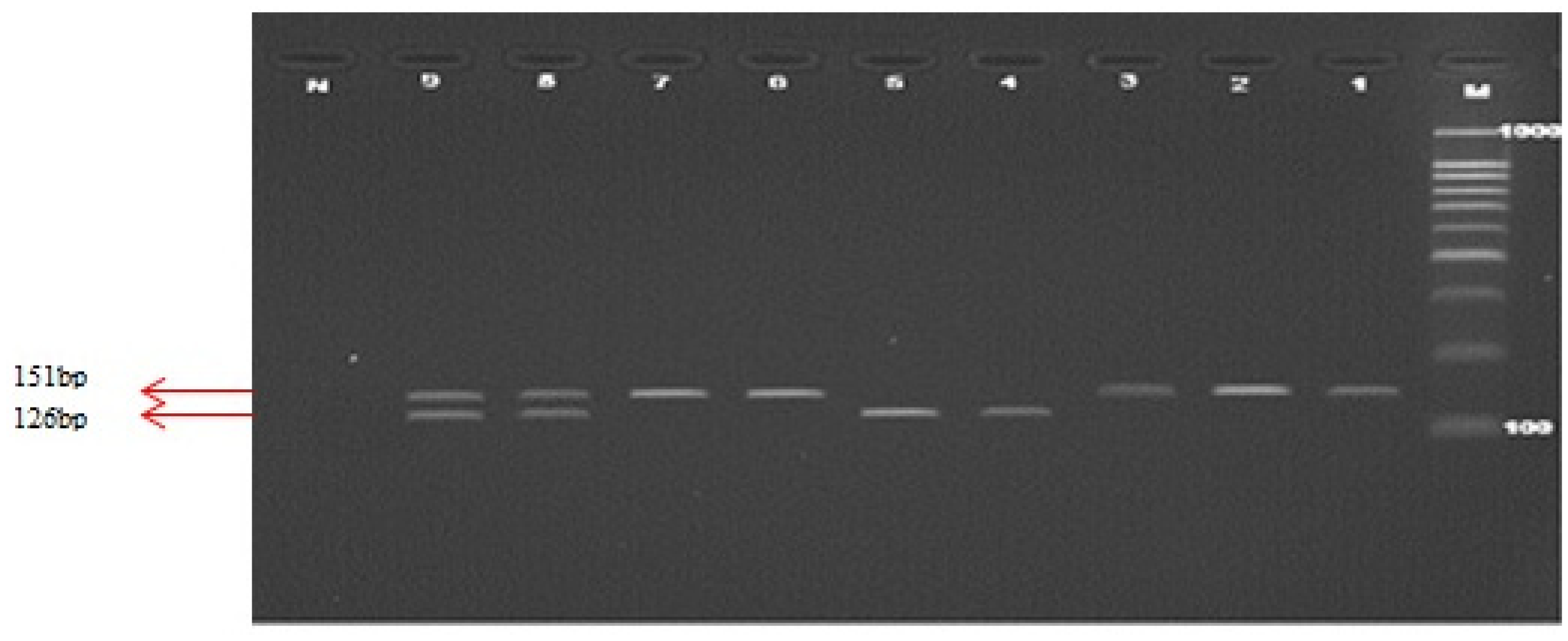
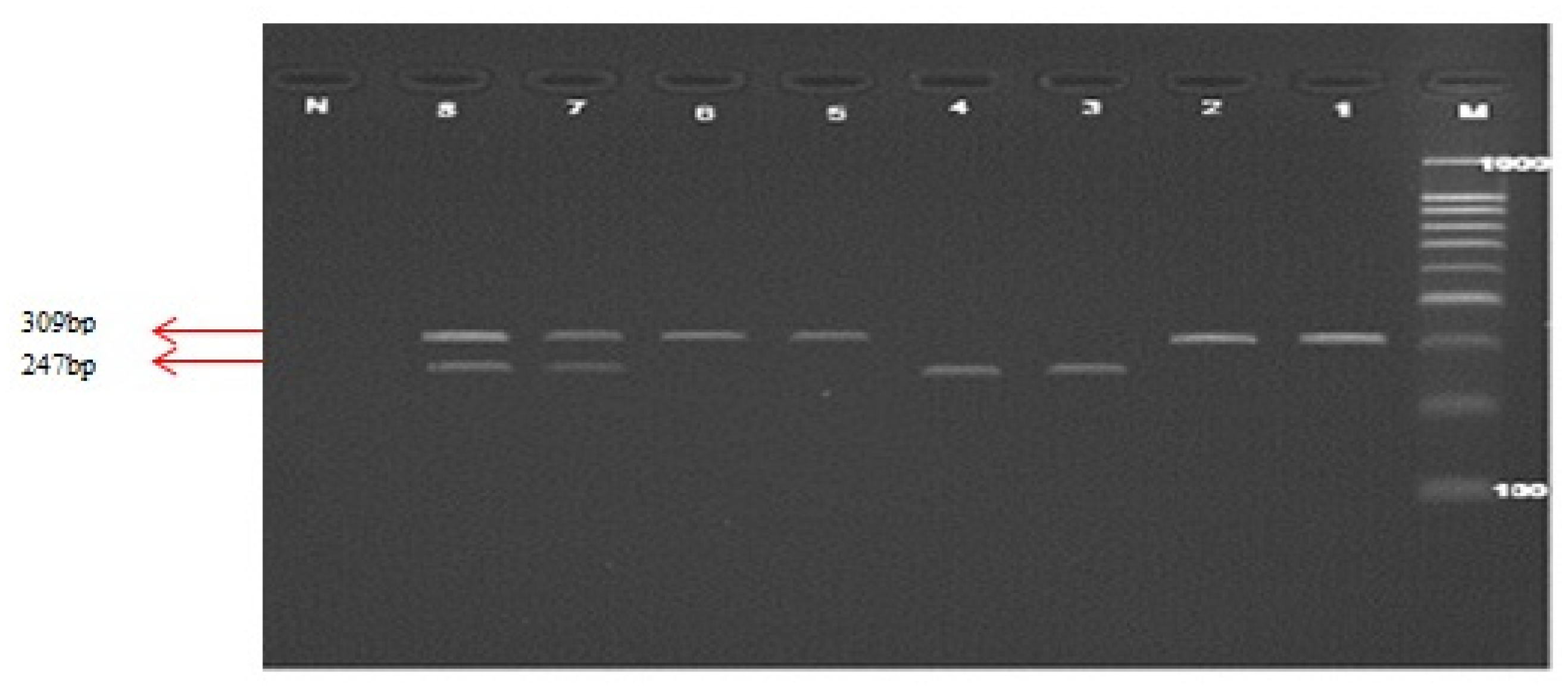
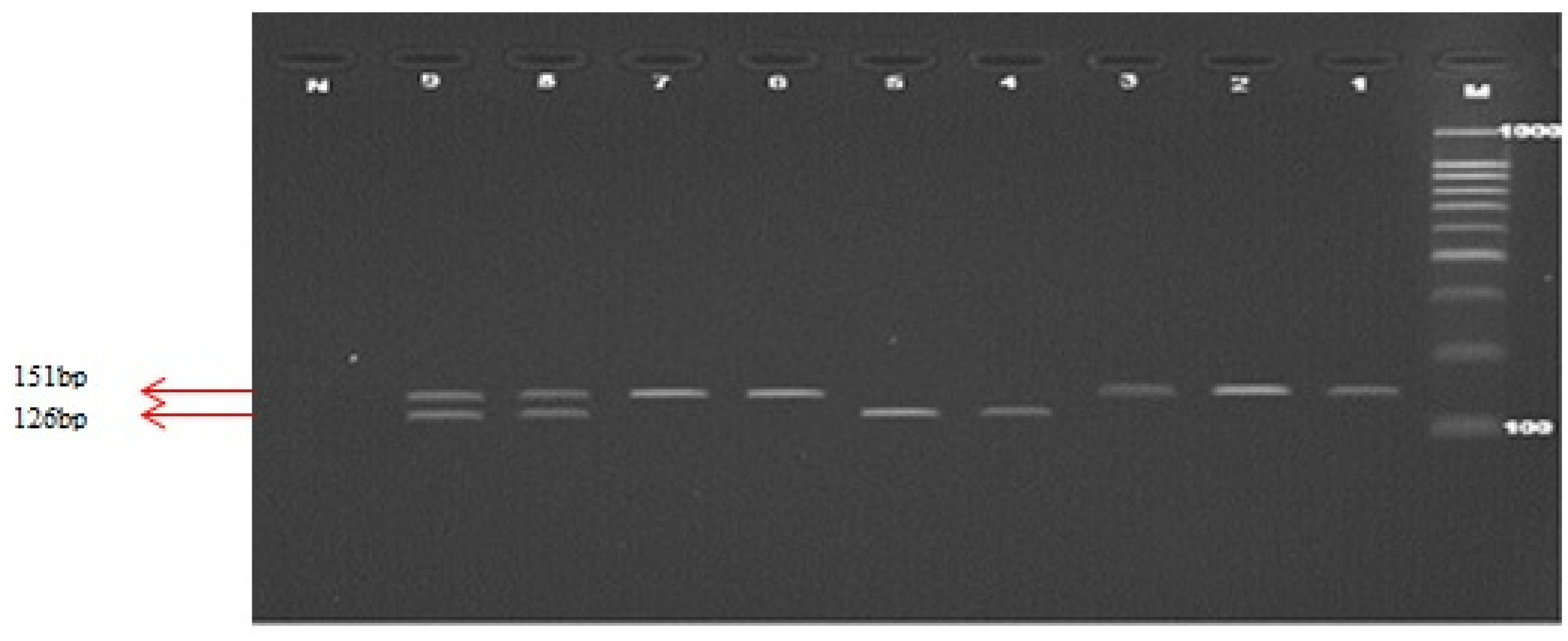
2.3. C524T and A66G Polymorphisms of MTRR Gene
2.4. DNA Sequencing
2.5. Study Limitations
3. Materials and Methods
3.1. Ethical Approval
3.2. Study Subjects
3.3. Genomic DNA Extraction
3.4. Genotyping MTHFR and MTRR Gene Polymorphisms
3.5. Automated Sequencing
3.6. Statistical Analysis
4. Conclusions
Acknowledgments
Conflict of Interest
References
- Liu, C.X.; Shen, A.D.; Li, X.F.; Jiao, W.W.; Bai, S.; Yung, F.; Guan, X.; Zhang, X.G.; Zhang, G.R.; Li, Z.Z. Association of TBX5 gene polymorphism with ventricular septal defect in the Chinese Han population. Chin. Med. J 2009, 122, 30–34. [Google Scholar]
- Van Beynum, I.M.; Blom, H.J.; Kapusta, L.; den Heijer, M. The MTHFR 677C→T polymorphism and the risk of congenital heart defects: A literature review and meta-analysis. QJM 2007, 100, 743–753. [Google Scholar]
- Shanley, T.P.; Wheeler, D.S.; Wong, H.R. Pediatric Critical Care Medicine: Basic Science and Clinical Evidence; Springer: New York, NY, USA, 2007. [Google Scholar]
- Minette, M.S.; Sahn, D.J. Congenital heart disease for the adult cardiologist, ventricular septal defects. Am. Heart Assoc 2006, 114, 2190–2197. [Google Scholar]
- Little, J.; Higgins, J.P.; Ioannidis, J.P.; Moher, D.; Gagnon, F.; von Elm, E.; Khoury, M.J.; Cohen, B.; Scheet, P.; Hutc, K. Association of strengthening the reporting of genetic association studies (STREGA): An extension of the STROBE statement the C677T methylenetetrahydrofolate reductase mutation with congenital heart diseases. Eur. J. Epidemiol 2009, 24, 37–55. [Google Scholar]
- Collins, F.S.; Brooks, L.D.; Chakravarti, A. A DNA polymorphism discovery resource for research on human genetic variation. Genome Res 1998, 8, 1229–1231. [Google Scholar]
- Gupta, S.K.; Kotwal, J.; Kotwal, A.; Dhall, A.; Garg, S. Role of homocysteine & MTHFR C677T gene polymorphism as risk factors for coronary artery disease in young Indians. Indian J. Med. Res 2012, 135, 506–512. [Google Scholar]
- Domagala, T.B.; Adamek, L.; Nizankowska, E.; Sanak, M.; Szczeklik, A. Mutations C677T and A1298C of the 5,10-methylenetetrahydrofolate reductase gene and fasting plasma homocysteine levels are not associated with the increased risk of venous thromboembolic disease. Blood Coagul. Fibrinolysis 2002, 13, 423–431. [Google Scholar]
- Frederiksen, J.; Juul, K.; Grande, P.; Jensen, G.B.; Schroeder, T.V.; Tybjaerg-Hansen, A.; Nordestgaard, B.G. Methylenetetrahydrofolate Reductase polymorphism (C677T), hyperhomocysteinemia, and risk of ischemic cardiovascular disease and venous thromboembolism: Prospective and case–control studies from the Copenhagen City Heart Study. Blood 2004, 104, 3046–3051. [Google Scholar]
- Wilson, R.P.; Leclerc, D.; Christensen, B.; Yang, H.; Gravel, R.A.; Rozen, R. A common variant in Methionine Synthase Reductase combined with low cobalamin (Vitamin B12) increases risk for spina bifida. Mol. Genet. Metab 1999, 67, 317–323. [Google Scholar]
- Gaughan, D.J.; Kluijtmans, L.A.; Barbaux, S.; McMaster, D.; Young, I.S.; Yarnell, J.W.; Evans, A.; Whitehead, A.S. The Methionine Synthase Reductase (MTRR) A66G polymorphism is a novel genetic determinant of plasma homocysteine concentrations. Atherosclerosis 2001, 157, 451–456. [Google Scholar]
- Guéant-Rodriguez, R.M.; Juillirrem, Y.; Candito, M.; Adjalla, C.E.; Gibelin, P.; Herbeth, B.; van Obberghen, E.; Gueánt, J.L. Association of MTRRA66G polymorphism (but not of MTHFR C677T and A1298C, MTRA2756G, TCN C776G) with homocysteine and coronary artery disease in the French population. Thromb. Haemost 2005, 94, 510–515. [Google Scholar]
- Laraqui, A.; Allami, A.; Carrié, A.; Coiffard, A.S.; Benkouka, F.; Benjouad, A.; Bendriss, A.; Kadiri, N.; Bennouar, N.; Benomar, A.; et al. Influence of methionine synthase (A2756G) and Methionine Synthase Reductase (A66G) polymorphisms on plasma homocysteine levels and relation to risk of coronary artery disease. Acta Cardiol 2006, 61, 51–61. [Google Scholar]
- Jacques, P.F.; Bostom, A.G.; Selhub, J.; Rich, S.; Ellison, R.C.; Eckfeldt, J.H.; Gravel, R.A.; Rozen, R. Effects of polymorphisms of methionine synthase and Methionine Synthase Reductase on total plasma homocysteine in the NHLBI Family Heart Study. Atherosclerosis 2003, 166, 49–55. [Google Scholar]
- Brilakis, E.S.; Berger, P.B.; Ballman, K.V.; Rozen, R. Methylenetetrahydrofolate Reductase (MTHFR) 677C>T and Methionine Synthase Reductase (MTRR) 66A>G polymorphisms: association with serum homocysteine and angiographic coronary artery disease in the era of flour products fortified with folic acid. Atherosclerosis 2003, 168, 315–322. [Google Scholar]
- Rahim, F.; Ebadi, A.; Saki, G.; Remazani, A. Prevalence of congenital heart disease in Iran: A clinical study. J. Med. Sci 2008, 8, 547–552. [Google Scholar]
- Scazzone, C.; Acuto, S.; Guglielmini, E.; Campisi, G.; Bono, A. Methionine Synthase Reductase (MTRR) A66G polymorphism is not related to plasma homocysteine concentration and the risk for vascular disease. Exp. Mol. Pathol 2009, 86, 131–133. [Google Scholar]
- Laraqui, A.; Allami, A.; Carrié, A.; Raisonnier, A.; Coiffard, A.-S.; Benkouka, F.; Bendriss, A.; Benjouad, A.; Bennouar, N.; El Kadiri, N.; et al. Relation between plasma homocysteine, gene polymorphisms of homocysteine metabolism-related enzymes, and angiographically proven coronary artery disease. Eur. J. Int. Med 2007, 18, 474–483. [Google Scholar]
- Vinukonda, G.; Shaik Mohammad, N.; Md Nurul Jain, J.; Prasad Chintakindi, K.; Rama Devi Akella, R. Genetic and environmental influences on total plasma homocysteine and coronary artery disease (CAD) risk among South Indians. Clin. Chim. Acta 2009, 405, 127–131. [Google Scholar]
- Soltanpour, M.S.; Soheili, Z.; Pourfathollah, A.A.; Samiei, S.; Meshkani, R.; Deyhim, M.R.; Safa, M.; Ataei, Z. The association between common C677T mutation in Methylenetetrahydrofolate reductase gene and the risk of venous thrombosis in an Iranian population. Lab. Med 2008, 39, 97–100. [Google Scholar]
- Ou, T.; Yamakawa, K.; Arinami, T.; Amemiya, H.; Fujiwara, H.; Kawata, K.; Saito, M.; Kikuchi, S.; Noguchi, Y.; Sugishita, Y.; et al. Methylenetetrahydrofolate reductase and apolipoprotein E polymorphisms are independent risk factors for coronary heart disease in Japanese: A case-control study. Atherosclerosis 1998, 137, 23–28. [Google Scholar]
- Lee, C.N.; Su, Y.N.; Cheng, W.F.; Lin, M.T.; Wang, J.K.; Wu, M.H.; Hsieh, F.J. Association of the C677T methylenetetrahydrofolate reductase mutation with congenital heart diseases. Acta Obstet. Gynecol. Scand 2005, 84, 1134–1140. [Google Scholar]
- Schluterman, M.K.; Krisiyak, A.; Kathiriya, I.S.; Abate, N.; Chandalia, M.; Srivastava, D.; Garg, V. Screening and biochemical analysis of GATA4 sequence variations identified in patients with congenital heart disease. Am. J. Med. Genet 2007, 143A, 817–823. [Google Scholar]
- Nemer, G.; Fadlalah, F.; Usta, J.; Nemer, M.; Dbaibo, G.; Obeid, M.; Bitar, F. A novel mutation in the GATA4 gene in patients with Tetralogy of Fallot. Human Mutat 2006, 27, 293–294. [Google Scholar]
- Zhang, W.M.; Li, X.; Ma, Z.Y.; Zhang, J.; Zhou, S.H.; Li, T.; Shi, L.; Li, Z.Z. GATA4 and NKX2.5 gene analysis in Chinese Uygur patients with congenital heart disease. Chin. Med 2009, 122, 416–419. [Google Scholar]
- Zhang, W.M.; Li, X.; Shen, A.; Jiao, W.; Guan, X.; Li, Z. Screening NKX2.5 mutation in a sample of 230 Han Chinese children with congenital heart diseases. Genet. Test Mol. Biomark 2009, 13, 159–162. [Google Scholar]
- Kluijtmans, L.A.; Young, I.; Boreham, C.A.; Murray, L.; McMaster, D.; McNulty, H.; Strain, J.J.; McPartlin, J.; Scott, J.M.; Whitehead, A.S. Genetic and nutritional factors contributing to hyperhomocysteinemia in young adults. Blood 2003, 101, 2483–2488. [Google Scholar]
- Van der Put, N.M.; Steegers-Theunissen, R.P.; Frosst, P.; Trijbels, F.J.; Eskes, T.K.; van den Heuvel, L.P.; Mariman, E.C.; den Heyer, M.; Rozen, R.; Blom, H.J. Mutated Methylenetetrahydrofolate Reductase as a risk factor for spina bifida. Lancet 1995, 346, 1070–1071. [Google Scholar]
- Jacques, P.F.; Bostom, A.G.; Williams, R.R.; Ellison, R.C.; Eckfeldt, J.H.; Rosenberg, I.H.; Selhub, J.; Rozen, R. Relation between folate status, a common mutation in Methylenetetrahydrofolate Reductase, and plasma homocysteine concentrations. Circulation 1996, 93, 7–9. [Google Scholar]
- Botto, L.D.; Yang, Q.H. 5,10-Methylenetetrahydrofolate Reductase gene variations and congenital anomalies: A huge review. Am. J. Epidemiol 2000, 151, 862–877. [Google Scholar]
- Shields, D.C.; Krike, P.; Mills, J.L.; Ramsbottom, D.; Molly, A.M.; Bruke, H.; Weir, D.G.; Scott, J.M.; Whitehead, A.S. The “thermolabile” variant of methylenetetrahydrofolate reductase and neural tube defects: An evaluation of genetic risk and relative importance of genotypes of embryo and the mother. Am. J. Hum. Genet 1999, 64, 1045–1055. [Google Scholar]
- Koch, M.C.; Stegmann, K.; Ziegler, A.; Schroter, B.; Ermert, A. Evaluation of the MTHFR C677T allele and the MTHFR gene locus in a German spina bifida population. Eur. J. Pediatr 1998, 157, 487–492. [Google Scholar]
- Molloy, A.M.; Mills, J.; Kirke, P.N.; Ramsbottom, D.; McPartlin, J.M.; Burke, H.; Conley, M.; Whitehead, A.S.; Weir, D.G.; Scott, J.M. Low blood folates in NTD pregnancies are only partly explained by thermolabile 5,10-methylenetetrahydrofolate reductase: Low folate status alone may be the critical factor. Am. J. Med. Genet 1988, 78, 155–159. [Google Scholar]
- Wenstrom, K.D.; Johanning, G.L.; Johnston, K.E.; DuBard, M. Association of the C677T methylenetetrahydrofolate reductase mutation and elevated homocysteine levels with congenital cardiac malformations. Am. J. Obstet. Gynecol 2001, 184, 806–812. [Google Scholar]
- Junker, R.; Kotthoff, S.; Vielhaber, H.; Halimeh, S.; Kosch, A.; Koch, H.G.; Kassenbohmer, R.; Heineking, B.; Nowak-Gottl, U. Infant methylenetetrahydrofolate reductase 667TT genotype is a risk factor for congenital heart disease. Cardiovasc. Res 2001, 51, 251–254. [Google Scholar]
- Storti, S.; Vittorini, S.; Lascone, M.R.; Sacchelli, M.; Collavoli, A.; Ripoli, A.; Cocchi, G.; Biagini, A.; Clerico, A. Association between 5,10-Methylenetetrahydrofolate Reductase C677T and A1298C polymorphisms and conotruncal heart defects. Clin. Chem. Lab. Med 2003, 41, 276–280. [Google Scholar]
- McBride, K.L.; Fernbach, S.; Menesses, A.; Molinari, L.; Quay, E.; Pignatelli, R.; Towbin, J.A.; Belmont, J.W. A family-based association study of congenital left-sided heart malformations and 5,10-Methylenetetrahydrofolate Reductase. Birth. Defects Res. A 2004, 78, 825–830. [Google Scholar]
- Pereira, A.C.; Xavier, N.J.; Mesquita, S.M.; Mota, G.F.; Lopes, A.A.; Krieger, J.E. Lack of evidence of association between MTHFR C677T polymorphism and congenital heart disease in a TDT study design. Int. J. Cardiol 2005, 105, 15–18. [Google Scholar]
- Shaw, G.M.; Iovannisci, D.; Yang, W.; Finnell, R.H.; Carmichael, S.L.; Cheng, S.; Lammer, E.J. Risks of human conotruncal heart defects associated with 32 single nucleotide polymorphisms of selected cardiovascular disease-related genes. Am. J. Med. Genet 2005, 138, 21–26. [Google Scholar]
- Cardon, L.R.; Bell, J.I. Association study designs for complex diseases. Nat. Rev. Genet 2001, 2, 91–99. [Google Scholar]
- Zhu, W.L.; Li, Y.; Yan, L.; Dao, J.; Li, S. Maternal and offspring MTHFR gene C677T polymorphism as predictors of congenital atrial septal defect and patent ductus arteriosus. Mol. Hum. Reprod 2006, 12, 51–54. [Google Scholar]
- Bennouar, N.; Allami, A.; Azeddoug, H.; Bendris, A.; Laraqui, A.; Jaffali, A.E.; Kadiri, N.E.; Benzidia, R.; Benomar, A.; Fellat, S.; et al. Thermolabile Methylenetetrahydrofolate Reductase C677T polymorphism and homocysteine are risk factors for coronary artery disease in Moroccan population. J. Biomed. Biotechnol 2007, 2007, 80687–80696. [Google Scholar]
- Verkleij-Hagoort, A.C.; Verlinde, M.; Ursem, N.T.; Lindemans, J.; Helbing, W.A.; Ottenkamp, J.; Siebel, F.M.; Gittenberger-de Groot, A.C.; de Jonge, R.; Bartelings, M.M.; et al. Maternal hyperhomocysteinaemia is a risk factor for congenital heart disease. BJOG 2006, 113, 1412–1418. [Google Scholar]
- Van Beynum, I.M.; Kouwenberg, M.; Kapusta, L.; den Heijer, M.; van der Linde, I.J.; Daniels, O.; Blom, H.J. MTRR 66A>G polymorphism in relation to congenital heart defects. Clin. Chem. Lab. Med 2006, 44, 1317–1323. [Google Scholar]
- Fredriksen, A.; Meyer, K.; Ueland, P.M.; Vollset, S.E.; Grotmol, T. Large-scale population-based metabolic phenotyping of thirteen genetic polymorphisms related to one-carbon metabolism. Hum. Mutat 2007, 28, 856–865. [Google Scholar]
- Verkleij-Hagoort, A.; van Driel, L.M.; Lindemans, J.; Isaacs, A.; Steegers, E.A.; Helbing, W.A.; Uitterlinden, A.G.; Steegers-Theunissen, R.P. Genetic and lifestyle factors related to the periconception vitamin B12 status and congenital heart defects: A dutch case-control study. Mol. Genet. Metab 2008, 94, 112–119. [Google Scholar]
- Shaw, G.M.; Iovannisc, D.; Yang, W.; Finnell, R.H.; Carmichael, S.L.; Cheng, S.; Lammer, E.J. 118 SNPs of folate-related genes and risks of spina bifida and conotruncal heart defects. BMC Med. Genet 2009, 10, 49. [Google Scholar]
- Tamura, K.; Dudley, J.; Nei, M.; Kumar, S. MEGA4: Molecular Evolutionary Genetics Analysis (MEGA) software version 4.0. Mol. Biol. Evol 2007, 24, 596–1599. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| Gene Variants | Disease | Population/Reference | No. of Subjects | p-value |
|---|---|---|---|---|
| MTRR A66G | Vascular disease | Italy [17] | 114 | NS |
| MTRR A66G | CAD | Morocco [18] | 151 | S |
| MTHFR C677T | CAD | South Indians [19] | 108 | S |
| MTHFR C677T | Venous Thrombosis | Iran [20] | 200 | NS |
| MTHFR C677T | CHD | Japan [21] | 233 | S |
| MTHFR C677T | CHD | Taiwan [22] | 231 | S |
| GATA4 | CHD | USA [23] | 157 | NS |
| GATA4 | CHD | Canada [24] | 120 | S |
| GATA4, NKX2.5 | CHD | China [25] | 62 | S |
| NKX2.5 | CHD | China [26] | 230 | NS |
| TBX5 | VSD | China [1] | 192 | S |
| Gene | Genotypes and Alleles | Case (%) | Control (%) |
|---|---|---|---|
| C677T Genotypes | CC | 63 (51.2) | 71 (56.8) |
| CT | 60 (48.8) | 54 (43.2) | |
| p value | 0.38 * | ||
| Odds Ratio (95% CI) | 0.82 (0.49–1.31) | ||
| Alleles | C | 186 (75.6) | 196 (78.4) |
| T | 60 (24.4) | 54 (21.6) | |
| p value | 0.47 * | ||
| Odds Ratio (95% CI) | 0.85 (0.56–1.30) | ||
| Gene | Genotypes and Alleles | Case (%) | Control (%) |
|---|---|---|---|
| C524T Genotypes | CC | 53 (43.1) | 66 (52.8) |
| CT | 50 (40.6) | 54 (43.2) | |
| TT | 20 (16.3) | 5 (4.0) | |
| p value | 0.00 * | ||
| CC vs. CT, p value | 0.60 ** | ||
| Odds Ratio (95% CI) | 0.87 (0.51–1.47) | ||
| CC vs. TT, p value | 0.00 * | ||
| Odds Ratio (95% CI) | 0.20 (0.07–0.57) | ||
| CT vs. TT, p value | 0.00 * | ||
| Odds Ratio (95% CI) | 0.23 (0.08–0.66) | ||
| Alleles | C | 156 (63.4) | 186 (74.4) |
| T | 90 (36.6) | 64 (25.6) | |
| p value | 0.00 * | ||
| Odds Ratio (95% CI) | 0.596 (0.40–0.87) | ||
| Gene | Genotypes and Alleles | Case (%) | Control (%) |
| A66G Genotypes | AA | 41 (33.3) | 62 (49.6) |
| AG | 54 (43.9) | 53 (42.4) | |
| GG | 28 (22.8) | 10 (8.0) | |
| p value | 0.00 * | ||
| AA vs. AG, p value | 0.12 * | ||
| Odds Ratio (95% CI) | 0.65 (0.38–1.12) | ||
| AA vs. GG, p value | 0.00 * | ||
| Odds Ratio (95% CI) | 0.24 (0.10–0.54) | ||
| AG vs. GG, p value | 0.00 * | ||
| Odds Ratio (95% CI) | 0.36 (0.16–0.82) | ||
| Alleles | A | 136 (55.3) | 177 (70.8) |
| G | 110 (44.7) | 73 (29.2) | |
| p value | 0.00 * | ||
| Odds Ratio (95% CI) | 0.51 (035–0.73) | ||
| Gene Polymorphism | Forward Primer (FP) Reverse Primer (RP) | Restriction Endonuclease Enzymes | PCR Products (bp) | Restriction Fragment Size (bp) |
|---|---|---|---|---|
| MTHFR C677T | FP-5′-TGAAGGAGAAGGT GTCTGCGGGA-3′ RP-5′AGGACGGTGCGGT GCGGTGAGAGTG-3′ | Hinf1 | 198 | Wild type: 198 Mutant: 175, 23 Heterozygote: 198,175, 23 |
| MTRR C524T | FP-5′-GTCAAGCAGAGGACA AGAG-3′ RP-5′AGAGACTCCTGCAGAT GTAC-3′ | Xho1 | 309 | Wild type: 247, 62 Mutant: 309 Heterozygote: 309, 247, 62 |
| MTRR A66G | FP-5′-CAGGCAAAGGCCAT CGCAGAAGACAT-3′ RP-5′CACTTCCCAACCAAAA TTCTTCAAAG-3′ | Nde1 | 151 | Wild type: 126, 25 Mutant: 151 Heterozygote: 151, 126, 25 |
© 2013 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Pishva, S.R.; Vasudevan, R.; Etemad, A.; Heidari, F.; Komara, M.; Ismail, P.; Othman, F.; Karimi, A.; Sabri, M.R. Analysis of MTHFR and MTRR Gene Polymorphisms in Iranian Ventricular Septal Defect Subjects. Int. J. Mol. Sci. 2013, 14, 2739-2752. https://doi.org/10.3390/ijms14022739
Pishva SR, Vasudevan R, Etemad A, Heidari F, Komara M, Ismail P, Othman F, Karimi A, Sabri MR. Analysis of MTHFR and MTRR Gene Polymorphisms in Iranian Ventricular Septal Defect Subjects. International Journal of Molecular Sciences. 2013; 14(2):2739-2752. https://doi.org/10.3390/ijms14022739
Chicago/Turabian StylePishva, Seyyed Reza, Ramachandran Vasudevan, Ali Etemad, Farzad Heidari, Makanko Komara, Patimah Ismail, Fauziah Othman, Abdollah Karimi, and Mohammad Reza Sabri. 2013. "Analysis of MTHFR and MTRR Gene Polymorphisms in Iranian Ventricular Septal Defect Subjects" International Journal of Molecular Sciences 14, no. 2: 2739-2752. https://doi.org/10.3390/ijms14022739