
Impact of Soluble HLA-G Levels and Endometrial NK Cells in Uterine Flushing Samples from Primary and Secondary Unexplained Infertile Women

Abstract
:1. Introduction
2. Results

{kind=link}
{kind=link}
| Items | Primary Infertility | Secondary Infertility | p Value |
|---|---|---|---|
| Age | 34.7 ± 3.5 | 35.6 ± 3.4 | 0.53 * |
| Duration of Infertility (years) | 2.7 ± 2.0 | 3.1 ± 2.3 | 0.61 * |
| Length of menstrual cycle (days) | 29.0 ± 4.0 | 28.2 ± 3.3 | 0.58 * |
| FSH (mUI/mL) day 3 of the menstrual cycle | 7.6 ± 2.7 | 6.9 ± 2.9 | 0.59 * |
| LH (mUI/mL) day 3 of the menstrual cycle | 6.9 ± 3.4 | 5.0 ± 2.2 | 0.13 * |
| Estradiol (pg/mL) day 3 of the menstrual cycle | 73.8 ± 65.5 | 54.9 ± 42.8 | 0.43 * |
| TSH (µUI/mL) | 3.8 ± 4.1 | 2.1 ± 1.4 | 0.0041 * |
| FT4 (pg/mL) | 2.8 ± 3.9 | 2.2 ± 3.0 | 0.45 |
| Progesterone (pg/mL) day 21 of the menstrual cycle | 13.7 ± 9.6 | 12.4 ± 2.7 | 0.76 * |
| Smoke habits (percentage) | 22.7% | 11.1% | 0.074 ** |
| Day (menstrual cycle) of sample collection | 8.9 ± 1.9 | 9.1 ± 1.8 | 0.84 * |
| Items | Primary Infertility | Secondary Infertility | p Value |
|---|---|---|---|
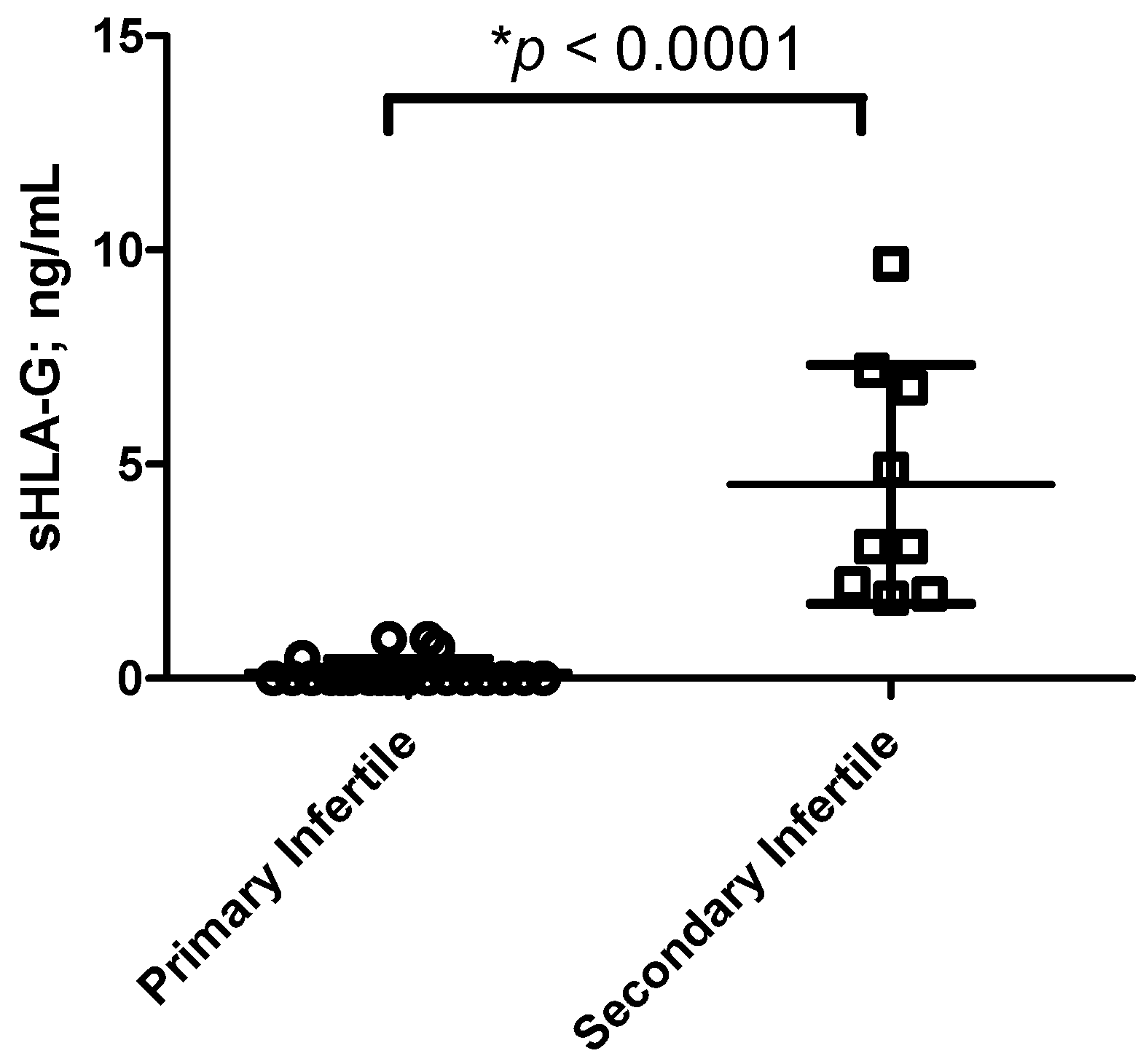
| NK cells N (%) | 84.1 ± 42.1 (21) | 212.1 ± 48.5 (21) | <0.0001 * |
| CD56+CD16− KIR2DL4+ N (%) | 80.1 ± 20.3 (8.4) | 200.0 ± 40.1 (20) | <0.0001 * |
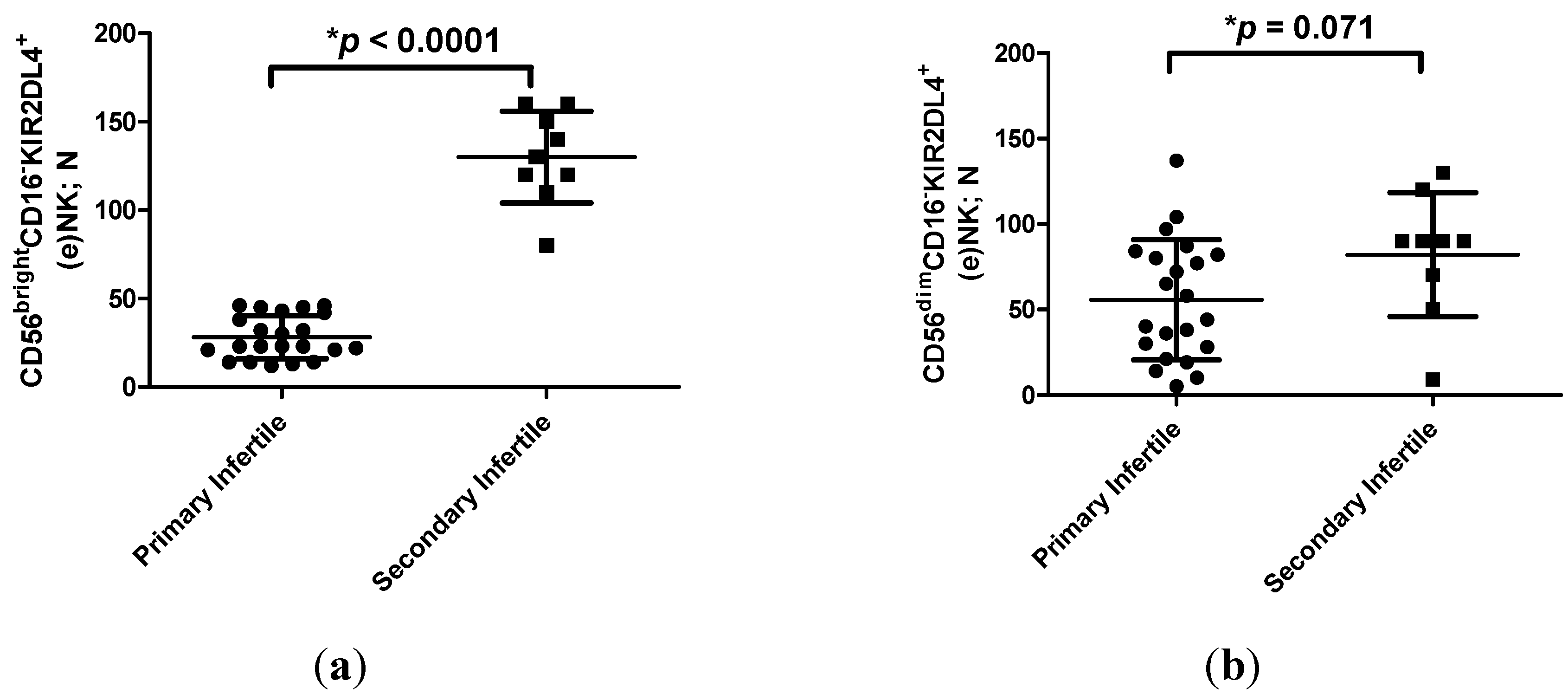
| CD56brightCD16−KIR2DL4+ N (%) | 28.3 ± 12.1 (2.8) | 118.8 ± 2.3 (12) | <0.0001 * |
| CD56dimCD16−KIR2DL4+ N (%) | 55.8 ± 35.2 (5.6) | 82.1 ± 36.2 (8.2) | 0.071 * |
| CD3+ N (%) | 0 | 0 | NA * |
| CD14+ N (%) | 3.4 ± 7.9 (0.3) | 2.4 ± 4.9 (0.2) | 0.74 * |


3. Discussion
4. Experimental Section
4.1. Patient Recruitment
4.2. Samples Collection
4.3. sHLA-G Analysis by ELISA
4.4. (e)NK Cell Analysis by Flow Cytometry
4.5. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Moffett-King, A. Natural killer cells and pregnancy. Nat. Rev. Immunol. 2002, 2, 656–663. [Google Scholar] [CrossRef] [PubMed]
- Geiselhart, A.; Dietl, J.; Marzusch, K.; Ruck, P.; Ruck, M.; Horny, H.P.; Kaiserling, E.; Handgretinger, R. Comparative analysis of the immunophenotypes of decidual and peripheral blood large granular lynphocytes and T cells during early human pregnancy. Am. J. Reprod. Immunol. 1995, 33, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Gonen-Gross, T.; Goldman-Wohl, D.; Huppertz, B.; Lankry, D.; Greenfield, C.; Natanson-Yaron, S.; Hamani, Y.; Gilad, R.; Yagel, S.; Mandelboim, O. Inhibitory NK receptor recognition of HLA-G: Regulation by contact residues and by cell specific expression at the fetal-maternal interface. PLoS One 2010, 5, e8941. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, R.; Bortolotti, D.; Baricordi, O.R.; Fainardi, E. New insights into HLA-G and inflammatory diseases. Inflamm. Allergy Drug Target 2012, 11, 448–463. [Google Scholar] [CrossRef]
- Rizzo, R.; Stignani, M.; Melchiorri, L.; Baricordi, O.R. Possible role of human leukocyte antigen-G molecules in human oocyte/embryo secretome. Hum. Immunol. 2009, 70, 970–975. [Google Scholar] [CrossRef] [PubMed]
- Dahl, M.; Perin, T.L.; Djurisic, S.; Rasmussen, M.; Ohlsson, J.; Buus, S.; Lindhard, A.; Hviid, T.V. Soluble human leukocyte antigen-G in seminal plasma is associated with HLA-G genotype: Possible implications for fertility success. Am. J. Reprod. Immunol. 2014, 72, 89–105. [Google Scholar] [CrossRef] [PubMed]
- Emmer, P.M.; Steegers, E.A.; Kerstens, H.M.; Bulten, J.; Nelen, W.L.; Boer, K.; Joosten, I. Altered phenotype of HLA-G expressing trophoblast and decidual natural killer cells in pathological pregnancies. Hum. Reprod. 2002, 17, 1072–1080. [Google Scholar] [CrossRef] [PubMed]
- Kotze, D.; Kruger, T.F.; Lombard, C.; Padayachee, T.; Keskintepe, L.; Sher, G. The effect of the biochemical marker soluble human leukocyte antigen G on pregnancy outcome in assisted reproductive technology—A multicenter study. Fertil. Steril. 2013, 100, 1303–1309. [Google Scholar] [CrossRef] [PubMed]
- Le Bouteiller, P. HLA-G in human early pregnancy: Control of uterine immune cell activation and likely vascular remodeling. Biomed. J. 2015, 38, 32–38. [Google Scholar]
- Perricone, R.; Perricone, C.; de Carolis, C.; Shoenfeld, Y. NK cells in autoimmunity: A two-edg’d weapon of the immune system. Autoimmun. Rev. 2008, 7, 384–390. [Google Scholar] [CrossRef] [PubMed]
- Mikołajczyk, M.; Skrzypczak, J.; Szymanowski, K.; Wirstlein, P. The assessment of LIF in uterine flushing: A possible new diagnostic tool in states of impared fertility. Reprod. Biol. 2003, 3, 259–270. [Google Scholar] [PubMed]
- Gonzalez, A.; Alegre, E.; Arroyo, A.; LeMaoult, J.; Echeveste, J.I. Identification of circulating nonclassic human leukocyte antigen G (HLA-G)-like molecules in exudates. Clin. Chem. 2011, 57, 1013–1022. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rizzo, R.; Lo Monte, G.; Bortolotti, D.; Graziano, A.; Gentili, V.; Di Luca, D.; Marci, R. Impact of Soluble HLA-G Levels and Endometrial NK Cells in Uterine Flushing Samples from Primary and Secondary Unexplained Infertile Women. Int. J. Mol. Sci. 2015, 16, 5510-5516. https://doi.org/10.3390/ijms16035510
Rizzo R, Lo Monte G, Bortolotti D, Graziano A, Gentili V, Di Luca D, Marci R. Impact of Soluble HLA-G Levels and Endometrial NK Cells in Uterine Flushing Samples from Primary and Secondary Unexplained Infertile Women. International Journal of Molecular Sciences. 2015; 16(3):5510-5516. https://doi.org/10.3390/ijms16035510
Chicago/Turabian StyleRizzo, Roberta, Giuseppe Lo Monte, Daria Bortolotti, Angela Graziano, Valentina Gentili, Dario Di Luca, and Roberto Marci. 2015. "Impact of Soluble HLA-G Levels and Endometrial NK Cells in Uterine Flushing Samples from Primary and Secondary Unexplained Infertile Women" International Journal of Molecular Sciences 16, no. 3: 5510-5516. https://doi.org/10.3390/ijms16035510