
The Association between Polymorphism of INSR and Polycystic Ovary Syndrome: A Meta-Analysis

Abstract
:1. Introduction
2. Results
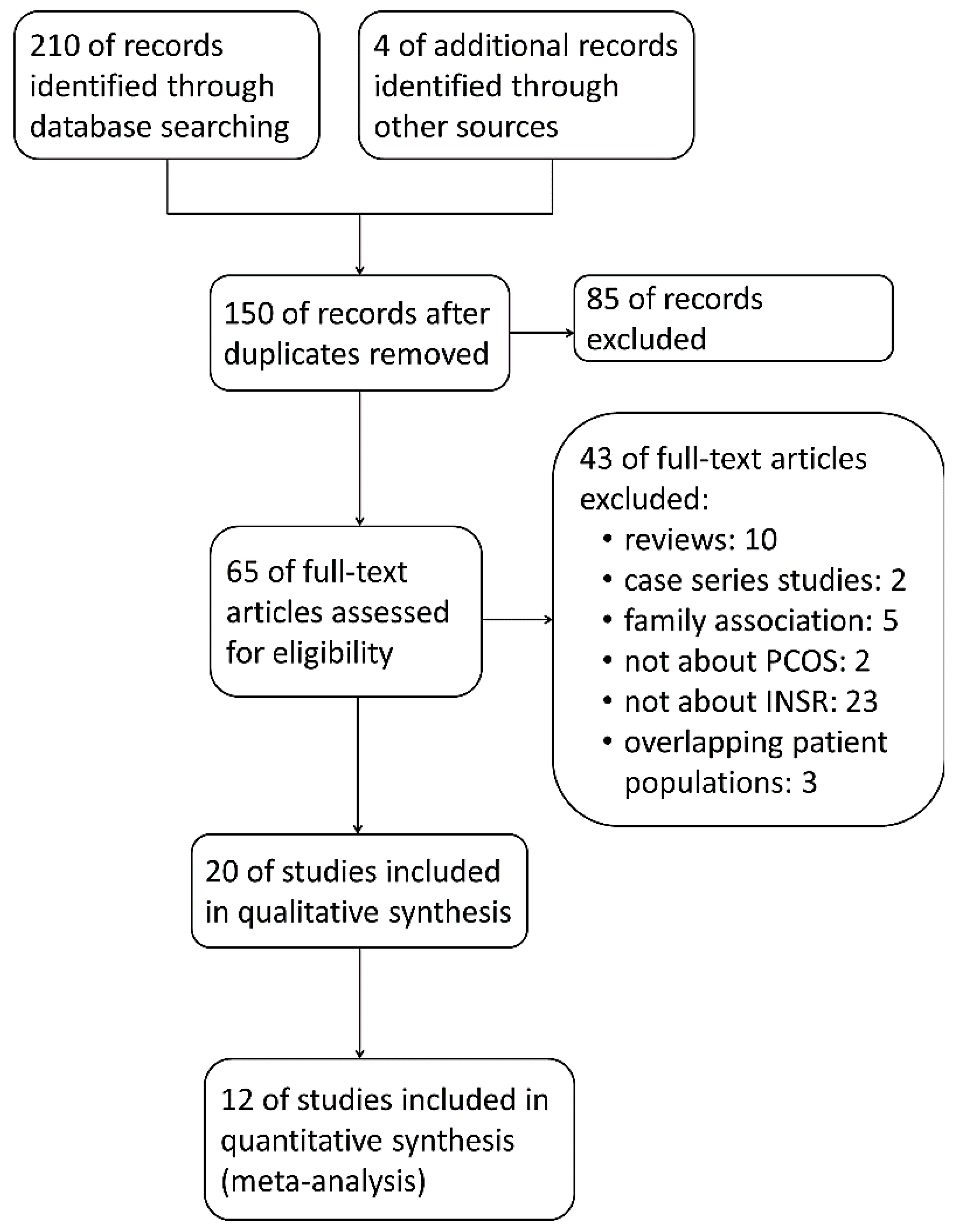
2.1. Selection of the Studies


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | Country | Ethnicity | Diagnosis Criteria | Number | Methodology | NOS Score | |
|---|---|---|---|---|---|---|---|---|
| Control | PCOS | |||||||
| Conway [26] | 1994 | UK | ND | ND | 8 | 22 | SSCP, sequencing | 6 |
| Talbot [27] | 1996 | UK | ND | Oligo/amenorrhea, hirsuitism, raised testosterone/androstenedione, polycystic ovaries | 5 | 24 | SSCP, sequencing | 6 |
| Siegel [12] | 2002 | USA | White | Oligomenorrhea, hyperandrogenism, polycystic ovaries | 136 | 99 | RFLP | 7 |
| Chen [28] | 2004 | China | Chinese | Oligo/amenorrhea, LH/FSH ≥ 2.5 or TT ≥ 1.56 nmol/L, polycystic ovaries, without endocrine disease or hypertension | 40 | 120 | RFLP | 8 |
| Jin [20] | 2006 | China | Chinese | Rotterdam criteria 2003 | 107 | 109 | SSCP, sequencing | 6 |
| Lee [29] | 2008 | Korea | Korean | Rotterdam criteria 2003 | 100 | 134 | sequencing | 7 |
| Mukherjee [30] | 2009 | India | Indian | Rotterdam criteria 2003 | 144 | 180 | sequencing | 7 |
| Unsal [13] | 2009 | Turkey | Caucasian | Rotterdam criteria 2003 | 50 | 44 | RFLP, sequencing | 8 |
| Hanzu [21] | 2010 | Romania | ND | Rotterdam criteria 2003 | 111 | 115 | sequencing | 7 |
| Goodarzi [22] | 2011 | USA | ND | Discover cohort: NIH criteria 1990; replication cohort: Rotterdam criteria 2003 | 3758 | 801 | Taqman assay, GWAS | 8 |
| Chen [15] | 2011 | China | Chinese | Rotterdam criteria 2003 | 6687 | 4082 | GWAS, LDR | 7 |
| Cirilo [31] | 2012 | Brazil | Brazian | Rotterdam criteria 2003 | 105 | 117 | RFLP | 6 |
| Ranjzad [32] | 2012 | Iran | ND | NIH criteria 1990 | 181 | 181 | RFLP, sequencing | 8 |
| Shi [16] | 2012 | China | Chinese | Rotterdam criteria 2003 | 9594 | 9736 | GWAS, LDR | 7 |
| Kashima [33] | 2013 | Japan | Japanese | Diagnostic criteria of the Japan Society of OBGY 2007 | 99 | 61 | Taqman assay | 7 |
| Skrgatic [34] | 2013 | Croatia | Crotian | Rotterdam criteria 2003 | 175 | 150 | Taqman assay | 5 |
| Ramezani [35] | 2013 | Iran | ND | NIH criteria | 156 | 186 | RFLP | 7 |
| Louwers [24] | 2013 | Netherlands | ND | Rotterdam criteria 2003 | 2164 | 703 | GWAS | 8 |
| Grigorescu [25] | 2013 | Romania | ND | ND | 177 | 500 | KASPar | 5 |
| Yin [23] | 2013 | China | Chinese | ND | 48 | 96 | ND | 5 |

| Study | SNP | Position | OR/RR (95% CI) | p Value |
|---|---|---|---|---|
| Conway [26] | rs1799817 | 7125286 | ND | ND |
| rs1799815 | 7125508 | ND | ND | |
| rs1799816 | 7125507 | ND | ND | |
| Talbot [27] | rs2860178 | 7170506 | ND | ND |
| rs2860177 | 7167940 | ND | ND | |
| rs2059806 | 7166365 | ND | ND | |
| rs2229429 | 7166377 | ND | ND | |
| rs41509747 | 7150480 | ND | ND | |
| rs2229431 | 7141764 | ND | ND | |
| rs41339753 | 7128812 | ND | ND | |
| rs1799815 | 7125508 | ND | ND | |
| rs1799817 | 7125286 | ND | ND | |
| Siegel [12] | rs1799817 * | 7125286 | RR: 2.1 in lean | 0.03 in lean, 0.32 in obese |
| Chen [28] | rs1799817 * | 7125286 | ND | <0.01 in total and lean, >0.05 in obese |
| Jin [20] | ND | 7125522 * | ND | <0.01 |
| Lee [29] | ND | 7184410 | ND | ND |
| rs6510959 | 7184227 | 1.39 (0.77–2.50) | 0.2726 | |
| rs2303672 | 7168394 | 0.82 (0.42–1.62) | 0.5707 | |
| rs2059806 | 7166365 | 1.31 (0.86–2.00) | 0.2134 | |
| rs2252673 | 7150407 | 0.90 (0.61–1.31) | 0.5688 | |
| rs2860175 | 7132070 | 1.46 (0.82–2.62) | 0.2010 | |
| rs1799817 | 7125286 | 0.83 (0.56–1.23) | 0.3541 | |
| ND | 7125064 | ND | ND | |
| rs78312382 * | 7117415 | 0.55 (0.32–0.96) | 0.0360 | |
| Mukherjee [30] | rs1799817 * | 7125286 | ND | 0.181 in total, 0.004 in lean |
| Unsal [13] | rs1799817 | 7125286 | ND | 0.437 |
| rs2229434 | 7142910 | ND | 1 | |
| rs2229430 | 7142832 | ND | 1 | |
| rs16994210 | 7142988 | ND | >0.05 | |
| rs35045353 | 7142927 | ND | >0.05 | |
| rs2162771 | 7142869 | ND | >0.05 | |
| rs1541806 | 7142844 | ND | >0.05 | |
| rs13306451 | 7142813 | ND | >0.05 | |
| Hanzu [21] | rs2245648 | 7163219 | ND | >0.05 |
| rs2962 | 7163054 | ND | >0.05 | |
| rs2245649 * | 7163203 | ND | 0.0086 | |
| rs2963 * | 7163143 | 2.99 (1.41–6.32) | 0.0025 | |
| rs2245655 * | 7163129 | ND | 0.0048 | |
| Goodarzi [22] | rs12459488 | 7206062 | 1.11 (0.92–1.34) | 0.3 |
| rs2971499 | 7214271 | 1.05 (0.86–1.28) | 0.067 | |
| rs2252673 * | 7150407 | 1.32 (1.08–1.60) | 0.006 | |
| rs10401628 | 7126207 | 1.00 (0.80–1.25) | 0.99 | |
| rs6510949 * | 7134391 | ND | 0.028 | |
| rs919275 | 7261430 | ND | 0.089 | |
| rs2042902 | 7204459 | ND | 0.099 | |
| rs4804404 | 7218371 | ND | 0.101 | |
| rs7254921 | 7278441 | ND | 0.111 | |
| rs7258382 | 7262558 | ND | 0.164 | |
| rs1549616 | 7132559 | ND | 0.166 | |
| rs7248939 | 7268427 | ND | 0.190 | |
| rs10408374 | 7127283 | ND | 0.249 | |
| rs8103483 | 7145363 | ND | 0.300 | |
| rs4804428 | 7235280 | ND | 0.360 | |
| rs3745550 | 7115562 | ND | 0.372 | |
| rs8112883 | 7179309 | ND | 0.404 | |
| rs10426094 | 7205229 | ND | 0.420 | |
| rs8110116 | 7143700 | ND | 0.511 | |
| rs2860172 | 7127364 | ND | 0.521 | |
| rs7245562 | 7218124 | ND | 0.522 | |
| rs890862 | 7233593 | ND | 0.536 | |
| rs10500204 | 7182952 | ND | 0.544 | |
| rs11668751 | 7251831 | ND | 0.586 | |
| rs3786680 | 7183540 | ND | 0.642 | |
| rs11667110 | 7136598 | ND | 0.644 | |
| rs6510960 | 7203721 | ND | 0.647 | |
| rs17254521 | 7238684 | ND | 0.689 | |
| rs4804195 | 7254933 | ND | 0.947 | |
| rs8111710 | 7292572 | ND | 0.962 | |
| rs12979424 | 7273481 | ND | 0.981 | |
| rs10408844 | 7244873 | ND | 0.992 | |
| rs11880337 | 7296441 | ND | ND | |
| rs6510975 | 7266867 | ND | ND | |
| rs2860183 | 7189364 | ND | ND | |
| Chen [15] | rs1864193 | 7114202 | 0.87 | 0.164 |
| rs11667110 | 7136598 | 0.92 | 0.343 | |
| rs16990074 | 7137340 | 1.14 | 0.494 | |
| rs4804304 | 7140514 | 1.18 | 0.387 | |
| rs2229431 | 7141764 | 1.03 | 0.832 | |
| rs2229430 | 7142832 | 1.09 | 0.672 | |
| rs2229434 | 7142910 | 1.05 | 0.814 | |
| rs2962 | 7163054 | 1.27 | 0.35 | |
| rs2059807 * | 7166098 | 1.34 | 3 × 10−4 | |
| rs3815902 * | 7166127 | 1.32 | 0.002 | |
| rs3786681 * | 7168922 | 1.34 | 9 × 10−4 | |
| rs6510956 * | 7169265 | 1.32 | 0.002 | |
| rs16994298 | 7170871 | 1.26 | 0.349 | |
| rs8109559 | 7171618 | 1.24 | 0.159 | |
| rs16994314 | 7176963 | 1.26 | 0.354 | |
| rs8108622 * | 7182742 | 1.5 | 7 × 10−5 | |
| rs10500204 * | 7182952 | 1.47 | 1 × 10−4 | |
| rs3786680 | 7183540 | 1.21 | 0.141 | |
| rs891088 * | 7184751 | 1.38 | 4 × 10−4 | |
| rs17253937 * | 7184790 | 1.43 | 0.001 | |
| rs7245757 | 7187617 | 0.94 | 0.476 | |
| rs1035939 | 7188968 | 0.93 | 0.337 | |
| rs4804368 | 7190279 | 0.96 | 0.602 | |
| rs7254358 | 7199330 | 0.91 | 0.204 | |
| rs1035942 | 7199792 | 0.93 | 0.354 | |
| rs8103883 | 7203411 | 1.24 | 0.075 | |
| rs2042901 | 7204383 | 0.91 | 0.241 | |
| rs10426094 * | 7205229 | 1.34 | 0.033 | |
| rs12459488 | 7206062 | 0.9 | 0.162 | |
| rs3745546 * | 7211805 | 1.25 | 0.036 | |
| rs3745545 | 7211830 | 1.07 | 0.584 | |
| rs7245562 | 7218124 | 0.93 | 0.364 | |
| rs7508679 | 7222821 | 0.99 | 0.879 | |
| rs4804415 | 7223808 | 1.05 | 0.636 | |
| rs4804416 | 7223837 | 0.97 | 0.677 | |
| rs7248104 | 7224420 | 0.97 | 0.643 | |
| rs4804424 | 7229666 | 1.06 | 0.553 | |
| rs10416429 | 7230427 | 1.03 | 0.758 | |
| rs890862 | 7233593 | 1.05 | 0.637 | |
| rs10424224 | 7240470 | 1.03 | 0.77 | |
| rs10404318 | 7247616 | 0.99 | 0.944 | |
| rs919275 | 7261430 | 1.09 | 0.283 | |
| rs8101064 | 7293108 | 1.15 | 0.273 | |
| Cirilo [31] | rs1799817 | 7125286 | ND | >0.05 |
| Ranjzad [32] | rs2059806 | 7166365 | ND | 0.519 |
| rs1799817 | 7125286 | ND | 0.630 | |
| Shi [16] | rs2059807 * | 7166098 | 1.14 | 1.09 × 10−8 |
| Kashima [33] | rs1799817 * | 7125286 | ND | 0.308 in total, 0.037 in lean, 0.644 in obese |
| Skrgatic [34] | rs1799817 | 7125286 | ND | 0.631 |
| Ramezani [35] | rs1799817 | 7125286 | ND | >0.05 |
| rs2059806 | 7166365 | ND | >0.05 | |
| Louwers [24] | rs2059807 | 7166098 | 0.93 | 0.27 |
| Grigorescu [25] | rs2059807 * | 7166098 | 3.1 (1.3–6.8) in non-insulin resistant | >0.05 in total, <0.006 in non-insulin resistant |
| Yin [23] | ND | 7125177 * | ND | 0.043 |
| ND | 7117386 * | ND | 0.055 in total, 0.042 in non-fat | |
| ND | 7117367 * | ND | 0.055 in total, 0.042 in non-fat |
2.2. Quality of the Included Studies
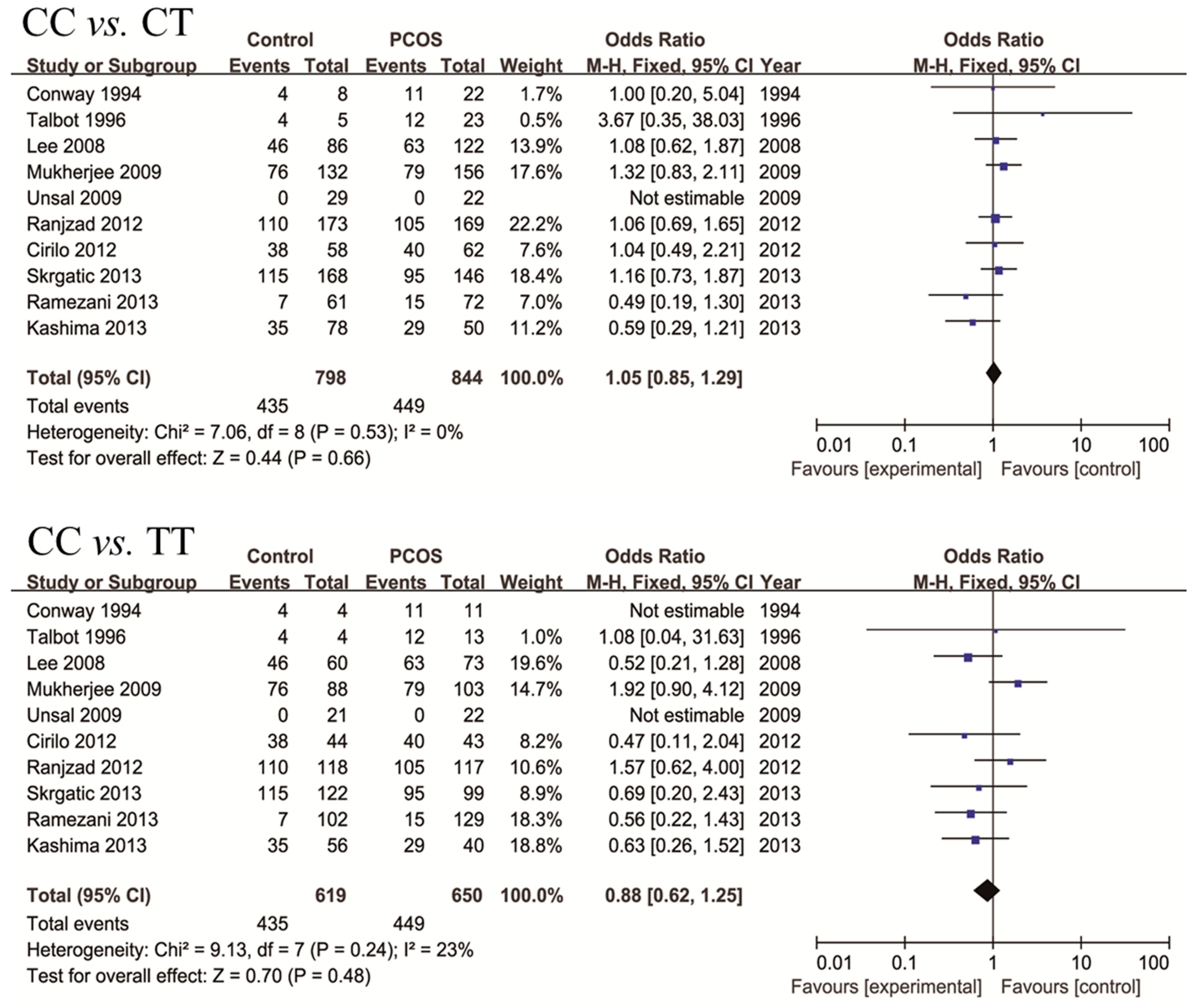
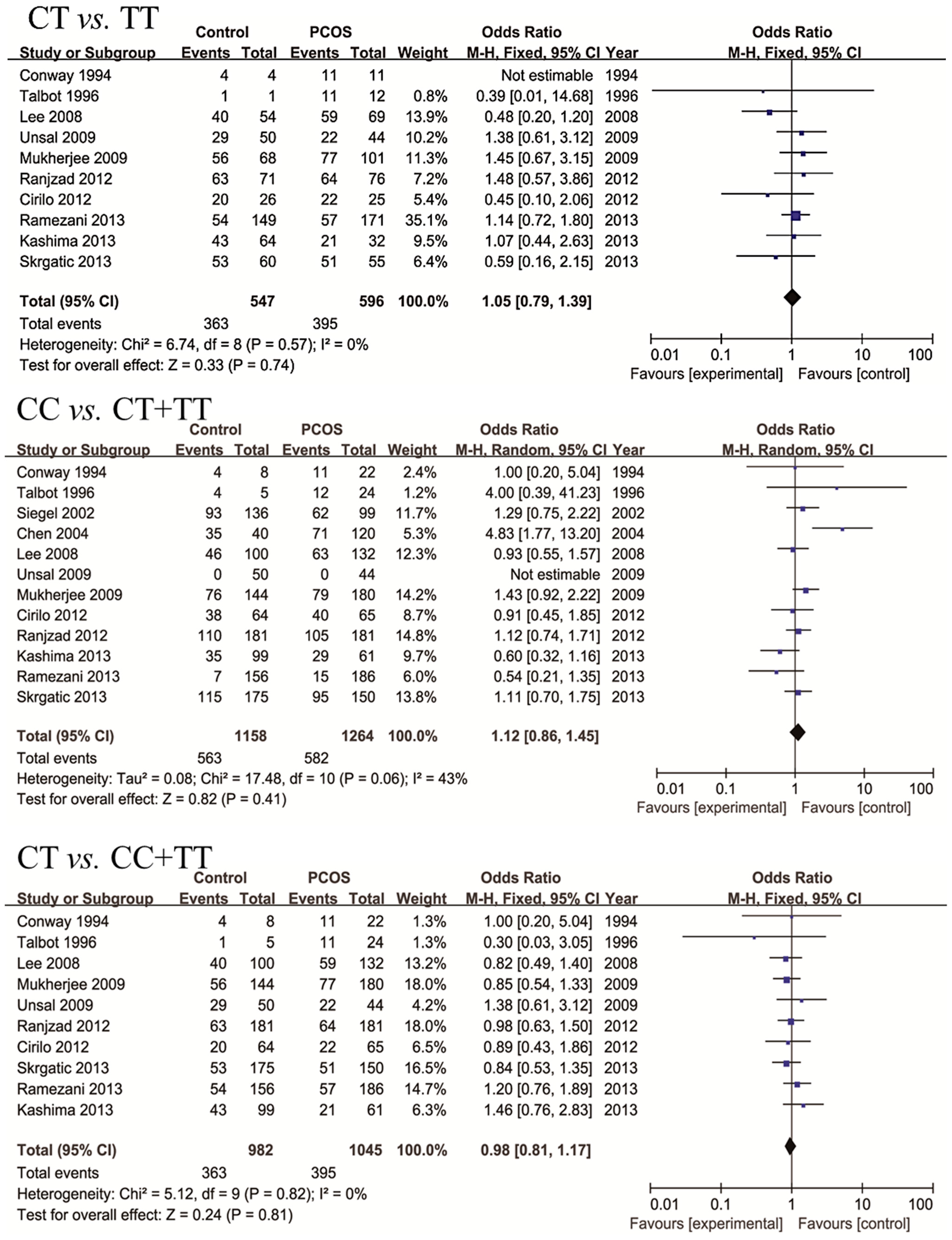
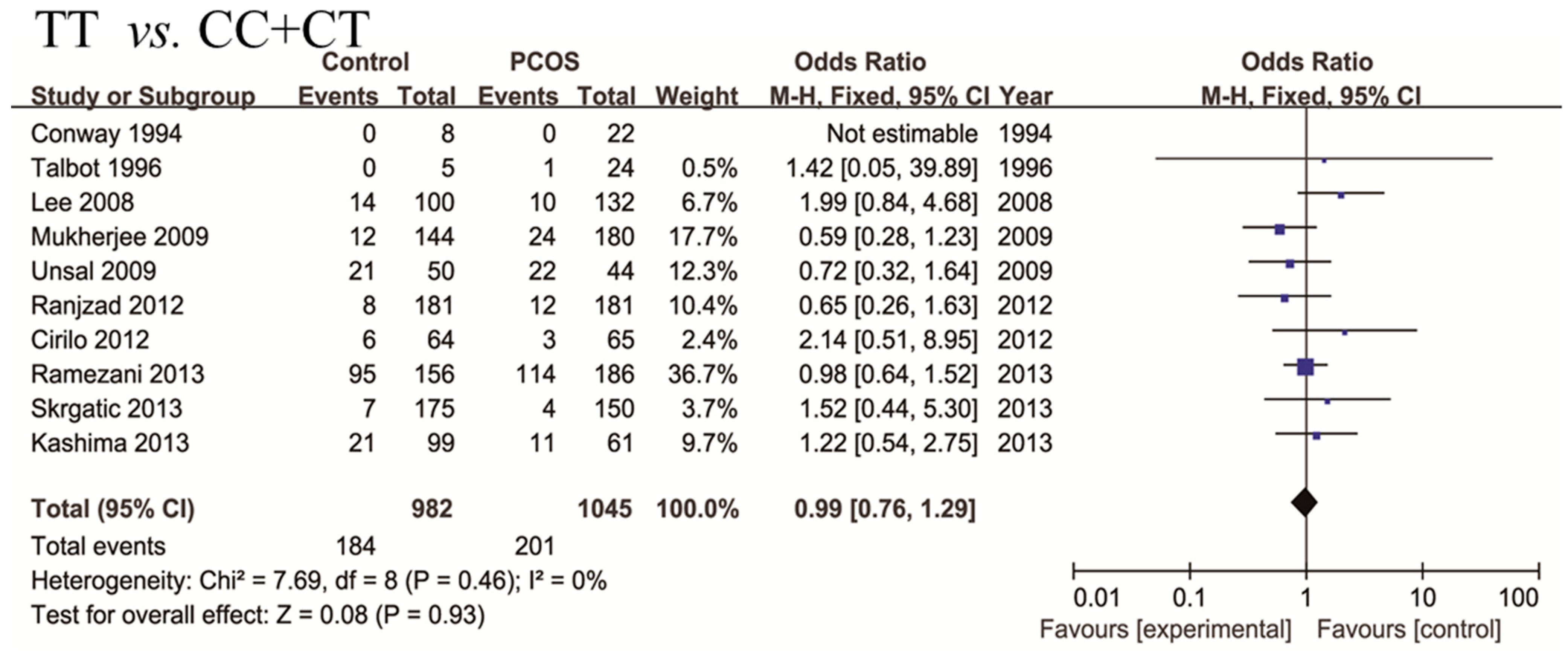
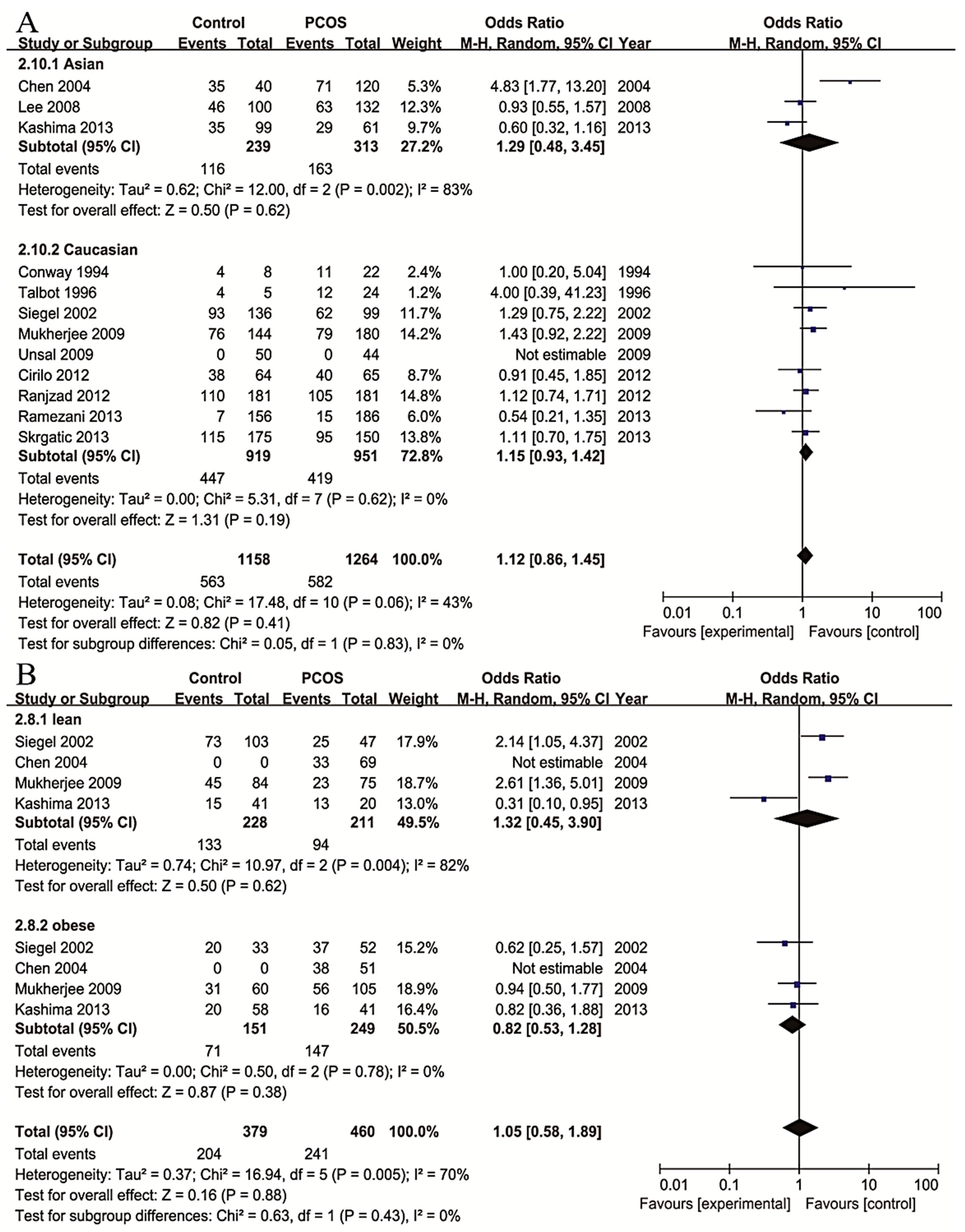
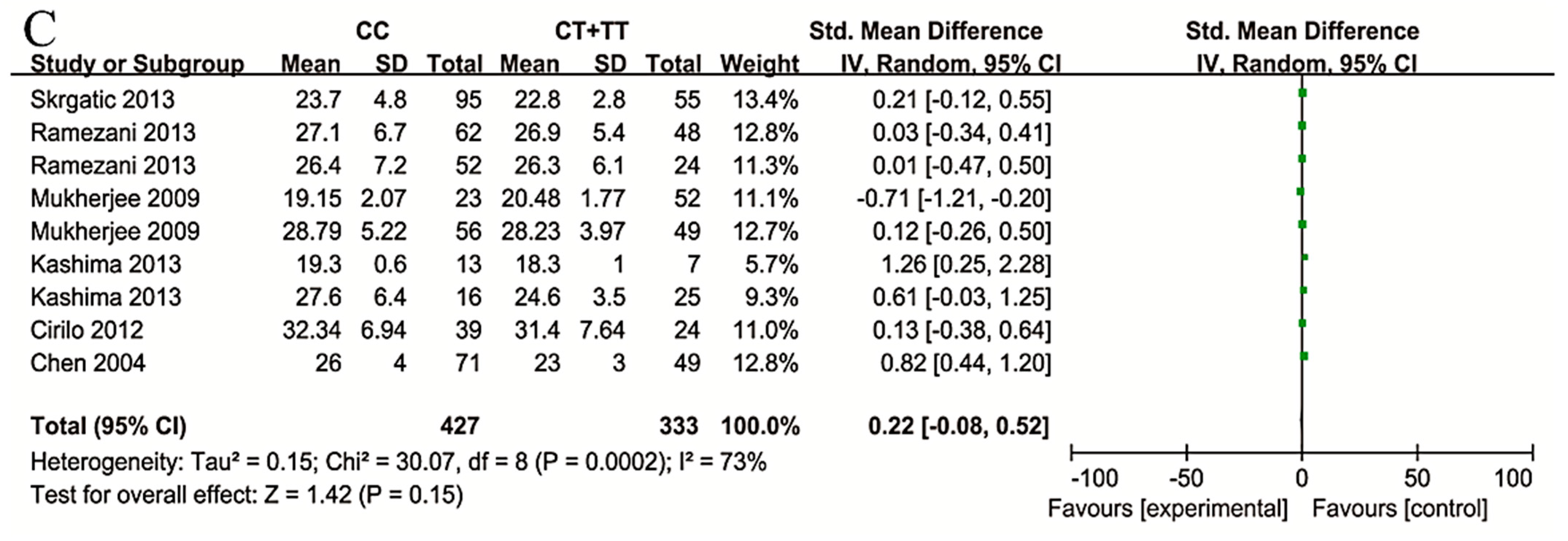
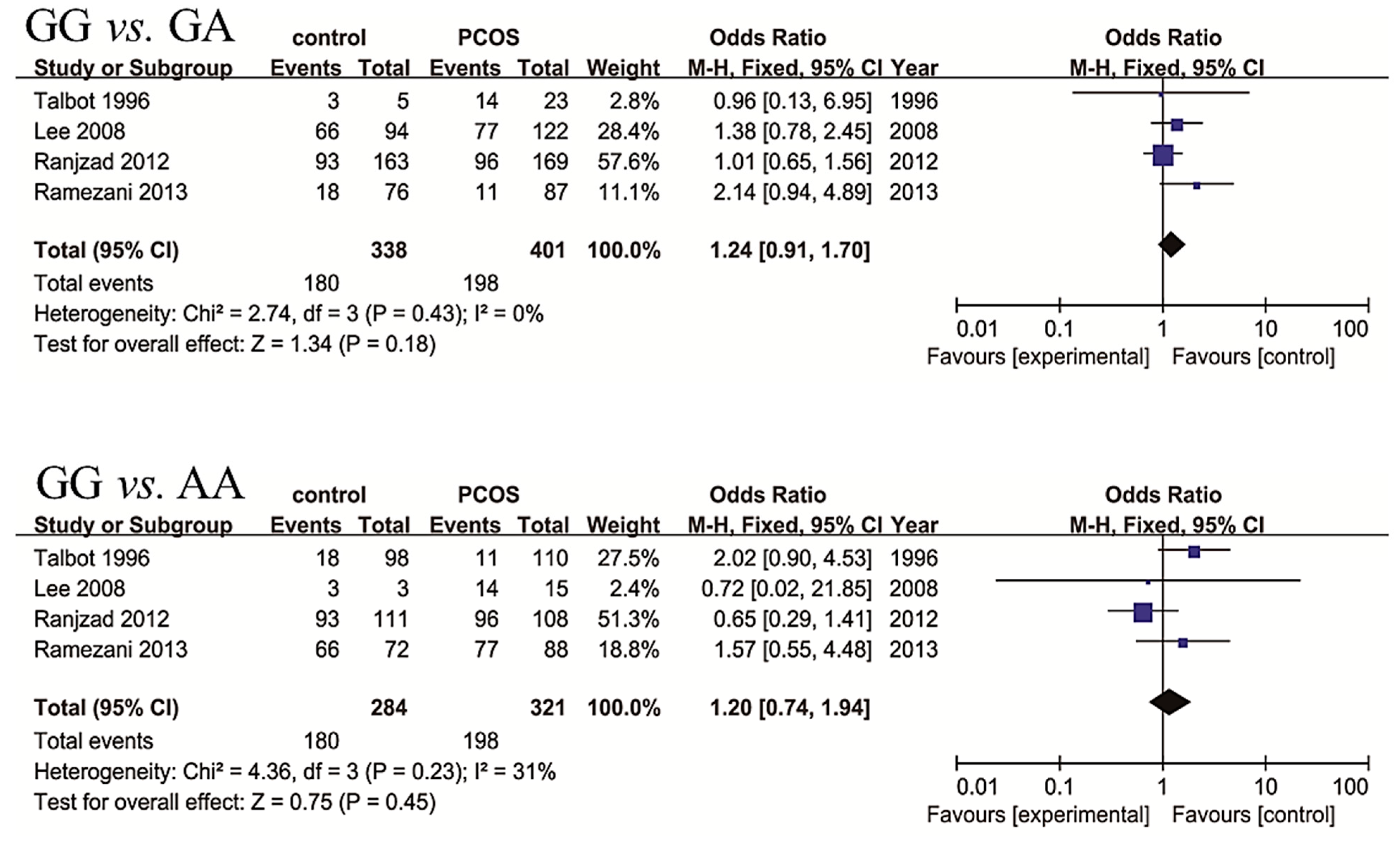
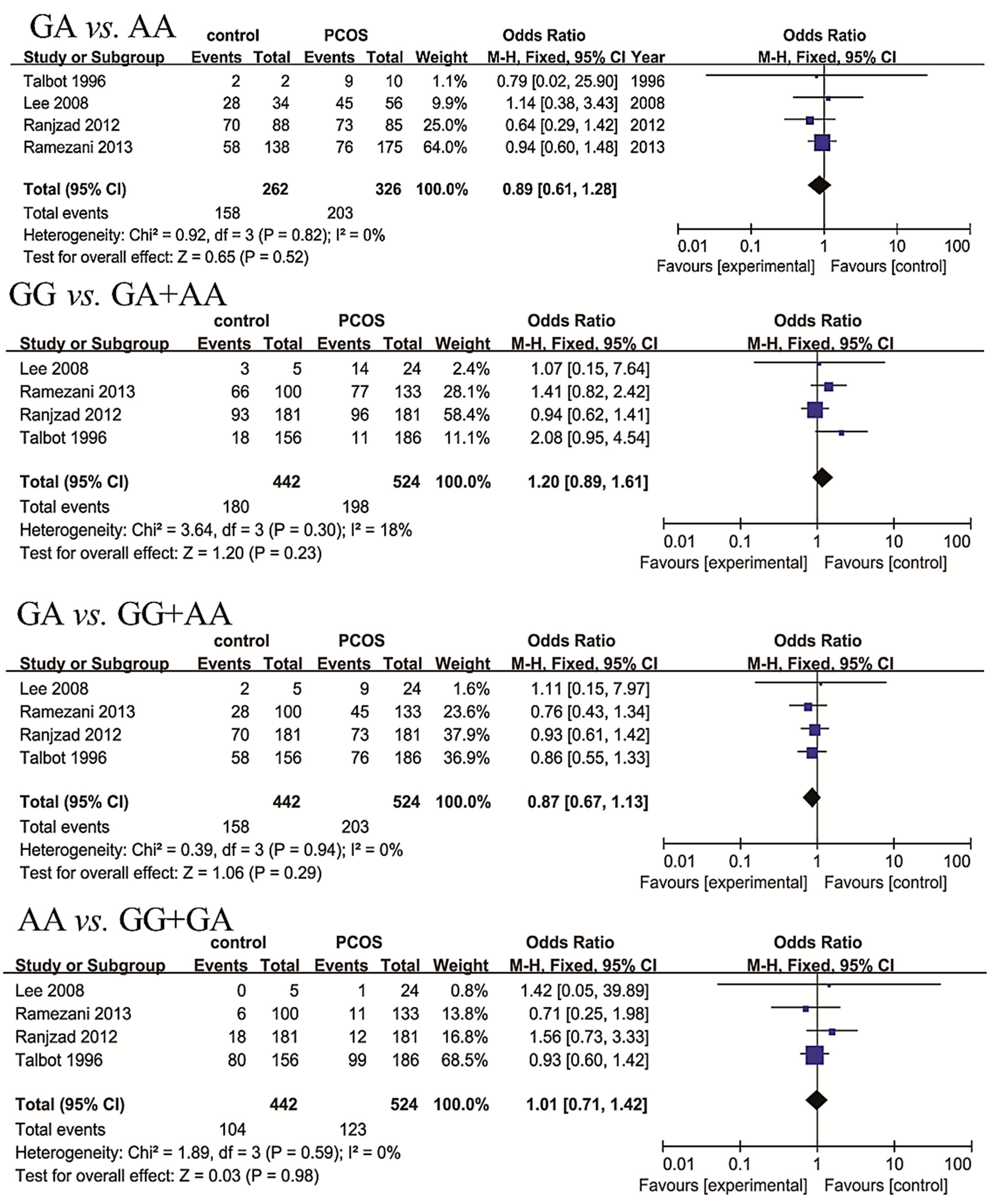
2.3. Meta-Analysis Results







| Study | Year | Country | Age | BMI | Control | PCOS Cases | p-Value of HWE | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Control | PCOS | Control | PCOS | Genotypes | Alleles | Cases | Genotypes | Alleles | Cases | ||||
| CC/CT/TT | C/T | CC/CT/TT | C/T | ||||||||||
| Conway [26] | 1994 | UK | ND | ND | 23.8 (21.0–24.7) | 32.1 (21.3–46.0) | 4/4/0 | 12/4 | 8 | 11/11/0 | 33/11 | 22 | 0.641 |
| Talbot [27] | 1996 | UK | 28 (25–33) | 24 (18–33) | 37.2 (30.5–45.8) | 36.6 (27.4–47) | 4/1/0 | 9/1 | 5 | 12/11/1 | 35/13 | 24 | 0.970 |
| Siegel [12] | 2002 | USA | age matched | 28 (16–52) | ND | ND | 93/43 | ND | 136 | 62/37 | ND | 99 | ND |
| Chen [28] | 2004 | China | 30 ± 4 | 29 ± 3 | 23 ± 3 | 25 ± 4 | 35/5 | ND | 40 | 71/49 | ND | 120 | ND |
| Lee [29] | 2008 | Korea | NDs | ND | 20.73 ± 2.36 | 23.22 ± 3.88 | 46/40/14 | 132/68 | 100 | 63/59/10 | 185/79 | 132 | 0.554 |
| Mukherjee [30] | 2009 | India | 24.94 ± 5.46 | 24.82 ± 5.26 | 22.16 ± 4.11 | 25.01 ± 5.63 | 76/56/12 | 208/80 | 144 | 79/77/24 | 235/125 | 180 | 0.934 |
| Unsal [13] | 2009 | Turkey | 14.0 ± 3.3 | 14.5 ± 1.3 | 20.7 ± 4.2 | 25.0 ± 5.5 | 0/29/21 | 29/71 | 50 | 0/22/22 | 22/66 | 44 | 0.015 * |
| Cirilo [31] | 2012 | Brazil | 32.53 ± 6.91 | 26.09 ± 6.90 | 25.61 ± 5.48 | 31.24 ± 7.15 | 38/20/6 | 96/32 | 64 | 40/22/3 | 102/28 | 65 | 0.411 |
| Ranjzad [32] | 2012 | Iran | 31.07 ± 5.84 | 27.13 ± 5.29 | 25.48 ± 4.21 | 26.80 ± 6.37 | 110/63/8 | 283/79 | 181 | 105/64/12 | 274/88 | 181 | 0.964 |
| Kashima [33] | 2013 | Japan | 34.6 ± 5.3 | 29.5 ± 3.7 | 20.8 ± 2.6 | 23.5 ± 5.2 | 35/43/21 | 113/85 | 99 | 29/21/11 | 79/43 | 61 | 0.528 |
| Skrgatic [34] | 2013 | Croatia | 29.1 ± 4.7 | 26.7 ± 5.9 | 22.4 ± 3.3 | 23.4 ± 4.2 | 115/53/7 | 283/67 | 175 | 95/51/4 | 241/59 | 150 | 0.960 |
| Ramezani [35] | 2013 | Iran | 30.8 ± 5.6 | 26.6 ± 5.6 | 25.5 ± 4.4 | 26.8 ± 6.4 | 7/54/95 | 68/244 | 156 | 15/57/114 | 87/285 | 186 | 0.982 |
| Study | Year | Country | Age | BMI | Control | PCOS | p-Value of HWE | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Control | PCOS | Control | PCOS | Genotypes | Alleles | Cases | Genotypes | Alleles | Cases | ||||
| GG/GA/AA | G/A | GG/GA/AA | G/A | ||||||||||
| Talbot [27] | 1996 | UK | 28 (25–33) | 24 (18–33) | 37.2 (30.5–45.8) | 36.6 (27.4–47) | 3/2/0 | 8/2 | 5 | 14/9/1 | 37/11 | 24 | 0.855 |
| Lee [29] | 2008 | Korean | ND | ND | 20.73 ± 2.36 | 23.22 ± 3.88 | 66/28/6 | 160/40 | 100 | 77/45/11 | 199/67 | 133 | 0.458 |
| Ranjzad [32] | 2012 | Iran | 31.07 ± 5.84 | 27.13 ± 5.29 | 25.48 ± 4.21 | 26.80 ± 6.37 | 93/70/18 | 256/106 | 181 | 96/73/12 | 265/97 | 181 | 0.673 |
| Ramezani [35] | 2013 | Iran | 30.8 ± 5.6 | 26.6 ± 5.6 | 25.5 ± 4.4 | 26.8 ± 6.4 | 18/58/80 | 94/218 | 156 | 11/76/99 | 98/274 | 186 | 0.344 |
| Study | Year | Country | Title of Cohort | Cases | Age | BMI | OR (95% CI) | p Value | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Control | PCOS | Control | PCOS | Control | PCOS | ||||||
| Chen [15] | 2011 | China | 895 | 744 | 30.68 ± 4.68 | 28.85 ± 3.62 | 22.68 ± 3.23 | 24.55 ± 3.99 | 1.34 (1.16–1.56) | 1.16 × 10−4 | |
| Shi [16] | 2012 | China | GWAS II | 2016 | 1510 | 53.95 ± 7.18 | 28.12 ± 2.75 | 24.93 ± 3.85 | 24.59 ± 3.17 | 1.19 (1.07–1.33) | 1.66 × 10−3 |
| REP I | 1913 | 1908 | 31.29 ± 5.00 | 28.01 ± 3.01 | 22.49 ± 2.17 | 24.23 ± 3.19 | 1.16 (1.05–1.28) | 4.40 × 10−3 | |||
| REP II | 5665 | 6318 | 29.52 ± 4.75 | 27.83 ± 3.11 | 21.95 ± 2.32 | 23.72 ± 3.18 | 1.09 (1.02–1.15) | 6.61 × 10−3 | |||
| Louwers [24] | 2013 | Dutch | 2164 | 703 | ND | 29.1 ± 5.73 | ND | 24.8 ± 5.6 | 0.93 | 0.27 | |
| Grigorescu [25] | 2013 | Romania | 177 | 500 | ND | ND | ND | 27.8 ± 0.35 | 3.1 (1.3-6.8) | <0.006 | |
2.4. Sensitivity Analysis
2.5. Publication Bias
3. Discussion
4. Experimental Section
4.1. Literature Retrieval
4.2. Data Extraction
4.3. Assessment of Study Quality
4.4. Statistical Analysis
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- The Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil. Steril. 2004, 81, 19–25. [Google Scholar]
- Moran, L.J.; Misso, M.L.; Wild, R.A.; Norman, R.J. Impaired glucose tolerance, type 2 diabetes and metabolic syndrome in polycystic ovary syndrome: A systematic review and meta-analysis. Hum. Reprod. Update 2010, 16, 347–363. [Google Scholar] [CrossRef] [PubMed]
- March, W.A.; Moore, V.M.; Willson, K.J.; Phillips, D.I.; Norman, R.J.; Davies, M.J. The prevalence of polycystic ovary syndrome in a community sample assessed under contrasting diagnostic criteria. Hum. Reprod. 2010, 25, 544–551. [Google Scholar] [CrossRef] [PubMed]
- Baptiste, C.G.; Battista, M.C.; Trottier, A.; Baillargeon, J.P. Insulin and hyperandrogenism in women with polycystic ovary syndrome. J. Steroid Biochem. Mol. Biol. 2010, 122, 42–52. [Google Scholar] [CrossRef]
- Gustin, S.; Lee, M.; Westphal, L. Differences in fertility and assisted reproduction in South Asian women. In Ethnic Differences in Fertility and Assisted Reproduction; Springer: New York, NY, USA, 2013; pp. 105–113. [Google Scholar]
- Vink, J.M.; Sadrzadeh, S.; Lambalk, C.B.; Boomsma, D.I. Heritability of polycystic ovary syndrome in a Dutch twin-family study. J. Clin. Endocrinol. MeTable 2006, 91, 2100–2104. [Google Scholar] [CrossRef]
- Diamanti-Kandarakis, E.; Papavassiliou, A.G. Molecular mechanisms of insulin resistance in polycystic ovary syndrome. Trends Mol. Med. 2006, 12, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Ben-Shlomo, I.; Younis, J.S. Basic research in PCOS: Are we reaching new frontiers. Reprod. Biomed. Online 2014, 28, 669–683. [Google Scholar] [CrossRef] [PubMed]
- Goodarzi, M.O.; Jones, M.R.; Li, X.; Chua, A.K.; Garcia, O.A.; Chen, Y.D.; Krauss, R.M.; Rotter, J.I.; Ankener, W.; Legro, R.S.; et al. Replication of association of DENND1A and THADA variants with polycystic ovary syndrome in European cohorts. J. Med. Genet. 2012, 49, 90–95. [Google Scholar] [CrossRef]
- Accili, D.; Drago, J.; Lee, E.J.; Johnson, M.D.; Cool, M.H.; Salvatore, P.; Asico, L.D.; Jose, P.A.; Taylor, S.I.; Westphal, H. Early neonatal death in mice homozygous for a null allele of the insulin receptor gene. Nat. Genet. 1996, 12, 106–109. [Google Scholar] [CrossRef] [PubMed]
- Chu, Y.L.; Gong, Y.D.; Su, Z.H.; Yu, H.N.; Cui, Q.; Jiang, H.Y.; Qu, H.M. Relationship between tyrosine phosphorylation and protein expression of insulin receptor and insulin resistance in gestational diabetes mellitus. J. Huazhong Univ. Sci. Technol. Med. Sci. 2014, 34, 393–397. [Google Scholar] [CrossRef] [PubMed]
- Siegel, S.; Futterweit, W.; Davies, T.F.; Concepcion, E.S.; Greenberg, D.A.; Villanueva, R.; Tomer, Y. A C/T single nucleotide polymorphism at the tyrosine kinase domain of the insulin receptor gene is associated with polycystic ovary syndrome. Fertil. Steril. 2002, 78, 1240–1243. [Google Scholar] [CrossRef] [PubMed]
- Unsal, T.; Konac, E.; Yesilkaya, E.; Yilmaz, A.; Bideci, A.; Ilke, O.H.; Cinaz, P.; Menevse, A. Genetic polymorphisms of FSHR, CYP17, CYP1A1, CAPN10, INSR, SERPINE1 genes in adolescent girls with polycystic ovary syndrome. J. Assist. Reprod. Genet. 2009, 26, 205–216. [Google Scholar] [CrossRef] [PubMed]
- Ioannidis, A.; Ikonomi, E.; Dimou, N.L.; Douma, L.; Bagos, P.G. Polymorphisms of the insulin receptor and the insulin receptor substrates genes in polycystic ovary syndrome: A Mendelian randomization meta-analysis. Mol. Genet. Metable 2010, 99, 174–183. [Google Scholar] [CrossRef]
- Chen, Z.J.; Zhao, H.; He, L.; Shi, Y.; Qin, Y.; Shi, Y.; Li, Z.; You, L.; Zhao, J.; Liu, J.; et al. Genome-wide association study identifies susceptibility loci for polycystic ovary syndrome on chromosome 2p16.3, 2p21 and 9q33.3. Nat. Genet. 2011, 43, 55–59. [Google Scholar] [CrossRef]
- Shi, Y.; Zhao, H.; Shi, Y.; Cao, Y.; Yang, D.; Li, Z.; Zhang, B.; Liang, X.; Li, T.; Chen, J.; et al. Genome-wide association study identifies eight new risk loci for polycystic ovary syndrome. Nat. Genet. 2012, 44, 1020–1025. [Google Scholar] [CrossRef]
- Jin, L. Polymorphism in insulin receptor gene exon 17 in women with polycystic ovary syndrome. Zhonghua Fu Chan Ke Za Zhi 2005, 40, 323–326. (in Chinese). [Google Scholar] [PubMed]
- Lee, E.J.; Yoo, K.J.; Kim, S.J.; Lee, S.H.; Cha, K.Y.; Baek, K.H. Single nucleotide polymorphism in exon 17 of the insulin receptor gene is not associated with polycystic ovary syndrome in a Korean population. Fertil. Steril. 2006, 86, 380–384. [Google Scholar] [CrossRef] [PubMed]
- Louwers, Y.V. Insulin receptor gene polymorphisms are associated with polycystic ovary syndrome (PCOS). Hum. Reprod. 2010, 25. [Google Scholar] [CrossRef]
- Jin, L.; Zhu, X.M.; Luo, Q.; Qian, Y.; Jin, F.; Huang, H.F. A novel SNP at exon 17 of INSR is associated with decreased insulin sensitivity in Chinese women with PCOS. Mol. Hum. Reprod. 2006, 12, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Hanzu, F.A.; Radian, S.; Attaoua, R.; Ait-El-Mkadem, S.; Fica, S.; Gheorghiu, M.; Coculescu, M.; Grigorescu, F. Association of insulin receptor genetic variants with polycystic ovary syndrome in a population of women from Central Europe. Fertil. Steril. 2010, 94, 2389–2392. [Google Scholar] [CrossRef] [PubMed]
- Goodarzi, M.O.; Louwers, Y.V.; Taylor, K.D.; Jones, M.R.; Cui, J.; Kwon, S.; Chen, Y.D.; Guo, X.; Stolk, L.; Uitterlinden, A.G.; et al. Replication of association of a novel insulin receptor gene polymorphism with polycystic ovary syndrome. Fertil. Steril. 2011, 95, 1736–1741. [Google Scholar] [CrossRef]
- Yin, C. Natural Cycle IVF and Mild Stimulation. J. Assist. Reprod. Genet. 2013, 30, 172–173. [Google Scholar]
- Louwers, Y.V.; Stolk, L.; Uitterlinden, A.G.; Laven, J.S. Cross-ethnic meta-analysis of genetic variants for polycystic ovary syndrome. J. Clin. Endocrinol. Metable 2013, 98, E2006–E2012. [Google Scholar] [CrossRef]
- Grigorescu, F. Sub-classification of polycystic ovary syndrome by rotterdam criteria reveals stronger association of the insulin receptor (INSR) and FTO genes in central European population. Diabetes 2013, 62, A716–A717. [Google Scholar]
- Conway, G.S.; Avey, C.; Rumsby, G. The tyrosine kinase domain of the insulin receptor gene is normal in women with hyperinsulinaemia and polycystic ovary syndrome. Hum. Reprod. 1994, 9, 1681–1683. [Google Scholar] [PubMed]
- Talbot, J.A.; Bicknell, E.J.; Rajkhowa, M.; Krook, A.; OʼRahilly, S.; Clayton, R.N. Molecular scanning of the insulin receptor gene in women with polycystic ovarian syndrome. J. Clin. Endocrinol. MeTable 1996, 81, 1979–1983. [Google Scholar]
- Chen, Z.J.; Shi, Y.H.; Zhao, Y.R.; Li, Y.; Tang, R.; Zhao, L.X.; Chang, Z.H. Correlation between single nucleotide polymorphism of insulin receptor gene with polycystic ovary syndrome. Zhonghua Fu Chan Ke Za Zhi 2004, 39, 582–585. [Google Scholar]
- Lee, E.J.; Oh, B.; Lee, J.Y.; Kimm, K.; Lee, S.H.; Baek, K.H. A novel single nucleotide polymorphism of INSR gene for polycystic ovary syndrome. Fertil. Steril. 2008, 89, 1213–1220. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, S.; Shaikh, N.; Khavale, S.; Shinde, G.; Meherji, P.; Shah, N.; Maitra, A. Genetic variation in exon 17 of INSR is associated with insulin resistance and hyperandrogenemia among lean Indian women with polycystic ovary syndrome. Eur. J. Endocrinol. 2009, 160, 855–862. [Google Scholar] [CrossRef] [PubMed]
- Ramos, C.P.D.; Rosa, F.E.; Moreira, F.M.F.; Rainho, C.A.; Pontes, A.; Rogatto, S.R. Genetic polymorphisms associated with steroids metabolism and insulin action in polycystic ovary syndrome. Gynecol. Endocrinol. 2012, 28, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Ranjzad, F.; Mahmoudi, T.; Irani, S.A.; Mahban, A.; Nikzamir, A.; Vahedi, M.; Ashrafi, M.; Gourabi, H. A common variant in the adiponectin gene and polycystic ovary syndrome risk. Mol. Biol. Rep. 2012, 39, 2313–2319. [Google Scholar] [CrossRef] [PubMed]
- Kashima, K.; Yahata, T.; Fujita, K.; Tanaka, K. Polycystic ovary syndrome: Association of a C/T single nucleotide polymorphism at tyrosine kinase domain of insulin receptor gene with pathogenesis among lean Japanese women. J. Reprod. Med. 2013, 58, 491–496. [Google Scholar] [PubMed]
- Skrgatic, L.; Baldani, D.P.; Gersak, K.; Cerne, J.Z.; Ferk, P.; Coric, M. Genetic polymorphisms of INS, INSR and IRS-1 genes are not associated with polycystic ovary syndrome in Croatian women. Coll. Antropol. 2013, 37, 141–146. [Google Scholar] [PubMed]
- Ramezani, T.F.; Daneshpour, M.; Hashemi, S.; Zarkesh, M.; Azizi, F. Relationship between polymorphism of insulin receptor gene, and adiponectin gene with PCOS. Iran. J. Reprod. Med. 2013, 11, 185–194. [Google Scholar] [PubMed]
- Seino, S.; Seino, M.; Nishi, S.; Bell, G.I. Structure of the human insulin receptor gene and characterization of its promoter. Proc. Natl. Acad. Sci. USA 1989, 86, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Moller, D.E.; Yokota, A.; White, M.F.; Pazianos, A.G.; Flier, J.S. A naturally occurring mutation sof insulin receptor alanine 1134 impairs tyrosine kinase function and is associated with dominantly inherited insulin resistance. J. Biol. Chem. 1990, 265, 14979–14985. [Google Scholar] [PubMed]
- Ioannidis, J.P.; Ntzani, E.E.; Trikalinos, T.A. “Racial” differences in genetic effects for complex diseases. Nat. Genet. 2004, 36, 1312–1318. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; OʼConnell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 1 July 2014).
- Lau, J.; Ioannidis, J.P.; Schmid, C.H. Quantitative synthesis in systematic reviews. Ann. Intern. Med. 1997, 127, 820–826. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feng, C.; Lv, P.-P.; Yu, T.-T.; Jin, M.; Shen, J.-M.; Wang, X.; Zhou, F.; Jiang, S.-W. The Association between Polymorphism of INSR and Polycystic Ovary Syndrome: A Meta-Analysis. Int. J. Mol. Sci. 2015, 16, 2403-2425. https://doi.org/10.3390/ijms16022403
Feng C, Lv P-P, Yu T-T, Jin M, Shen J-M, Wang X, Zhou F, Jiang S-W. The Association between Polymorphism of INSR and Polycystic Ovary Syndrome: A Meta-Analysis. International Journal of Molecular Sciences. 2015; 16(2):2403-2425. https://doi.org/10.3390/ijms16022403
Chicago/Turabian StyleFeng, Chun, Ping-Ping Lv, Tian-Tian Yu, Min Jin, Jin-Ming Shen, Xue Wang, Feng Zhou, and Shi-Wen Jiang. 2015. "The Association between Polymorphism of INSR and Polycystic Ovary Syndrome: A Meta-Analysis" International Journal of Molecular Sciences 16, no. 2: 2403-2425. https://doi.org/10.3390/ijms16022403