
Common Genetic Variation in CYP17A1 and Response to Abiraterone Acetate in Patients with Metastatic Castration-Resistant Prostate Cancer

 ,
,
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Cohort and Clinical Data
4.2. Genetic Data
4.3. Outcomes
4.4. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2016. CA Cancer J. Clin. 2016, 66, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Huggins, C. Effect of orchiectomy and irradiation on cancer of the prostate. Ann. Surg. 1942, 115, 1192–1200. [Google Scholar] [CrossRef] [PubMed]
- Huggins, C. Prostatic cancer treated by orchiectomy; the five year results. J. Am. Med. Assoc. 1946, 131, 576–581. [Google Scholar] [CrossRef] [PubMed]
- Huggins, C.; Hodges, C.V. Studies on prostatic cancer: I. The effect of castration, of estrogen and of androgen injection on serum phosphatases in metastatic carcinoma of the prostate. 1941. J. Urol. 2002, 168, 9–12. [Google Scholar] [CrossRef]
- Crawford, E.D.; Eisenberger, M.A.; McLeod, D.G.; Spaulding, J.T.; Benson, R.; Dorr, F.A.; Blumenstein, B.A.; Davis, M.A.; Goodman, P.J. A controlled trial of leuprolide with and without flutamide in prostatic carcinoma. N. Engl. J. Med. 1989, 321, 419–424. [Google Scholar] [CrossRef] [PubMed]
- Eisenberger, M.A.; Blumenstein, B.A.; Crawford, E.D.; Miller, G.; McLeod, D.G.; Loehrer, P.J.; Wilding, G.; Sears, K.; Culkin, D.J.; Thompson, I.M.; et al. Bilateral orchiectomy with or without flutamide for metastatic prostate cancer. N. Engl. J. Med. 1998, 339, 1036–1042. [Google Scholar] [CrossRef] [PubMed]
- Denis, L.J.; Keuppens, F.; Smith, P.H.; Whelan, P.; de Moura, J.L.; Newling, D.; Bono, A.; Sylvester, R. Maximal androgen blockade: Final analysis of eortc phase iii trial 30853. Eortc genito-urinary tract cancer cooperative group and the eortc data center. Eur. Urol. 1998, 33, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Prostate Cancer Trialists’ Collaborative Group. Maximum androgen blockade in advanced prostate cancer: An overview of the randomised trials. Lancet 2000, 355, 1491–1498. [Google Scholar]
- Kantoff, P.W.; Higano, C.S.; Shore, N.D.; Berger, E.R.; Small, E.J.; Penson, D.F.; Redfern, C.H.; Ferrari, A.C.; Dreicer, R.; Sims, R.B.; et al. Sipuleucel-T immunotherapy for castration-resistant prostate cancer. N. Engl. J. Med. 2010, 363, 411–422. [Google Scholar] [CrossRef] [PubMed]
- Fizazi, K.; Scher, H.I.; Molina, A.; Logothetis, C.J.; Chi, K.N.; Jones, R.J.; Staffurth, J.N.; North, S.; Vogelzang, N.J.; Saad, F.; et al. Abiraterone acetate for treatment of metastatic castration-resistant prostate cancer: Final overall survival analysis of the COU-AA-301 randomised, double-blind, placebo-controlled phase 3 study. Lancet Oncol. 2012, 13, 983–992. [Google Scholar] [CrossRef]
- Scher, H.I.; Fizazi, K.; Saad, F.; Taplin, M.-E.; Sternberg, C.N.; Miller, K.; de Wit, R.; Mulders, P.; Chi, K.N.; Shore, N.D.; et al. Increased survival with enzalutamide in prostate cancer after chemotherapy. N. Engl. J. Med. 2012, 367, 1187–1197. [Google Scholar] [PubMed]
- Beer, T.M.; Armstrong, A.J.; Rathkopf, D.E.; Loriot, Y.; Sternberg, C.N.; Higano, C.S.; Iversen, P.; Bhattacharya, S.; Carles, J.; Chowdhury, S.; et al. Enzalutamide in metastatic prostate cancer before chemotherapy. N. Engl. J. Med. 2014, 371, 424–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sartor, O.; Coleman, R.; Nilsson, S.; Heinrich, D.; Helle, S.I.; O’Sullivan, J.M.; Fosså, S.D.; Chodacki, A.; Wiechno, P.; Logue, J.; et al. Effect of radium-223 dichloride on symptomatic skeletal events in patients with castration-resistant prostate cancer and bone metastases: Results from a phase 3, double-blind, randomised trial. Lancet Oncol. 2014, 15, 738–746. [Google Scholar] [CrossRef]
- De Bono, J.S.; Logothetis, C.J.; Molina, A.; Fizazi, K.; North, S.; Chu, L.; Chi, K.N.; Jones, R.J.; Goodman, O.B.; Saad, F.; et al. Abiraterone and increased survival in metastatic prostate cancer. N. Engl. J. Med. 2011, 364, 1995–2005. [Google Scholar] [CrossRef] [PubMed]
- Ryan, C.J.; Smith, M.R.; de Bono, J.S.; Molina, A.; Logothetis, C.J.; de Souza, P.; Fizazi, K.; Mainwaring, P.; Piulats, J.M.; Ng, S.; et al. Abiraterone in metastatic prostate cancer without previous chemotherapy. N. Engl. J. Med. 2013, 368, 138–148. [Google Scholar] [CrossRef] [PubMed]
- Rathkopf, D.E.; Smith, M.R.; de Bono, J.S.; Logothetis, C.J.; Shore, N.D.; de Souza, P.; Fizazi, K.; Mulders, P.F.A.; Mainwaring, P.; Hainsworth, J.D.; et al. Updated interim efficacy analysis and long-term safety of abiraterone acetate in metastatic castration-resistant prostate cancer patients without prior chemotherapy (COU-AA-302). Eur. Urol. 2014, 66, 815–825. [Google Scholar] [CrossRef] [PubMed]
- Ryan, C.J.; Smith, M.R.; Fizazi, K.; Saad, F.; Mulders, P.F.A.; Sternberg, C.N.; Miller, K.; Logothetis, C.J.; Shore, N.D.; Small, E.J.; et al. Abiraterone acetate plus prednisone versus placebo plus prednisone in chemotherapy-naive men with metastatic castration-resistant prostate cancer (COU-AA-302): Final overall survival analysis of a randomised, double-blind, placebo-controlled phase 3 study. Lancet Oncol. 2015, 16, 152–160. [Google Scholar] [CrossRef]
- Miller, W.L.; Auchus, R.J. The molecular biology, biochemistry, and physiology of human steroidogenesis and its disorders. Endocr. Rev. 2011, 32, 81–151. [Google Scholar] [CrossRef] [PubMed]
- DeVore, N.M.; Scott, E.E. Structures of cytochrome p450 17a1 with prostate cancer drugs abiraterone and tok-001. Nature 2012, 482, 116–119. [Google Scholar] [CrossRef] [PubMed]
- Newton-Cheh, C.; Johnson, T.; Gateva, V.; Tobin, M.D.; Bochud, M.; Coin, L.; Najjar, S.S.; Zhao, J.H.; Heath, S.C.; Eyheramendy, S.; et al. Genome-wide association study identifies eight loci associated with blood pressure. Nat. Genet. 2009, 41, 666–676. [Google Scholar] [CrossRef] [PubMed]
- Levy, D.; Ehret, G.B.; Rice, K.; Verwoert, G.C.; Launer, L.J.; Dehghan, A.; Glazer, N.L.; Morrison, A.C.; Johnson, A.D.; Aspelund, T.; et al. Genome-wide association study of blood pressure and hypertension. Nat. Genet. 2009, 41, 677–687. [Google Scholar] [CrossRef] [PubMed]
- Ehret, G.B.; Munroe, P.B.; Rice, K.M.; Bochud, M.; Johnson, A.D.; Chasman, D.I.; Smith, A.V.; Tobin, M.D.; Verwoert, G.C.; Hwang, S.-J.; et al. Genetic variants in novel pathways influence blood pressure and cardiovascular disease risk. Nature 2011, 478, 103–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Attard, G.; Reid, A.H.M.; Olmos, D.; de Bono, J.S. Antitumor activity with CYP17 blockade indicates that castration-resistant prostate cancer frequently remains hormone driven. Cancer Res. 2009, 69, 4937–4940. [Google Scholar] [CrossRef] [PubMed]
- Beuten, J.; Gelfond, J.A.L.; Franke, J.L.; Weldon, K.S.; Crandall, A.C.; Johnson-Pais, T.L.; Thompson, I.M.; Leach, R.J. Single and multigenic analysis of the association between variants in 12 steroid hormone metabolism genes and risk of prostate cancer. Cancer Epidemiol. Biomark. Prev. 2009, 18, 1869–1880. [Google Scholar] [CrossRef] [PubMed]
- Setiawan, V.W.; Schumacher, F.R.; Haiman, C.A.; Stram, D.O.; Albanes, D.; Altshuler, D.; Berglund, G.; Buring, J.; Calle, E.E.; Clavel-Chapelon, F.; et al. CYP17 genetic variation and risk of breast and prostate cancer from the national cancer institute breast and prostate cancer cohort consortium (BPC3). Cancer Epidemiol. Biomark. Prev. 2007, 16, 2237–2246. [Google Scholar] [CrossRef] [PubMed]
- Lindström, S.; Wiklund, F.; Adami, H.-O.; Bälter, K.A.; Adolfsson, J.; Grönberg, H. Germ-line genetic variation in the key androgen-regulating genes androgen receptor, cytochrome p450, and steroid-5-α-reductase type 2 is important for prostate cancer development. Cancer Res. 2006, 66, 11077–11083. [Google Scholar] [CrossRef] [PubMed]
- Lindström, S.; Adami, H.-O.; Bälter, K.A.; Xu, J.; Zheng, S.L.; Stattin, P.; Grönberg, H.; Wiklund, F. Inherited variation in hormone-regulating genes and prostate cancer survival. Clin. Cancer Res. 2007, 13, 5156–5161. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Zou, Y.-F.; Feng, X.-L.; Su, H.; Huang, F. CYP17 gene polymorphisms and prostate cancer risk: A meta-analysis based on 38 independent studies. Prostate 2011, 71, 1167–1177. [Google Scholar] [CrossRef] [PubMed]
- Mostaghel, E.A.; Marck, B.T.; Plymate, S.R.; Vessella, R.L.; Balk, S.; Matsumoto, A.M.; Nelson, P.S.; Montgomery, R.B. Resistance to CYP17A1 inhibition with abiraterone in castration-resistant prostate cancer: Induction of steroidogenesis and androgen receptor splice variants. Clin. Cancer Res. 2011, 17, 5913–5925. [Google Scholar] [CrossRef] [PubMed]
- Fizazi, K.; Flaig, T.W.; Stöckle, M.; Scher, H.I.; de Bono, J.S.; Rathkopf, D.E.; Ryan, C.J.; Kheoh, T.; Li, J.; Todd, M.B.; et al. Does gleason score at initial diagnosis predict efficacy of abiraterone acetate therapy in patients with metastatic castration-resistant prostate cancer? An analysis of abiraterone acetate phase iii trials. Ann. Oncol. 2016, 27, 699–705. [Google Scholar] [CrossRef] [PubMed]
- Bellmunt, J.; Kheoh, T.; Yu, M.K.; Smith, M.R.; Small, E.J.; Mulders, P.F.A.; Fizazi, K.; Rathkopf, D.E.; Saad, F.; Scher, H.I.; et al. Prior endocrine therapy impact on abiraterone acetate clinical efficacy in metastatic castration-resistant prostate cancer: Post-hoc analysis of randomised phase 3 studies. Eur. Urol. 2015, 69, 924–932. [Google Scholar] [CrossRef] [PubMed]
- Davies, R.S.; Smith, C.; Button, M.R.; Tanguay, J.; Barber, J.; Palaniappan, N.; Staffurth, J.; Lester, J.F. What predicts minimal response to abiraterone in metastatic castrate-resistant prostate cancer? Anticancer Res. 2015, 35, 5615–5621. [Google Scholar] [PubMed]
- Diver, L.A.; MacKenzie, S.M.; Fraser, R.; McManus, F.; Freel, E.M.; Alvarez-Madrazo, S.; McClure, J.D.; Friel, E.C.; Hanley, N.A.; Dominiczak, A.F.; et al. Common polymorphisms at the CYP17A1 locus associate with steroid phenotype: Support for blood pressure genome-wide association study signals at this locus. Hypertension 2016, 67, 724–732. [Google Scholar] [CrossRef] [PubMed]
- Iversen, A.; Thune, I.; McTiernan, A.; Makar, K.W.; Wilsgaard, T.; Ellison, P.T.; Jasienska, G.; Flote, V.; Poole, E.M.; Furberg, A.-S. Genetic polymorphism CYP17 rs2486758 and metabolic risk factors predict daily salivary 17β-estradiol concentration in healthy premenopausal norwegian women. The EBBA-I study. J. Clin. Endocrinol. Metab. 2012, 97, E852–E857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salvi, S.; Casadio, V.; Conteduca, V.; Burgio, S.L.; Menna, C.; Bianchi, E.; Rossi, L.; Carretta, E.; Masini, C.; Amadori, D.; et al. Circulating cell-free ar and CYP17A1 copy number variations may associate with outcome of metastatic castration-resistant prostate cancer patients treated with abiraterone. Br. J. Cancer 2015, 112, 1717–1724. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, N.; Alex, A.B.; Farnham, J.M.; Patel, S.; Gill, D.; Buckley, T.H.; Stephenson, R.A.; Cannon-Albright, L. Inherited variants in sult1e1 and response to abiraterone acetate in men with metastatic castration refractory prostate cancer (mCRPC). J. Urol. 2016. [Google Scholar] [CrossRef] [PubMed]
- Antonarakis, E.S.; Lu, C.; Wang, H.; Luber, B.; Nakazawa, M.; Roeser, J.C.; Chen, Y.; Mohammad, T.A.; Chen, Y.; Fedor, H.L.; et al. AR-V7 and resistance to enzalutamide and abiraterone in prostate cancer. N. Engl. J. Med. 2014, 371, 1028–1038. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, T.; Okuno, Y.; Hattori-Kato, M.; Zaitsu, M.; Mikami, K. Detection of AR-V7 mrna in whole blood may not predict the effectiveness of novel endocrine drugs for castration-resistant prostate cancer. Res. Rep. Urol. 2016, 8, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Kohli, M.; Riska, S.M.; Mahoney, D.W.; Chai, H.S.; Hillman, D.W.; Rider, D.N.; Costello, B.A.; Qin, R.; Lamba, J.; Sahasrabudhe, D.M.; et al. Germline predictors of androgen deprivation therapy response in advanced prostate cancer. Mayo Clin. Proc. 2012, 87, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Xia, S.; Kohli, M.; Du, M.; Dittmar, R.L.; Lee, A.; Nandy, D.; Yuan, T.; Guo, Y.; Wang, Y.; Tschannen, M.R.; et al. Plasma genetic and genomic abnormalities predict treatment response and clinical outcome in advanced prostate cancer. Oncotarget 2015, 6, 16411–16421. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Yuan, T.; Liang, M.; Du, M.; Xia, S.; Dittmar, R.; Wang, D.; See, W.; Costello, B.A.; Quevedo, F.; et al. Exosomal miR-1290 and miR-375 as prognostic markers in castration-resistant prostate cancer. Eur. Urol. 2015, 67, 33–41. [Google Scholar] [CrossRef] [PubMed]
- De Bakker, P.I.W.; Yelensky, R.; Pe'er, I.; Gabriel, S.B.; Daly, M.J.; Altshuler, D. Efficiency and power in genetic association studies. Nat. Genet. 2005, 37, 1217–1223. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Willer, C.J.; Ding, J.; Scheet, P.; Abecasis, G.R. Mach: Using sequence and genotype data to estimate haplotypes and unobserved genotypes. Genet. Epidemiol. 2010, 34, 816–834. [Google Scholar] [CrossRef] [PubMed]
- International HapMap Consortium. The international hapmap project. Nature 2003, 426, 789–796. [Google Scholar]
- Kaplan, E.L.; Meier, P. Nonparametric estimation from incomplete observations. J. Am. Stat. Assoc. 1958, 53, 457–481. [Google Scholar] [CrossRef]
- Cox, D.R. Regression models and life-tables. J. R. Stat. Soc. B 1972, 34, 187–220. [Google Scholar]
- Aulchenko, Y.S.; Struchalin, M.V.; van Duijn, C.M. Probabel package for genome-wide association analysis of imputed data. BMC Bioinform. 2010, 11, 134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, X.; Starmer, J.; Martin, E.R. A multiple testing correction method for genetic association studies using correlated single nucleotide polymorphisms. Genet. Epidemiol. 2008, 32, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Becker, L.C.; Becker, D.M.; Starmer, J.D.; Province, M.A. Avoiding the high bonferroni penalty in genome-wide association studies. Genet. Epidemiol. 2010, 34, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Gao, X. Multiple testing corrections for imputed snps. Genet. Epidemiol. 2011, 35, 154–158. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Demographics at the Time of Initial Prostate Cancer Diagnosis | |
|---|---|
| Median age (years) | 64 (43–89) |
| Median prostate-specific antigen (ng/dL) | 7 (0–3229) |
| Stage | |
| T1–T2b | 24 (28%) |
| T2c | 25 (29%) |
| T3+ | 38 (43%) |
| N+ | 23 (38%) |
| M+ | 18 (56%) |
| Gleason grade | |
| 5–6 | 11 (13%) |
| 7 | 27 (31%) |
| 8–10 | 49 (56%) |
| Radical prostatectomy | 51 (71%) |
| Patient Characteristics at the Time of Initiation of Abiraterone Acetate and Prednisone for Castration-Resistant Stage | |
| Median age (years) | 73 (54–90) |
| Median prostate-specific antigen (ng/dL) | 66 (0–100) |
| Median body mass index (kg/m2) | 30 (21–56) |
| Bone metastases | 73 (84%) |
| Soft tissue metastases | 43 (49%) |
| Previous androgen-deprivation therapy | 87 (100%) |
| Previous docetaxel | 56 (65%) |
| Previous enzalutamide | 5 (6%) |
| Previous cabazitaxel | 5 (6%) |
| Time from initial diagnosis (years) | 8 (1–24) |
| Patients alive at the time of data analysis | 38 (44%) |
| SNP | n | Biochemical Response to Treatment | p | |
|---|---|---|---|---|
| Response Rates 1 | Effect Estimate | |||
| rs2486758 | 87 | 50%/17% | OR 0.22 (0.07–0.63) | 0.005 |
| rs4919685 | 87 | 38%/39% | OR 1.24 (0.64–2.40) | 0.524 |
| rs17115100 | 87 | 40%/37% | OR 0.82 (0.31–2.19) | 0.689 |
| rs743572 | 87 | 33%/40% | OR 1.13 (0.58–2.20) | 0.718 |
| Time to Biochemical Progression | ||||
| Median Time to Progression 1 | Effect Estimate | |||
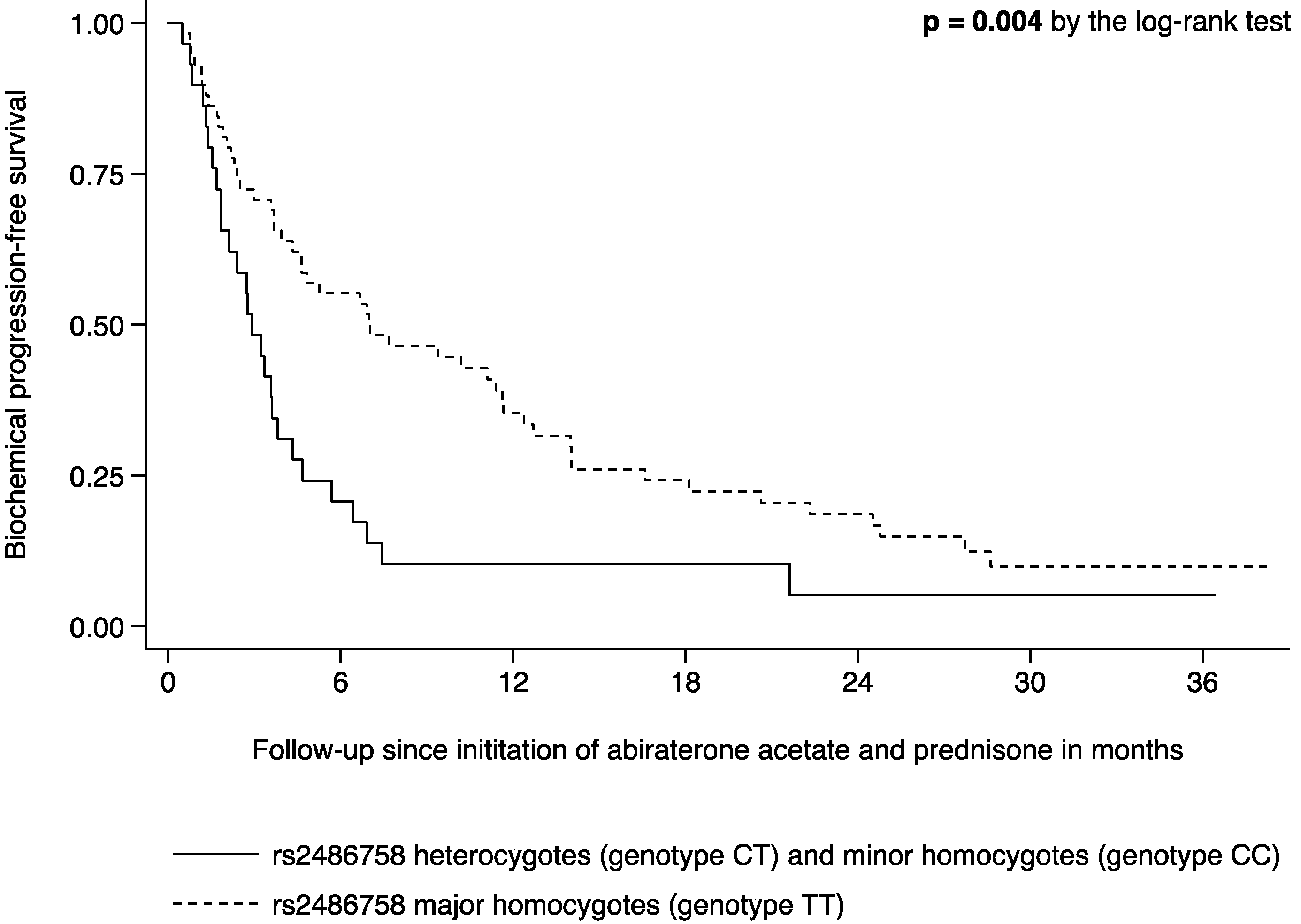
| rs2486758 | 87 | 7.0 months/2.9 months | HR 2.23 (1.39–3.56) | <0.001 |
| rs4919685 | 87 | 3.5 months/4.6 months | HR 0.82 (0.47–1.42) | 0.429 |
| rs17115100 | 87 | 4.5 months/5.3 months | HR 0.95 (0.67–1.35) | 0.693 |
| rs743572 | 87 | 3.5 months/4.6 months | HR 1.03 (0.73–1.46) | 0.889 |
| Model | n | Response to Treatment | p |
|---|---|---|---|
| Unadjusted | 87 | OR 0.22 (0.07–0.63) | 0.005 |
| Age-adjusted (I) | 87 | OR 0.21 (0.07–0.62) | 0.005 |
| Multivariable-adjusted (II) | 87 | OR 0.22 (0.07–0.63) | 0.005 |
| Multivariable-adjusted (III) | 87 | OR 0.21 (0.07–0.62) | 0.005 |
| Multivariable-adjusted (IV) | 87 | OR 0.18 (0.06–0.57) | 0.003 |
| Time to Progression | |||
| Unadjusted | 87 | HR 2.23 (1.39–3.56) | <0.001 |
| Age-adjusted (I) | 87 | HR 2.22 (1.40–3.55) | 0.001 |
| Multivariable-adjusted (II) | 87 | HR 2.26 (1.41–3.62) | 0.001 |
| Multivariable-adjusted (III) | 87 | HR 2.29 (1.43–3.67) | 0.001 |
| Multivariable-adjusted (IV) | 87 | HR 2.67 (1.64–4.36) | <0.001 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Binder, M.; Zhang, B.Y.; Hillman, D.W.; Kohli, R.; Kohli, T.; Lee, A.; Kohli, M. Common Genetic Variation in CYP17A1 and Response to Abiraterone Acetate in Patients with Metastatic Castration-Resistant Prostate Cancer. Int. J. Mol. Sci. 2016, 17, 1097. https://doi.org/10.3390/ijms17071097
Binder M, Zhang BY, Hillman DW, Kohli R, Kohli T, Lee A, Kohli M. Common Genetic Variation in CYP17A1 and Response to Abiraterone Acetate in Patients with Metastatic Castration-Resistant Prostate Cancer. International Journal of Molecular Sciences. 2016; 17(7):1097. https://doi.org/10.3390/ijms17071097
Chicago/Turabian StyleBinder, Moritz, Ben Y. Zhang, David W. Hillman, Rhea Kohli, Tanvi Kohli, Adam Lee, and Manish Kohli. 2016. "Common Genetic Variation in CYP17A1 and Response to Abiraterone Acetate in Patients with Metastatic Castration-Resistant Prostate Cancer" International Journal of Molecular Sciences 17, no. 7: 1097. https://doi.org/10.3390/ijms17071097