Current Status in the Therapy of Liver Diseases

Abstract
:1. Introduction
2. Hepatitis
2.1. Hepatitis A
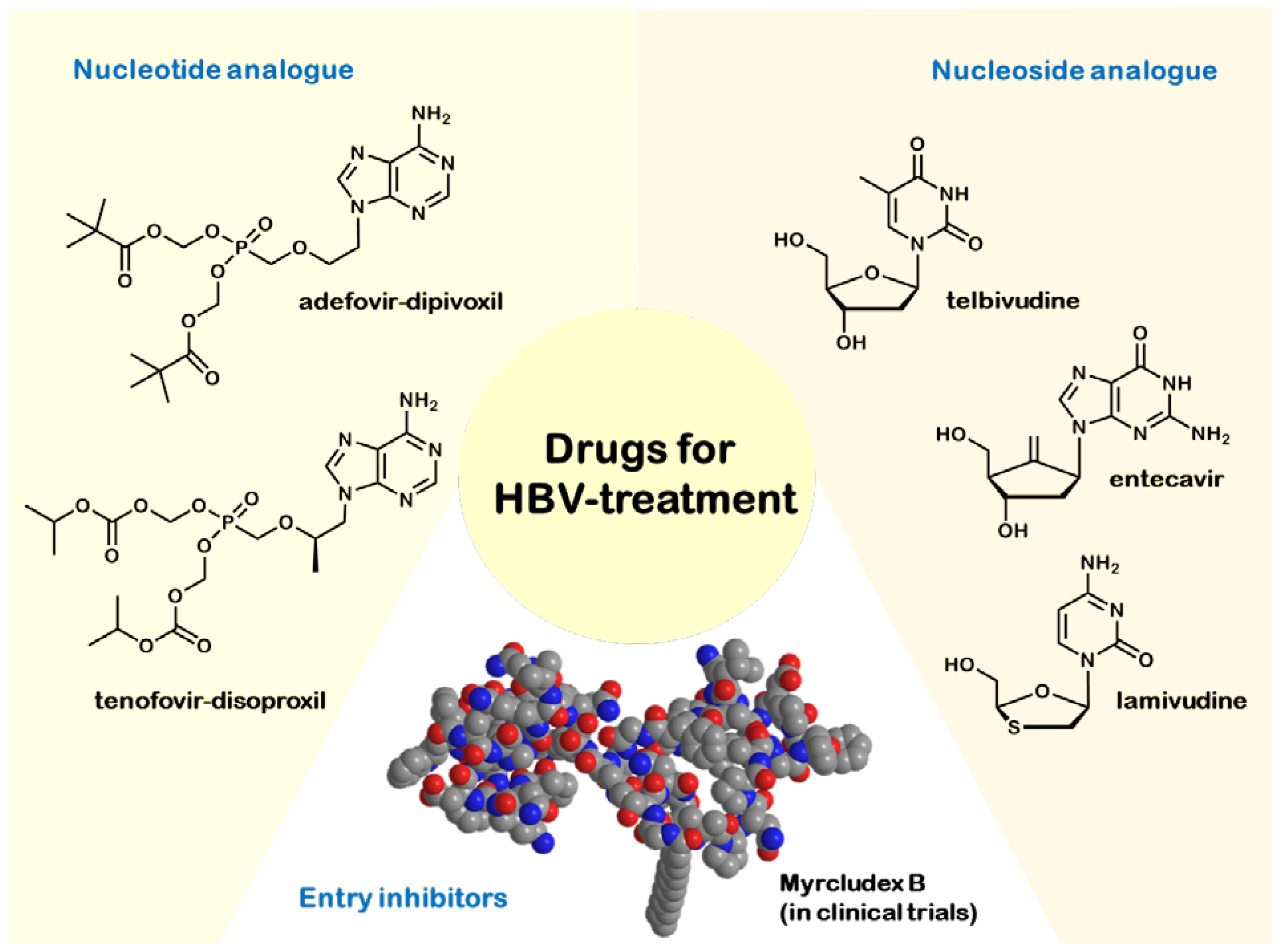
2.2. Hepatitis B
2.3. Hepatitis C
2.4. Hepatitis D
2.5. Hepatitis E
3. Others
3.1. Autoimmune Hepatitis
3.2. Hereditary Hemochromatosis
3.3. Non-Alcoholic Fatty Liver Disease (NAFLD)
3.4. Wilson’s Disease
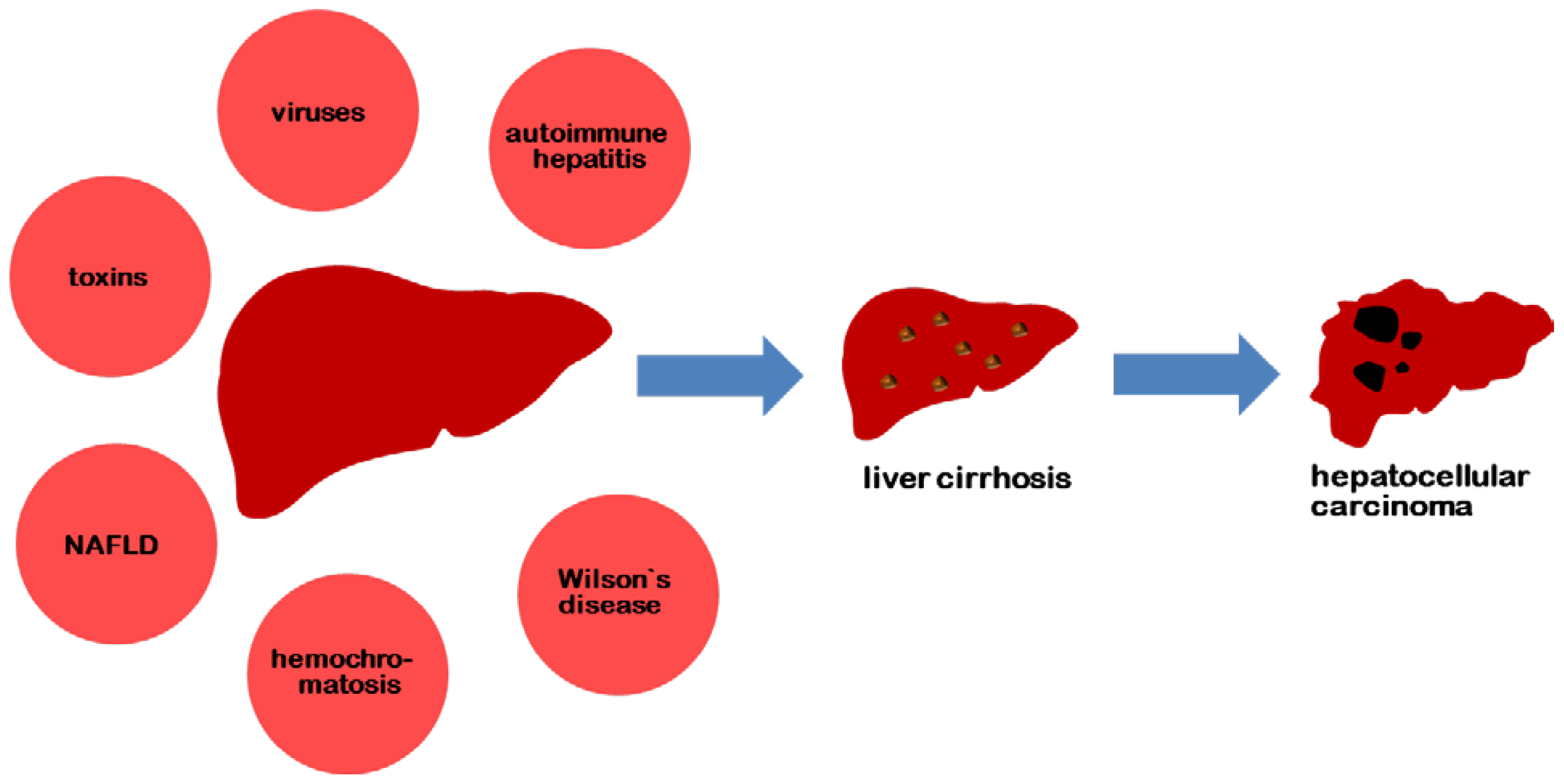
4. Liver Cirrhosis and Hepatocellular Carcinoma (HCC)
4.1. Liver Cirrhosis
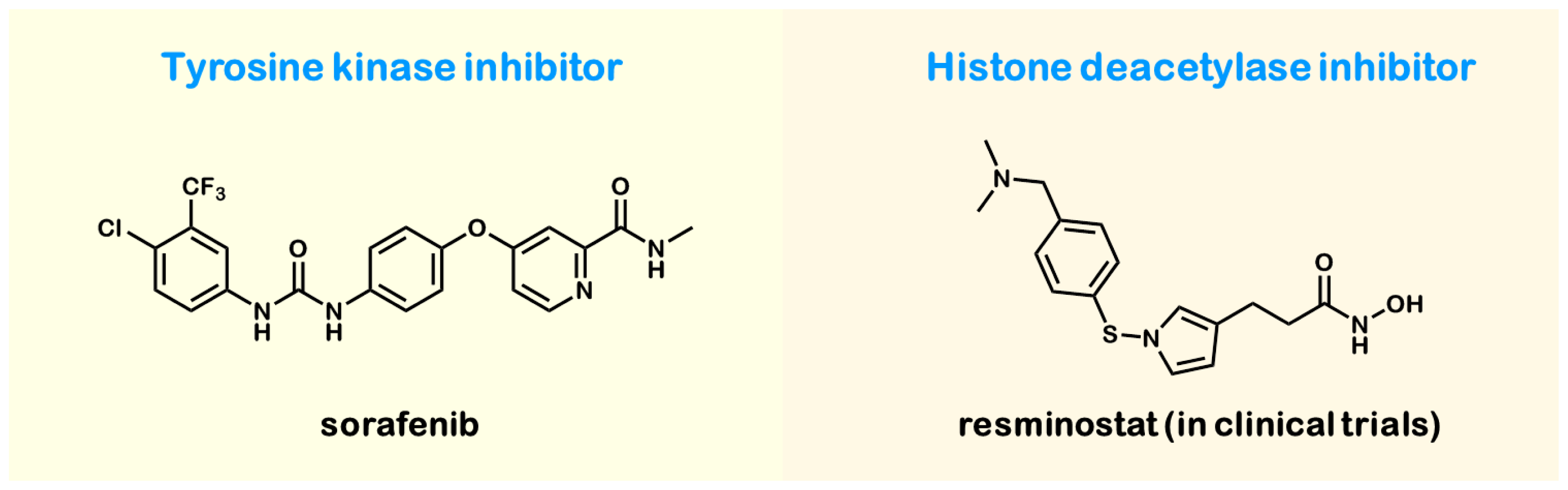
4.2. Hepatocellular Carcinoma (HCC)
5. Conclusions
Conflicts of Interest
- Author ContributionsGert Fricker, Uwe Haberkorn and Walter Mier wrote the vital passages and designed and revised the manuscript. Philipp Uhl composed the main part of the manuscript and composed the figures.
References
- Rehermann, B.; Nascimbeni, M. Immunology of hepatitis B virus and hepatitis C virus infection. Nat. Rev. Immunol 2005, 5, 215–229. [Google Scholar]
- Perz, J.F.; Armstrong, G.L.; Farrington, L.A.; Hutin, Y.J.; Bell, B.P. The contributions of hepatitis B virus and hepatitis C virus infections to cirrhosis and primary liver cancer worldwide. J. Hepatol 2006, 45, 529–538. [Google Scholar]
- Desmet, V.J.; Gerber, M.; Hoofnagle, J.H.; Manns, M.; Scheuer, P.J. Classification of chronic hepatitis: Diagnosis, grading and staging. Hepatology 1994, 19, 1513–1520. [Google Scholar]
- Van Herck, K.; van Damme, P. Prevention of hepatitis A by Havrix™: A review. Expert Rev. Vaccines 2005, 4, 459–471. [Google Scholar]
- Böttcher, B.; Wynne, S.A.; Crowther, R.A. Determination of the fold of the core protein of hepatitis B virus by electron cryomicroscopy. Nature 1997, 386, 88–91. [Google Scholar]
- Mutschler, E. Arzneimittelwirkungen. Lehrbuch der Pharmakologie und Toxikologie, 10th ed; Wissenschaftliche Verlagsgesellschaft mbH: Stuttgart, Germany, 2013. (In German) [Google Scholar]
- Kwon, H.; Lok, A.S. Hepatitis B therapy. Nat. Rev. Gastroenterol. Hepatol 2011, 8, 275–284. [Google Scholar]
- Okanoue, T.; Sakamoto, S.; Itoh, Y.; Minami, M.; Yasui, K.; Sakamoto, M.; Kashima, K. Side effects of high-dose interferon therapy for chronic hepatitis C. J. Hepatol 1996, 25, 283–291. [Google Scholar]
- Lok, A.S.; McMahon, B.J. Chronic hepatitis B: Update. Hepatology 2009, 50, 661–662. [Google Scholar]
- Glebe, D.; Urban, S. Viral and cellular determinants involved in hepadnaviral entry. World J. Gastroenterol 2007, 13, 22. [Google Scholar]
- Schieck, A.; Schulze, A.; Gähler, C.; Müller, T.; Haberkorn, U.; Alexandrov, A.; Mier, W. Hepatitis B virus hepatotropism is mediated by specific receptor recognition in the liver and not restricted to susceptible hosts. Hepatology 2013, 58, 43–53. [Google Scholar]
- Petersen, J.; Dandri, M.; Mier, W.; Lütgehetmann, M.; Volz, T.; von Weizsäcker, F.; Urban, S. Prevention of hepatitis B virus infection in vivo by entry inhibitors derived from the large envelope protein. Nat. Biotechnol 2008, 26, 335–341. [Google Scholar]
- Chen, P.J.; Wu, T.C. One step closer to an experimental infection system for Hepatitis B Virus? The identification of sodium taurocholate cotransporting peptide as a viral receptor. Cell Biosci 2013, 3. [Google Scholar] [CrossRef]
- Lupberger, J.; Zeisel, M.B.; Xiao, F.; Thumann, C.; Fofana, I.; Zona, L.; Baumert, T.F. EGFR and EphA2 are host factors for hepatitis C virus entry and possible targets for antiviral therapy. Nat. Med 2011, 17, 589–595. [Google Scholar]
- Sainz, B., Jr.; Barretto, N.; Martin, D.N.; Hiraga, N.; Imamura, M.; Hussain, S.; Uprichard, S.L. Identification of the Niemann-Pick C1-like 1 cholesterol absorption receptor as a new hepatitis C virus entry factor. Nat. Med 2012, 18, 281–285. [Google Scholar]
- Garcia-Calvo, M.; Lisnock, J.; Bull, H.G.; Hawes, B.E.; Burnett, D.A.; Braun, M.P.; Crona, J.H.; Davis, H.R., Jr; Dean, D.C.; Detmers, P.A.; et al. The target of ezetimibe is Niemann-Pick C1-Like 1 (NPC1L1). Proc. Natl. Acad. Sci. USA 2005, 102, 8132–8137. [Google Scholar]
- McHutchison, J.G.; Lawitz, E.J.; Shiffman, M.L.; Muir, A.J.; Galler, G.W.; McCone, J.; Nyberg, L.M.; Lee, W.M.; Ghalib, R.H.; Schiff, E.R.; et al. Peginterferon alfa-2b or alfa-2a with ribavirin for treatment of hepatitis C infection. N. Eng. J. Med 2009, 361, 580–593. [Google Scholar]
- Kwo, P.Y.; Lawitz, E.J.; McCone, J.; Schiff, E.R.; Vierling, J.M.; Pound, D.; Albrecht, J.K. Efficacy of boceprevir, An NS3 protease inhibitor, In combination with peginterferon alfa-2b and ribavirin in treatment-naive patients with genotype 1 hepatitis C infection (SPRINT-1): An open-label, randomised, multicentre phase 2 trial. Lancet 2010, 376, 705–716. [Google Scholar]
- Sarrazin, C.; Berg, T.; Cornberg, M.; Dollinger, M.; Ferenci, P.; Hinrichsen, H.; Zeuzem, S. Expert opinion on boceprevir-and telaprevir-based triple therapies of chronic hepatitis C. Z. Gastroenterol 2012, 50, 57–72. [Google Scholar]
- Kowdley, K.V.; Lawitz, E.; Crespo, I.; Hassanein, T.; Davis, M.N.; DeMicco, M.; Bernstein, D.E.; Afdhal, N.; Vierling, J.M.; Gordon, S.C.; et al. JKSofosbuvir with pegylated interferon alfa-2a and ribavirin for treatment-naive patients with hepatitis C genotype-1 infection (ATOMIC): An open-label, randomised, multicentre phase 2 trial. Lancet 2013, 381, 2100–2107. [Google Scholar]
- Fried, M.W.; Buti, M.; Dore, G.J.; Flisiak, R.; Ferenci, P.; Jacobson, I.; Marcellin, P.; Manns, M.; Nikitin, I.; Poordad, F.; et al. -daily simeprevir (TMC435) with pegylated interferon and ribavirin in treatment-naïve genotype 1 hepatitis C: The randomized PILLAR study. Hepatology 2013, 58, 1918–1929. [Google Scholar]
- Jensen, D.; Asselah, T.; Dieterich, D.; Foster, G.; Sulkowski, M.; Zeuzem, S. A pooled analysis of two randomized, double-blind, placebo-controlled Phase III trials (STARTVersol and 2) of faldaprevir plus pegylated interferon alfa-2a and ribavirin in treatment-naïve patients with chronic hepatitis C genotype-1 infection. Proceeding of the 64th Annual Meeting of the American Association for the Study of Liver Diseases, Washington, DC, USA, 1–5 November 2013.
- Zeuzem, S.; Soriano, V.; Asselah, T.; Bronowicki, J.P.; Lohse, A.W.; Müllhaupt, B.; Schuchmann, M.; Bourlière, M.; Buti, M.; Roberts, S.K.; et al. Faldaprevir and deleobuvir for HCV genotype 1 infection. N. Eng. J. Med 2013, 369, 630–639. [Google Scholar]
- Suzuki, Y.; Ikeda, K.; Suzuki, F.; Toyota, J.; Karino, Y.; Chayama, K.; Kumada, H. Dual oral therapy with daclatasvir and asunaprevir for patients with HCV genotype 1b infection and limited treatment options. J. Hepatol 2012, 58, 655–662. [Google Scholar]
- Proffitt, A. First HEV vaccine approved. Nat. Biotech 2012, 30, 300. [Google Scholar]
- Shrestha, M.P.; Scott, R.M.; Joshi, D.M.; Mammen, M.P., Jr.; Thapa, G.B.; Thapa, N.; Myint, K.S.; Fourneau, M.; Kuschner, R.A.; Shrestha, S.K.; et al. Safety and efficacy of a recombinant hepatitis E vaccine. N. Eng. J. Med 2007, 356, 895–903. [Google Scholar]
- Czaja, A.J.; Freese, D.K. Diagnosis and treatment of autoimmune hepatitis. Hepatology 2002, 36, 479–497. [Google Scholar]
- Manns, M.P.; Woynarowski, M.; Kreisel, W.; Lurie, Y.; Rust, C.; Zuckerman, E.; Strassburg, C.P. Budesonide induces remission more effectively than prednisone in a controlled trial of patients with autoimmune hepatitis. Gastroenterology 2010, 139, 1198–1206. [Google Scholar]
- Bacon, B.R.; Powell, L.W.; Adams, P.C.; Kresina, T.F.; Hoofnagle, J.H. Molecular medicine and hemochromatosis: At the crossroads. Gastroenterology 1999, 116, 193–207. [Google Scholar]
- Hutchinson, C.; Geissler, C.A.; Powell, J.J.; Bomford, A. Proton pump inhibitors suppress absorption of dietary non-haem iron in hereditary haemochromatosis. Gut 2007, 56, 1291–1295. [Google Scholar]
- Belfort, R.; Harrison, S.A.; Brown, K.; Darland, C.; Finch, J.; Hardies, J.; Balas, B.; Gastaldelli, A.; Tio, F.; Pulcini, J.; et al. A placebo-controlled trial of pioglitazone in subjects with nonalcoholic steatohepatitis. N. Engl. J. Med 2006, 355, 2297–2307. [Google Scholar]
- Adams, L.A.; Waters, O.R.; Knuiman, M.W.; Elliott, R.R.; Olynyk, J.K. NAFLD as a risk factor for the development of diabetes and the metabolic syndrome: An eleven-year follow-up study. Am. J. Gastroenterol 2009, 104, 861–867. [Google Scholar]
- Sanyal, A.J.; Chalasani, N.; Kowdley, K.V.; McCullough, A.; Diehl, A.M.; Bass, N.M.; Neuschwander-Tetri, B.A.; Lavine, J.E.; Tonascia, J.; Unalp, A.; et al. Pioglitazone, vitamin E, or placebo for nonalcoholic steatohepatitis. N. Eng. J. Med 2010, 362, 1675–1685. [Google Scholar]
- Loudianos, G.; Gitlin, J.D. Wilson’s disease. Semin. Liver Dis 2000, 20, 353–364. [Google Scholar]
- Walshe, J.M. Treatment of Wilson’s disease with trientine (triethylene tetramine) dihydrochloride. Lancet 1982, 319, 643–647. [Google Scholar]
- Roberts, E.A.; Schilsky, M.L. A practice guideline on Wilson disease. Hepatology 2003, 37, 1475–1492. [Google Scholar]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; de Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcinoma. N. Eng. J. Med 2008, 359, 378–390. [Google Scholar]
- Bitzer, M.; Horger, M.; Ganten, T.; Lauer, U.M.; Woerns, M.A.; Siveke, J.; Dollinger, M.M.; Gerken, G.; Scheulen, M.E.; Wege, H.; et al. Efficacy, Safety, Tolerability and PK of the HDAC inhibitor resminostat in sorafenib-refractory hepatocellular carcinoma (HCC): Phase II SHELTER study. J. Clin. Oncol 2012, 30, 4115. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Hepatitis A virus | Hepatitis B virus | Hepatitis C virus | Hepatitis D virus | Hepatitis E virus |
|---|---|---|---|---|---|
| family | Picornaviridae | Hepadnaviridae | Flaviviridae | unknown | Hepeviridae |
| genome | single-stranded RNA | double-stranded DNA | single-stranded RNA | single-stranded RNA | single-stranded RNA |
| transmission route | fecal-oral | parenteral, sexual, perinatal | parenteral, sexual, perinatal | parenteral, sexual, perinatal | fecal-oral |
| incubation period | 2–7 weeks | 1–6 months | 2–25 weeks | 1–6 months | 2–9 weeks |
| immunoprophylaxis | active, inactive | active, inactive | not available | active, inactive | not available |
| Characteristics | Lamivudine | Tenofovir | Adefovir | Entecavir | Telbivudine |
|---|---|---|---|---|---|
| year of approval | 1999 | 2001 | 2002 | 2006 | 2007 |
| resistance after five years | ca. 70% | not found yet | ca. 30% | ca. 1% | ca. 22% |
| medical assessment | well tolerated, main concern: resistance | less nephrotoxic than adefovir | nephrotoxic, less prone to resistance than lamivudine | well tolerated, more potent than lamivudine and adefovir | well tolerated, high potency, resistances appear after one year |
| Treatment-naive patients eligible to receive interferon | Treatment-naive patients ineligible to receive interferon |
|---|---|
| sofosbuvir (400 mg) daily | sofosbuvir (400 mg) daily |
| weight-based ribavirin daily | simeprevir (150 mg) daily |
| peginterferon on a weekly basis | with/without weight-based ribavirin |
© 2014 by the authors; licensee MDPI, Basel, Switzerland This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Uhl, P.; Fricker, G.; Haberkorn, U.; Mier, W. Current Status in the Therapy of Liver Diseases. Int. J. Mol. Sci. 2014, 15, 7500-7512. https://doi.org/10.3390/ijms15057500
Uhl P, Fricker G, Haberkorn U, Mier W. Current Status in the Therapy of Liver Diseases. International Journal of Molecular Sciences. 2014; 15(5):7500-7512. https://doi.org/10.3390/ijms15057500
Chicago/Turabian StyleUhl, Philipp, Gert Fricker, Uwe Haberkorn, and Walter Mier. 2014. "Current Status in the Therapy of Liver Diseases" International Journal of Molecular Sciences 15, no. 5: 7500-7512. https://doi.org/10.3390/ijms15057500