
Impact of Single Nucleotide Polymorphisms (SNPs) on Immunosuppressive Therapy in Lung Transplantation

Abstract
:
1. Introduction
2. Results and Discussion

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gender (Male/Female) | 34/17 |
|---|---|
| Age at transplant (Mean (SD)) | 45.4 (16.3) |
| Type of lung transplantation (Single/Double/Heart-Lung) | (17/32/2) |
| Primary indication of lung transplantation, no. (%) | |
| COPD 1, including emphysema | 15 (29.4) |
| Cystic fibrosis | 13 (25.5) |
| Idiopathic pulmonary fibrosis | 16 (31.3) |
| Others | 7 (13.8) |
| Gene | SNP | Variant | Frequency (%) | Expected Frequency (%) * |
|---|---|---|---|---|
| ABCB1 | rs1045642 (3435 C > T) | CC | 39.2 | 27.1 |
| CT | 35.3 | 51.8 | ||
| TT | 25.5 | 21.1 | ||
| rs1128503 (1236 T > C) | CC | 47.0 | 32.5 | |
| CT | 37.3 | 49.8 | ||
| TT | 15.7 | 17.7 | ||
| rs2032582 (2677 G > T/A) | GG | 45.1 | 35.1 | |
| GT | 50.1 | 50.8 | ||
| TT | 4.8 | 12.1 | ||
| rs9282564 (61 A > G) | AA | 90.2 | 81.7 | |
| AG | 9.8 | 16.7 | ||
| GG | 0.0 | 1.7 | ||
| ABCC2 | rs3740066 (3972 C > T) | CC | 41.2 | 58.3 |
| TC | 41.2 | 35.7 | ||
| TT | 17.6 | 6.0 | ||
| rs2273697 (1249 G > A) | GG | 64.7 | 57.6 | |
| GA | 33.3 | 35.3 | ||
| AA | 2.0 | 7.1 | ||
| rs717620 (-24 C > T) | CC | 54.9 | 56.7 | |
| CT | 41.2 | 41.6 | ||
| TT | 3.9 | 1.7 | ||
| CYP3A5 | rs776746 (CYP3A5*3) | GA | 96.1 | 83.3 |
| GA | 3.9 | 15.7 | ||
| AA | 0.0 | 1.1 | ||
| NOD2/CARD15 | rs2066844 (R702W) | CC | 84.3 | 87.7 |
| CT | 15.7 | 11.8 | ||
| TT | 0.0 | 0.5 | ||
| SLCO1B1 | rs2306283 (SLCO1B1*1B) | AA | 43.7 | 40.1 |
| AG | 41.7 | 43.7 | ||
| GG | 15.6 | 16.2 | ||
| rs4149056 (SLCO1B1*5) | TT | 74.5 | 70.0 | |
| TC | 19.6 | 28.3 | ||
| CC | 5.9 | 1.7 | ||
| UGT1A9 | rs6714486 (-275T > A) | TT | 88.2 | 85.0 |
| TA | 11.8 | 15.0 | ||
| AA | 0.0 | 0.0 | ||
| rs17868320 (-2152 C > CT) | CC | 100.0 | 98.2 | |
| CT | 0.0 | 1.2 | ||
| TT | 0.0 | 0.0 |
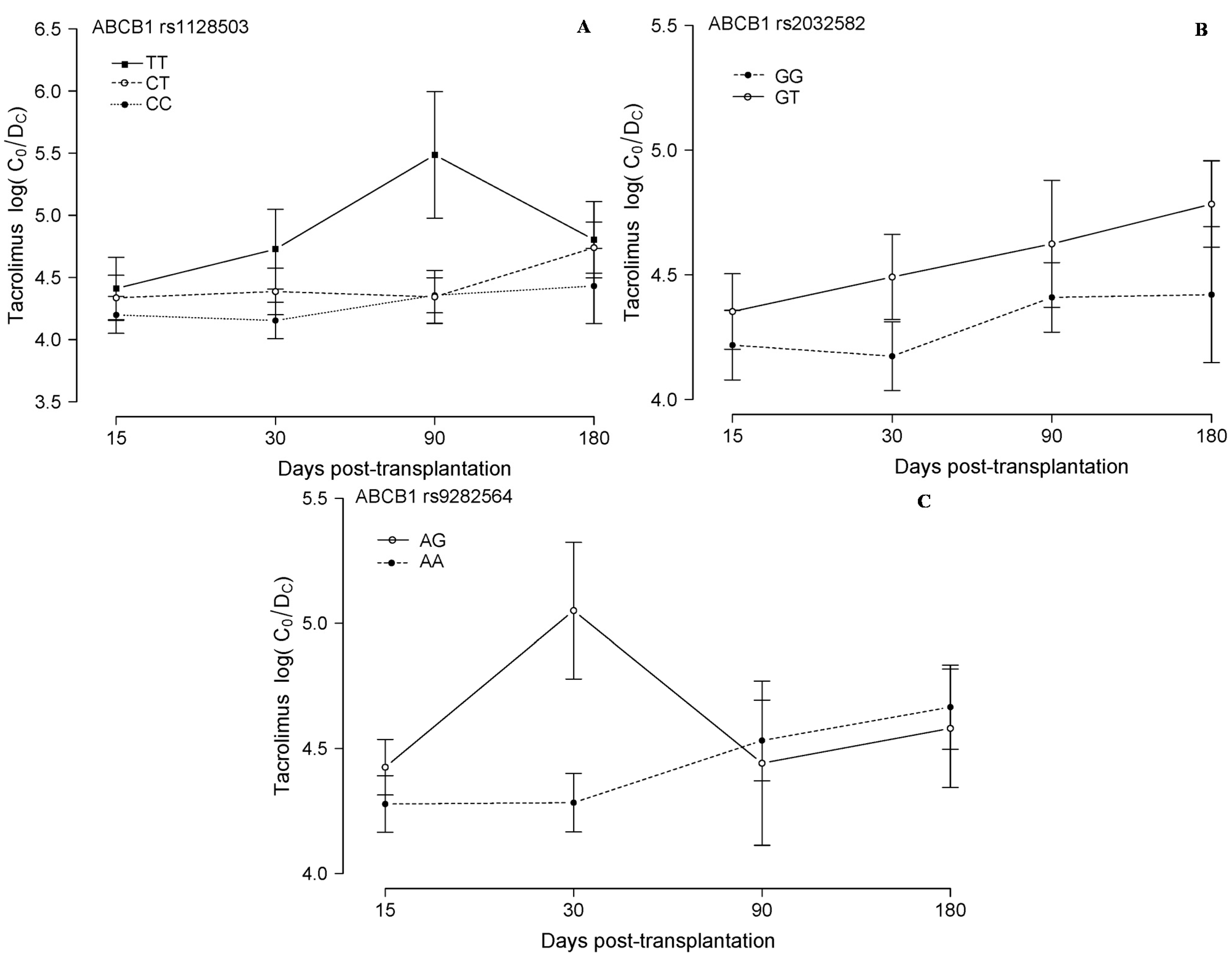
2.1. Tacrolimus Analysis



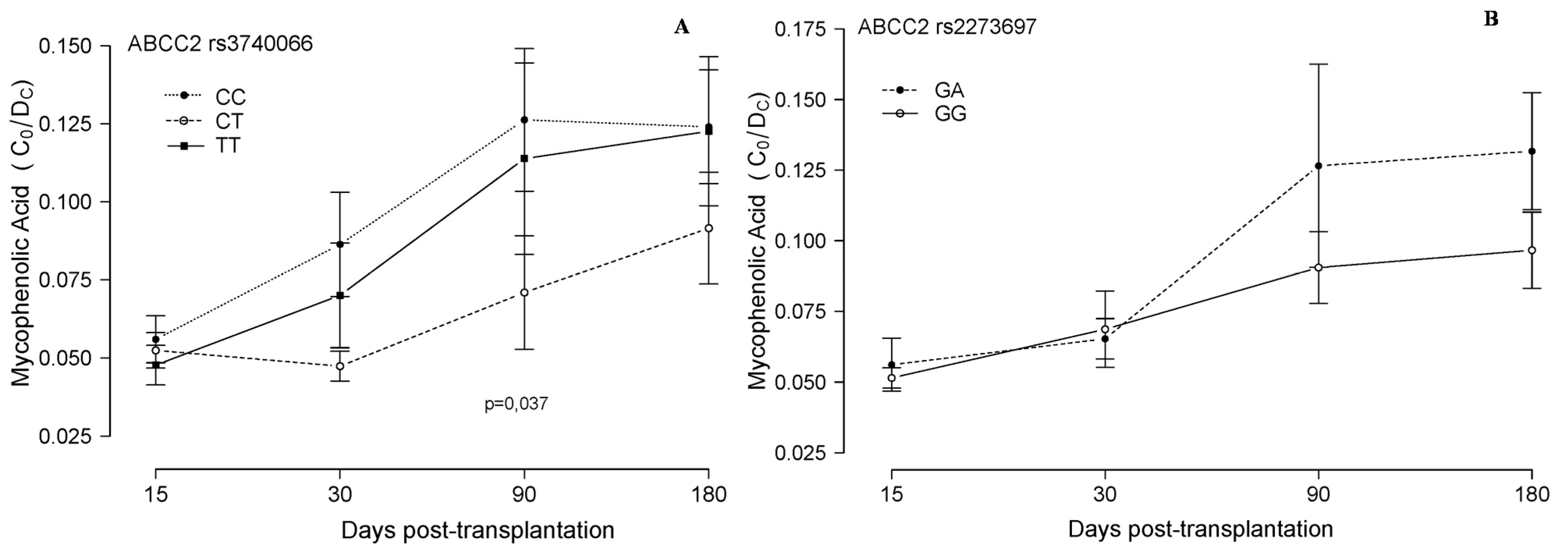
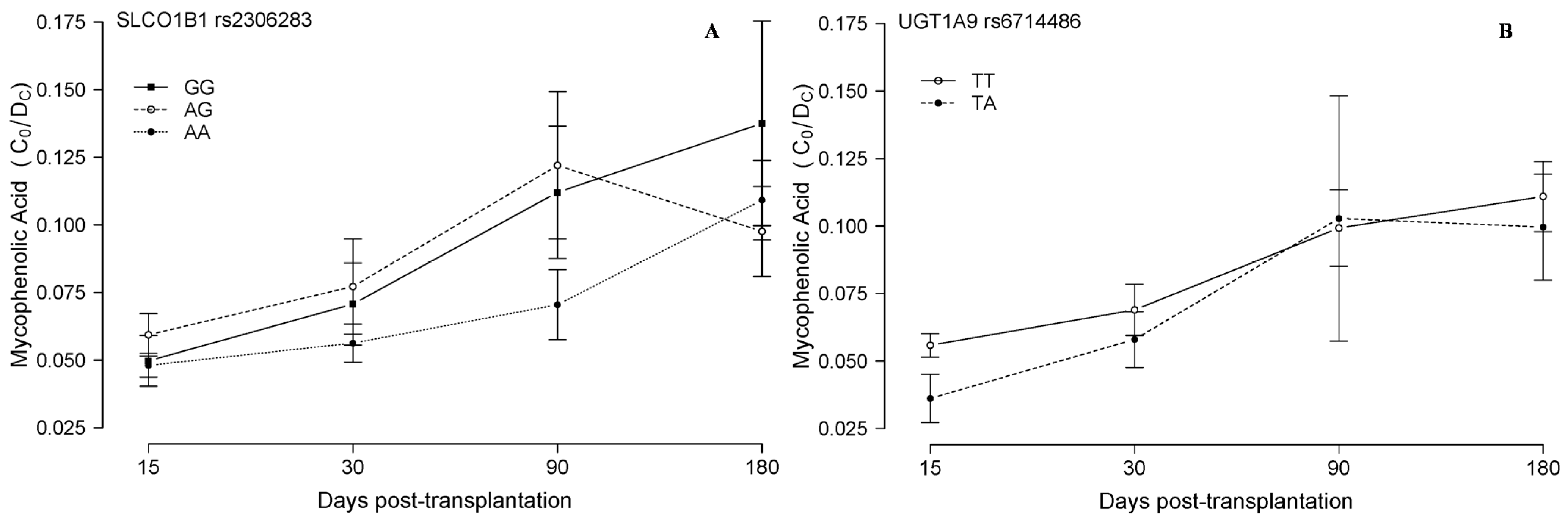
2.2. Mycophenolic Acid Analysis

2.3. Adverse Events
3. Experimental Section
3.1. Blood Immunosuppressants Concentration
3.2. Genotyping
3.3. Clinical Outcomes
3.4. Statistical Analysis
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- ISHLT Transplant Registry Quarterly Reports for Lung in Europe. Available online: https://www.ishlt.org/registries/quarterlyDataReportResults.asp?organ=LU&rptType=recip_p_surv&continent=3 (accessed on 10 May 2015).
- Studer, S.M.; Levy, R.D.; McNeil, K.; Orens, J.B. Lung transplant outcomes: A review of survival, graft function, physiology, health-related quality of life and cost-effectiveness. Eur. Respir. J. 2004, 24, 674–685. [Google Scholar] [CrossRef] [PubMed]
- Trindade, A.J.; Palmer, S.M. Current concepts and controversies in lung transplantation. Respir. Care Clin. N. Am. 2004, 10, 427–447. [Google Scholar] [CrossRef] [PubMed]
- Staatz, C.E.; Goodman, L.K.; Tett, S.E. Effect of CYP3A and ABCB1 single nucleotide polymorphisms on the pharmacokinetics and pharmacodynamics of calcineurin inhibitors: Part I. Clin. Pharmacokinet. 2010, 49, 141–175. [Google Scholar] [CrossRef] [PubMed]
- Dupuis, R.; Yuen, A.; Innocenti, F. The influence of UGT polymorphisms as biomarkers in solid organ transplantation. Int. J. Clin. Chem. 2012, 413, 1318–1325. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Figurski, M.; Shaw, L.M.; Burckart, G.J. The impact of P-glycoprotein and Mrp2 on mycophenolic acid levels in mice. Transpl. Immunol. 2008, 19, 192–196. [Google Scholar] [CrossRef] [PubMed]
- Stingl, J.C.; Bartels, H.; Viviani, R.; Lehmann, M.L.; Brockmöller, J. Relevance of UDP-glucuronosyltransferase polymorphisms for drug dosing: A quantitative systematic review. Pharmacol. Ther. 2014, 141, 92–116. [Google Scholar] [CrossRef] [PubMed]
- Naesens, M.; Kuypers, D.R.; Verbeke, K.; Vanrenterghem, Y. Multidrug resistance protein 2 genetic polymorphisms influence mycophenolic acid exposition allograft recipients. Transplantation 2006, 1074–1084. [Google Scholar] [CrossRef] [PubMed]
- Ting, L.S.L.; Benoit-Biancamano, M.O.; Bernard, O.; Riggs, K.W.; Guillemette, C.; Ensom, M.H.H. Pharmacogenetic impact of UDP-glucuronosyltransferase metabolic pathway and multidrug resistance-associated protein 2 transport pathway on mycophenolic acid in thoracic transplant recipients: An exploratory study. Pharmacotherapy 2010, 30, 1097–1108. [Google Scholar] [CrossRef] [PubMed]
- Burckart, G.J.; Hutchinson, I.V.; Zeevi, A. Pharmacogenomics and lung transplantation: Clinical implications. Pharmacogenomics J. 2006, 6, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Herrero, M.J.; Boso, V.; Rojas, L.; Bea, S.; Sanchez, J.; Hernandez, J.; Poveda, J.L.; Aliño, S. Practical Pharmacogenetics and Single Nucleotide Polymorphisms (SNPs) in Renal Transplantation. In Current Issues and Future Direction in Kidney Transplantation; Rath, T., Ed.; InTech Open Science: Valencia, Spain, 2013; pp. 287–307. [Google Scholar]
- Staatz, C.E.; Goodman, L.K.; Tett, S.E. Effect of CYP3A and ABCB1 single nucleotide polymorphisms on the pharmacokinetics and pharmacodynamics of calcineurin inhibitors: Part II. Clin. Pharmacokinet. 2010, 49, 207–221. [Google Scholar] [CrossRef] [PubMed]
- Provenzani, A.; Santeusanio, A.; Mathis, E.; Notarbartolo, M.; Labbozzetta, M.; Poma, P.; Provenzani, A.; Polidori, C.; Vizzini, G.; Polidori, P.; et al. Pharmacogenetic considerations for optimizing tacrolimus dosing in liver and kidney transplant patients. World J. Gastroenterol. 2013, 19, 9156–9173. [Google Scholar] [CrossRef] [PubMed]
- Zaza, G.; Granata, S.; Tomei, P.; Dalla Gassa, A.; Lupo, A. Personalization of the immunosuppressive treatment in renal transplant recipients: The great challenge in “omics” medicine. Int. J. Mol. Sci. 2015, 16, 4281–4305. [Google Scholar] [CrossRef] [PubMed]
- Murray, B.; Hawes, E.; Lee, R.A.; Watson, R.; Roederer, M.W. Genes and beans: Pharmacogenomics of renal transplant. Pharmacogenomics 2013, 14, 783–798. [Google Scholar] [CrossRef] [PubMed]
- Monchaud, C.; Marquet, P. Pharmacokinetic optimization of immunosuppressive therapy in thoracic transplantation: Part I. Clin. Pharmacokinet. 2009, 48, 419–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosó, V.; Herrero, M.J.; Buso, E.; Galán, J.; Almenar, L.; Sánchez-Lázaro, I. Genotype and allele frequencies of drug-metabolizing enzymes and drug transporter genes affecting immunosuppressants in the Spanish white population. Ther. Drug Monit. 2014, 36, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Herrero, M.J.; Almenar, L.; Jordán, C.; Sánchez, I.; Poveda, J.L.; Aliño, S.F. Clinical interest of pharmacogenetic polymorphisms in the immunosuppressive treatment after heart transplantation. Transplant. Proc. 2010, 42, 3181–3182. [Google Scholar] [CrossRef] [PubMed]
- Herrero, M.J.; Sánchez-Plumed, J.; Galiana, M.; Bea, S.; Marqués, M.R.; Aliño, S.F. Influence of pharmacogenetic polymorphisms in routine immunosuppression therapy after renal transplantation. Transplant. Proc. 2010, 42, 3134–3136. [Google Scholar] [CrossRef] [PubMed]
- Cusinato, D.A.C.; Lacchini, R.; Romao, E.A.; Moysés-Neto, M.; Coelho, E.B. Relationship of CYP3A5 genotype and ABCB1 diplotype to tacrolimus disposition in Brazilian kidney transplant patients. Br. J. Clin. Pharmacol. 2014, 78, 364–372. [Google Scholar] [CrossRef] [PubMed]
- Kimchi-Sarfaty, C.; Gribar, J.J.; Gottesman, M.M. Functional characterization of coding polymorphisms in the human MDR1 gene using a vaccinia virus expression system. Mol. Pharmacol. 2002, 62, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Lázaro, I.; Herrero, M.J.; Jordán-De Luna, C.; Bosó, V.; Almenar, L.; Rojas, L.; Martínez-Dolz, L.; Megías-Vericat, J.E.; Sendra, L.; Miguel, A.; et al. Association of single nucleotide polymorphisms to the efficacy and safety of immunosuppressant therapy after heart transplantation. Pharmacogenomics 2015, 24, 1–9. [Google Scholar]
- Jordán de Luna, C.; Herrero Cervera, M.J.; Sánchez Lázaro, I.; Almenar Bonet, L.; Poveda Andrés, J.L.; Aliño Pellicer, S.F. Pharmacogenetic study of ABCB1 and CYP3A5 genes during the first year following heart transplantation regarding tacrolimus or cyclosporine levels. Transplant. Proc. 2011, 43, 2241–2243. [Google Scholar] [CrossRef] [PubMed]
- Hesselink, D.A.; Bouamar, R.; Elens, L.; van Schaik, R.H.N.; van Gelder, T. The role of pharmacogenetics in the disposition of and response to tacrolimus in solid organ transplantation. Clin. Pharmacokinet. 2014, 53, 123–139. [Google Scholar] [CrossRef] [PubMed]
- Rojas, L.E.; Herrero, M.J.; Bosó, V.; García-Eliz, M.; Poveda, J.L.; Librero, J. Meta-analysis and systematic review of the effect of the donor and recipient CYP3A5 6986A>G genotype on tacrolimus dose requirements in liver transplantation. Pharmacogenet. Genomics 2013, 23, 509–517. [Google Scholar] [CrossRef] [PubMed]
- Rojas, L.; Neumann, I.; Herrero, M.J.; Bosó, V.; Reig, J.; Poveda, J.L.; Aliño, S.F. Effect of CYP3A5*3 on kidney transplant recipients treated with tacrolimus: A systematic review and meta-analysis of observational studies. Pharmacogenomics J. 2015, 15, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Thervet, E.; Loriot, M.A.; Barbier, S.; Buchler, M.; Ficheux, M.; Choukroun, G.; Toupance, O.; Touchard, G.; Alberti, C.; Le Pogamp, P.; et al. Optimization of initial tacrolimus dose using pharmacogenetic testing. Clin. Pharmacol. Ther. 2010, 87, 721–726. [Google Scholar] [PubMed]
- Birdwell, K.A.; Decker, B.; Barbarino, J.M.; Peterson, J.F.; Stein, C.M.; Sadee, W.; Wang, D.; Vinks, A.A.; He, Y.; Swen, J.J.; et al. Clinical pharmacogenetics implementation consortium (CPIC) guidelines for CYP3A5 genotype and tacrolimus dosing. Clin. Pharmacol. Ther. 2015, 98, 19–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naito, T.; Mino, Y.; Aoki, Y.; Hirano, K.; Shimoyama, K.; Ogawa, N.; Kagawa, Y.; Kawakami, J. ABCB1 genetic variant and its associated tacrolimus pharmacokinetics affect renal function in patients with rheumatoid arthritis. Clin. Chim. Acta 2015, 445, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Woodahl, E.L.; Ho, R.J.Y. The role of MDR1 genetic polymorphisms in interindividual variability in P-glycoprotein expression and function. Curr. Drug Metab. 2004, 5, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Marzolini, C.; Paus, E.; Buclin, T.; Kim, R.B. Polymorphisms in human MDR1 (P-glycoprotein): Recent advances and clinical relevance. Clin. Pharmacol. Ther. 2004, 75, 13–33. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zeevi, A.; McCurry, K.; Schuetz, E.; Zheng, H.; Iacono, A. Impact of ABCB1 (MDR1) haplotypes on tacrolimus dosing in adult lung transplant patients who are CYP3A5 *3/*3 non-expressors. Transpl. Immunol. 2006, 15, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Hesselink, D.A.; van Schaik, R.H.N.; van der Heiden, I.P.; van der Werf, M.; Gregoor, P.J.; Lindemans, J. Genetic polymorphisms of the CYP3A4; CYP3A5; and MDR-1 genes and pharmacokinetics of the calcineurin inhibitors cyclosporine and tacrolimus. Clin. Pharmacol. Ther. 2003, 74, 245–254. [Google Scholar] [CrossRef]
- Haufroid, V.; Mourad, M.; van Kerckhove, V.; Wawrzyniak, J.; de Meyer, M.; Eddour, D.C. The effect of CYP3A5 and MDR1 (ABCB1) polymorphisms on cyclosporine and tacrolimus dose requirements and trough blood levels in stable renal transplant patients. Pharmacogenetics 2004, 14, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Zheng, H.; Zeevi, A.; Schuetz, E.; Lamba, J.; McCurry, K.; Griffith, B.P. Tacrolimus dosing in adult lung transplant patients is related to cytochrome P4503A5 gene polymorphism. J. Clin. Pharmacol. 2004, 44, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Mazidi, T.; Rouini, M.-R.; Ghahremani, M.-H.; Dashti-Khavidaki, S.; Lessan-Pezeshki, M.; Ahmadi, F.L. Impact of UGT1A9 polymorphism on mycophenolic acid pharmacokinetic parameters in stable renal transplant patients. Iran J. Pharm. Res. 2013, 12, 547–556. [Google Scholar] [PubMed]
- Fukuda, T.; Goebel, J.; Cox, S.; Maseck, D.; Zhang, K.; Sherbotie, J.R. UGT1A9; UGT2B7; and MRP2 genotypes can predict mycophenolic acid pharmacokinetic variability in pediatric kidney transplant recipients. Ther. Drug Monit. 2012, 34, 671–679. [Google Scholar] [CrossRef] [PubMed]
- Ohmann, E.L.; Burckart, G.J.; Brooks, M.M.; Chen, Y.; Pravica, V.; Girnita, D.M. Genetic polymorphisms influence mycophenolate mofetil-related adverse events in pediatric heart transplant patients. J. Heart Lung Transplant. 2010, 29, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Woillard, J.-B.; Rerolle, J.-P.; Picard, N.; Rousseau, A.; Drouet, M.; Munteanu, E. Risk of diarrhoea in a long-term cohort of renal transplant patients given mycophenolate mofetil: The significant role of the UGT1A8*2 variant allele. Br. J. Clin. Pharmacol. 2010, 69, 675–683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burckart, G.J.; Figg, W.D.; Brooks, M.M.; Green, D.J.; Troutman, S.M.; Ferrell, R. Multi-institutional study of outcomes after pediatric heart transplantation: Candidate gene polymorphism analysis of ABCC2. J. Pediatr. Pharmacol. Ther. 2014, 19, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Staatz, C.E.; Tett, S.E. Clinical pharmacokinetics and pharmacodynamics of mycophenolate in solid organ transplant recipients. Clin. Pharmacokinet. 2007, 46, 13–58. [Google Scholar]
- Tsai, S.-J.; Hong, C.-J.; Yeh, H.-L.; Liou, Y.-J.; Yang, A.C.; Liu, M.-E. Heterozygote advantage of the MTHFR C677T polymorphism on specific cognitive performance in elderly Chinese males without dementia. Dement. Geriatr. Cogn. Disord. 2011, 32, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Shao, M.; Wang, S.; Zhao, X.; Chen, H.; Qian, J. Heterozygote advantage of methylenetetrahydrofolate reductase polymorphisms on clinical outcomes in advanced non-small cell lung cancer (NSCLC) patients treated with platinum-based chemotherapy. Tumour Biol. 2014, 35, 11159–11170. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.X.; Chen, B.; Jin, Z.; Yu, Z.; Wang, X.; Chen, H.; Mao, A.; Cai, W. Influence of uridine diphosphate (UDP)-glucuronosyltransferases and ABCC2 genetic polymorphisms on the pharmacokinetics of mycophenolic acid and its metabolites in Chinese renal transplant recipients. Xenobiotica 2008, 38, 1422–1436. [Google Scholar] [CrossRef] [PubMed]
- Michelon, H.; König, J.; Durrbach, A.; Quteineh, L.; Verstuyft, C.; Furlan, V. SLCO1B1 genetic polymorphism influences mycophenolic acid tolerance in renal transplant recipients. Pharmacogenomics 2010, 11, 1703–1713. [Google Scholar] [CrossRef] [PubMed]
- Sarangi, S.C.; Reeta, K.H.; Agarwal, S.K.; Kaleekal, T.; Guleria, S.; Gupta, Y.K. A pilot study on area under curve of mycophenolic acid as a guide for its optimal use in renal transplant recipients. Indian J. Med. Res. 2012, 135, 84–91. [Google Scholar] [PubMed]
- Ningappa, M.; Higgs, B.W.; Weeks, D.E.; Ashokkumar, C.; Duerr, R.H.; Sun, Q. NOD2 gene polymorphism rs2066844 associates with need for combined liver-intestine transplantation in children with short-gut syndrome. Am. J. Gastroenterol. 2011, 106, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Saner, F.H.; Nowak, K.; Hoyer, D.; Rath, P.; Canbay, A.; Paul, A. A non-interventional study of the genetic polymorphisms of NOD2 associated with increased mortality in non-alcoholic liver transplant patients. BMC Gastroenterol. 2014, 14, 4. [Google Scholar] [CrossRef] [PubMed]
- Van Gelder, T.; van Schaik, R.H.; Hesselink, D.A. Practicability of pharmacogenetics in transplantation medicine. Clin. Pharmacol. Ther. 2014, 95, 262–264. [Google Scholar] [CrossRef] [PubMed]
- Pallet, N.; Jannot, A.S.; El Bahri, M.; Etienne, I.; Buchler, M.; de Ligny, B.H.; Choukroun, G.; Colosio, C.; Thierry, A.; Vigneau, C.; et al. Kidney transplant recipients carrying the CYP3A4*22 allelic variant have reduced tacrolimus clearance and often reach supratherapeutic tacrolimus concentrations. Am. J. Transplant. 2015, 15, 800–805. [Google Scholar] [CrossRef] [PubMed]
- Shi, W.L.; Tang, H.L.; Zhai, S.D. Effects of the CYP3A4*1B genetic polymorphism on the pharmacokinetics of tacrolimus in adult renal transplant recipients: A meta-analysis. PLoS ONE 2015, 10, e0127995. [Google Scholar] [CrossRef] [PubMed]
- Sombogaard, F.; van Schaik, R.H.; Mathot, R.A.; Budde, K.; van der Werf, M.; Vulto, A.G.; Weimar, W.; Glander, P.; Essioux, L.; van Gelder, T. Interpatient variability in IMPDH activity in MMF-treated renal transplant patients is correlated with IMPDH type II 3757T>C polymorphism. Pharmacogenet. Genomics 2009, 19, 626–634. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.; Harwood, S.M.; Döhler, B.; Opelz, G.; Yaqoob, M.M. Inosine monophosphate dehydrogenase polymorphisms and renal allograft outcome. Transplantation 2012, 94, 486–491. [Google Scholar] [CrossRef] [PubMed]
- Bosó, V.; Herrero, M.J.; Bea, S.; Galiana, M.; Marrero, P.; Marqués, M.R.; Hernández, J.; Sánchez-Plumed, J.; Poveda, J.L.; Aliño, S.F. Increased hospital stay and allograft dysfunction in renal transplant recipients with Cyp2c19 AA variant in SNP rs4244285. Drug Metab. Dispos. 2013, 41, 480–487. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruiz, J.; Herrero, M.J.; Bosó, V.; Megías, J.E.; Hervás, D.; Poveda, J.L.; Escrivá, J.; Pastor, A.; Solé, A.; Aliño, S.F. Impact of Single Nucleotide Polymorphisms (SNPs) on Immunosuppressive Therapy in Lung Transplantation. Int. J. Mol. Sci. 2015, 16, 20168-20182. https://doi.org/10.3390/ijms160920168
Ruiz J, Herrero MJ, Bosó V, Megías JE, Hervás D, Poveda JL, Escrivá J, Pastor A, Solé A, Aliño SF. Impact of Single Nucleotide Polymorphisms (SNPs) on Immunosuppressive Therapy in Lung Transplantation. International Journal of Molecular Sciences. 2015; 16(9):20168-20182. https://doi.org/10.3390/ijms160920168
Chicago/Turabian StyleRuiz, Jesus, María José Herrero, Virginia Bosó, Juan Eduardo Megías, David Hervás, Jose Luis Poveda, Juan Escrivá, Amparo Pastor, Amparo Solé, and Salvador Francisco Aliño. 2015. "Impact of Single Nucleotide Polymorphisms (SNPs) on Immunosuppressive Therapy in Lung Transplantation" International Journal of Molecular Sciences 16, no. 9: 20168-20182. https://doi.org/10.3390/ijms160920168