
Reduced 5-Methylcytosine Level as a Potential Progression Predictor in Patients with T1 or Non-Invasive Urothelial Carcinoma

 ,
,
Abstract
:1. Introduction
2. Results and Discussion
2.1. Study Subjects

{kind=link}
{kind=link}
{kind=link}
| Variables | n (%) | H-Score (Mean ± SD) | ||
|---|---|---|---|---|
| 5-MeC | DNMT1 | |||
| All cases | 150 (100.0) | 104.9 ± 23.2 | 162.3 ± 19.3 | |
| Age (year) | Median (range) | 68 (26–87) | – | – |
| Sex | Male | 65 (43.3) | 109.9 ± 25.6 | 163.5 ± 19.9 |
| Female | 85 (56.7) | 101.0 ± 20.5 | 161.4 ± 8.9 | |
| Smoking | Never | 66 (44.0) | 108.5 ± 24.1 | 161.8 ± 17.3 |
| Ever | 36 (24.0) | 109.4 ± 22.5 | 159.9 ± 23.3 | |
| Missing cases | 48 (32.0) | – | – | |
| Tumor histology | UIS | 5 (3.3) | 126.8 ± 18.3 | 174.8 ± 21.3 |
| Noninvasive papillary UC | 35 (23.3) | 110.7 ± 24.2 | 162.4 ± 22.7 | |
| Invasive UC | 108 (72.0) | 102.1 ± 23.3 | 161.7 ± 18.1 | |
| Small cell carcinoma | 2 (1.4) | 115.7 ± 3.9 | 149.6 ± 0.38 | |
| Tumor location | Pelvis | 27 (18.0) | 108.7 ± 22.4 | 163.2 ± 17.6 |
| Ureter | 65 (43.3) | 98.0 ± 20.8 | 161.4 ± 17.4 | |
| Urinary bladder | 58 (38.7) | 110.9 ± 24.3 | 162.8 ± 22.2 | |
| Tumor grading | Low grade | 34 (22.7) | 107.3 ± 25.1 | 166.1 ± 20.7 |
| High grade | 116 (77.3) | 104.2 ± 22.7 | 161.2 ± 8.9 | |
| TNM stage | 0a | 35 (23.3) | 110.7 ± 4.2 | 162.4 ± 22.7 |
| 0is | 5 (3.3) | 126.8 ± 18.3 | 174.8 ± 1.3 | |
| I | 42 (28.0) | 105.0 ± 22.9 | 162.9 ± 18.6 | |
| II | 34 (22.7) | 100.3 ± 20.2 | 159.2 ± 19.0 | |
| III | 33 (22.0) | 99.8 ± 24.2 | 162.1 ± 6.5 | |
| IV | 1 (0.7) | 113.2 | 183.5 | |
| Tumor recurrence | Absent | 134 (89.3) | 105.2 ± 23.6 | 162.9 ± 18.7 |
| Present | 16 (10.7) | 102.3 ± 20.1 | 157.5 ± 24.3 | |
| Pathologic Features | ||||
| Subjacent UIS | Absent | 90 (60.0) | 109.3 ± 22.3 | 164.2 ± 19.2 |
| Present | 60 (40.0) | 98.4 ± 23.1 | 159.4 ± 9.3 | |
| Inflammation | None | 54 (36.0) | 107.4 ± 24.8 | 163.7 ± 19.4 |
| + | 41 (27.3) | 108.4 ± 19.8 | 167.4 ± 19.1 | |
| ++ | 33 (22.0) | 103.5 ± 25.2 | 160.6 ± 15.9 | |
| +++ | 22 (14.7) | 94.5 ± 19.6 | 151.9 ± 21.2 | |
| Tumor with SD | Absent | 107 (71.3) | 106.5 ± 22.6 | 163.5 ± 19.8 |
| Present | 43 (28.7) | 100.9 ± 24.5 | 159.3 ± 18.1 | |
| Tumor with GD | Absent | 137 (91.3) | 105.3 ± 23.7 | 162.9 ± 19.3 |
| Present | 13 (8.7) | 100.4 ± 17.4 | 155.3 ± 19.2 | |
| LVI or PNI | Absent | 128 (85.3) | 105.2 ± 23.2 | 161.6 ± 19.7 |
| Present | 22 (14.7) | 103.2 ± 23.7 | 166.3 ± 17.3 | |
2.2. Correlation of 5-MeC and DNMT1 Levels


| Variables | 5-MeC Level | |||
|---|---|---|---|---|
| Low | High | p-Value | ||
| Tumor location | Normal urothelia (n = 23) | 2 | 21 | |
| Pelvis (n = 27) | 15 | 12 | 0.0014 * | |
| Ureter (n = 65) | 43 | 22 | <0.0001 * | |
| Urinary bladder (n = 58) | 25 | 33 | 0.0069 * | |
| For 150 UC Tissue Samples | ||||
| DNMT1 level | Low (n = 129) | 76 (50.7%) | 53 (35.3%) | 0.0288 † |
| High (n = 21) | 7 (4.7%) | 14 (9.3%) | ||
2.3. Relationship among 5-Methylocytosine (5-MeC) Level, Clinicopathologic Features, and Urothelial Carcinomas (UC) Recurrence
| Variables | All Cases | Biomarkers with Low Level, n (%) | ||||
|---|---|---|---|---|---|---|
| 5-MeC | p-Value | DNMT1 | p-Value | |||
| Age | <68 | 73 | 43 (58.9) | 0.3917 | 64 (87.7) | 0.5657 |
| ≥68 | 77 | 40 (52.0) | 65 (84.4) | |||
| Sex | Male | 65 | 30 (46.2) | 0.0480 * | 54 (83.1) | 0.3669 |
| Female | 85 | 53 (62.4) | 75 (88.2) | |||
| Smoking † | Never | 66 | 35 (53.0) | 0.4072 | 55 (83.3) | 0.7124 |
| Ever | 36 | 16 (44.4) | 31 (86.1) | |||
| Tumor location | Pelvis | 27 | 15 (55.6) | 0.0371 * | 22 (81.5) | 0.1500 |
| Ureter | 65 | 43 (66.2) | 60 (92.3) | |||
| Urinary bladder | 58 | 25 (43.1) | 47 (81.0) | |||
| Tumor grade | Low grade | 34 | 18 (52.9) | 0.7500 | 30 (88.2) | 0.6690 |
| High grade | 116 | 65 (56.0) | 99 (85.3) | |||
| TNM stage | 0a/0is | 40 | 18 (45.0) | 0.0321 * | 33 (82.5) | 0.7250 |
| I | 42 | 20 (47.6) | 36 (85.7) | |||
| II/III/IV | 68 | 45 (66.2) | 60 (88.2) | |||
| Tumor recurrence | Absent | 134 | 75 (56.0) | 0.6493 | 115 (85.8) | 0.8548 |
| Present | 16 | 8 (50.0) | 14 (87.5) | |||
| Pathologic Features | ||||||
| UIS | Absent | 90 | 41 (45.6) | 0.0032 * | 74 (82.2) | 0.1024 |
| Present | 60 | 42 (70.0) | 55 (91.7) | |||
| Inflammation | None/+/++ | 128 | 65 (50.8) | 0.0068 * | 109 (85.2) | 0.7402 |
| +++ | 22 | 18 (81.8) | 20 (90.9) | |||
| SD | Absent | 107 | 56 (52.3) | 0.2442 | 88 (82.2) | 0.0365 * |
| Present | 43 | 27 (62.8) | 41 (95.4) | |||
| GD | Absent | 137 | 74 (54.0) | 0.2916 | 117 (85.4) | 0.6948 |
| Present | 13 | 9 (69.2) | 12 (92.3) | |||
| LVI or PNI | Absent | 128 | 71 (55.5) | 0.9359 | 110 (85.9) | 0.9576 |
| Present | 22 | 12 (54.6) | 19 (86.4) | |||
| Independent Variables | Dependent Variable: 5-MeC | Dependent Variable: DNMT1 | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |||
| Age (≥68 compared with <68) | 0.74 (0.39–1.43) | 0.3752 | 0.76 (0.30–1.93) | 0.5594 | ||
| Sex (Female compared with Male) | 1.95 (1.01–3.76) | 0.0476 * | 1.53 (0.61–3.87) | 0.3656 | ||
| Smoking (Ever compared with Never) | 1.32 (0.41–4.26) | 0.6416 | 2.98 (0.67–13.15) | 0.1499 | ||
| Tumor recurrence (Present compared with Absent) | 0.89 (0.31–2.58) | 0.8336 | 1.28 (0.27–6.21) | 0.7570 | ||
| Tumor Location | ||||||
| Pelvis compared with Urinary bladder | 1.46 (0.57–3.77) | 0.4302 | 2.82 (0.90–8.88) | 0.0762 | ||
| Ureter compared with Urinary bladder | 2.55 (1.20–5.44) | 0.0150 * | 0.95 (0.28–3.16) | 0.9264 | ||
| Tumor grade (High compared with Low) | 0.86 (0.42–1.76) | 0.6779 | 0.71 (0.25–2.02) | 0.5206 | ||
| TNM Stage | ||||||
| I compared with 0a/0is | 1.09 (0.45–2.63) | 0.8478 | 1.33 (0.40–4.40) | 0.6365 | ||
| II–IV compared with 0a/0is | 2.76 (1.20–6.35) | 0.0168 * | 1.65 (0.54–5.03) | 0.3806 | ||
| UIS (present compared with absent) | 2.76 (1.37–5.56) | 0.0045 * | 2.34 (0.80–6.79) | 0.1190 | ||
| Inflammation (+++ compared with None/+/++) | 4.96 (1.53–16.08) | 0.0076 * | 1.85 (0.39–8.81) | 0.4379 | ||
| SD (present compared with absent) | 1.38 (0.66–2.91) | 0.3917 | 4.23 (0.93–19.20) | 0.0620 | ||
| GD (present compared with absent) | 2.09 (0.59–7.35) | 0.2519 | 2.21 (0.27–18.31) | 0.4630 | ||
| LVI or PNI (present compared with absent) | 0.94 (0.37–2.36) | 0.8925 | 1.01 (0.27–3.79) | 0.9851 | ||
2.4. Discussion
3. Experimental Section
3.1. Ethics Statement
3.2. Clinical and Pathological Features
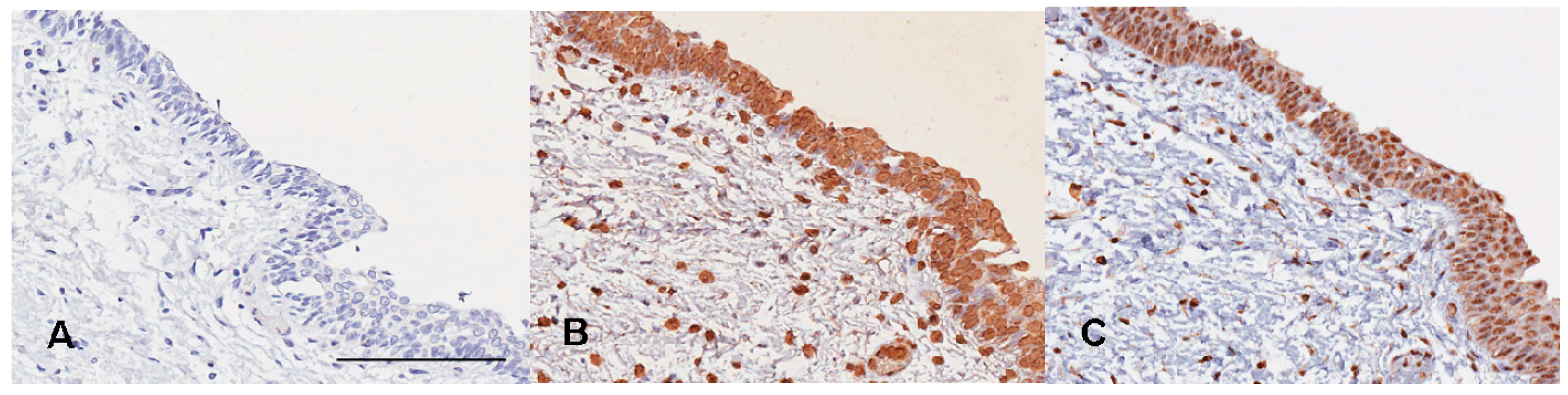
3.3. 5-MeC and DNA (Cytosine-5)-Methyltransferase 1 (DNMT1) Immunohistochemistry
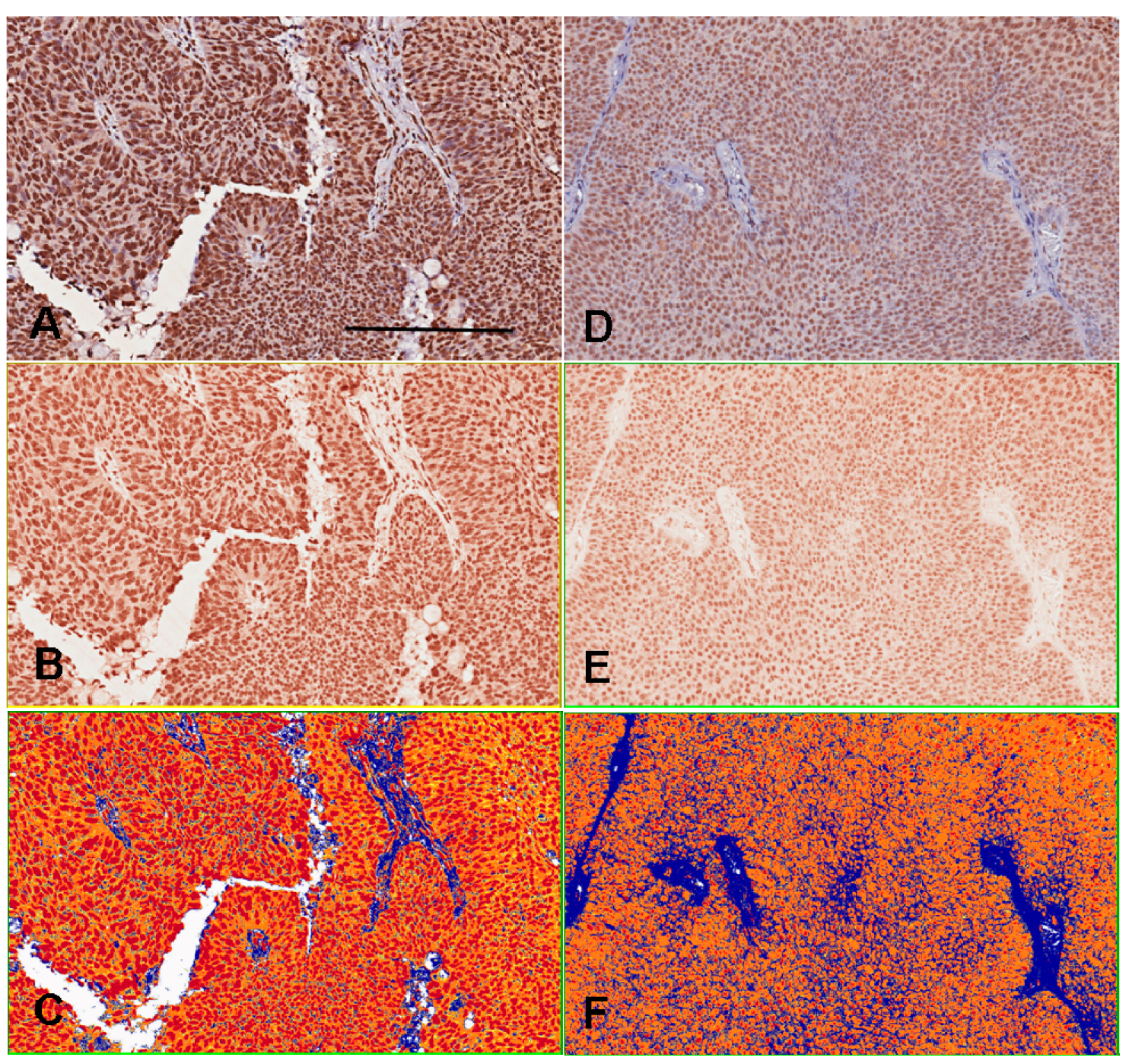
3.4. Assessments for 5-MeC and DNMT1 Immunoreactivities

3.5. Statistical Analysis
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Volanis, D.; Kadiyska, T.; Galanis, A.; Delakas, D.; Logotheti, S.; Zoumpourlis, V. Environmental factors and genetic susceptibility promote urinary bladder cancer. Toxicol. Lett. 2010, 193, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.D.; Uthus, E.O. DNA methylation, cancer susceptibility, and nutrient interactions. Exp. Biol. Med. 2004, 229, 988–995. [Google Scholar]
- Jones, P.A. DNA methylation errors and cancer. Cancer Res. 1996, 56, 2463–2467. [Google Scholar] [PubMed]
- Kanai, Y. Genome-wide DNA methylation profiles in precancerous conditions and cancers. Cancer Sci. 2010, 101, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Robertson, K.D. DNA methylation, methyltransferases, and cancer. Oncogene 2001, 20, 3139–3155. [Google Scholar] [CrossRef] [PubMed]
- Horikawa, Y.; Sugano, K.; Shigyo, M.; Yamamoto, H.; Nakazono, M.; Fujimoto, H.; Kanai, Y.; Hirohashi, S.; Kakizoe, T.; Habuchi, T.; et al. Hypermethylation of an E-cadherin (CDH1) promoter region in high grade transitional cell carcinoma of the bladder comprising carcinoma in situ. J. Urol. 2003, 169, 1541–1545. [Google Scholar]
- Maruyama, R.; Toyooka, S.; Toyooka, K.O.; Harada, K.; Virmani, A.K.; Zochbauer-Muller, S.; Farinas, A.J.; Vakar-Lopez, F.; Minna, J.D.; Sagalowsky, A.; et al. Aberrant promoter methylation profile of bladder cancer and its relationship to clinicopathological features. Cancer Res. 2001, 61, 8659–8663. [Google Scholar]
- Etoh, T.; Kanai, Y.; Ushijima, S.; Nakagawa, T.; Nakanishi, Y.; Sasako, M.; Kitano, S.; Hirohashi, S. Increased DNA methyltransferase 1 (DNMT1) protein expression correlates significantly with poorer tumor differentiation and frequent DNA hypermethylation of multiple CpG islands in gastric cancers. Am. J. Pathol. 2004, 164, 689–699. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, T.; Kanai, Y.; Ushijima, S.; Kitamura, T.; Kakizoe, T.; Hirohashi, S. DNA hypermethylation on multiple CpG islands associated with increased DNA methyltransferase DNMT1 protein expression during multistage urothelial carcinogenesis. J. Urol. 2005, 173, 1767–1771. [Google Scholar] [CrossRef] [PubMed]
- Compare, D.; Rocco, A.; Liguori, E.; D’Armiento, F.P.; Persico, G.; Masone, S.; Coppola-Bottazzi, E.; Suriani, R.; Romano, M.; Nardone, G. Global DNA hypomethylation is an early event in Helicobacter pylori-related gastric carcinogenesis. J. Clin. Pathol. 2011, 64, 677–682. [Google Scholar] [CrossRef] [PubMed]
- Eden, A.; Gaudet, F.; Waghmare, A.; Jaenisch, R. Chromosomal instability and tumors promoted by DNA hypomethylation. Science 2003, 300, 455. [Google Scholar] [CrossRef] [PubMed]
- Shen, R.; Tao, L.; Xu, Y.; Chang, S.; van Brocklyn, J.; Gao, J.X. Reversibility of aberrant global DNA and estrogen receptor-α gene methylation distinguishes colorectal precancer from cancer. Int. J. Clin. Exp. Pathol. 2009, 2, 21–33. [Google Scholar] [PubMed]
- Yang, B.; Sun, H.; Lin, W.; Hou, W.; Li, H.; Zhang, L.; Li, F.; Gu, Y.; Song, Y.; Li, Q.; Zhang, F. Evaluation of global DNA hypomethylation in human prostate cancer and prostatic intraepithelial neoplasm tissues by immunohistochemistry. Urol. Oncol. 2013, 31, 628–634. [Google Scholar] [CrossRef] [PubMed]
- Moore, L.E.; Pfeiffer, R.M.; Poscablo, C.; Real, F.X.; Kogevinas, M.; Silverman, D.; Garcia-Closas, R.; Chanock, S.; Tardon, A.; Serra, C.; et al. Genomic DNA hypomethylation as a biomarker for bladder cancer susceptibility in the Spanish bladder cancer study: A case-control study. Lancet Oncol. 2008, 9, 359–366. [Google Scholar]
- Minardi, D.; Lucarini, G.; Filosa, A.; Milanese, G.; Zizzi, A.; di Primio, R.; Montironi, R.; Muzzonigro, G. Prognostic role of global DNA-methylation and histone acetylation in pT1a clear cell renal carcinoma in partial nephrectomy specimens. J. Cell. Mol. Med. 2009, 13, 2115–2121. [Google Scholar] [CrossRef] [PubMed]
- Anisowicz, A.; Huang, H.; Braunschweiger, K.I.; Liu, Z.; Giese, H.; Wang, H.; Mamaev, S.; Olejnik, J.; Massion, P.P.; del Mastro, R.G. A high-throughput and sensitive method to measure global DNA methylation: Application in lung cancer. BMC Cancer 2008, 8, 222. [Google Scholar] [CrossRef] [PubMed]
- Barbisan, F.; Mazzucchelli, R.; Santinelli, A.; Stramazzotti, D.; Scarpelli, M.; Lopez-Beltran, A.; Cheng, L.; Montironi, R. Immunohistochemical evaluation of global DNA methylation and histone acetylation in papillary urothelial neoplasm of low malignant potential. Int. J. Immunopathol. Pharmacol. 2008, 21, 615–623. [Google Scholar] [PubMed]
- Berdasco, M.; Fraga, M.F.; Esteller, M. Quantification of global DNA methylation by capillary electrophoresis and mass spectrometry. Methods Mol. Biol. 2009, 507, 23–34. [Google Scholar]
- Nephew, K.P.; Balch, C.; Skalnik, D.G. Methyl group acceptance assay for the determination of global DNA methylation levels. Methods Mol. Biol. 2009, 507, 35–41. [Google Scholar] [PubMed]
- Hurst, C.D.; Platt, F.M.; Taylor, C.F.; Knowles, M.A. Novel tumor subgroups of urothelial carcinoma of the bladder defined by integrated genomic analysis. Clin. Cancer Res. 2012, 18, 5865–5877. [Google Scholar] [CrossRef] [PubMed]
- Goll, M.G.; Bestor, T.H. Eukaryotic cytosine methyltransferases. Annu. Rev. Biochem. 2005, 74, 481–514. [Google Scholar] [CrossRef] [PubMed]
- Kimura, F.; Seifert, H.H.; Florl, A.R.; Santourlidis, S.; Steinhoff, C.; Swiatkowski, S.; Mahotka, C.; Gerharz, C.D.; Schulz, W.A. Decrease of DNA methyltransferase 1 expression relative to cell proliferation in transitional cell carcinoma. Int. J. Cancer 2003, 104, 568–578. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.S.; Power, B.E.; Molloy, P.L. DNA hypomethylation and human diseases. Biochim. Biophys. Acta 2007, 1775, 138–162. [Google Scholar] [PubMed]
- Foran, E.; Garrity-Park, M.M.; Mureau, C.; Newell, J.; Smyrk, T.C.; Limburg, P.J.; Egan, L.J. Up-regulation of DNA methyltransferase-mediated gene silencing, anchorage-independent growth, and migration of colon cancer cells by interleukin-6. Mol. Cancer Res. 2010, 8, 471–481. [Google Scholar] [CrossRef] [PubMed]
- Nakano, K.; Boyle, D.L.; Firestein, G.S. Regulation of DNA methylation in rheumatoid arthritis synoviocytes. J. Immunol. 2013, 190, 1297–1303. [Google Scholar] [CrossRef] [PubMed]
- Weitzman, S.A.; Turk, P.W.; Milkowski, D.H.; Kozlowski, K. Free radical adducts induce alterations in DNA cytosine methylation. Proc. Natl. Acad. Sci. USA 1994, 91, 1261–1264. [Google Scholar] [CrossRef] [PubMed]
- Niculescu, M.D.; Zeisel, S.H. Diet, methyl donors and DNA methylation: interactions between dietary folate, methionine and choline. J. Nutr. 2002, 132, 2333S–2335S. [Google Scholar] [PubMed]
- Wang, T.C.; Song, Y.S.; Wang, H.; Zhang, J.; Yu, S.F.; Gu, Y.E.; Chen, T.; Wang, Y.; Shen, H.Q.; Jia, G. Oxidative DNA damage and global DNA hypomethylation are related to folate deficiency in chromate manufacturing workers. J. Hazard. Mater. 2012, 213–214, 440–446. [Google Scholar]
- Benard, A.; van de Velde, C.J.; Lessard, L.; Putter, H.; Takeshima, L.; Kuppen, P.J.; Hoon, D.S. Epigenetic status of LINE-1 predicts clinical outcome in early-stage rectal cancer. Br. J. Cancer 2013, 109, 3073–3083. [Google Scholar] [CrossRef] [PubMed]
- Van Bemmel, D.; Lenz, P.; Liao, L.M.; Baris, D.; Sternberg, L.R.; Warner, A.; Johnson, A.; Jones, M.; Kida, M.; Schwenn, M.; et al. Correlation of LINE-1 methylation levels in patient-matched buffy coat, serum, buccal cell, and bladder tumor tissue DNA samples. Cancer Epidemiol. Biomark. Prev. 2012, 21, 1143–1148. [Google Scholar]
- Seifert, H.H.; Schmiemann, V.; Mueller, M.; Kazimirek, M.; Onofre, F.; Neuhausen, A.; Florl, A.R.; Ackermann, R.; Boecking, A.; Schulz, W.A.; et al. In situ detection of global DNA hypomethylation in exfoliative urine cytology of patients with suspected bladder cancer. Exp. Mol. Pathol. 2007, 82, 292–297. [Google Scholar]
- Hernandez-Blazquez, F.J.; Habib, M.; Dumollard, J.M.; Barthelemy, C.; Benchaib, M.; de Capoa, A.; Niveleau, A. Evaluation of global DNA hypomethylation in human colon cancer tissues by immunohistochemistry and image analysis. Gut 2000, 47, 689–693. [Google Scholar] [CrossRef] [PubMed]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chung, C.-J.; Chang, C.-H.; Chuu, C.-P.; Yang, C.-R.; Chang, Y.-H.; Huang, C.-P.; Chen, W.-C.; Chung, M.-C.; Chang, H. Reduced 5-Methylcytosine Level as a Potential Progression Predictor in Patients with T1 or Non-Invasive Urothelial Carcinoma. Int. J. Mol. Sci. 2015, 16, 677-690. https://doi.org/10.3390/ijms16010677
Chung C-J, Chang C-H, Chuu C-P, Yang C-R, Chang Y-H, Huang C-P, Chen W-C, Chung M-C, Chang H. Reduced 5-Methylcytosine Level as a Potential Progression Predictor in Patients with T1 or Non-Invasive Urothelial Carcinoma. International Journal of Molecular Sciences. 2015; 16(1):677-690. https://doi.org/10.3390/ijms16010677
Chicago/Turabian StyleChung, Chi-Jung, Chao-Hsiang Chang, Chih-Pin Chuu, Chi-Rei Yang, Yi-Huei Chang, Chi-Ping Huang, Wen-Chi Chen, Mu-Chi Chung, and Han Chang. 2015. "Reduced 5-Methylcytosine Level as a Potential Progression Predictor in Patients with T1 or Non-Invasive Urothelial Carcinoma" International Journal of Molecular Sciences 16, no. 1: 677-690. https://doi.org/10.3390/ijms16010677