Endothelial Nitric Oxide Synthase (eNOS) 4b/a Gene Polymorphisms and Coronary Artery Disease: Evidence from a Meta-Analysis

Abstract
:1. Introduction
2. Results and Discussion
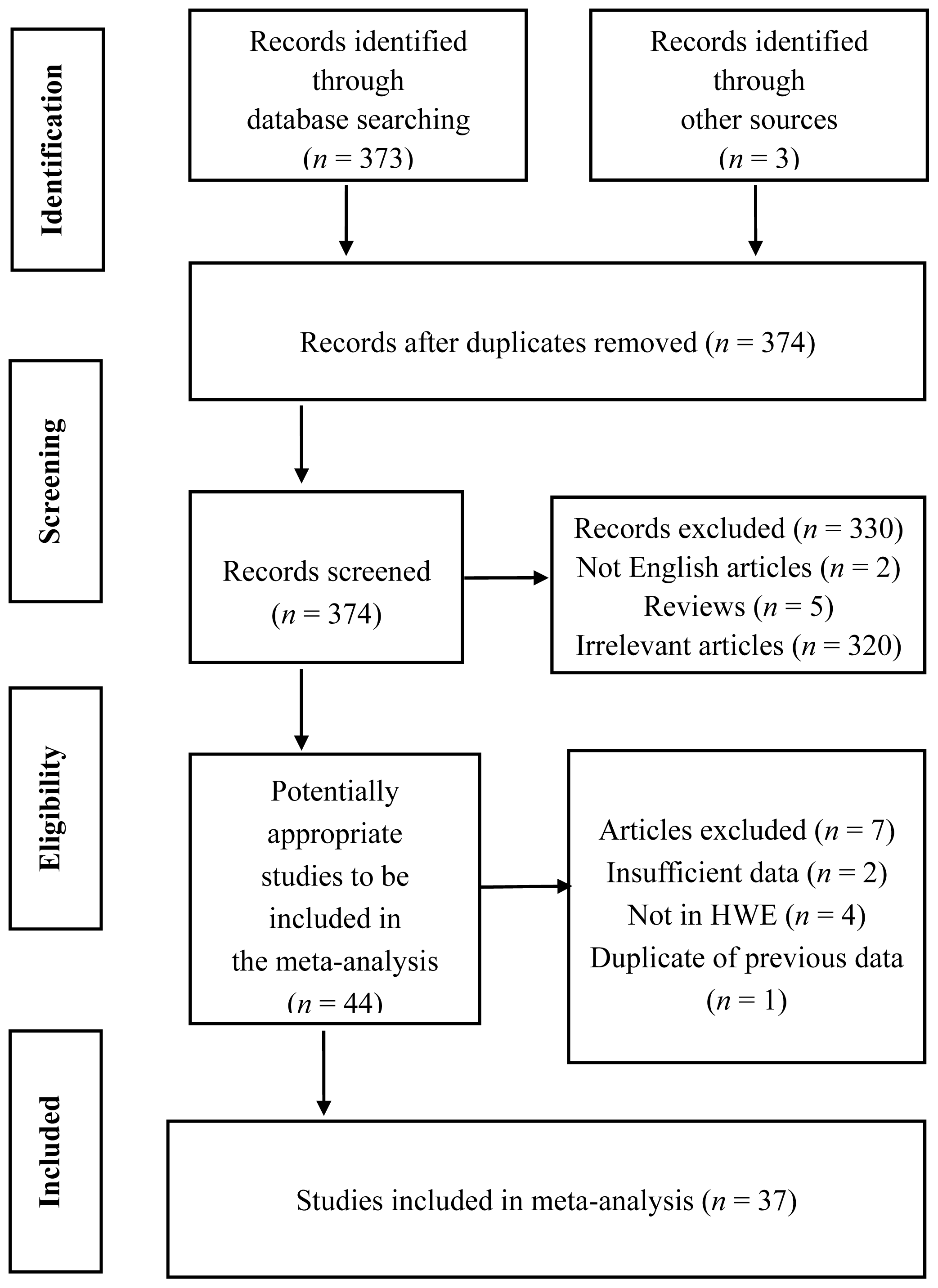
2.1. Characteristics of Included Studies
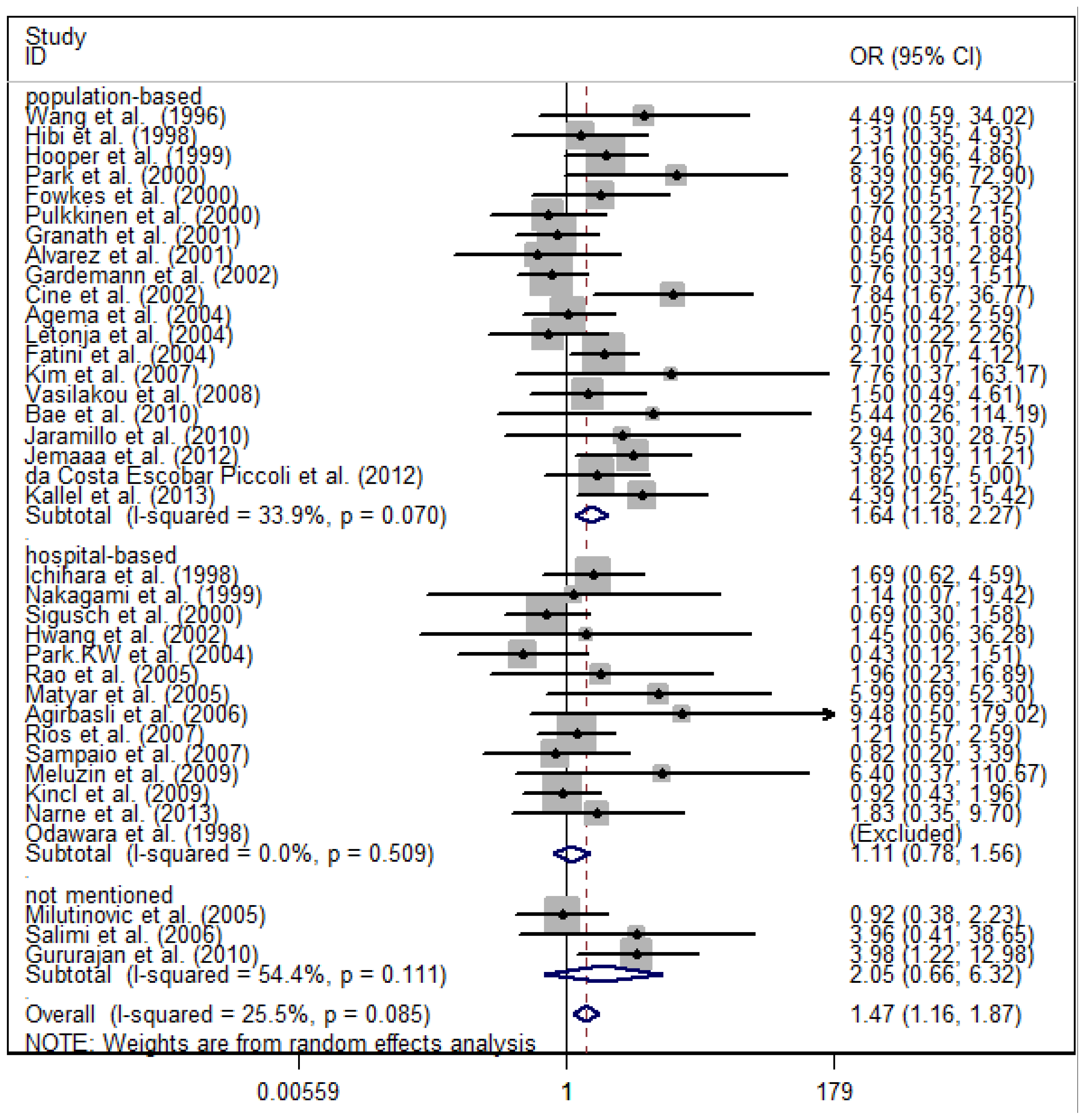
2.2. Meta-Analysis Results
2.3. Evaluation of Heterogeneity
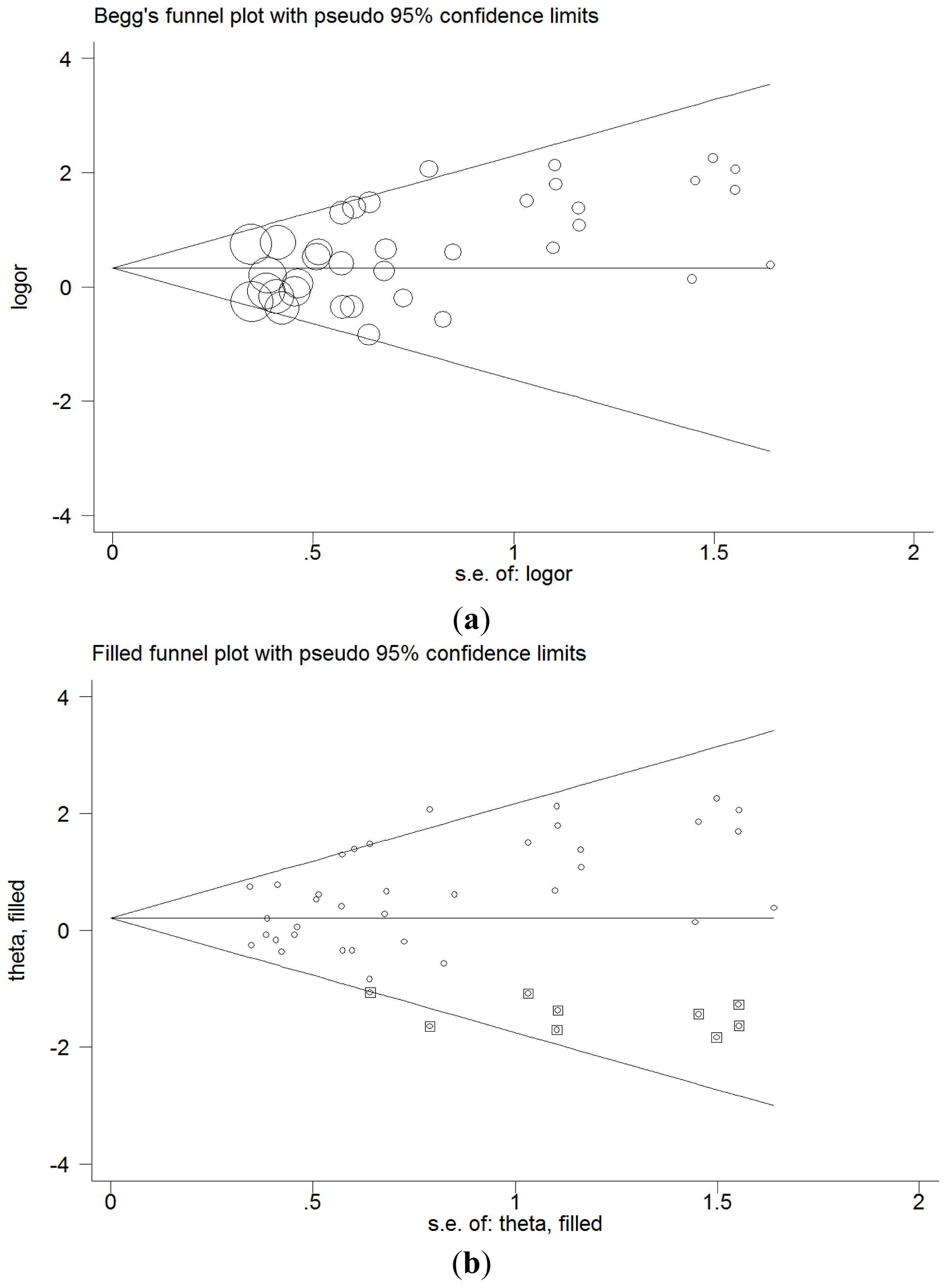
2.4. Sensitivity Analysis and Publication Bias
2.5. Discussion
3. Experimental Section
3.1. Literature Search
3.2. Inclusion and Exclusion Criteria
3.3. Data Extraction
3.4. Statistical Analysis
4. Conclusions
Supplementary Information
ijms-15-07987-s001.pdfAcknowledgments
Conflicts of Interest
References
- Gouvinhas, C.; Severo, M.; Azevedo, A.; Lunet, N. Worldwide patterns of ischemic heart disease mortality from 1980 to 2010. Int. J. Cardiol 2013, 170, 309–314. [Google Scholar]
- Salomon, J.A.; Vos, T.; Hogan, D.R.; Gagnon, M.; Naghavi, M.; Mokdad, A.; Begum, N.; Shah, R.; Karyana, M.; Kosen, S.; et al. Common values in assessing health outcomes from disease and injury: Disability weights measurement study for the global burden of disease study 2010. Lancet 2012, 380, 2129–2143. [Google Scholar]
- Prins, B.P.; Lagou, V.; Asselbergs, F.W.; Snieder, H.; Fu, J. Genetics of coronary artery disease: Genome- wide association studies and beyond. Atherosclerosis 2012, 225, 1–10. [Google Scholar]
- Smith, F.B.; Lee, A.J.; Fowkes, F.G.; Price, J.F.; Rumley, A.; Lowe, G.D. Hemostatic factors as predictors of ischemic heart disease and stroke in the Edinburgh artery study. Arterioscler. Thromb. Vasc. Biol 1997, 17, 3321–3325. [Google Scholar]
- Kraus, W.E. Genetic approaches for the investigation of genes associated with coronary heart disease. Am. Heart J 2000, 140, S27–S35. [Google Scholar]
- Kugiyama, K.; Yasue, H.; Okumura, K.; Ogawa, H.; Fujimoto, K.; Nakao, K.; Yoshimura, M.; Motoyama, T.; Inobe, Y.; Kawano, H. Nitric oxide activity is deficient in spasm arteries of patients with coronary spastic angina. Circulation 1996, 94, 266–271. [Google Scholar]
- Nathan, C.; Xie, Q.W. Nitric oxide synthases: Roles, tolls, and controls. Cell 1994, 78, 915–918. [Google Scholar]
- Marsden, P.A.; Heng, H.H.; Scherer, S.W.; Stewart, R.J.; Hall, A.V.; Shi, X.M.; Tsui, L.C.; Schappert, K.T. Structure and chromosomal localization of the human constitutive endothelial nitric oxide synthase gene. J. Biol. Chem 1993, 268, 17478–17488. [Google Scholar]
- Wang, X.L.; Sim, A.S.; Badenhop, R.F.; McCredie, R.M.; Wilcken, D.E. A smoking- dependent risk of coronary artery disease associated with a polymorphism of the endothelial nitric oxide synthase gene. Nat. Med 1996, 2, 41–45. [Google Scholar]
- Casas, J.P.; Bautista, L.E.; Humphries, S.E.; Hingorani, A.D. Endothelial nitric oxide synthase genotype and ischemic heart disease: Meta-analysis of 26 studies involving 23028 subjects. Circulation 2004, 109, 1359–1365. [Google Scholar]
- Li, J.; Wu, X.; Li, X.; Feng, G.; He, L.; Shi, Y. The endothelial nitric oxide synthase gene is associated with coronary artery disease: A meta-analysis. Cardiology 2010, 116, 271–278. [Google Scholar]
- Hooper, W.C.; Lally, C.; Austin, H.; Benson, J.; Dilley, A.; Wenger, N.K.; Whitsett, C.; Rawlins, P.; Evatt, B.L. The relationship between polymorphisms in the endothelial cell nitric oxide synthase gene and the platelet gpiiia gene with myocardial infarction and venous thromboembolism in African Americans. Chest 1999, 116, 880–886. [Google Scholar]
- Kallel, A.; Sbai, M.H.; Sediri, Y.; Abdessalem, S.; Mourali, M.S.; Feki, M.; Mechmeche, R.; Jemaa, R.; Kaabachi, N. Polymorphisms of the NOS3 gene and risk of myocardial infarction in the Tunisian population. Cytokine 2013, 64, 646–651. [Google Scholar]
- Jemaa, R.; Kallel, A.; Sediri, Y.; Abdessalem, S.; Mourali, M.S.; Feki, M.; Mechmeche, R.; Kaabachi, N. Association between endothelial nitric oxide gene intron 4a 4b VNTR polymorphism and plasma homocysteine concentrations in Tunisian male patients with myocardial infarction. Nutr. Res 2012, 32, 342–346. [Google Scholar]
- Hibi, K.; Ishigami, T.; Tamura, K.; Mizushima, S.; Nyui, N.; Fujita, T.; Ochiai, H.; Kosuge, M.; Watanabe, Y.; Yoshii, Y.; et al. Endothelial nitric oxide synthase gene polymorphism and acute myocardial infarction. Hypertension 1998, 32, 521–526. [Google Scholar]
- Ichihara, S.; Yamada, Y.; Fujimura, T.; Nakashima, N.; Yokota, M. Association of a polymorphism of the endothelial constitutive nitric oxide synthase gene with myocardial infarction in the Japanese population. Am. J. Cardiol 1998, 81, 83–86. [Google Scholar]
- Odawara, M.; Sasaki, K.; Tachi, Y.; Yamashita, K. Endothelial nitric oxide synthase gene polymorphism and coronary heart disease in Japanese NIDDM. Diabetologia 1998, 41, 365–366. [Google Scholar]
- Nakagami, H.; Ikeda, U.; Maeda, Y.; Yamamoto, K.; Hojo, Y.; Kario, K.; Kuroki, S.; Shimada, K. Coronary artery disease and endothelial nitric oxide synthase and angiotensin-converting enzyme gene polymorphisms. J. Thromb. Thrombolysis 1999, 8, 191–195. [Google Scholar]
- Park, J.E.; Lee, W.H.; Hwang, T.H.; Chu, J.A.; Kim, S.; Choi, Y.H.; Kim, J.S.; Kim, D.K.; Lee, S.H.; Hong, K.P.; et al. Aging affects the association between endothelial nitric oxide synthase gene polymorphism and acute myocardial infarction in the Korean male population. Korean J. Intern. Med 2000, 15, 65–70. [Google Scholar]
- Hwang, J.J.; Tsai, C.T.; Yeh, H.M.; Chiang, F.T.; Hsu, K.L.; Tseng, C.D.; Liau, C.S.; Tseng, Y.Z.; Lai, L.P. The 27-bp tandem repeat polymorphism in intron 4 of the endothelial nitric oxide synthase gene is not associated with coronary artery disease in a hospital-based Taiwanese population. Cardiology 2002, 97, 67–72. [Google Scholar]
- Park, K.W.; You, K.H.; Oh, S.; Chae, I.H.; Kim, H.S.; Oh, B.H.; Lee, M.M.; Park, Y.B. Association of endothelial constitutive nitric oxide synthase gene polymorphism with acute coronary syndrome in Koreans. Heart 2004, 90, 282–285. [Google Scholar]
- Kim, I.J.; Bae, J.; Lim, S.W.; Cha, D.H.; Cho, H.J.; Kim, S.; Yang, D.H.; Hwang, S.G.; Oh, D.; Kim, N.K. Influence of endothelial nitric oxide synthase gene polymorphisms (-786T>C, 4a4b, 894G>T) in Korean patients with coronary artery disease. Thromb. Res 2007, 119, 579–585. [Google Scholar]
- Bae, J.; Kim, I.J.; Hong, S.H.; Sung, J.H.; Lim, S.W.; Cha, D.H.; Cho, Y.W.; Oh, D.; Kim, N.K. Association of endothelial nitric oxide synthase polymorphisms with coronary artery disease in Korean individuals with or without diabetes mellitus. Exp. Ther. Med 2010, 1, 719–724. [Google Scholar]
- Gururajan, P.; Gurumurthy, P.; Victor, D.; Rao, G.S.N.; Babu, R.S.; Bharati, A.S.; Cherian, K.M. Plasma total nitric oxide and endothelial constitutive nitric oxide synthase (ecNOS) gene polymorphism: A study in a South Indian population. Biochem. Genet 2011, 49, 96–103. [Google Scholar]
- Narne, P.; Ponnaluri, K.C.; Singh, S.; Siraj, M.; Ishaq, M. Association of the genetic variants of endothelial nitric oxide synthase gene with angiographically defined coronary artery disease and myocardial infarction in south Indian patients with type 2 diabetes mellitus. J. Diabetes Complicat 2013, 27, 255–261. [Google Scholar]
- Fowkes, F.G.; Lee, A.J.; Hau, C.M.; Cooke, A.; Connor, J.M.; Lowe, G.D. Methylene tetrahydrofolate reductase (MTHFR) and nitric oxide synthase (ecNOS) genes and risks of peripheral arterial disease and coronary heart disease: Edinburgh artery study. Atherosclerosis 2000, 150, 179–185. [Google Scholar]
- Pulkkinen, A.; Viitanen, L.; Kareinen, A.; Lehto, S.; Vauhkonen, I.; Laakso, M. Intron 4 polymorphism of the endothelial nitric oxide synthase gene is associated with elevated blood pressure in type 2 diabetic patients with coronary heart disease. J. Mol. Med 2000, 78, 372–379. [Google Scholar]
- Sigusch, H.H.; Surber, R.; Lehmann, M.H.; Surber, S.; Weber, J.; Henke, A.; Reinhardt, D.; Hoffmann, A.; Figulla, H.R. Lack of association between 27-bp repeat polymorphism in intron 4 of the endothelial nitric oxide synthase gene and the risk of coronary artery disease. Scand. J. Clin. Lab. Investig 2000, 60, 229–235. [Google Scholar]
- Alvarez, R.; Gonzalez, P.; Batalla, A.; Reguero, J.R.; Iglesias-Cubero, G.; Hevia, S.; Cortina, A.; Merino, E.; Gonzalez, I.; Alvarez, V.; et al. Association between the NOS3 (−786 T/C) and the ACE (I/D) DNA genotypes and early coronary artery disease. Nitric Oxide 2001, 5, 343–348. [Google Scholar]
- Granath, B.; Taylor, R.R.; van Bockxmeer, F.M.; Mamotte, C.D. Lack of evidence for association between endothelial nitric oxide synthase gene polymorphisms and coronary artery disease in the Australian Caucasian population. Eur. J. Prev. Cardiol 2001, 8, 235–241. [Google Scholar]
- Gardemann, A.; Lohre, J.; Cayci, S.; Katz, N.; Tillmanns, H.; Haberbosch, W. The T allele of the missense Glu298Asp endothelial nitric oxide synthase gene polymorphism is associated with coronary heart disease in younger individuals with high atherosclerotic risk profile. Atherosclerosis 2002, 160, 167–175. [Google Scholar]
- Agema, W.R.; de Maat, M.P.; Zwinderman, A.H.; Kastelein, J.J.; Rabelink, T.J.; van Boven, A.J.; Feskens, E.J.; Boer, J.M.; van der Wall, E.E.; Jukema, J.W. An integrated evaluation of endothelial constitutive nitric oxide synthase polymorphisms and coronary artery disease in men. Clin. Sci 2004, 107, 255–261. [Google Scholar]
- Fatini, C.; Sofi, F.; Sticchi, E.; Gensini, F.; Gori, A.M.; Fedi, S.; Lapini, I.; Rostagno, C.; Comeglio, M.; Brogi, D.; et al. Influence of endothelial nitric oxide synthase gene polymorphisms (G894T, 4a4b, T-786C) and hyperhomocysteinemia on the predisposition to acute coronary syndromes. Am. Heart J 2004, 147, 516–521. [Google Scholar]
- Letonja, M. The eNOS gene polymorphism does not have a major impact on lipid parameters and premature coronary artery disease in Caucasian women. Acta Cardiol 2004, 59, 618–622. [Google Scholar]
- Milutinovic, A.; Hruskovicova, H. The eNOS gene polymorphism does not have a major impact on lipid parameters and premature coronary artery disease in Slovene men (Caucasians). Folia Biol 2005, 51, 47–49. [Google Scholar]
- Vasilakou, M.; Votteas, V.; Kasparian, C.; Pantazopoulos, N.; Dedoussis, G.; Deltas, C.; Nastos, P.; Nikolakis, D.; Lamnissou, K. Lack of association between endothelial nitric oxide synthase gene polymorphisms and risk of premature coronary artery disease in the Greek population. Acta Cardiol 2008, 63, 609–614. [Google Scholar]
- Kincl, V.; Vasku, A.; Meluzin, J.; Panovsky, R.; Semenka, J.; Groch, L. Association of the eNOS 4a/b and -786T/C polymormphisms with coronary artery disease, obesity and diabetes mellitus. Folia Biol 2009, 55, 187–191. [Google Scholar]
- Meluzin, J.; Vasku, A.; Kincl, V.; Panovsky, R.; Sramkova, T. Association of coronary artery disease, erectile dysfunction, and endothelial nitric oxide synthase polymorphisms. Heart Vessels 2009, 24, 157–163. [Google Scholar]
- Rao, S.; Austin, H.; Davidoff, M.N.; Zafari, A.M. Endothelial nitric oxide synthase intron 4 polymorphism is a marker for coronary artery disease in African-American and Caucasian men. Ethn. Dis 2005, 15, 191–197. [Google Scholar]
- Rios, D.L.; D’Onofrio, L.O.; Souza, J.K.; Queiroz, A.M.; Raduy-Maron, L.; Silva-Neto, N.; Carvalho, H.G.; Santos-Filho, A.; Galvao-Castro, B. Smoking-dependent and haplotype-specific effects of endothelial nitric oxide synthase gene polymorphisms on angiographically assessed coronary artery disease in Caucasian- And african-Brazilians. Atherosclerosis 2007, 193, 135–141. [Google Scholar]
- Cine, N.; Hatemi, A.C.; Erginel-Unaltuna, N. Association of a polymorphism of the ecNOS gene with myocardial infarction in a subgroup of Turkish MI patients. Clin. Genet 2002, 61, 66–70. [Google Scholar]
- Matyar, S.; Attila, G.; Acarturk, E.; Akpinar, O.; Inal, T. eNOS gene intron 4 a/b VNTR polymorphism is a risk factor for coronary artery disease in Southern Turkey. Clin. Chim. Acta 2005, 354, 153–158. [Google Scholar]
- Agirbasli, D.; Agirbasli, M.; Williams, S.M.; Phillips, J.A., III. Interaction among 5,10 methylenetetrahydrofolate reductase, plasminogen activator inhibitor and endothelial nitric oxide synthase gene polymorphisms predicts the severity of coronary artery disease in Turkish patients. Coron. Artery Dis 2006, 17, 413–417. [Google Scholar]
- Salimi, S.; Firoozrai, M.; Nourmohammadi, I.; Shabani, M.; Mohebbi, A. Endothelial nitric oxide synthase gene intron4 VNTR polymorphism in patients with coronary artery disease in Iran. Indian J. Med. Res 2006, 124, 683–688. [Google Scholar]
- Sampaio, M.F.; Hirata, M.H.; Hirata, R.D.; Santos, F.C.; Picciotti, R.; Luchessi, A.D.; de Quateli Doi, S.; Armaganijan, D.; Batlouni, M. AMI is associated with polymorphisms in the NOS3 and FGB but not in PAI-1 genes in young adults. Clin. Chim. Acta 2007, 377, 154–162. [Google Scholar]
- Jaramillo, P.C.; Lanas, C.; Lanas, F.; Salazar, L.A. Polymorphisms of the NOS3 gene in Southern Chilean subjects with coronary artery disease and controls. Clin. Chim. Acta 2010, 411, 258–262. [Google Scholar]
- Da Costa, Escobar; Piccoli, J.; Manfredini, V.; Hamester, F.I.; Bandinelli, J.B.; Turkienicz, I.M.; Chies, J.A.; Peres, A.; Bodanese, L.C.; Bogo, M.R. Interaction between endothelial nitric oxide synthase gene polymorphisms (-786T>C, 894G>T and intron 4 a/b) and cardiovascular risk factors in acute coronary syndromes. Arch. Med. Res 2012, 43, 205–211. [Google Scholar]
- Tsukada, T.; Yokoyama, K.; Arai, T.; Takemoto, F.; Hara, S.; Yamada, A.; Kawaguchi, Y.; Hosoya, T.; Igari, J. Evidence of association of the ecNOS gene polymorphism with plasma no metabolite levels in humans. Biochem. Biophys. Res. Commun 1998, 245, 190–193. [Google Scholar]
- Rittig, K.; Holder, K.; Stock, J.; Tschritter, O.; Peter, A.; Stefan, N.; Fritsche, A.; Machicao, F.; Haring, H.U.; Balletshofer, B. Endothelial no-synthase intron 4 polymorphism is associated with disturbed in vivo nitric oxide production in individuals prone to type 2 diabetes. Horm. Metab. Res 2008, 40, 13–17. [Google Scholar]
- Kojda, G.; Harrison, D. Interactions between no and reactive oxygen species: Pathophysiological importance in atherosclerosis, hypertension, diabetes and heart failure. Cardiovasc. Res 1999, 43, 562–571. [Google Scholar]
- Skovgaard, N.; Galli, G.; Abe, A.; Taylor, E.W.; Wang, T. The role of nitric oxide in regulation of the cardiovascular system in reptiles. Comp. Biochem. Physiol. A Mol. Integr. Physiol 2005, 142, 205–214. [Google Scholar]
- Wang, J.; Dudley, D.; Wang, X.L. Haplotype-specific effects on endothelial no synthase promoter efficiency: Modifiable by cigarette smoking. Arteriosclerosis 2002, 22, e1–e4. [Google Scholar]
- Yoon, Y.; Song, J.; Hong, S.H.; Kim, J.Q. Plasma nitric oxide concentrations and nitric oxide synthase gene polymorphisms in coronary artery disease. Clin. Chem 2000, 46, 1626–1630. [Google Scholar]
- Lee, W.H.; Hwang, T.H.; Oh, G.T.; Kwon, S.U.; Choi, Y.H.; Park, J.E. Genetic factors associated with endothelial dysfunction affect the early onset of coronary artery disease in Korean males. Vasc. Med 2001, 6, 103–108. [Google Scholar]
- Angeline, T.; Isabel, W.; Tsongalis, G.J. Endothelial nitric oxide gene polymorphisms, nitric oxide production and coronary artery disease risk in a South Indian population. Exp. Mol. Pathol 2010, 89, 205–208. [Google Scholar]
- Syed, R.; Biyabani, M.U.; Prasad, S.; Deeba, F.; Jamil, K. Correlation and identification of variable number of tandem repeats of eNOS gene in coronary artery disease (CAD). Saudi J. Biol. Sci 2010, 17, 209–213. [Google Scholar]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Author | Year | Country | Ethnicity | Source of controls | End points | Sample size | Genotype distribution | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Control | Case | ||||||||||||
| Control | Case | aa | ab | bb | aa | ab | bb | ||||||
| Wang et al. | 1996 | Australia | Caucasian | PB | CAD | 153 | 549 | 1 | 50 | 102 | 18 | 122 | 409 |
| Hibi et al. | 1998 | Japan | Asian | PB | AMI | 357 | 226 | 5 | 68 | 284 | 4 | 48 | 174 |
| Ichihara et al. | 1998 | Japan | Asian | HB | MI | 550 | 455 | 7 | 97 | 446 | 9 | 107 | 339 |
| Odawara et al. | 1998 | Japan | Asian | HB | CHD | 122 | 42 | 0 | 19 | 103 | 0 | 11 | 31 |
| Hooper et al. | 1999 | American | African | PB | MI | 185 | 110 | 15 | 68 | 102 | 14 | 52 | 44 |
| Nakagami et al. | 1999 | Japan | Asian | HB | CAD | 34 | 40 | 1 | 9 | 24 | 1 | 18 | 21 |
| Park et al. | 2000 | Korea | Asian | PB | AMI | 206 | 121 | 1 | 49 | 156 | 5 | 23 | 93 |
| Fowkes et al. | 2000 | UK | Caucasian | PB | CHD | 300 | 137 | 5 | 64 | 231 | 4 | 37 | 96 |
| Pulkkinen et al. | 2000 | Finland | Caucasian | PB | CHD | 110 | 308 | 5 | 26 | 79 | 9 | 96 | 203 |
| Sigusch et al. | 2000 | Germany | Caucasian | HB | CHD | 413 | 625 | 11 | 115 | 287 | 12 | 159 | 454 |
| Granath et al. | 2001 | Australia | Caucasian | PB | CAD | 620 | 567 | 14 | 158 | 448 | 11 | 138 | 418 |
| Alvarez et al. | 2001 | Spain | Caucasian | PB | CAD | 300 | 170 | 6 | 72 | 222 | 2 | 37 | 131 |
| Hwang et al. | 2002 | Taiwan | Asian | HB | CAD | 70 | 149 | 0 | 14 | 56 | 1 | 32 | 116 |
| Gardemann et al. | 2002 | Germany | Caucasian | PB | MI | 528 | 1265 | 13 | 144 | 371 | 25 | 306 | 934 |
| Cine et al. | 2002 | Turkey | other | PB | MI | 306 | 207 | 2 | 55 | 249 | 9 | 55 | 143 |
| Park et al. | 2004 | Korea | Asian | HB | ACS | 142 | 164 | 7 | 30 | 105 | 4 | 21 | 139 |
| Agema et al. | 2004 | Netherlands | Caucasian | PB | CAD | 466 | 752 | 8 | 77 | 381 | 12 | 195 | 545 |
| Letonja et al. | 2004 | Slovenia | Caucasian | PB | CAD | 109 | 151 | 6 | 30 | 73 | 6 | 41 | 104 |
| Fatini et al. | 2004 | Italy | Caucasian | PB | ACS | 537 | 477 | 14 | 138 | 385 | 24 | 138 | 315 |
| Milutinovic et al. | 2005 | Slovenia | Caucasian | NM | CAD | 188 | 215 | 10 | 58 | 120 | 11 | 60 | 144 |
| Rao et al. | 2005 | America | Caucasia + African | HB | CAD | 50 | 144 | 1 | 17 | 32 | 6 | 40 | 98 |
| Matyar et al. | 2005 | Turkey | other | HB | CAD | 133 | 133 | 1 | 35 | 97 | 5 | 47 | 81 |
| Salimi et al. | 2006 | Iran | other | NM | CAD | 158 | 141 | 1 | 29 | 128 | 3 | 41 | 97 |
| Agirbasli et al. | 2006 | Turkey | other | HB | CAD | 100 | 100 | 0 | 21 | 79 | 4 | 21 | 75 |
| Kim et al. | 2007 | Korea | Asian | PB | CAD | 211 | 147 | 0 | 40 | 171 | 2 | 35 | 110 |
| Rios et al. | 2007 | Brazil | Caucasia + African | HB | CAD | 267 | 323 | 12 | 90 | 165 | 18 | 101 | 204 |
| Sampaio et al. | 2007 | Brazil | other | HB | AMI | 103 | 115 | 4 | 32 | 67 | 4 | 29 | 82 |
| Vasilakou et al. | 2008 | Greece | Caucasian | PB | CAD | 161 | 209 | 5 | 39 | 117 | 9 | 60 | 140 |
| Meluzin et al. | 2009 | Czech rep | Caucasian | HB | CAD | 89 | 321 | 0 | 26 | 63 | 10 | 103 | 208 |
| Kincl et al. | 2009 | Czech rep | Caucasian | HB | CAD | 222 | 939 | 9 | 63 | 150 | 35 | 272 | 632 |
| Bae et al. | 2010 | Korea | Asian | PB | CAD | 196 | 192 | 0 | 35 | 161 | 2 | 42 | 148 |
| Gururajan et al. | 2010 | India | Asian | NM | ACS | 100 | 106 | 4 | 19 | 77 | 12 | 36 | 58 |
| Jaramillo et al. | 2010 | Chile | other | PB | CAD | 112 | 112 | 1 | 16 | 95 | 3 | 12 | 97 |
| Jemaaa et al. | 2012 | Tunisia | African | PB | MI | 250 | 310 | 4 | 61 | 185 | 15 | 105 | 190 |
| Da Costa Escobar Piccoli et al. | 2012 | Brazil | other | PB | ACS | 108 | 132 | 6 | 34 | 68 | 14 | 31 | 87 |
| Kallel et al. | 2013 | Tunisia | African | PB | MI | 225 | 303 | 3 | 58 | 164 | 15 | 101 | 187 |
| Narne et al. | 2013 | India | Asian | HB | CAD | 121 | 160 | 2 | 42 | 77 | 5 | 50 | 105 |
| Total and subgroups | Studies | Homozygote comparison (aa vs. bb) | Heterozygote comparison (ab vs. bb) | Dominant model (aa + ab vs. bb) | Recessive model (ab + bb vs. aa) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | p | I2 (%) | OR (95% CI) | p | I2 (%) | OR (95% CI) | p | I2 (%) | OR (95% CI) | p | I2 (%) | ||
| Total | 37 | 1.47 (1.16–1.87) | 0.085 | 25.5 | 1.14 (1.02–1.27) | <0.001 | 56.7 | 1.18 (1.06–1.33) | <0.001 | 61.1 | 0.72 (0.58–0.89) | 0.213 | 15.4 |
| MI | 6 | 2.30 (1.17–4.51) | 0.020 | 62.6 | 1.42 (1.07–1.89) | 0.002 | 74.2 | 1.50 (1.09–2.07) | <0.001 | 80.7 | 0.56 (0.39–0.82) | 0.054 | 54.1 |
| Ethnicity | |||||||||||||
| Caucasian | 16 | 1.03 (0.80–1.31) | 0.621 | 0.0 | 1.04 (0.90–1.20) | 0.006 | 53.3 | 1.04 (0.91–1.19) | 0.007 | 53.0 | 0.98 (0.77–1.25) | 0.679 | 0.0 |
| Asian | 11 | 1.82 (1.03–3.20) | 0.316 | 13.8 | 1.21 (0.96–1.54) | 0.027 | 50.5 | 1.26 (0.99–1.61) | 0.011 | 56.3 | 0.60 (0.36–0.99) | 0.434 | 0.4 |
| African | 5 | 2.93 (1.71–5.03) | 0.821 | 0.0 | 1.46 (1.16–1.83) | 0.353 | 9.4 | 1.58 (1.27–1.96) | 0.370 | 6.5 | 0.41 (0.24–0.70) | 0.684 | 0.0 |
| Other | 7 | 2.65 (1.37–5.13) | 0.369 | 7.8 | 1.17 (0.84–1.62) | 0.033 | 56.4 | 1.29 (0.94–1.77) | 0.033 | 56.3 | 0.39 (0.21–0.71) | 0.511 | 0.0 |
| Source of control | |||||||||||||
| HB | 14 | 1.11 (0.78–1.56) | 0.509 | 0.0 | 1.04 (0.88–1.23) | 0.072 | 38.2 | 1.07 (0.89–1.27) | 0.027 | 46.8 | 0.90 (0.64–1.26) | 0.613 | 0.0 |
| PB | 20 | 1.64 (1.18–2.27) | 0.070 | 33.9 | 1.16 (1.00–1.35) | <0.001 | 61.8 | 1.21 (1.05–1.40) | <0.001 | 63.4 | 0.65 (0.48–0.89) | 0.113 | 28.7 |
| NM | 3 | 2.05 (0.66–6.32) | 0.111 | 54.4 | 1.54 (0.80–2.98) | 0.011 | 77.6 | 1.63 (0.80–3.30) | 0.003 | 82.6 | 0.58 (0.24–1.40) | 0.232 | 31.6 |
| Case size | |||||||||||||
| >500 | 6 | 0.88 (0.62–1.24) | 0.666 | 0.0 | 0.96 (0.74–1.25) | <0.001 | 78.7 | 0.97 (0.76–1.22) | 0.001 | 75.9 | 1.14 (0.80–1.60) | 0.642 | 0.0 |
| <500 | 31 | 1.75 (1.35–2.28) | 0.262 | 13.2 | 1.20 (1.07–1.35) | 0.011 | 40.7 | 1.26 (1.11–1.42) | 0.002 | 48.0 | 0.61 (0.48–0.77) | 0.453 | 0.8 |
| Control size | |||||||||||||
| >500 | 4 | 1.21 (0.72–2.05) | 0.138 | 45.6 | 1.07 (0.85–1.36) | 0.024 | 68.3 | 1.09 (0.84–1.42) | 0.007 | 75.1 | 0.84 (0.52–1.34) | 0.214 | 33.1 |
| <500 | 33 | 1.56 (1.19–2.05) | 0.113 | 23.9 | 1.15 (1.01–1.31) | <0.001 | 55.6 | 1.20 (1.06–1.36) | <0.001 | 59.0 | 0.68 (0.53–0.88) | 0.233 | 14.8 |
© 2014 by the authors; licensee MDPI, Basel, Switzerland This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Yang, Y.; Du, K.; Liu, Z.; Lu, X. Endothelial Nitric Oxide Synthase (eNOS) 4b/a Gene Polymorphisms and Coronary Artery Disease: Evidence from a Meta-Analysis. Int. J. Mol. Sci. 2014, 15, 7987-8003. https://doi.org/10.3390/ijms15057987
Yang Y, Du K, Liu Z, Lu X. Endothelial Nitric Oxide Synthase (eNOS) 4b/a Gene Polymorphisms and Coronary Artery Disease: Evidence from a Meta-Analysis. International Journal of Molecular Sciences. 2014; 15(5):7987-8003. https://doi.org/10.3390/ijms15057987
Chicago/Turabian StyleYang, Yujiao, Kang Du, Zhengxia Liu, and Xiang Lu. 2014. "Endothelial Nitric Oxide Synthase (eNOS) 4b/a Gene Polymorphisms and Coronary Artery Disease: Evidence from a Meta-Analysis" International Journal of Molecular Sciences 15, no. 5: 7987-8003. https://doi.org/10.3390/ijms15057987