Different Role of Tumor Necrosis Factor-α Polymorphism in Non-Hodgkin Lymphomas among Caucasian and Asian Populations: A Meta-Analysis

Abstract
:1. Introduction
2. Results and Discussion
2.1. Eligible Studies
2.2. Quantitative Synthesis
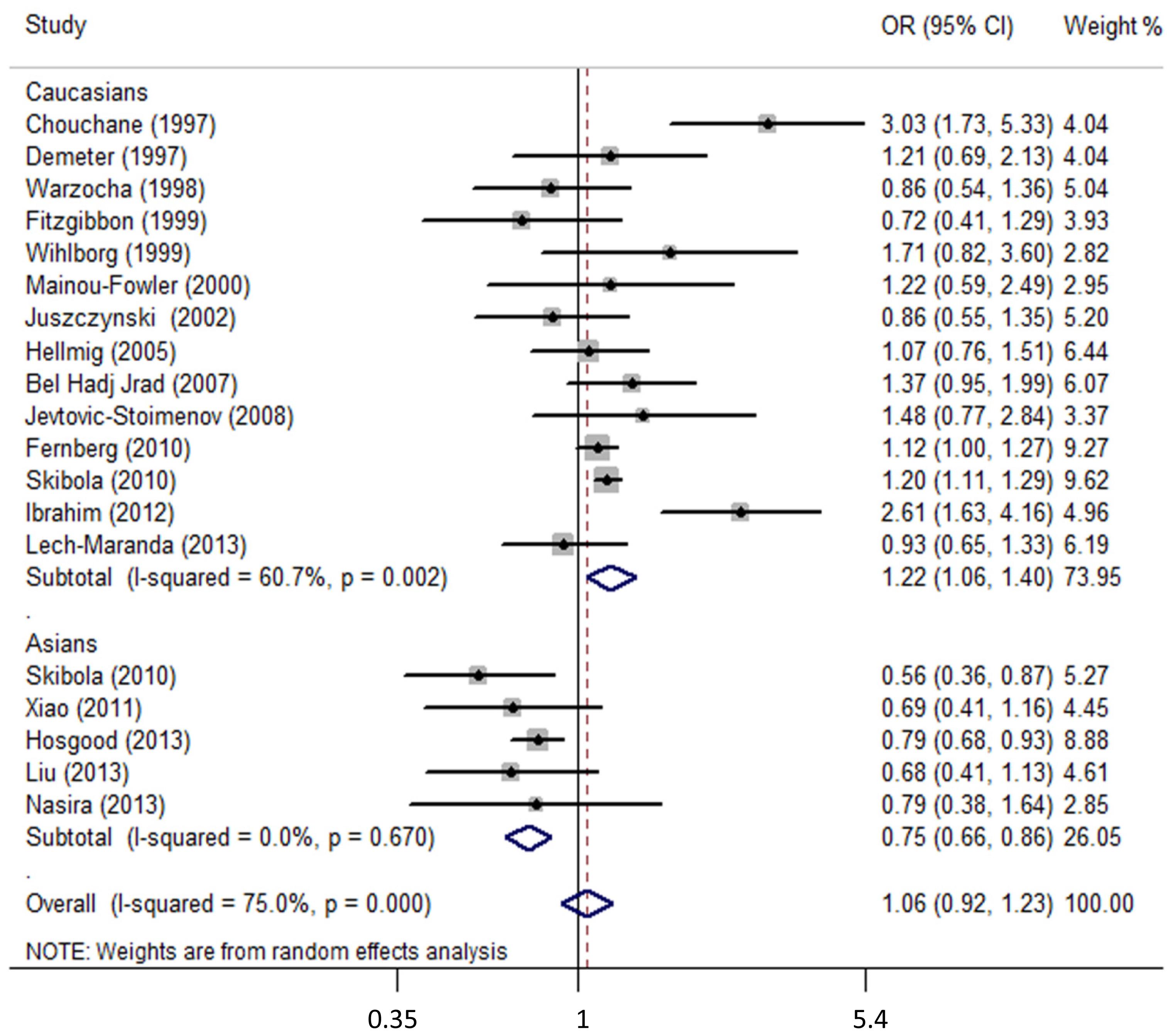
2.2.1. TNF-α-308G>A and NHL
2.2.2. TNF-α-308G>A and B- or T-CL
2.2.3. TNF-α-308G>A and NHL Subtypes
2.3. Discussion
3. Experimental Section
3.1. Publication Search
3.2. Inclusion Criteria
3.3. Data Extraction
3.4. Statistical Analysis
4. Conclusions
Acknowledgments
Conflicts of Interest
Abbreviations
| TNF | tumor necrosis factor |
| NHL | non-Hodgkin lymphomas |
| BCL | B-cell lymphomas |
| TCL | T-cell lymphomas |
| DLBCL | diffuse large B-cell lymphomas |
| FL | follicular lymphomas |
| CLL/SLL | chronic lymphocytic leukemias/small lymphocytic lymphomas |
| MCL | mantel cell lymphomas |
| MALT | mucosal-associated lymphomas |
| PTCL | peripheral T-cell lymphomas |
| NK/TCL | natural killer/T-cell lymphomas |
| OR | odds ratio |
| 95% CI | 95% confidence interval |
- Author ContributionsConceived and designed the experiments: K.Z. Performed the experiments: K.Z. and J.D. Analyzed the data: K.Z., J.D. and Y.Z. Wrote the paper: K.Z. J.D. and Y.Z.
References
- Shankland, K.R.; Armitage, J.O.; Hancock, B.W. Non-Hodgkin lymphoma. Lancet 2012, 380, 848–857. [Google Scholar]
- Evans, L.S.; Hancock, B.W. Non-Hodgkin lymphoma. Lancet 2003, 362, 139–146. [Google Scholar]
- Alexander, D.D.; Mink, P.J.; Adami, H.O.; Chang, E.T.; Cole, P.; Mandel, J.S.; Trichopoulos, D. The non-Hodgkin lymphomas: A review of the epidemiologic literature. Int. J. Cancer 2007, 120 Suppl 12, 1–39. [Google Scholar]
- Kumar, V.; Matsuo, K.; Takahashi, A.; Hosono, N.; Tsunoda, T.; Kamatani, N.; Kong, S.Y.; Nakagawa, H.; Cui, R.; Tanikawa, C.; et al. Common variants on 14q32 and 13q12 are associated with DLBCL susceptibility. J. Hum. Genet 2011, 56, 436–439. [Google Scholar]
- Skibola, C.F.; Conde, L.; Foo, J.N.; Riby, J.; Humphreys, K.; Sille, F.C.; Darabi, H.; Sanchez, S.; Hjalgrim, H.; Liu, J.; et al. A meta-analysis of genome-wide association studies of follicular lymphoma. BMC Genomics 2012, 13, 516. [Google Scholar]
- Zhai, K.; Tian, X.; Wu, C.; Lu, N.; Chang, J.; Huang, L.; Zhang, T.; Zhou, Y.; Qiao, Y.; Yu, D.; et al. Cytokine BAFF gene variation is associated with survival of patients with T-cell lymphomas. Clin. Cancer Res 2012, 18, 2250–2256. [Google Scholar]
- Berndt, S.I.; Skibola, C.F.; Joseph, V.; Camp, N.J.; Nieters, A.; Wang, Z.; Cozen, W.; Monnereau, A.; Wang, S.S.; Kelly, R.S.; et al. Genome-wide association study identifies multiple risk loci for chronic lymphocytic leukemia. Nat. Genet 2013, 45, 868–876. [Google Scholar]
- Tan, D.E.; Foo, J.N.; Bei, J.X.; Chang, J.; Peng, R.; Zheng, X.; Wei, L.; Huang, Y.; Lim, W.Y.; Li, J.; et al. Genome-wide association study of B cell non-Hodgkin lymphoma identifies 3q27 as a susceptibility locus in the Chinese population. Nat. Genet 2013, 45, 804–807. [Google Scholar]
- Vijai, J.; Kirchhoff, T.; Schrader, K.A.; Brown, J.; Dutra-Clarke, A.V.; Manschreck, C.; Hansen, N.; Rau-Murthy, R.; Sarrel, K.; Przybylo, J.; et al. Susceptibility loci associated with specific and shared subtypes of lymphoid malignancies. PLoS Genet 2013, 9, e1003220. [Google Scholar]
- Zhu, K.; Levine, R.S.; Gu, Y.; Brann, E.A.; Hall, I.; Caplan, L.S.; Baum, M.K. Non-Hodgkin’s lymphoma and family history of malignant tumors in a case-control study (United States). Cancer Causes Control 1998, 9, 77–82. [Google Scholar]
- Altieri, A.; Bermejo, J.L.; Hemminki, K. Familial risk for non-Hodgkin lymphoma and other lymphoproliferative malignancies by histopathologic subtype: The Swedish Family-Cancer Database. Blood 2005, 106, 668–672. [Google Scholar]
- Wang, S.S.; Slager, S.L.; Brennan, P.; Holly, E.A.; de Sanjose, S.; Bernstein, L.; Boffetta, P.; Cerhan, J.R.; Maynadie, M.; Spinelli, J.J.; et al. Family history of hematopoietic malignancies and risk of non-Hodgkin lymphoma (NHL): A pooled analysis of 10,211 cases and 11,905 controls from the International Lymphoma Epidemiology Consortium (InterLymph). Blood 2007, 109, 3479–3488. [Google Scholar]
- Sethi, G.; Sung, B.; Aggarwal, B.B. TNF: A master switch for inflammation to cancer. Front. Biosci 2008, 13, 5094–5107. [Google Scholar]
- Macia, J.; Gomez, X.; Esquerda, A.; Perez, B.; Callao, V.; Marzo, C. Value of the determination of TNF-alpha in the plasma of patients with non-Hodgkins lymphoma. Leuk. Lymphoma 1996, 20, 481–486. [Google Scholar]
- Adami, F.; Guarini, A.; Pini, M.; Siviero, F.; Sancetta, R.; Massaia, M.; Trentin, L.; Foa, R.; Semenzato, G. Serum levels of tumour necrosis factor-alpha in patients with B-cell chronic lymphocytic leukaemia. Eur. J. Cancer 1994, 30A, 1259–1263. [Google Scholar]
- Warzocha, K.; Ribeiro, P.; Bienvenu, J.; Roy, P.; Charlot, C.; Rigal, D.; Coiffier, B.; Salles, G. Genetic polymorphisms in the tumor necrosis factor locus influence non-Hodgkin’s lymphoma outcome. Blood 1998, 91, 3574–3581. [Google Scholar]
- Halida, Y.; Guo, X.H.; Aliya, R. Expression of plasma TNF-alpha and TNF-beta in different subtypes lymphoma and its significance. Zhonghua Xue Ye Xue Za Zhi 2011, 32, 695–697. (In Chinese) [Google Scholar]
- Wilson, A.G.; di Giovine, F.S.; Duff, G.W. Genetics of tumour necrosis factor-alpha in autoimmune, infectious, and neoplastic diseases. J. Inflamm 1995, 45, 1–12. [Google Scholar]
- Neben, K.; Mytilineos, J.; Moehler, T.M.; Preiss, A.; Kraemer, A.; Ho, A.D.; Opelz, G.; Goldschmidt, H. Polymorphisms of the tumor necrosis factor-alpha gene promoter predict for outcome after thalidomide therapy in relapsed and refractory multiple myeloma. Blood 2002, 100, 2263–2265. [Google Scholar]
- Ho, S.Y.; Wang, Y.J.; Chen, H.L.; Chen, C.H.; Chang, C.J.; Wang, P.J.; Chen, H.H.; Guo, H.R. Increased risk of developing hepatocellular carcinoma associated with carriage of the TNF2 allele of the -308 tumor necrosis factor-alpha promoter gene. Cancer Causes Control 2004, 15, 657–663. [Google Scholar]
- Kroeger, K.M.; Carville, K.S.; Abraham, L.J. The -308 tumor necrosis factor-alpha promoter polymorphism effects transcription. Mol. Immunol 1997, 34, 391–399. [Google Scholar]
- Wilson, A.G.; Symons, J.A.; McDowell, T.L.; McDevitt, H.O.; Duff, G.W. Effects of a polymorphism in the human tumor necrosis factor alpha promoter on transcriptional activation. Proc. Natl. Acad. Sci. USA 1997, 94, 3195–3199. [Google Scholar]
- Pikarsky, E.; Porat, R.M.; Stein, I.; Abramovitch, R.; Amit, S.; Kasem, S.; Gutkovich-Pyest, E.; Urieli-Shoval, S.; Galun, E.; Ben-Neriah, Y. NF-κB functions as a tumour promoter in inflammation-associated cancer. Nature 2004, 431, 461–466. [Google Scholar]
- Batten, M.; Fletcher, C.; Ng, L.G.; Groom, J.; Wheway, J.; Laabi, Y.; Xin, X.; Schneider, P.; Tschopp, J.; Mackay, C.R.; et al. TNF deficiency fails to protect BAFF transgenic mice against autoimmunity and reveals a predisposition to B cell lymphoma. J. Immunol 2004, 172, 812–822. [Google Scholar]
- Skibola, C.F.; Bracci, P.M.; Nieters, A.; Brooks-Wilson, A.; de Sanjose, S.; Hughes, A.M.; Cerhan, J.R.; Skibola, D.R.; Purdue, M.; Kane, E.; et al. Tumor necrosis factor (TNF) and lymphotoxin-alpha (LTA) polymorphisms and risk of non-Hodgkin lymphoma in the InterLymph Consortium. Am. J. Epidemiol 2010, 171, 267–276. [Google Scholar]
- Rothman, N.; Skibola, C.F.; Wang, S.S.; Morgan, G.; Lan, Q.; Smith, M.T.; Spinelli, J.J.; Willett, E.; de Sanjose, S.; Cocco, P.; et al. Genetic variation in TNF and IL10 and risk of non-Hodgkin lymphoma: A report from the InterLymph Consortium. Lancet Oncol 2006, 7, 27–38. [Google Scholar]
- Chouchane, L.; Ahmed, S.B.; Baccouche, S.; Remadi, S. Polymorphism in the tumor necrosis factor-alpha promotor region and in the heat shock protein 70 genes associated with malignant tumors. Cancer 1997, 80, 1489–1496. [Google Scholar]
- Demeter, J.; Porzsolt, F.; Ramisch, S.; Schmidt, D.; Schmid, M.; Messer, G. Polymorphism of the tumour necrosis factor-α and lymphotoxin-α genes in chronic lymphocytic leukaemia. Br. J. Haematol 1997, 97, 107–112. [Google Scholar]
- Fitzgibbon, J.; Grenzelias, D.; Matthews, J.; Lister, T.A.; Gupta, R.K. Tumour necrosis factor polymorphisms and susceptibility to follicular lymphoma. Br. J. Haematol 1999, 107, 388–391. [Google Scholar]
- Wihlborg, C.; Sjoberg, J.; Intaglietta, M.; Axdorph, U.; Pisa, E.K.; Pisa, P. Tumour necrosis factor-alpha cytokine promoter gene polymorphism in Hodgkin’s disease and chronic lymphocytic leukaemia. Br. J. Haematol 1999, 104, 346–349. [Google Scholar]
- Mainou-Fowler, T.; Dickinson, A.M.; Taylor, P.R.; Mounter, P.; Jack, F.; Proctor, S.J.; Nordon, J.; Middleton, P.G. Tumour necrosis factor gene polymorphisms in lymphoproliferative disease. Leuk. Lymphoma 2000, 38, 547–552. [Google Scholar]
- Juszczynski, P.; Kalinka, E.; Bienvenu, J.; Woszczek, G.; Borowiec, M.; Robak, T.; Kowalski, M.; Lech-Maranda, E.; Baseggio, L.; Coiffier, B.; et al. Human leukocyte antigens class II and tumor necrosis factor genetic polymorphisms are independent predictors of non-Hodgkin lymphoma outcome. Blood 2002, 100, 3037–3040. [Google Scholar]
- Hellmig, S.; Fischbach, W.; Goebeler-Kolve, M.E.; Folsch, U.R.; Hampe, J.; Schreiber, S. A functional promotor polymorphism of TNF-α is associated with primary gastric B-Cell lymphoma. Am. J. Gastroenterol 2005, 100, 2644–2649. [Google Scholar]
- Bel Hadj Jrad, B.; Chatti, A.; Laatiri, A.; Ahmed, S.B.; Romdhane, A.; Ajimi, S.; Chouchane, L. Tumor necrosis factor promoter gene polymorphism associated with increased susceptibility to non-Hodgkin’s lymphomas. Eur. J. Haematol 2007, 78, 117–122. [Google Scholar]
- Jevtovic-Stoimenov, T.; Kocic, G.; Pavlovic, D.; Macukanovic-Golubovic, L.; Marjanovic, G.; Djordjevic, V.; Tosic, N.; Pavlovic, S. Polymorphisms of tumor-necrosis factor-α-308 and lymphotoxin-α + 250: Possible modulation of susceptibility to apoptosis in chronic lymphocytic leukemia and non-Hodgkin lymphoma mononuclear cells. Leuk. Lymphoma 2008, 49, 2163–2169. [Google Scholar]
- Fernberg, P.; Chang, E.T.; Duvefelt, K.; Hjalgrim, H.; Eloranta, S.; Sorensen, K.M.; Porwit, A.; Humphreys, K.; Melbye, M.; Ekstrom Smedby, K. Genetic variation in chromosomal translocation breakpoint and immune function genes and risk of non-Hodgkin lymphoma. Cancer Causes Control 2010, 21, 759–769. [Google Scholar]
- Ibrahim, A.; Abdel Rahman, H.; Khorshied, M.; Sami, R.; Nasr, N.; Khorshid, O. Tumor necrosis factor α-308 and Lymphotoxin α + 252 genetic polymorphisms and the susceptibility to non-Hodgkin lymphoma in Egypt. Leuk. Res 2012, 36, 694–698. [Google Scholar]
- Lech-Maranda, E.; Mlynarski, W.; Grzybowska-Izydorczyk, O.; Borowiec, M.; Pastorczak, A.; Cebula-Obrzut, B.; Klimkiewicz-Wojciechowska, G.; Wcislo, M.; Majewski, M.; Kotkowska, A.; et al. Polymorphisms of TNF and IL-10 genes and clinical outcome of patients with chronic lymphocytic leukemia. Genes Chromosom. Cancer 2013, 52, 287–296. [Google Scholar]
- Xiao, H.; Zhang, K. Genetic polymorphisms of tumor necrosis factor-α and lymphotoxin-α in Chinese patients with non-Hodgkin lymphoma. Ann. Hematol 2011, 90, 725–727. [Google Scholar]
- Hosgood, H.D., 3rd; Au, W.Y.; Kim, H.N.; Liu, J.; Hu, W.; Tse, J.; Song, B.; Wong, K.F.; Lee, J.J.; Chanock, S.J.; et al. IL10 and TNF variants and risk of non-Hodgkin lymphoma among three Asian populations. Int. J. Hematol 2013, 97, 793–799. [Google Scholar]
- Liu, J.; Song, B.; Wang, T.; Liu, Y.; Hao, J.; Yu, J. Genetic variations in CTLA-4, TNF-α, and LTA and susceptibility to T-cell lymphoma in a Chinese population. Cancer Epidemiol 2013, 37, 930–934. [Google Scholar]
- Nasiri, H.; Farajnia, S.; Rezamand, A.; Movassaghpour, A.A.; Esmaeili, H.A.; Monfaredan, A.; Mobarra, N.; Rahimifar, N.; Sahebi, L.; Farshdousti Hagh, M. Genetic variations of tumor necrosis factor-α-308 and lymphtoxin-α + 252 in non-hodgkin lymphoma and acute lymphoblastic leukemia patients. Iran. J. Basic Med. Sci 2013, 16, 990–995. [Google Scholar]
- Chu, W.M. Tumor necrosis factor. Cancer Lett 2013, 328, 222–225. [Google Scholar]
- Jost, P.J.; Ruland, J. Aberrant NF-κB signaling in lymphoma: Mechanisms, consequences, and therapeutic implications. Blood 2007, 109, 2700–2707. [Google Scholar]
- Shih, V.F.; Tsui, R.; Caldwell, A.; Hoffmann, A. A single NF κB system for both canonical and non-canonical signaling. Cell Res 2011, 21, 86–102. [Google Scholar]
- Younes, A.; Aggarwall, B.B. Clinical implications of the tumor necrosis factor family in benign and malignant hematologic disorders. Cancer 2003, 98, 458–467. [Google Scholar]
- Zhang, Q.; Wang, H.Y.; Bhutani, G.; Liu, X.; Paessler, M.; Tobias, J.W.; Baldwin, D.; Swaminathan, K.; Milone, M.C.; Wasik, M.A. Lack of TNFalpha expression protects anaplastic lymphoma kinase-positive T-cell lymphoma (ALK + TCL) cells from apoptosis. Proc. Natl. Acad. Sci. USA 2009, 106, 15843–15848. [Google Scholar]
- Brown, T.; Rushton, L. Occupational cancer in Britain. Haematopoietic malignancies: Leukaemia, multiple myeloma, non-Hodgkins lymphoma. Br. J. Cancer 2012, 107 Suppl 1, S41–S48. [Google Scholar]
- Zhao, X.F.; Reitz, M.; Chen, Q.C.; Stass, S. Pathogenesis of early leukemia and lymphoma. Cancer Biomark 2010, 9, 341–374. [Google Scholar]
- Carroll, M.C.; Katzman, P.; Alicot, E.M.; Koller, B.H.; Geraghty, D.E.; Orr, H.T.; Strominger, J.L.; Spies, T. Linkage map of the human major histocompatibility complex including the tumor necrosis factor genes. Proc. Natl. Acad. Sci. USA 1987, 84, 8535–8539. [Google Scholar]
- Harris, N.L.; Jaffe, E.S.; Diebold, J.; Flandrin, G.; Muller-Hermelink, H.K.; Vardiman, J. Lymphoma classification—from controversy to consensus: The R.E.A.L. and WHO Classification of lymphoid neoplasms. Ann. Oncol 2000, 11 Suppl 1, 3–10. [Google Scholar]
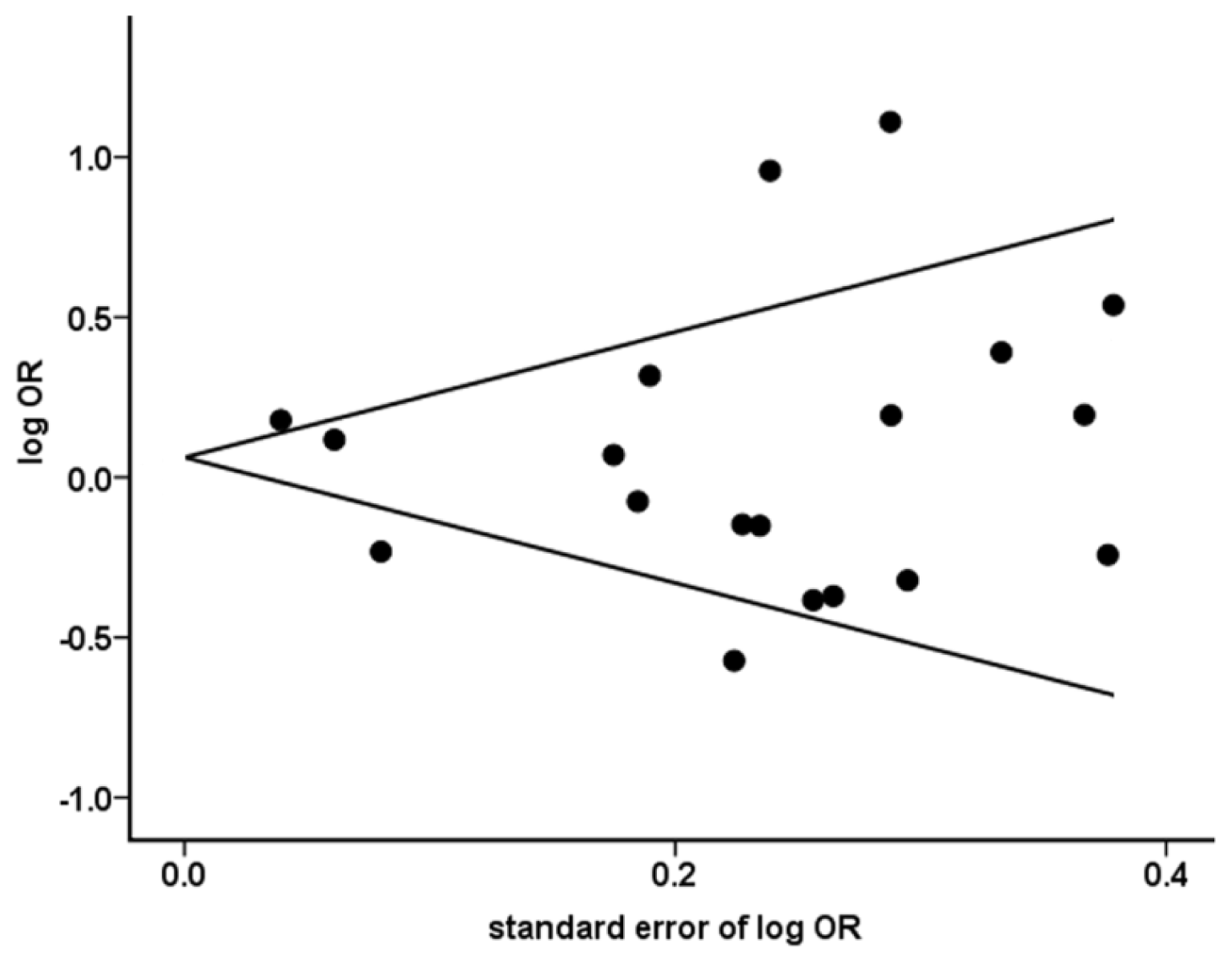
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar]
- Lau, J.; Antman, E.M.; Jimenez-Silva, J.; Kupelnick, B.; Mosteller, F.; Chalmers, T.C. Cumulative meta-analysis of therapeutic trials for myocardial infarction. N. Engl. J. Med 1992, 327, 248–254. [Google Scholar]



{kind=link}
{kind=link}
| Study | Ethnicity | Genotyping Method | Samples | Characteristics | |
|---|---|---|---|---|---|
| NHLs (n) | Controls (n) | ||||
| Chouchane, 1997 | Caucasians | ASPCR | 44 | 106 | All subtypes |
| Demeter, 1997 | Caucasians | PCR-RFLP | 63 | 117 | HCL only |
| Warzocha, 1998 | Caucasians | ASPCR | 273 | 96 | All subtypes |
| Fitzgibbon, 1999 | Caucasians | PCR-RFLP | 121 | 88 | FL only |
| Wihlborg, 1999 | Caucasians | PCR-SPM | 49 | 51 | CLL only |
| Mainou-Fowler, 2000 | Caucasians | PCR-RFLP | 76 | 40 | CLL |
| Juszczynski, 2002 | Caucasians | Sequencing | 204 | 120 | All subtypes |
| Hellmig, 2005 | Caucasians | TaqMan | 138 | 533 | MALT only |
| Bel Hadj Jrad, 2007 | Caucasians | PCR-RFLP | 194 | 160 | All subtypes |
| Jevtovic-Stoimenov, 2008 | Caucasians | PCR-RFLP | 80 | 34 | All subtypes |
| Fernberg, 2010 | Caucasians | Sequenom | 2267 | 1484 | All subtypes |
| Skibola, 2010 | Caucasians, Asians | TaqMan or Pyrosequencing | 4287 | 5591 | All subtypes |
| Xiao, 2011 | Asians | PCR-RFLP | 160 | 214 | All subtypes |
| Ibrahim, 2012 | Caucasians | PCR-RFLP | 84 | 100 | BCL only |
| Hosgood, 2013 | Asians | TaqMan | 291 | 300 | All subtypes |
| Lech-Maranda, 2013 | Caucasians | TaqMan | 288 | 192 | CLL only |
| Liu, 2013 | Asians | PCR-LDR | 1932 | 3622 | TCL only |
| Nasira, 2013 | Asians | PCR-RFLP | 68 | 129 | All subtypes |
| Type | Ethnicity | Study (n) | Samples | OR (95% CI) | p | I2 (%) | phet | |
|---|---|---|---|---|---|---|---|---|
| Cases (n) | Controls (n) | |||||||
| NHL | Caucasians | 14 | 7893 | 8447 | 1.22 (1.06–1.40) | 0.007 | 60.7 | 0.002 |
| Asians | 5 | 2726 | 4530 | 0.75 (0.66–0.86) | <0.001 | 0.0 | 0.670 | |
| Overall | 19 | 10,619 | 12,977 | 1.06 (0.92–1.23) | 0.413 | 75.0 | <0.001 | |
| BCL | Caucasians | 11 | 6369 | 8085 | 1.18 (1.03–1.34) | 0.014 | 44.6 | 0.054 |
| Asians | 2 | 1723 | 3887 | 0.70 (0.52–0.94) | 0.018 | 41.9 | 0.189 | |
| Overall | 13 | 8092 | 11,972 | 1.07 (0.91–1.26) | 0.411 | 74.4 | <0.001 | |
| TCL | Caucasians | 2 | 467 | 6810 | 1.20 (1.01–1.42) | 0.040 | 0.0 | 0.361 |
| Asians | 2 | 633 | 3922 | 0.96 (0.74–1.23) | 0.723 | 57.8 | 0.124 | |
| Overall | 4 | 1100 | 10,732 | 1.11 (0.96–1.28) | 0.145 | 43.1 | 0.153 | |
| DLBCL | Caucasians | 3 | 2325 | 6930 | 1.21 (1.11–1.32) | <0.001 | 0.0 | 0.491 |
| Asians | 2 | 1028 | 3887 | 0.70 (0.57–0.86) | 0.001 | 0.0 | 0.908 | |
| Overall | 5 | 3353 | 10,817 | 0.97 (0.75–1.26) | 0.840 | 83.9 | <0.001 | |
| FL | Caucasians | 3 | 1233 | 6898 | 1.00 (0.89–1.13) | 0.949 | 31.0 | 0.235 |
| Asians | 2 | 184 | 3887 | 0.72 (0.47–1.12) | 0.142 | 12.4 | 0.285 | |
| Overall | 5 | 1417 | 10,785 | 0.98 (0.87–1.10) | 0.706 | 32.3 | 0.206 | |
| CLL/SLL | Caucasians | 6 | 1859 | 7127 | 1.02 (0.92–1.13) | 0.767 | 13.8 | 0.326 |
| MCL | Caucasians | 2 | 250 | 6810 | 1.25 (1.00–1.57) | 0.052 | 0.0 | 0.560 |
| MALT | Caucasians | 1 | 138 | 533 | 1.07 (0.76–1.51) | 0.689 | ||
| PTCL | Caucasians | 1 | 183 | 5326 | 1.11 (0.85–1.47) | 0.446 | ||
| Asians | 1 | 79 | 300 | 0.65 (0.29–1.48) | 0.303 | |||
| Overall | 2 | 262 | 5636 | 1.05 (0.80–1.36) | 0.741 | 32.9 | 0.222 | |
| NK/TCL | Asians | 2 | 190 | 3922 | 0.74 (0.46–1.17) | 0.196 | 12.4 | 0.285 |
| Type | Ethnicity | Study | Cases | Controls | ||||
|---|---|---|---|---|---|---|---|---|
| GG | GA | AA | GG | GA | AA | |||
| NHL | Caucasians | Chouchane, 1997 | 11 | 33 | 0 | 72 | 33 | 1 |
| Demeter, 1997 | 42 | 18 | 3 | 81 | 34 | 2 | ||
| Warzocha, 1998 | 203 | 65 | 5 | 69 | 24 | 3 | ||
| Fitzgibbon, 1999 | 96 | 23 | 2 | 64 | 22 | 2 | ||
| Wihlborg, 1999 | 29 | 19 | 1 | 37 | 14 | 0 | ||
| Mainou-Fowler, 2000 | 50 | 23 | 3 | 28 | 11 | 1 | ||
| Juszczynski, 2002 | 151 | 49 | 4 | 85 | 32 | 3 | ||
| Hellmig, 2005 | 93 | 39 | 6 | 360 | 160 | 13 | ||
| Bel Hadj Jrad, 2007 | 120 | 59 | 15 | 107 | 49 | 4 | ||
| Jevtovic-Stoimenov, 2008 | 32 | 46 | 2 | 19 | 14 | 1 | ||
| Fernberg, 2010 | 1490 | 675 | 102 | 1007 | 431 | 46 | ||
| Skibola, 2010 | 2712 | 1136 | 164 | 3791 | 1394 | 141 | ||
| Ibrahim, 2012 | 41 | 21 | 22 | 67 | 27 | 6 | ||
| Lech-Maranda, 2013 | 213 | 67 | 8 | 136 | 53 | 3 | ||
| Asians | Skibola, 2010 | 243 | 29 | 3 | 212 | 49 | 4 | |
| Xiao, 2011 | 138 | 20 | 2 | 174 | 35 | 5 | ||
| Hosgood, 2013 | 1702 | 221 | 9 | 3091 | 506 | 25 | ||
| Liu, 2013 | 264 | 27 | 0 | 260 | 40 | 0 | ||
| Nasira, 2013 | 58 | 9 | 1 | 105 | 22 | 2 | ||
| BCL | Caucasians | Demeter, 1997 | 42 | 18 | 3 | 81 | 34 | 2 |
| Fitzgibbon, 1999 | 96 | 23 | 2 | 64 | 22 | 2 | ||
| Wihlborg, 1999 | 29 | 19 | 1 | 37 | 14 | 0 | ||
| Mainou-Fowler, 2000 | 50 | 23 | 3 | 28 | 11 | 1 | ||
| Juszczynski, 2002 | 72 | 29 | 3 | 85 | 32 | 3 | ||
| Hellmig, 2005 | 93 | 39 | 6 | 360 | 160 | 13 | ||
| Jevtovic-Stoimenov, 2008 | 24 | 29 | 2 | 19 | 14 | 1 | ||
| Fernberg, 2010 | 1395 | 630 | 91 | 1007 | 431 | 46 | ||
| Skibola, 2010 | 2221 | 915 | 139 | 3791 | 1394 | 141 | ||
| Ibrahim, 2012 | 41 | 21 | 22 | 67 | 27 | 6 | ||
| Lech-Maranda, 2013 | 213 | 67 | 8 | 136 | 53 | 3 | ||
| BCL | Asians | Skibola, 2010 | 194 | 23 | 2 | 212 | 49 | 4 |
| Hosgood, 2013 | 1332 | 164 | 8 | 3091 | 506 | 25 | ||
| TCL | Caucasians | Fernberg, 2010 | 95 | 45 | 11 | 1007 | 431 | 46 |
| Skibola, 2010 | 216 | 90 | 10 | 3791 | 1394 | 141 | ||
| Asians | Hosgood, 2013 | 287 | 54 | 1 | 3091 | 506 | 25 | |
| Liu, 2013 | 264 | 27 | 0 | 260 | 40 | 0 | ||
| DLBCL | Caucasians | Fernberg, 2010 | 371 | 173 | 23 | 1007 | 431 | 46 |
| Juszczynski, 2002 | 72 | 29 | 3 | 85 | 32 | 3 | ||
| Skibola, 2010 | 1093 | 495 | 66 | 3791 | 1394 | 141 | ||
| Asians | Skibola, 2010 | 86 | 11 | 2 | 212 | 49 | 4 | |
| Hosgood, 2013 | 829 | 97 | 3 | 3091 | 506 | 25 | ||
| FL | Caucasians | Fitzgibbon, 1999 | 96 | 23 | 2 | 64 | 22 | 2 |
| Fernberg, 2010 | 297 | 115 | 12 | 1007 | 431 | 46 | ||
| Skibola, 2010 | 489 | 167 | 32 | 3791 | 1394 | 141 | ||
| Asians | Skibola, 2010 | 48 | 6 | 0 | 212 | 49 | 4 | |
| Hosgood, 2013 | 115 | 13 | 2 | 3091 | 506 | 25 | ||
| CLL/SLL | Caucasians | Wihlborg, 1999 | 29 | 19 | 1 | 37 | 14 | 0 |
| Mainou-Fowler, 2000 | 50 | 23 | 3 | 28 | 11 | 1 | ||
| Jevtovic-Stoimenov, 2008 | 24 | 29 | 2 | 19 | 14 | 1 | ||
| Fernberg, 2010 | 373 | 171 | 24 | 1007 | 431 | 46 | ||
| Skibola, 2010 | 605 | 193 | 25 | 3791 | 1394 | 141 | ||
| Lech-Maranda, 2013 | 213 | 67 | 8 | 136 | 53 | 3 | ||
| MCL | Caucasians | Fernberg, 2010 | 76 | 33 | 10 | 1007 | 431 | 46 |
| Skibola, 2010 | 90 | 35 | 6 | 3791 | 1394 | 141 | ||
| MALT | Caucasians | Hellming, 2005 | 93 | 39 | 6 | 360 | 160 | 13 |
| PTCL | Caucasians | Skibola, 2010 | 125 | 53 | 5 | 3791 | 1394 | 141 |
| Asians | Liu, 2013 | 72 | 7 | 0 | 260 | 40 | 0 | |
| NK/TCL | Asians | Hosgood, 2013 | 89 | 14 | 0 | 3091 | 506 | 25 |
| Liu, 2013 | 81 | 6 | 0 | 260 | 40 | 0 | ||
© 2014 by the authors; licensee MDPI, Basel, Switzerland This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Zhai, K.; Ding, J.; Zhou, Y. Different Role of Tumor Necrosis Factor-α Polymorphism in Non-Hodgkin Lymphomas among Caucasian and Asian Populations: A Meta-Analysis. Int. J. Mol. Sci. 2014, 15, 7684-7698. https://doi.org/10.3390/ijms15057684
Zhai K, Ding J, Zhou Y. Different Role of Tumor Necrosis Factor-α Polymorphism in Non-Hodgkin Lymphomas among Caucasian and Asian Populations: A Meta-Analysis. International Journal of Molecular Sciences. 2014; 15(5):7684-7698. https://doi.org/10.3390/ijms15057684
Chicago/Turabian StyleZhai, Kan, Jie Ding, and Yan Zhou. 2014. "Different Role of Tumor Necrosis Factor-α Polymorphism in Non-Hodgkin Lymphomas among Caucasian and Asian Populations: A Meta-Analysis" International Journal of Molecular Sciences 15, no. 5: 7684-7698. https://doi.org/10.3390/ijms15057684