
Radiation-Induced Organizing Pneumonia: A Characteristic Disease that Requires Symptom-Oriented Management


{kind=link}
Abstract
:1. Introduction
2. Diagnosis
2.1. Partial Irradiation Involving the Lung Occurring Approximately within 12 Months
2.2. Lung Infiltrates Outside the High Irradiation Dose Area
2.3. No Other Specific Cause
3. Pathogenesis and Epidemiology
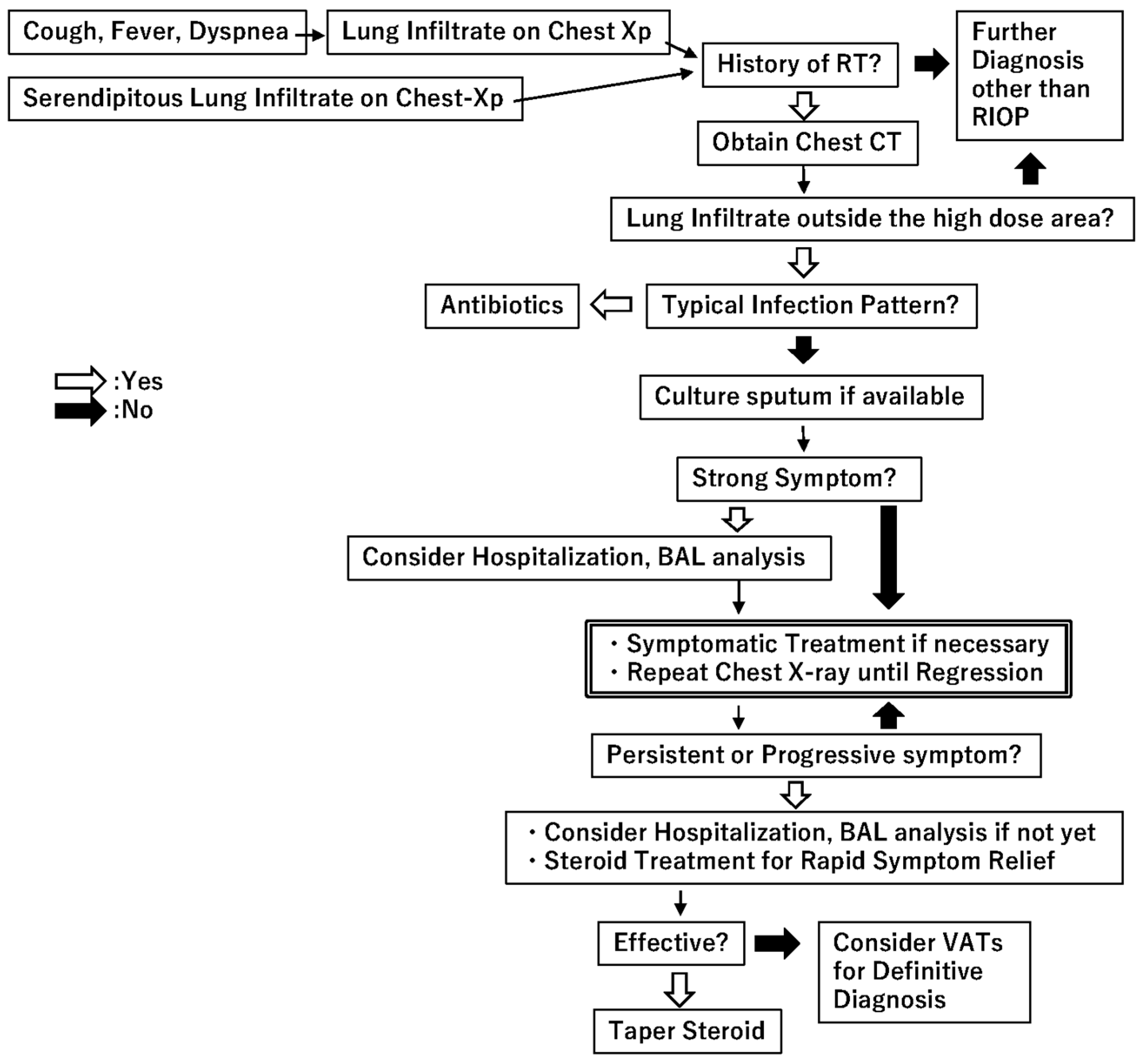
4. Patient Management
5. Conclusions
Conflicts of Interest
Abbreviations
| RIOP | Radiation-induced organizing pneumonia |
| OP | Organizing pneumonia |
| COP | Cryptogenic organizing pneumonia |
| SOP | Secondary organizing pneumonia |
| BOOP | Bronchiolitis obliterans organizing pneumonia |
| SBRT | Stereotactic body radiotherapy |
| CT | Computed tomography |
| BAL | Bronchoalveolar lavage |
| CEP | Chronic eosinophilic pneumonia |
| ATM | Ataxia telangiectasia mutated |
| TGF-β | Transforming growth factor-β |
References
- American Thoracic Society/European Respiratory Society International Multidisciplinary Consensus Classification of the Idiopathic Interstitial Pneumonias. This joint statement of the American Thoracic Society (ATS), and the European Respiratory Society (ERS) was adopted by the ATS board of directors, June 2001 and by the ERS Executive Committee, June 2001. Am. J. Respir. Crit. Care Med. 2002, 165, 277–304. [Google Scholar]
- Vasu, T.S.; Cavallazzi, R.; Hirani, A.; Sharma, D.; Weibel, S.B.; Kane, G.C. Clinical and radiologic distinctions between secondary bronchiolitis obliterans organizing pneumonia and cryptogenic organizing pneumonia. Respir. Care 2009, 54, 1028–1032. [Google Scholar] [PubMed]
- Crestani, B.; Kambouchner, M.; Soler, P.; Crequit, J.; Brauner, M.; Battesti, J.P.; Valeyre, D. Migratory bronchiolitis obliterans organizing pneumonia after unilateral radiation therapy for breast carcinoma. Eur. Respir. J. 1995, 8, 318–321. [Google Scholar] [CrossRef] [PubMed]
- Bayle, J.Y.; Nesme, P.; Bejui-Thivolet, F.; Loire, R.; Guerin, J.C.; Cordier, J.F. Migratory organizing pneumonitis “primed” by radiation therapy. Eur. Respir. J. 1995, 8, 322–326. [Google Scholar] [CrossRef] [PubMed]
- Otani, K.; Nishiyama, K.; Ito, Y.; Kawaguchi, Y.; Inaji, H. Steroid treatment increases the recurrence of radiation-induced organizing pneumonia after breast-conserving therapy. Cancer Med. 2014, 3, 947–953. [Google Scholar] [CrossRef] [PubMed]
- Takigawa, N.; Segawa, Y.; Saeki, T.; Kataoka, M.; Ida, M.; Kishino, D.; Fujiwara, K.; Ohsumi, S.; Eguchi, K.; Takashima, S. Bronchiolitis obliterans organizing pneumonia syndrome in breast-conserving therapy for early breast cancer: Radiation-induced lung toxicity. Int. J. Radiat. Oncol. Biol. Phys. 2000, 48, 751–755. [Google Scholar] [CrossRef]
- Miwa, S.; Morita, S.; Suda, T.; Suzuki, K.; Hayakawa, H.; Chida, K.; Nakamura, H. The incidence and clinical characteristics of bronchiolitis obliterans organizing pneumonia syndrome after radiation therapy for breast cancer. Sarcoidosis Vasc. Diffuse Lung Dis. 2004, 21, 212–218. [Google Scholar] [PubMed]
- Ogo, E.; Komaki, R.; Fujimoto, K.; Uchida, M.; Abe, T.; Nakamura, K.; Mitsumori, M.; Sekiguchi, K.; Kaneyasu, Y.; Hayabuchi, N. A survey of radiation-induced bronchiolitis obliterans organizing pneumonia syndrome after breast-conserving therapy in Japan. Int. J. Radiat. Oncol. Biol. Phys. 2008, 71, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Kubo, A.; Osaki, K.; Kawanaka, T.; Furutani, S.; Ikushima, H.; Nishitani, H. Risk factors for radiation pneumonitis caused by whole breast irradiation following breast-conserving surgery. J. Med. Investig. 2009, 56, 99–110. [Google Scholar] [CrossRef]
- Ogo, E.; Komaki, R.; Abe, T.; Uchida, M.; Fujimoto, K.; Suzuki, G.; Tsuji, C.; Suefuji, H.; Etou, H.; Hattori, C.; et al. The clinical characteristics and non-steroidal treatment for radiation-induced bronchiolitis obliterans organizing pneumonia syndrome after breast-conserving therapy. Radiother. Oncol. 2010, 97, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Katayama, N.; Sato, S.; Katsui, K.; Takemoto, M.; Tsuda, T.; Yoshida, A.; Morito, T.; Nakagawa, T.; Mizuta, A.; Waki, T.; et al. Analysis of factors associated with radiation-induced bronchiolitis obliterans organizing pneumonia syndrome after breast-conserving therapy. Int. J. Radiat. Oncol. Biol. Phys. 2009, 73, 1049–1054. [Google Scholar] [CrossRef] [PubMed]
- Okada, Y.; Sakamoto, S.; Abe, T.; Shinozaki, M.; Gomi, H.; Kanemaki, Y.; Matsuoka, S.; Nakajima, Y. Factors Predicting the Relapse of Radiation-Induced Organizing Pneumonia after Breast-Conserving Therapy. Open J. Radiol. 2015, 5, 159–169. [Google Scholar] [CrossRef]
- Epler, G.R.; Kelly, E.M. Systematic review of postradiotherapy bronchiolitis obliterans organizing pneumonia in women with breast cancer. Oncologist 2014, 19, 1216–1226. [Google Scholar] [CrossRef] [PubMed]
- Epler, G.R. Bronchiolitis obliterans organizing pneumonia, 25 years: A variety of causes, but what are the treatment options? Expert Rev. Respir. Med. 2011, 5, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.J.; King, T.E., Jr.; Downey, G.P. Rapidly progressive bronchiolitis obliterans with organizing pneumonia. Am. J. Respir. Crit. Care Med. 1994, 149, 1670–1675. [Google Scholar] [CrossRef] [PubMed]
- Lohr, R.H.; Boland, B.J.; Douglas, W.W.; Dockrell, D.H.; Colby, T.V.; Swensen, S.J.; Wollan, P.C.; Silverstein, M.D. Organizing pneumonia: Features and prognosis of cryptogenic, secondary, and focal variants. Arch. Intern. Med. 1997, 157, 1323–1329. [Google Scholar] [CrossRef] [PubMed]
- Crestani, B.; Valeyre, D.; Roden, S.; Wallaert, B.; Dalphin, J.C.; Cordier, J.F. Bronchiolitis obliterans organizing pneumonia syndrome primed by radiation therapy to the breast. The Groupe d’Etudes et de Recherche sur les Maladies Orphelines Pulmonaires (GERM”O”P). Am. J. Respir. Crit. Care Med. 1998, 158, 1929–1935. [Google Scholar] [CrossRef] [PubMed]
- Stover, D.E.; Milite, F.; Zakowski, M. A newly recognized syndrome—Radiation-related bronchiolitis obliterans and organizing pneumonia. A case report and literature review. Respiration 2001, 68, 540–544. [Google Scholar] [CrossRef] [PubMed]
- Arbetter, K.R.; Prakash, U.B.; Tazelaar, H.D.; Douglas, W.W. Radiation-induced pneumonitis in the “nonirradiated” lung. Mayo Clin. Proc. 1999, 74, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Van Laar, J.M.; Holscher, H.C.; van Krieken, J.H.; Stolk, J. Bronchiolitis obliterans organizing pneumonia after adjuvant radiotherapy for breast carcinoma. Respir. Med. 1997, 91, 241–244. [Google Scholar] [CrossRef]
- Hamanishi, T.; Morimatu, T.; Oida, K.; Kori, Y.; Taguchi, Y.; Tanaka, E.; Inoue, T.; Kato, T.; Maniwa, K.; Kobashi, Y. Occurrence of BOOP outside radiation field after radiation therapy for small cell lung cancer. Nihon Kokyuki Gakkai Zasshi 2001, 39, 683–688. [Google Scholar] [PubMed]
- Iijima, M.; Sakahara, H. Radiation pneumonitis resembling bronchiolitis obliterans organizing pneumonia after postoperative irradiation for lung cancer: A case report. Nihon Igaku Hoshasen Gakkai Zasshi 2003, 63, 332–333. [Google Scholar] [PubMed]
- Kwok, E.; Chan, C.K. Corticosteroids and azathioprine do not prevent radiation-induced lung injury. Can. Respir. J. 1998, 5, 211–214. [Google Scholar] [CrossRef] [PubMed]
- Nogi, S.; Nakayama, H.; Tajima, Y.; Okubo, M.; Mikami, R.; Sugahara, S.; Akata, S.; Tokuuye, K. Cryptogenic organizing pneumonia associated with radiation: A report of two cases. Oncol. Lett. 2014, 7, 321–324. [Google Scholar] [PubMed]
- Falcinelli, L.; Bellavita, R.; Rebonato, A.; Chiari, R.; Vannucci, J.; Puma, F.; Aristei, C. Bronchiolitis obliterans organizing pneumonia after radiation therapy for lung cancer: A case report. Tumori 2015, 101, e88–e91. [Google Scholar] [CrossRef] [PubMed]
- Murai, T.; Shibamoto, Y.; Nishiyama, T.; Baba, F.; Miyakawa, A.; Ayakawa, S.; Ogino, H.; Otsuka, S.; Iwata, H. Organizing pneumonia after stereotactic ablative radiotherapy of the lung. Radiat. Oncol. 2012, 7, 123. [Google Scholar] [CrossRef] [PubMed]
- Ochiai, S.; Nomoto, Y.; Yamashita, Y.; Murashima, S.; Hasegawa, D.; Kurobe, Y.; Toyomasu, Y.; Kawamura, T.; Takada, A.; Noriko, I. Radiation-induced organizing pneumonia after stereotactic body radiotherapy for lung tumor. J. Radiat. Res. 2015, 56, 904–911. [Google Scholar] [CrossRef] [PubMed]
- Krengli, M.; Sacco, M.; Loi, G.; Masini, L.; Ferrante, D.; Gambaro, G.; Ronco, M.; Magnani, C.; Carriero, A. Pulmonary changes after radiotherapy for conservative treatment of breast cancer: A prospective study. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 1460–1467. [Google Scholar] [CrossRef] [PubMed]
- Cordier, J.-F. Cryptogenic organising pneumonia. Eur. Respir. J. 2006, 28, 422–446. [Google Scholar] [CrossRef] [PubMed]
- Majori, M.; Poletti, V.; Curti, A.; Corradi, M.; Falcone, F.; Pesci, A. Bronchoalveolar lavage in bronchiolitis obliterans organizing pneumonia primed by radiation therapy to the breast. J. Allergy Clin. Immunol. 2000, 105, 239–244. [Google Scholar] [CrossRef]
- Cottin, V.; Frognier, R.; Monnot, H.; Levy, A.; DeVuyst, P.; Cordier, J.F. Chronic eosinophilic pneumonia after radiation therapy for breast cancer. Eur. Respir. J. 2004, 23, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Cottin, V.; Cordier, J.-F. Cryptogenic organizing pneumonia. Semin. Respir. Crit. Care Med. 2012, 33, 462–475. [Google Scholar] [PubMed]
- Roberton, B.J.; Hansell, D.M. Organizing pneumonia: A kaleidoscope of concepts and morphologies. Eur. Radiol. 2011, 21, 2244–2254. [Google Scholar] [CrossRef] [PubMed]
- Beardsley, B.; Rassl, D. Fibrosing organising pneumonia. J. Clin. Path. 2013, 66, 875–881. [Google Scholar] [CrossRef] [PubMed]
- Izykowski, N.; Kuehnel, M.; Hussein, K.; Mitschke, K.; Gunn, M.; Janciauskiene, S.; Haverich, A.; Warnecke, G.; Laenger, F.; Maus, U. Organizing pneumonia in mice and men. J. Transl. Med. 2016, 14, 169. [Google Scholar] [CrossRef] [PubMed]
- Endlich, B.; Radford, I.R.; Forrester, H.B.; Dewey, W.C. Computerized video time-lapse microscopy studies of ionizing radiation-induced rapid-interphase and mitosis-related apoptosis in lymphoid cells. Radiat. Res. 2000, 153, 36–48. [Google Scholar] [CrossRef]
- Cordier, J.-F.; Cottin, V.; Lazor, R.; Stoppa-Lyonnet, D. Monoallelic germline ATM mutation and organising pneumonia induced by radiation therapy to the breast. Eur. Respir. J. 2016, 47, 997–1000. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Paull, T. Activation and regulation of ATM kinase activity in response to DNA double-strand breaks. Oncogene 2007, 26, 7741–7748. [Google Scholar] [CrossRef] [PubMed]
- Thompson, D.; Duedal, S.; Kirner, J.; McGuffog, L.; Last, J.; Reiman, A.; Byrd, P.; Taylor, M.; Easton, D.F. Cancer risks and mortality in heterozygous ATM mutation carriers. J. Natl. Cancer Inst. 2005, 97, 813–822. [Google Scholar] [CrossRef] [PubMed]
- Renwick, A.; Thompson, D.; Seal, S.; Kelly, P.; Chagtai, T.; Ahmed, M.; North, B.; Jayatilake, H.; Barfoot, R.; Spanova, K. ATM mutations that cause ataxia-telangiectasia are breast cancer susceptibility alleles. Nat. Genet. 2006, 38, 873–875. [Google Scholar] [CrossRef] [PubMed]
- Murofushi, K.N.; Oguchi, M.; Gosho, M.; Kozuka, T.; Sakurai, H. Radiation-induced bronchiolitis obliterans organizing pneumonia (BOOP) syndrome in breast cancer patients is associated with age. Radiat. Oncol. 2015, 10, 103. [Google Scholar] [CrossRef] [PubMed]
- Colletta, A.; Wakefield, L.; Howell, F.; Van Roozendaal, K.; Danielpour, D.; Ebbs, S.; Sporn, M.; Baum, M. Anti-oestrogens induce the secretion of active transforming growth factor β from human fetal fibroblasts. Br. J. Cancer 1990, 62, 405–409. [Google Scholar] [CrossRef] [PubMed]
- Bentzen, S.M.; Skoczylas, J.Z.; Overgaard, M.; Overgaard, J. Radiotherapy-related lung fibrosis enhanced by tamoxifen. J. Natl. Cancer Inst. 1996, 88, 918–922. [Google Scholar] [CrossRef] [PubMed]
- Huang, E.-Y.; Wang, C.-J.; Chen, H.-C.; Sun, L.-M.; Fang, F.-M.; Yeh, S.-A.; Hsu, H.-C.; Hsiung, C.-Y.; Wu, J.-M. Multivariate analysis of pulmonary fibrosis after electron beam irradiation for postmastectomy chest wall and regional lymphatics: Evidence for non-dosimetric factors. Radiother. Oncol. 2000, 57, 91–96. [Google Scholar] [CrossRef]
- Harris, E.E.; Christensen, V.J.; Hwang, W.-T.; Fox, K.; Solin, L.J. Impact of concurrent versus sequential tamoxifen with radiation therapy in early-stage breast cancer patients undergoing breast conservation treatment. J. Clin. Oncol. 2005, 23, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Pierce, L.J.; Hutchins, L.F.; Green, S.R.; Lew, D.L.; Gralow, J.R.; Livingston, R.B.; Osborne, C.K.; Albain, K.S. Sequencing of tamoxifen and radiotherapy after breast-conserving surgery in early-stage breast cancer. J. Clin. Oncol. 2005, 23, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Azria, D.; Belkacemi, Y.; Romieu, G.; Gourgou, S.; Gutowski, M.; Zaman, K.; Moscardo, C.L.; Lemanski, C.; Coelho, M.; Rosenstein, B. Concurrent or sequential adjuvant letrozole and radiotherapy after conservative surgery for early-stage breast cancer (CO-HO-RT): A phase 2 randomised trial. Lancet Oncol. 2010, 11, 258–265. [Google Scholar] [CrossRef]
- McEvoy, C.E.; Niewoehner, D.E. Adverse effects of corticosteroid therapy for COPD: A critical review. Chest 1997, 111, 732–743. [Google Scholar] [CrossRef] [PubMed]
- Rutz, H.P. Effects of corticosteroid use on treatment of solid tumours. Lancet 2002, 360, 1969–1970. [Google Scholar] [CrossRef]
- Vento, S.; Cainelli, F.; Temesgen, Z. Lung infections after cancer chemotherapy. Lancet Oncol. 2008, 9, 982–992. [Google Scholar] [CrossRef]
- Herr, I.; Pfitzenmaier, J. Glucocorticoid use in prostate cancer and other solid tumours: Implications for effectiveness of cytotoxic treatment and metastases. Lancet Oncol. 2006, 7, 425–430. [Google Scholar] [CrossRef]
- Zhang, C.; Kolb, A.; Mattern, J.; Gassler, N.; Wenger, T.; Herzer, K.; Debatin, K.; Büchler, M.; Friess, H.; Rittgen, W. Dexamethasone desensitizes hepatocellular and colorectal tumours toward cytotoxic therapy. Cancer Lett. 2006, 242, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Johkoh, T.; Muller, N.L.; Cartier, Y.; Kavanagh, P.V.; Hartman, T.E.; Akira, M.; Ichikado, K.; Ando, M.; Nakamura, H. Idiopathic Interstitial Pneumonias: Diagnostic Accuracy of Thin-Section CT in 129 Patients. Radiology 1999, 211, 555–560. [Google Scholar] [CrossRef] [PubMed]

© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Otani, K.; Seo, Y.; Ogawa, K. Radiation-Induced Organizing Pneumonia: A Characteristic Disease that Requires Symptom-Oriented Management. Int. J. Mol. Sci. 2017, 18, 281. https://doi.org/10.3390/ijms18020281
Otani K, Seo Y, Ogawa K. Radiation-Induced Organizing Pneumonia: A Characteristic Disease that Requires Symptom-Oriented Management. International Journal of Molecular Sciences. 2017; 18(2):281. https://doi.org/10.3390/ijms18020281
Chicago/Turabian StyleOtani, Keisuke, Yuji Seo, and Kazuhiko Ogawa. 2017. "Radiation-Induced Organizing Pneumonia: A Characteristic Disease that Requires Symptom-Oriented Management" International Journal of Molecular Sciences 18, no. 2: 281. https://doi.org/10.3390/ijms18020281