
Endometriosis Might Be Inversely Associated with Developing Chronic Kidney Disease: A Population-Based Cohort Study in Taiwan


 ,
,
Abstract
:1. Introduction
2. Results
2.1. General Characteristics
2.2. Incidence Rates and Crude and Adjusted Risks of CKD among Women with and without Endometriosis
2.3. The Role of Age in the Relevance between CKD and Endometriosis
2.4. Comparison of the Risk of CKD among Women with and without Endometriosis, According to Age
2.5. Comparison of CKD Risk among Women with and without Endometriosis, According to Age
3. Discussion
4. Materials and Methods
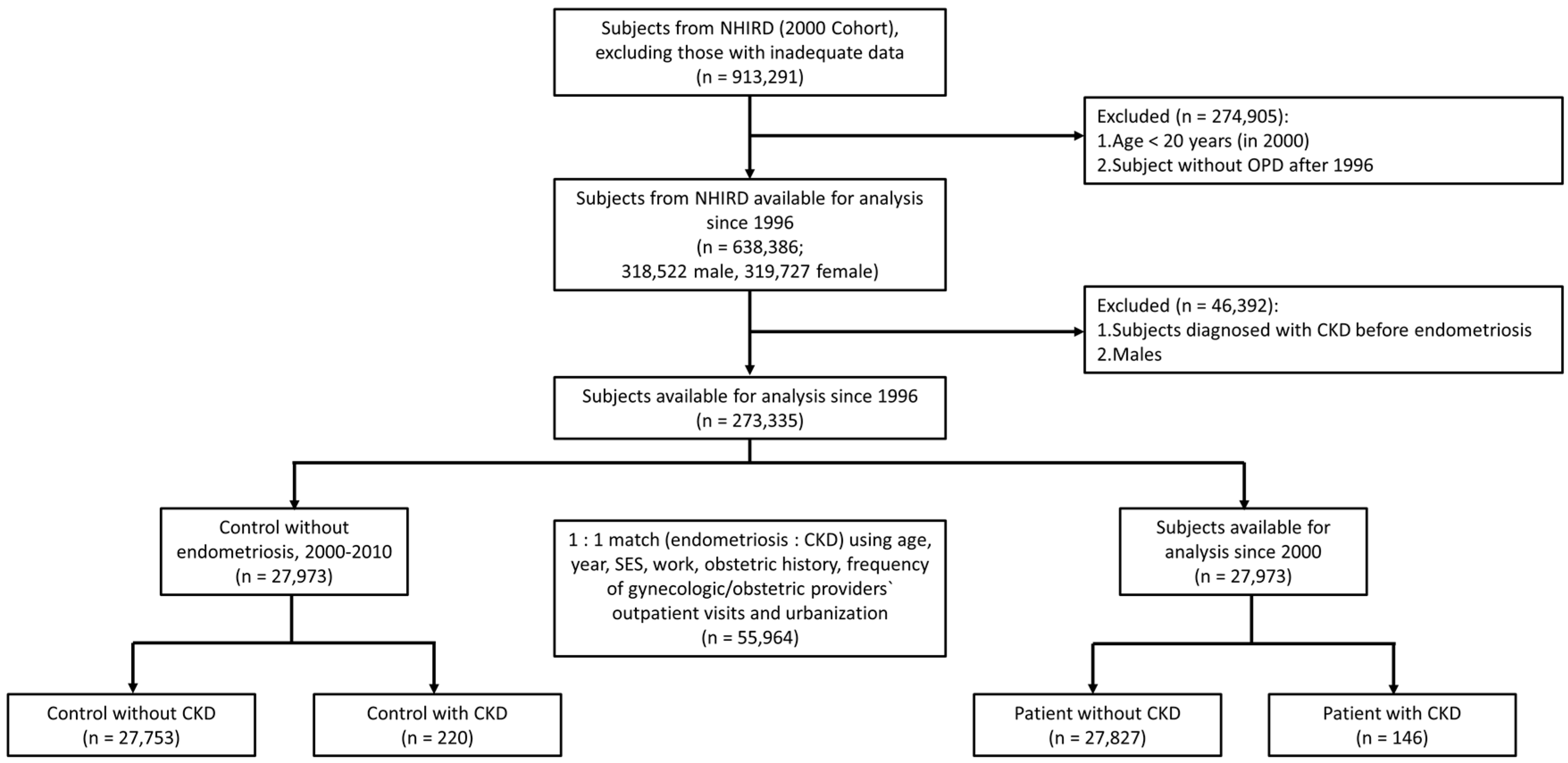
4.1. Study Population
4.2. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| MDPI | Multidisciplinary Digital Publishing Institute |
| DOAJ | Directory of Open Access Journals |
| CKD | chronic kidney disease |
| HR | hazard ratio |
| IR | incidence rate |
| CI | confidence interval |
| GFR | glomerular filtration rate |
| ESRD | end-stage renal disease |
| DM | diabetes mellitus |
| CVD | cardiovascular disease |
| NHI | National Health Insurance |
| LHID | Longitudinal Health Insurance Database |
| NHRI | National Health Research Institute |
| NHIRD | National Health Insurance Research Database |
| ICD9-CM | International Classification of Diseases, Ninth Revision, and Clinical Modifications |
| PID | pelvic inflammatory disease |
| OR | odds ratio |
| ER | estrogen receptor |
| GPER | G-protein-couple protein 30 |
| ERK | elementary response kinase |
| OPD | outpatient clinics |
| TPVGH-IRB (2) | Institutional Review Broad (2) of Taipei Veterans General Hospital |
References
- Stevens, P.E.; Levin, A.; Kidney Disease: Improving Global Outcomes Chronic Kidney Disease Guideline Development Work Group Members. Evaluation and management of chronic kidney disease: Synopsis of the kidney disease: Improving global outcomes 2012 clinical practice guideline. Ann. Intern. Med. 2013, 158, 825–830. [Google Scholar] [CrossRef] [PubMed]
- Mills, K.T.; Xu, Y.; Zhang, W.; Bundy, J.D.; Chen, C.S.; Kelly, T.N.; Chen, J.; He, J. A systematic analysis of worldwide population-based data on the global burden of chronic kidney disease in 2010. Kidney Int. 2015, 88, 950–957. [Google Scholar] [CrossRef] [PubMed]
- Go, A.S.; Chertow, G.M.; Fan, D.; McCulloch, C.E.; Hsu, C.Y. Chronic kidney disease and the risks of death; cardiovascular events; and hospitalization. N. Engl. J. Med. 2004, 351, 1296–1305. [Google Scholar] [CrossRef] [PubMed]
- GBD 2013 Mortality and Cause of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death; 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2013, 385, 117–171. [Google Scholar]
- Chang, Y.K.; Liu, J.S.; Hsu, Y.H.; Tarng, D.C.; Hsu, C.C. Increased risk of end-stage renal disease (ESRD) requiring chronic dialysis is associated with use of nonsteroidal anti-inflammatory drugs (NSAIDs): Nationwide case-crossover study. Medicine 2015, 94, e1362. [Google Scholar] [CrossRef] [PubMed]
- Chien, S.C.; Ou, S.M.; Shih, C.J.; Chao, P.W.; Li, S.Y.; Lee, Y.J.; Kuo, S.C.; Wang, S.J.; Chen, T.J.; Tarng, D.C.; et al. Comparative effectiveness of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers in terms of major cardiovascular disease outcomes in elderly patients: A nationwide population-based cohort study. Medicine 2015, 94, e1751. [Google Scholar] [CrossRef] [PubMed]
- Jha, V.; Garcia-Garcia, G.; Iseki, K.; Li, Z.; Naicker, S.; Plattner, B.; Saran, R.; Wang, A.Y.; Yang, C.W. Chronic kidney disease: Global dimension and perspectives. Lancet 2013, 382, 260–272. [Google Scholar] [CrossRef]
- Huang, B.S.; Lee, W.L.; Wang, P.H. The slowing down of renal deterioration but acceleration of cardiac hypertrophy: Is the estrogen receptor-α a hero or villain? Am. J. Physiol. Ren. Physiol. 2014, 307, F1352–F1354. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.L.; Chang, W.H.; Wang, K.C.; Guo, C.Y.; Chou, Y.J.; Huang, N.; Huang, H.Y.; Yen, M.S.; Wang, P.H. The risk of epithelial ovarian cancer of women with endometriosis may be varied greatly if diagnostic criteria are different: A nationwide population-based cohort study. Medicine 2015, 94, e1633. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.H.; Wang, K.C.; Lee, W.L.; Huang, N.; Chou, Y.J.; Feng, R.C.; Yen, M.S.; Huang, B.S.; Guo, C.Y.; Wang, P.H. Endometriosis and the subsequent risk of epithelial ovarian cancer. Taiwan J. Obstet. Gynecol. 2014, 53, 530–535. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.C.; Chang, W.H.; Lee, W.L.; Huang, N.; Huang, H.Y.; Yen, M.S.; Guo, C.Y.; Wang, P.H. An increased risk of epithelial ovarian cancer in Taiwanese women with a new surgico-pathological diagnosis of endometriosis. BMC Cancer 2014. [Google Scholar] [CrossRef] [PubMed]
- Bulun, S.E. Endometriosis. N. Engl. J. Med. 2009, 360, 268–279. [Google Scholar] [CrossRef] [PubMed]
- Mourin-Jouret, A.; Squifflet, J.P.; Cosyns, J.P.; Pirson, Y.; Alexandre, G.P. Bilateral ureteral endometriosis with end-stage renal failure. Urology 1987, 29, 302–306. [Google Scholar] [CrossRef]
- Hsieh, M.F.; Wu, I.W.; Tsai, C.J.; Huang, S.S.; Chang, L.C.; Wu, M.S. Ureteral endometriosis with obstructive uropathy. Intern. Med. 2010, 49, 573–576. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, J.L.; Jiménez, J.S.; Tejerizo, A.; Lopez, G.; Duarte, J.; Sánchez Bustos, F. Rectosigmoid deep infiltrating endometriosis and ureteral involvement with loss of renal function. Eur. J. Obstet. Gynecol. Reprod. Biol. 2012, 162, 121–124. [Google Scholar] [CrossRef] [PubMed]
- Arrieta Bretón, S.; López Carrasco, A.; Hernández Gutiérrez, A.; Rodríguez González, R.; de Santiago García, J. Complete loss of unilateral renal function secondary to endometriosis: A report of three cases. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 171, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Brosius, F.C., 3rd; Hostetter, T.H.; Kelepouris, E.; Mitsnefes, M.M.; Moe, S.M.; Moore, M.A.; Pennathur, S.; Smith, G.L.; Wilson, P.W.; American Heart Association Kidney and Cardiovascular Disease Council; et al. Detection of chronic kidney disease in patients with or at increased risk of cardiovascular disease: A science advisory from the American Heart Association Kidney And Cardiovascular Disease Council; the Councils on High Blood Pressure Research; Cardiovascular Disease in the Young; and Epidemiology and Prevention; and the Quality of Care and Outcomes Research Interdisciplinary Working Group: Developed in collaboration with the National Kidney Foundation. Circulation 2006, 114, 1083–1087. [Google Scholar] [PubMed]
- Tsai, W.C.; Wu, H.Y.; Peng, Y.S.; Ko, M.J.; Wu, M.S.; Hung, K.Y.; Wu, K.D.; Chu, T.S.; Chien, K.L. Risk factors for development and progression of chronic kidney disease: A systematic review and exploratory meta-analysis. Medicine 2016, 95, e3013. [Google Scholar] [CrossRef] [PubMed]
- Chou, C.Y.; Wang, S.M.; Liang, C.C.; Chang, C.T.; Liu, J.H.; Wang, I.K.; Hsiao, L.C.; Muo, C.H.; Chung, C.J.; Huang, C.C. Peritoneal dialysis is associated with a better survival in cirrhotic patients with chronic kidney disease. Medicine 2016, 95, e2465. [Google Scholar] [CrossRef] [PubMed]
- Burns, K.A.; Korach, K.S. Estrogen receptors and human disease: An update. Arch. Toxicol. 2012, 86, 1491–1504. [Google Scholar] [CrossRef] [PubMed]
- Ng, R.R.; Tan, G.H.; Liu, W.; Ti, L.K.; Chew, S.T. The association of acute kidney injury and atrial fibrillation after cardiac surgery in an Asian prospective cohort study. Medicine 2016, 95, e3005. [Google Scholar] [CrossRef] [PubMed]
- Lee, F.K.; Yen, M.S.; Wang, P.H. Is it safe to preserve the ovary of premenopausal women with supposed early-stage endometrial cancer? Taiwan J. Obstet. Gynecol. 2016, 55, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.H.; Ho, C.H.; Chen, Y.J.; Horng, H.C.; Chang, Y.H.; Chao, H.T.; Yen, M.S.; Chow, S.N.; Sheu, B.C.; Taiwan Association of Gynecology Systematic Review Group; et al. Highlights from the 2015 annual meeting and first international congress of the Taiwan association of gynecology. Taiwan J. Obstet. Gynecol. 2015, 54, 803–805. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.L.; Lee, F.K.; Su, W.H.; Tsui, K.H.; Kuo, C.D.; Hsieh, S.L.; Wang, P.H. Hormone therapy for younger patients with endometrial cancer. Taiwan J. Obstet. Gynecol. 2012, 51, 495–505. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.H.; Pan, H.A.; Wang, S.T.; Hsu, C.C.; Chang, F.M.; Huang, K.E. Quality of life and sexuality changes in postmenopausal women receiving tibolone therapy. Climacteric 2001, 4, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.H.; Cheng, C.L.; Kao Yang, Y.H.; Lin, L.J. Hormone therapy and risk of venous thromboembolism among postmenopausal women in Taiwan—A 10-year nationwide population-based study. Circ. J. 2015, 79, 1107–1114. [Google Scholar] [CrossRef] [PubMed]
- Chou, C.H.; Ko, H.C.; Wu, J.Y.; Chang, F.M.; Tung, Y.Y. Effect of previous diagnoses of depression, menopause status, vasomotor symptoms, and neuroticism on depressive symptoms among climacteric women: A 30-month follow-up. Taiwan J. Obstet. Gynecol. 2015, 54, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Leibetseder, V.; Humpeler, S.; Zuckermann, A.; Svoboda, M.; Thalhammer, T.; Marktl, W.; Ekmekcioglu, C. Time dependence of estrogen receptor expression in human hearts. Biomed. Pharmacother. 2010, 64, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Yang, D.H.; Chiang, T.I.; Chang, I.C.; Lin, F.H.; Wei, C.C.; Cheng, Y.W. Increased levels of circulating advanced glycation end-products in menopausal women with osteoporosis. Int. J. Med. Sci. 2014, 11, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Markićević, M.; Džodić, R.; Buta, M.; Kanjer, K.; Mandušić, V.; Nešković-Konstantinović, Z.; Nikolić-Vukosavljević, D. Trefoil factor 1 in early breast carcinoma: A potential indicator of clinical outcome during the first 3 years of follow-up. Int. J. Med. Sci. 2014, 11, 663–673. [Google Scholar] [CrossRef] [PubMed]
- Bulun, S.E.; Lin, Z.; Imir, G.; Amin, S.; Demura, M.; Yilmaz, B.; Martin, R.; Utsunomiya, H.; Thung, S.; Gurates, B.; et al. Regulation of aromatase expression in estrogen-responsive breast and uterine disease: From bench to treatment. Pharmacol. Rev. 2005, 57, 359–383. [Google Scholar] [CrossRef] [PubMed]
- Tsai, H.W.; Wang, P.H.; Huang, B.S.; Twu, N.F.; Yen, M.S.; Chen, Y.J. Low-dose add-back therapy during postoperative GnRH agonist treatment. Taiwan J. Obstet. Gynecol. 2016, 55, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Eriksen, B.O.; Ingebretsen, O.C. The progression of chronic kidney disease: A 10-year population-based study of the effects of gender and age. Kidney Int. 2006, 69, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Ciccone, M.M.; Bilianou, E.; Balbarini, A.; Gesualdo, M.; Ghiadoni, L.; Metra, M.; Palmiero, P.; Pedrinelli, R.; Salvetti, M.; Scicchitano, P.; et al. Task force on: ‘Early markers of atherosclerosis: Influence of age and sex’. J. Cardiovasc. Med. 2013, 14, 757–766. [Google Scholar] [CrossRef] [PubMed]
- Turin, T.C.; Tonelli, M.; Manns, B.J.; Ahmed, S.B.; Ravani, P.; James, M.; Hemmelgarn, B.R. Lifetime risk of ESRD. J. Am. Soc. Nephrol. 2012, 23, 1569–1578. [Google Scholar] [CrossRef] [PubMed]
- Martin, Y.N.; Pabelick, C.M. Sex differences in the pulmonary circulation: Implications for pulmonary hypertension. Am. J. Physiol. Heart Circ. Physiol. 2014, 306, H1253–H1264. [Google Scholar] [CrossRef] [PubMed]
- Diwan, V.; Small, D.; Kauter, K.; Gobe, G.C.; Brown, L. Gender differences in adenine-induced chronic kidney disease and cardiovascular complications in rats. Am. J. Physiol. Ren. Physiol. 2014, 307, F1169–F1178. [Google Scholar] [CrossRef] [PubMed]
- Kummer, S.; Jeruschke, S.; Wegerich, L.V.; Peters, A.; Lehmann, P.; Seibt, A.; Mueller, F.; Koleganova, N.; Halbenz, E.; Schmitt, C.P.; et al. Estrogen receptor alpha expression in podocytes mediates protection against apoptosis in vitro and in vivo. PLoS ONE 2011, 6, e27457. [Google Scholar] [CrossRef] [PubMed]
- Fung, M.M.; Poddar, S.; Bettencourt, R.; Jassal, S.K.; Barrett-Connor, E. A cross-sectional and 10-year prospective study of postmenopausal estrogen therapy and blood pressure, renal function, and albuminuria: The Rancho Bernardo Study. Menopause 2011, 18, 629–637. [Google Scholar] [CrossRef] [PubMed]
- Practice Committee of the American Society for Reproductive Medicine. Endometriosis and infertility: A committee opinion. Fertil. Steril. 2012, 98, 591–598. [Google Scholar]
- Yang, M.H.; Wang, P.H.; Wang, S.J.; Sun, W.Z.; Oyang, Y.J.; Fuh, J.L. Women with endometriosis are more likely to suffer from migraines: A population-based study. PLoS ONE 2012, 7, e33941. [Google Scholar] [CrossRef] [PubMed]
- Hung, G.Y.; Yen, C.C.; Horng, J.L.; Liu, C.Y.; Chen, W.M.; Chen, T.H.; Liu, C.L. Incidences of primary soft tissue sarcoma diagnosed on extremities and trunk wall: A population-based study in Taiwan. Medicine 2015, 94, e1696. [Google Scholar] [CrossRef] [PubMed]
- Valsecchi, M.G.; Silvestri, D.; Sasieni, P. Evaluation of long-term survival: Use of diagnostics and robust estimators with Cox’s proportional hazards model. Stat. Med. 1996, 15, 2763–2780. [Google Scholar] [CrossRef]


{kind=link}
| Study or Subgroup | Total (n = 55,964) | Endometriosis (n = 27,973) | Controls (n = 27,973) | p-Value | |||
|---|---|---|---|---|---|---|---|
| Person-Years | 628,337 | 314,514 | 313,823 | ||||
| Variable | n | % | n | % | n | % | |
| Target | <0.0001 | ||||||
| CKD | 366 | 0.65 | 146 | 0.52 | 220 | 0.79 | |
| No CKD | 55,580 | 99.35 | 27,827 | 99.48 | 27,753 | 99.21 | |
| Age * | 0.6059 | ||||||
| ≤42 | 28,573 | 51.07 | 14,256 | 50.96 | 14,317 | 51.18 | |
| >42 | 27,373 | 48.93 | 13,717 | 49.04 | 13,656 | 48.82 | |
| SES | 0.5376 | ||||||
| ≥40,000 | 6145 | 10.98 | 3059 | 10.94 | 3086 | 11.03 | |
| 20,000–39,999 | 13,382 | 23.92 | 6742 | 24.10 | 6640 | 23.74 | |
| <20,000 | 24,582 | 43.94 | 12,313 | 44.02 | 12,269 | 43.86 | |
| Others | 11,837 | 21.16 | 5859 | 20.95 | 5978 | 21.37 | |
| Work | 0.7336 | ||||||
| Yes | 48,068 | 85.92 | 24,020 | 85.87 | 24,048 | 85.97 | |
| No | 7878 | 14.08 | 3953 | 14.13 | 3925 | 14.03 | |
| Urbanization | 0.8194 | ||||||
| Urban | 19,002 | 33.96 | 9475 | 33.87 | 9527 | 34.06 | |
| Suburban | 25,546 | 45.66 | 12,772 | 45.66 | 12,774 | 45.67 | |
| Rural | 11,398 | 20.37 | 5726 | 20.47 | 5672 | 20.28 | |
| PID | <0.0001 | ||||||
| Yes | 37,928 | 67.79 | 22,449 | 80.25 | 15,479 | 55.34 | |
| No | 18,018 | 32.21 | 5524 | 19.75 | 12,494 | 44.66 | |
| Infertility | <0.0001 | ||||||
| Yes | 3056 | 5.46 | 2356 | 8.42 | 700 | 2.50 | |
| No | 52,890 | 94.54 | 25,617 | 91.58 | 27,273 | 97.50 | |
| Menopause | <0.0001 | ||||||
| Yes | 27,026 | 48.31 | 20,460 | 73.14 | 6566 | 23.47 | |
| No | 28,920 | 51.69 | 7513 | 26.86 | 21,407 | 76.53 | |
| CVD | <0.0001 | ||||||
| Yes | 6411 | 11.46 | 3380 | 12.08 | 3031 | 10.84 | |
| No | 49,535 | 88.54 | 24,593 | 87.92 | 24,942 | 89.16 | |
| DM | 0.1343 | ||||||
| Yes | 7259 | 12.98 | 3689 | 13.19 | 3570 | 12.76 | |
| No | 48,687 | 87.02 | 24,284 | 86.81 | 24,403 | 87.24 | |
| CLD | <0.0001 | ||||||
| Yes | 1851 | 3.31 | 1050 | 3.75 | 801 | 2.86 | |
| No | 54,095 | 96.69 | 26,923 | 96.25 | 27,172 | 97.14 | |
| RD | <0.0001 | ||||||
| Yes | 2891 | 5.17 | 1672 | 5.98 | 1219 | 4.36 | |
| No | 53,055 | 94.83 | 26,301 | 94.02 | 26,754 | 95.64 | |
| Incidence or Risk | Patients with Endometriosis (n = 27,973) | Controls (n = 27,973) |
|---|---|---|
| Number of patients with CKD | 146 | 220 |
| Incidence per 10,000 person-years | 4.64 | 7.01 |
| Crude HR (95% CI) | 0.65 (0.53–0.81) *** | 1.00 |
| Ad HR1 (95% CI) | 0.69 (0.56–0.86) *** | 1.00 |
| Ad HR2 (95% CI) | 0.85 (0.65–1.10) | 1.00 |
| Age | <40 Years | 40–49 Years | 50–59 Years | 60–69 Years | ≥70 Years | p * |
|---|---|---|---|---|---|---|
| n = 18 | n = 55 | n = 47 | n = 20 | n = 6 | ||
| IR | 1.324 | 5.744 | 7.682 | 11.669 | 13.339 | |
| C HR | 1.00 (Ref.) | 4.72 (2.74–8.13) | 5.99 (3.44–10.44) | 9.26 (4.85–17.68) | 10.66 (4.20–27.06) | <0.0001 |
| p ** | <0.0001 | <0.0001 | <0.0001 | <0.0001 | ||
| Ad HR1 | 1.00 (Ref.) | 2.86 (1.58–5.16) | 2.33 (1.24–4.37) | 2.43 (1.16–5.07) | 2.29 (0.84–6.23) | 0.0162 |
| p ** | 0.0005 | 0.0087 | 0.0181 | 0.1066 | ||
| Ad HR2 | 1.00 (Ref.) | 2.92 (1.61–5.27) | 2.53 (1.34–4.79) | 2.64 (1.26–5.54) | 2.46 (0.90–6.73) | 0.0132 |
| p ** | 0.0004 | 0.0044 | 0.0104 | 0.0803 |
| Age | <40 Years (n = 23873) | 40–49 Years (n = 18576) | 50–59 Years (n = 10156) | 60–69 Years (n = 2629) | ≥70 Years (n = 712) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Patients | Controls | Patients | Controls | Patients | Controls | Patients | Controls | Patients | Controls | |
| Diagnosis of CKD | ||||||||||
| Yes | 18 | 29 | 55 | 81 | 47 | 62 | 20 | 37 | 6 | 11 |
| No | 11872 | 11954 | 9310 | 9130 | 5001 | 5046 | 1298 | 1274 | 346 | 349 |
| IR | 1.32 | 2.12 | 5.74 | 8.53 | 7.68 | 10.17 | 11.67 | 21.97 | 13.34 | 24.18 |
| Crude HR | 0.59 | 1.00 | 0.67 | 1.00 | 0.73 | 1.00 | 0.53 | 1.00 | 0.55 | 1.00 |
| (95% CI) | (0.32–1.07) | (0.48–0.95) | (0.50–1.07) | (0.31–0.92) | (0.20–1.50) | |||||
| Ad HR1 | 0.60 | 1.00 | 0.66 | 1.00 | 0.74 | 1.00 | 0.60 | 1.00 | 0.52 | 1.00 |
| (95% CI) | (0.32–1.13) | (0.46–0.94) | (0.50–1.09) | (0.341–1.044) | (0.18–1.48) | |||||
| Ad HR2 | 0.68 | 1.00 | 0.85 | 1.00 | 1.06 | 1.00 | 0.62 | 1.00 | 0.94 | 1.00 |
| (95% CI) | (0.29–1.61) | (0.57–1.25) | (0.65–1.73) | (0.30–1.25) | (0.18–4.93) | |||||
| CKD | Total (n = 366) | Endometrioses (n = 146) | Controls (n = 220) | p-Value |
|---|---|---|---|---|
| Age (years) | ||||
| Mean ± SD | 50.6 ± 11.1 | 50.2 ± 10.8 | 50.8 ± 11.4 | 0.6367 |
| Median (Min–Max) | 49.5 (19–82) | 49.5 (19–81) | 49.5 (20–82) | |
| Interval (years) | ||||
| Mean ± SD | 6.53 ± 4.50 | 7.58 ± 4.03 | 5.83 ± 4.67 | 0.0002 |
| Median (Min–Max) | 6.47 (0–15.29) | 7.45 (0.13–15.29) | 5.86 (0–14.97) | |
| All Women | Total (n = 55,946) | Endometrioses (n = 27,973) | Controls (n = 27,973) | p-Value |
|---|---|---|---|---|
| Age (years) | ||||
| Mean ± SD | 41.6 ± 11.5 | 41.6 ± 11.5 | 41.6 ± 11.6 | 0.8205 |
| Median (Min–Max) | 42.0 (16–97) | 42.0 (16–94) | 42.0 (16–97) | |
| Interval (years) | ||||
| Mean ± SD | 11.231 ± 4.11 | 11.24 ± 4.10 | 11.22 ± 4.12 | 0.4780 |
| Median (Min–Max) | 12.91 (0–15.29) | 12.91 (0.01–15.29) | 12.92 (0–15.16) | |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, B.-S.; Chang, W.-H.; Wang, K.-C.; Huang, N.; Guo, C.-Y.; Chou, Y.-J.; Huang, H.-Y.; Chen, T.-J.; Lee, W.-L.; Wang, P.-H. Endometriosis Might Be Inversely Associated with Developing Chronic Kidney Disease: A Population-Based Cohort Study in Taiwan. Int. J. Mol. Sci. 2016, 17, 1079. https://doi.org/10.3390/ijms17071079
Huang B-S, Chang W-H, Wang K-C, Huang N, Guo C-Y, Chou Y-J, Huang H-Y, Chen T-J, Lee W-L, Wang P-H. Endometriosis Might Be Inversely Associated with Developing Chronic Kidney Disease: A Population-Based Cohort Study in Taiwan. International Journal of Molecular Sciences. 2016; 17(7):1079. https://doi.org/10.3390/ijms17071079
Chicago/Turabian StyleHuang, Ben-Shian, Wen-Hsun Chang, Kuan-Chin Wang, Nicole Huang, Chao-Yu Guo, Yiing-Jen Chou, Hsin-Yi Huang, Tzeng-Ji Chen, Wen-Ling Lee, and Peng-Hui Wang. 2016. "Endometriosis Might Be Inversely Associated with Developing Chronic Kidney Disease: A Population-Based Cohort Study in Taiwan" International Journal of Molecular Sciences 17, no. 7: 1079. https://doi.org/10.3390/ijms17071079