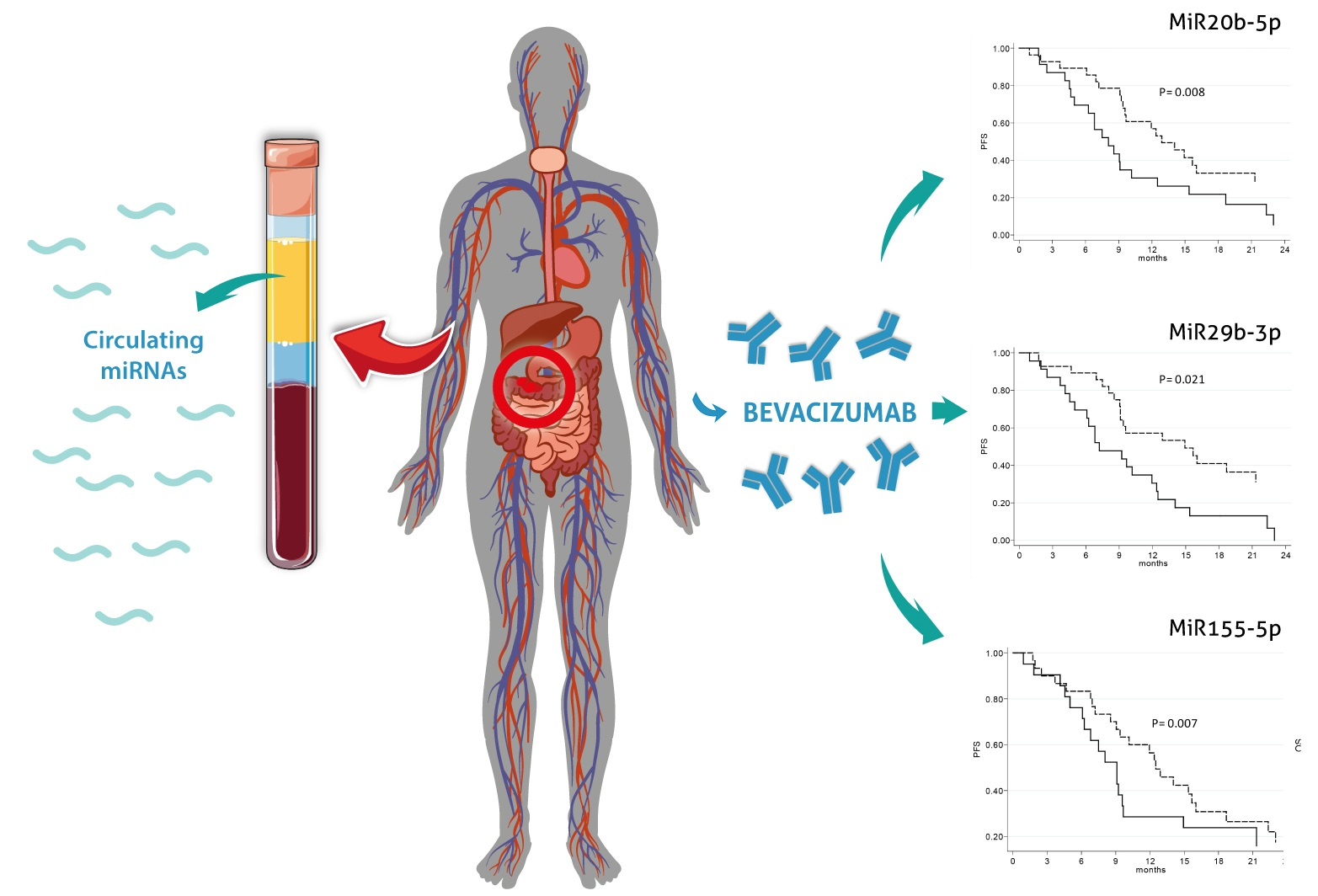
Circulating Plasma Levels of miR-20b, miR-29b and miR-155 as Predictors of Bevacizumab Efficacy in Patients with Metastatic Colorectal Cancer



 ,
,  ,
,
Abstract
:
1. Introduction
2. Results
2.1. Case Series
2.2. Baseline Circulating miRNAs in Relation to Clinical Pathological Characteristics of Patients
2.3. Response to Therapy and Prognosis in Relation to Clinical Pathological Characteristics of Patients
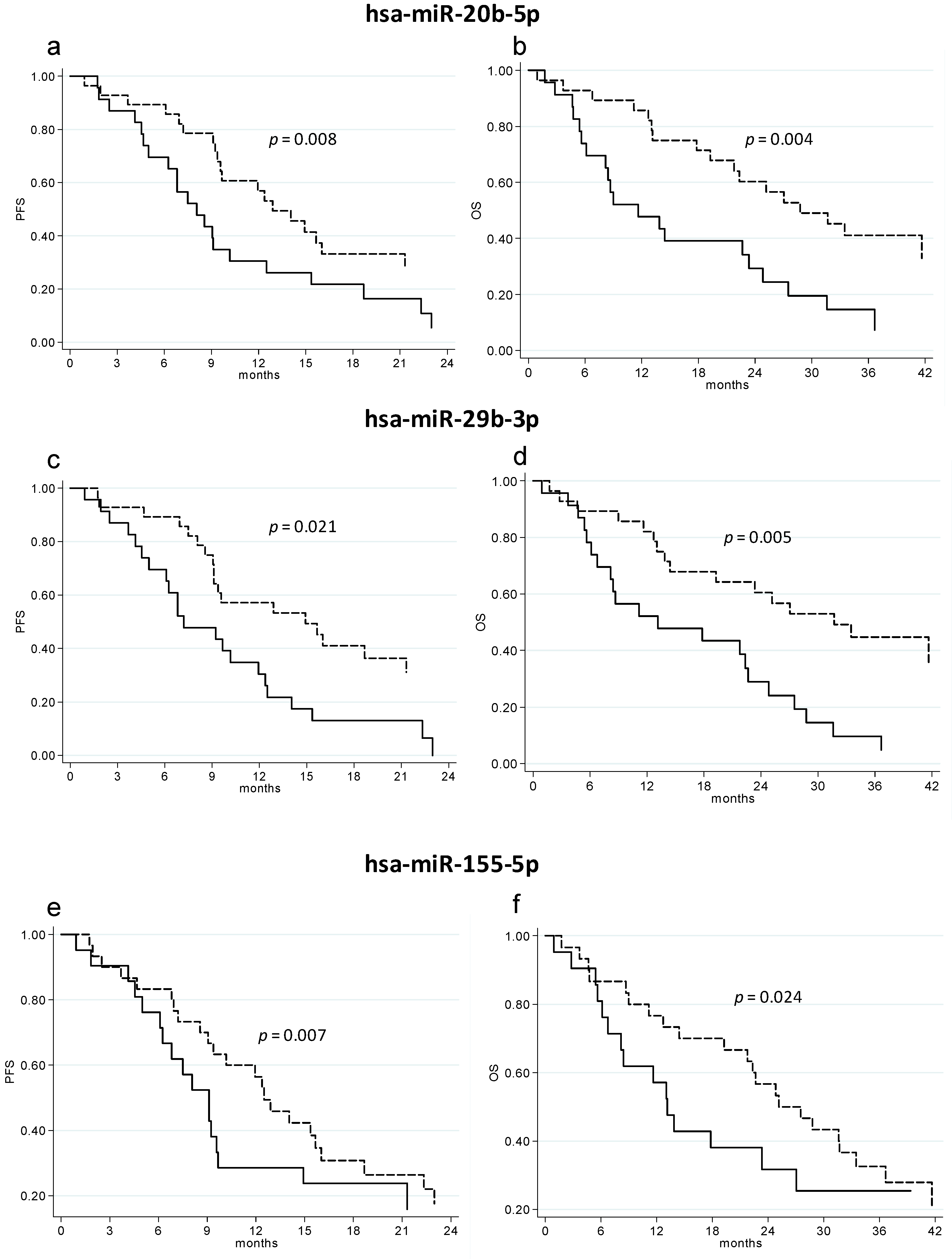
2.4. Baseline Circulating miRNAs in Relation to Response to Therapy and Patient Prognosis
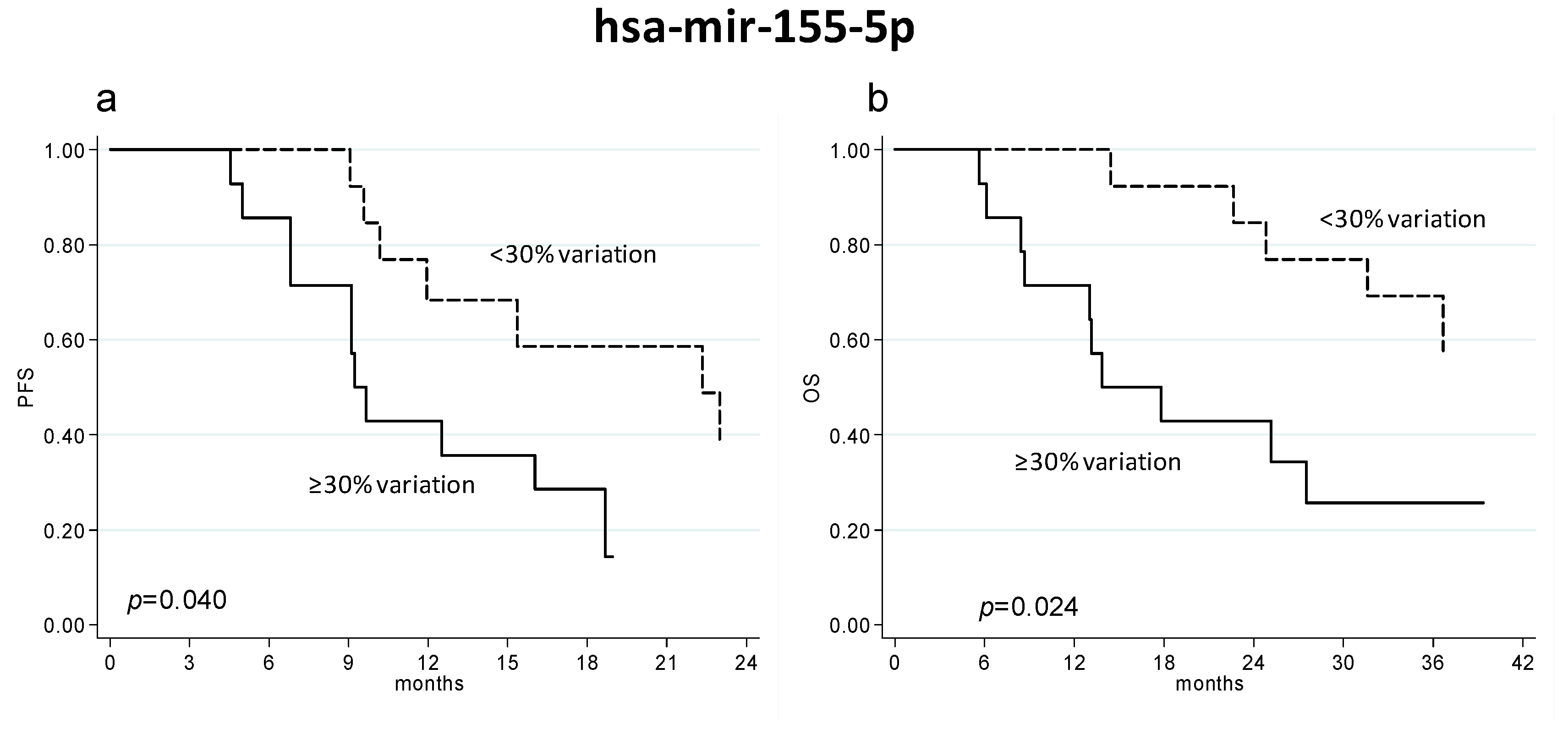
2.5. Circulating miRNAs’ Variations during Treatment in Relation to Patient Outcome
3. Discussion
4. Materials and Methods
4.1. Case Series
4.2. miRNA Selection
4.3. Circulating miRNA Expression Analysis
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| B | bevacizumab |
| CT | chemotherapy |
| eNOS | nitric oxide synthase |
| mCRC | metastatic colorectal cancer |
| miRNA | microRNA |
| MMP2 | metalloproteinase-2 |
| ORR | objective response rate |
| OS | overall survival |
| PFS | progression-free survival |
References
- Hochster, H.S.; Hart, L.L.; Ramanathan, R.K.; Childs, B.H.; Hainsworth, J.D.; Cohn, A.L.; Wong, L.; Fehrenbacher, L.; Abubakr, Y.; Saif, M.W.; et al. Safety and Efficacy of Oxaliplatin and Fluoropyrimidine Regimens with or without Bevacizumab as First-Line Treatment of Metastatic Colorectal Cancer: Results of the TREE Study. J. Clin. Oncol. 2008, 26, 3523–3529. [Google Scholar] [CrossRef] [PubMed]
- Saltz, L.B.; Clarke, S.; Diaz-Rubio, E.; Scheithauer, W.; Figer, A.; Wong, R.; Koski, S.; Lichinitser, M.; Yang, T.S.; Rivera, F.; et al. Bevacizumab in Combination with Oxaliplatin-Based Chemotherapy as First-Line Therapy in Metastatic Colorectal Cancer: A Randomized Phase III Study. J. Clin. Oncol. 2008, 26, 2013–2019. [Google Scholar] [CrossRef] [PubMed]
- Hurwitz, H.; Fehrenbacher, L.; Novotny, W.; Cartwright, T.; Hainsworth, J.; Heim, W.; Berlin, J.; Baron, A.; Griffing, S.; Holmgren, E.; et al. Bevacizumab Plus Irinotecan, Fluorouracil, and Leucovorin for Metastatic Colorectal Cancer. N. Engl. J. Med. 2004, 350, 2335–2342. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Vacarezza, N.; Alonso, I.; Arroyo, G.; Martinez, J.; De Andres, F.; LLerena, A.; Estevez-Carrizo, F. Predictive Biomarkers Candidates for Patients with Metastatic Colorectal Cancer Treated with Bevacizumab-Containing Regimen. Drug Metab. Pers. Ther. 2016, 31, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Marien, K.M.; Croons, V.; Martinet, W.; De Loof, H.; Ung, C.; Waelput, W.; Scherer, S.J.; Kockx, M.M.; De Meyer, G.R. Predictive Tissue Biomarkers for Bevacizumab-Containing Therapy in Metastatic Colorectal Cancer: An Update. Expert Rev. Mol. Diagn. 2015, 15, 399–414. [Google Scholar] [CrossRef] [PubMed]
- Cidon, E.U.; Alonso, P.; Masters, B. Markers of Response to Antiangiogenic Therapies in Colorectal Cancer: Where are we Now and what should be Next? Clin. Med. Insights Oncol. 2016, 10, 41–55. [Google Scholar] [CrossRef] [PubMed]
- Inamura, K.; Ishikawa, Y. MicroRNA in Lung Cancer: Novel Biomarkers and Potential Tools for Treatment. J. Clin. Med. 2016, 5. [Google Scholar] [CrossRef] [PubMed]
- Fish, J.E.; Santoro, M.M.; Morton, S.U.; Yu, S.; Yeh, R.F.; Wythe, J.D.; Ivey, K.N.; Bruneau, B.G.; Stainier, D.Y.; Srivastava, D. MiR-126 Regulates Angiogenic Signaling and Vascular Integrity. Dev. Cell. 2008, 15, 272–284. [Google Scholar] [CrossRef] [PubMed]
- Ota, T.; Doi, K.; Fujimoto, T.; Tanaka, Y.; Ogawa, M.; Matsuzaki, H.; Kuroki, M.; Miyamoto, S.; Shirasawa, S.; Tsunoda, T. KRAS Up-Regulates the Expression of miR-181a, miR-200c and miR-210 in a Three-Dimensional-Specific Manner in DLD-1 Colorectal Cancer Cells. Anticancer Res. 2012, 32, 2271–2275. [Google Scholar] [PubMed]
- Wang, X.; Wang, J.; Ma, H.; Zhang, J.; Zhou, X. Downregulation of miR-195 Correlates with Lymph Node Metastasis and Poor Prognosis in Colorectal Cancer. Med. Oncol. 2012, 29, 919–927. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.J.; Stratmann, J.; Zhou, Z.G.; Sun, X.F. Suppression of microRNA-31 Increases Sensitivity to 5-FU at an Early Stage, and Affects Cell Migration and Invasion in HCT-116 Colon Cancer Cells. BMC Cancer 2010, 10, 616. [Google Scholar] [CrossRef] [PubMed]
- Kanaan, Z.; Rai, S.N.; Eichenberger, M.R.; Barnes, C.; Dworkin, A.M.; Weller, C.; Cohen, E.; Roberts, H.; Keskey, B.; Petras, R.E.; et al. Differential microRNA Expression Tracks Neoplastic Progression in Inflammatory Bowel Disease-Associated Colorectal Cancer. Hum. Mutat. 2012, 33, 551–560. [Google Scholar] [CrossRef] [PubMed]
- Hur, K.; Toiyama, Y.; Takahashi, M.; Balaguer, F.; Nagasaka, T.; Koike, J.; Hemmi, H.; Koi, M.; Boland, C.R.; Goel, A. MicroRNA-200c Modulates Epithelial-to-Mesenchymal Transition (EMT) in Human Colorectal Cancer Metastasis. Gut 2013, 62, 1315–1326. [Google Scholar] [CrossRef] [PubMed]
- Xu, K.; Liang, X.; Shen, K.; Sun, L.; Cui, D.; Zhao, Y.; Tian, J.; Ni, L.; Liu, J. miR-222 Modulates Multidrug Resistance in Human Colorectal Carcinoma by Down-Regulating ADAM-17. Exp. Cell Res. 2012, 318, 2168–2177. [Google Scholar] [CrossRef] [PubMed]
- Boisen, M.K.; Dehlendorff, C.; Linnemann, D.; Nielsen, B.S.; Larsen, J.S.; Osterlind, K.; Nielsen, S.E.; Tarpgaard, L.S.; Qvortrup, C.; Pfeiffer, P.; et al. Tissue microRNAs as Predictors of Outcome in Patients with Metastatic Colorectal Cancer Treated with First Line Capecitabine and Oxaliplatin with or without Bevacizumab. PLoS ONE 2014, 9, e109430. [Google Scholar] [CrossRef] [PubMed]
- Inamura, K. Diagnostic and Therapeutic Potential of MicroRNAs in Lung Cancer. Cancers (Basel) 2017, 9. [Google Scholar] [CrossRef] [PubMed]
- Hayes, J.; Thygesen, H.; Gregory, W.; Westhead, D.R.; French, P.J.; Van Den Bent, M.J.; Lawler, S.E.; Short, S.C. A Validated microRNA Profile with Predictive Potential in Glioblastoma Patients Treated with Bevacizumab. Mol. Oncol. 2016, 10, 1296–1304. [Google Scholar] [CrossRef] [PubMed]
- Joerger, M.; Baty, F.; Fruh, M.; Droege, C.; Stahel, R.A.; Betticher, D.C.; von Moos, R.; Ochsenbein, A.; Pless, M.; Gautschi, O.; et al. Circulating microRNA Profiling in Patients with Advanced Non-Squamous NSCLC Receiving bevacizumab/erlotinib Followed by Platinum-Based Chemotherapy at Progression (SAKK 19/05). Lung Cancer 2014, 85, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Hansen, T.F.; Carlsen, A.L.; Heegaard, N.H.; Sorensen, F.B.; Jakobsen, A. Changes in Circulating microRNA-126 during Treatment with Chemotherapy and Bevacizumab Predicts Treatment Response in Patients with Metastatic Colorectal Cancer. Br. J. Cancer 2015, 112, 624–629. [Google Scholar] [CrossRef] [PubMed]
- Passardi, A.; Nanni, O.; Tassinari, D.; Turci, D.; Cavanna, L.; Fontana, A.; Ruscelli, S.; Mucciarini, C.; Lorusso, V.; Ragazzini, A.; et al. Effectiveness of Bevacizumab Added to Standard Chemotherapy in Metastatic Colorectal Cancer: Final Results for First-Line Treatment from the ITACa Randomized Clinical Trial. Ann. Oncol. 2015, 26, 1201–1207. [Google Scholar] [CrossRef] [PubMed]
- Fang, J.H.; Zhou, H.C.; Zeng, C.; Yang, J.; Liu, Y.; Huang, X.; Zhang, J.P.; Guan, X.Y.; Zhuang, S.M. MicroRNA-29b Suppresses Tumor Angiogenesis, Invasion, and Metastasis by Regulating Matrix Metalloproteinase 2 Expression. Hepatology 2011, 54, 1729–1740. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Guan, X.; Tu, Y.; Zheng, S.; Long, J.; Li, S.; Qi, C.; Xie, X.; Zhang, H.; Zhang, Y. MicroRNA-29b Attenuates Non-Small Cell Lung Cancer Metastasis by Targeting Matrix Metalloproteinase 2 and PTEN. J. Exp. Clin. Cancer Res. 2015, 34. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Cai, B.; Shen, L.; Dong, Y.; Lu, Q.; Sun, S.; Liu, S.; Ma, S.; Ma, P.X.; Chen, J. MiRNA-29b Suppresses Tumor Growth through Simultaneously Inhibiting Angiogenesis and Tumorigenesis by Targeting Akt3. Cancer Lett. 2017, 397, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Wong, P.F.; Jamal, J.; Tong, K.L.; Khor, E.S.; Yeap, C.E.; Jong, H.L.; Lee, S.T.; Mustafa, M.R.; Abubakar, S. Deregulation of hsa-miR-20b Expression in TNF-α-Induced Premature Senescence of Human Pulmonary Microvascular Endothelial Cells. Microvasc. Res. 2017, 114, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Yang, D.; Wang, J.; Xiao, M.; Zhou, T.; Shi, X. Role of Mir-155 in Controlling HIF-1α Level and Promoting Endothelial Cell Maturation. Sci. Rep. 2016, 6, 35316. [Google Scholar] [CrossRef] [PubMed]
- Pankratz, F.; Bemtgen, X.; Zeiser, R.; Leonhardt, F.; Kreuzaler, S.; Hilgendorf, I.; Smolka, C.; Helbing, T.; Hoefer, I.; Esser, J.S.; et al. MicroRNA-155 Exerts Cell-Specific Antiangiogenic but Proarteriogenic Effects during Adaptive Neovascularization. Circulation 2015, 131, 1575–1589. [Google Scholar] [CrossRef] [PubMed]
- Kong, W.; He, L.; Richards, E.J.; Challa, S.; Xu, C.X.; Permuth-Wey, J.; Lancaster, J.M.; Coppola, D.; Sellers, T.A.; Djeu, J.Y.; et al. Upregulation of miRNA-155 Promotes Tumour Angiogenesis by Targeting VHL and is Associated with Poor Prognosis and Triple-Negative Breast Cancer. Oncogene 2014, 33, 679–689. [Google Scholar] [CrossRef] [PubMed]
- Robertson, E.D.; Wasylyk, C.; Ye, T.; Jung, A.C.; Wasylyk, B. The Oncogenic MicroRNA hsa-miR-155–5p Targets the Transcription Factor ELK3 and Links it to the Hypoxia Response. PLoS ONE 2014, 9, e113050. [Google Scholar] [CrossRef] [PubMed]
- Wan, J.; Xia, L.; Xu, W.; Lu, N. Expression and Function of miR-155 in Diseases of the Gastrointestinal Tract. Int. J. Mol. Sci. 2016, 17. [Google Scholar] [CrossRef] [PubMed]
- Meloni, M.; Marchetti, M.; Garner, K.; Littlejohns, B.; Sala-Newby, G.; Xenophontos, N.; Floris, I.; Suleiman, M.S.; Madeddu, P.; Caporali, A.; et al. Local Inhibition of microRNA-24 Improves Reparative Angiogenesis and Left Ventricle Remodeling and Function in Mice with Myocardial Infarction. Mol. Ther. 2013, 21, 1390–1402. [Google Scholar] [CrossRef] [PubMed]
- Marisi, G.; Scarpi, E.; Passardi, A.; Nanni, O.; Ragazzini, A.; Valgiusti, M.; Casadei Gardini, A.; Neri, L.; Frassineti, G.; Amadori, D.; et al. Circulating VEGF and eNOS Variations as Predictors of Outcome in Metastatic Colorectal Cancer Patients Receiving Bevacizumab. Sci. Rep. 2017, 7. [Google Scholar] [CrossRef] [PubMed]
- Tejpar, S.; Stintzing, S.; Ciardiello, F.; Tabernero, J.; van Cutsem, E.; Beier, F.; Esser, R.; Lenz, H.J.; Heinemann, V. Prognostic and Predictive Relevance of Primary Tumor Location in Patients with RAS Wild-Type Metastatic Colorectal Cancer: Retrospective Analyses of the CRYSTAL and FIRE-3 Trials. JAMA Oncol. 2017, 3, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Sun, Z.; Zhang, Z.; Liu, Z.; Qiu, B.; Liu, K.; Dong, G. MicroRNA-335 Inhibits Invasion and Metastasis of Colorectal Cancer by Targeting ZEB2. Med. Oncol. 2014, 31. [Google Scholar] [CrossRef] [PubMed]
- Sun, D.; Han, S.; Liu, C.; Zhou, R.; Sun, W.; Zhang, Z.; Qu, J. Microrna-199a-5p Functions as a Tumor Suppressor Via Suppressing Connective Tissue Growth Factor (CTGF) in Follicular Thyroid Carcinoma. Med. Sci. Monit. 2016, 22, 1210–1217. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Lei, S.; Long, J.; Liu, X.; Wu, Q. MicroRNA-199a-5p Inhibits Tumor Proliferation in Melanoma by Mediating HIF-1α. Mol. Med. Rep. 2016, 13, 5241–5247. [Google Scholar] [CrossRef] [PubMed]
- Tsuno, S.; Wang, X.; Shomori, K.; Hasegawa, J.; Miura, N. Hsa-miR-520d Induces Hepatoma Cells to Form Normal Liver Tissues Via a Stemness-Mediated Process. Sci. Rep. 2014, 4, 3852. [Google Scholar] [CrossRef] [PubMed]
- Ulivi, P.; Scarpi, E.; Chiadini, E.; Marisi, G.; Valgiusti, M.; Capelli, L.; Casadei Gardini, A.; Monti, M.; Ruscelli, S.; Frassineti, G.L.; et al. Right- vs. Left-Sided Metastatic Colorectal Cancer: Differences in Tumor Biology and Bevacizumab Efficacy. Int. J. Mol. Sci. 2017, 18. [Google Scholar] [CrossRef] [PubMed]
- Hong, L.; Han, Y.; Zhou, Y.; Nita, A. Angiogenesis-Related microRNAs in Colon Cancer. Expert Opin. Biol. Ther. 2013, 13, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Muhammad, S.; Kaur, K.; Huang, R.; Zhang, Q.; Kaur, P.; Yazdani, H.O.; Bilal, M.U.; Zheng, J.; Zheng, L.; Wang, X.S. MicroRNAs in Colorectal Cancer: Role in Metastasis and Clinical Perspectives. World J. Gastroenterol. 2014, 20, 17011–17019. [Google Scholar] [CrossRef] [PubMed]
- Gallach, S.; Calabuig-Farinas, S.; Jantus-Lewintre, E.; Camps, C. MicroRNAs: Promising New Antiangiogenic Targets in Cancer. Biomed. Res. Int. 2014, 2014, 878450. [Google Scholar] [CrossRef] [PubMed]
- Altman, D.G.; McShane, L.M.; Sauerbrei, W.; Taube, S.E. Reporting Recommendations for Tumor Marker Prognostic Studies (REMARK): Explanation and Elaboration. PLoS Med. 2012, 9, e1001216. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | No. (%) |
|---|---|
| Median age, years (range) | 65 (37–83) |
| Gender | |
| Male | 35 (67.3) |
| Female | 17 (32.7) |
| Performance Status (ECOG) | |
| 0 | 44 (84.6) |
| 1–2 | 8 (15.4) |
| Stage at Diagnosis | |
| I–III | 12 (23.1) |
| IV | 40 (76.9) |
| Tumor Localization | |
| Colon | 37 (71.1) |
| Rectum | 15 (28.9) |
| Left-sided | 27 (55.1) |
| Right-sided | 22 (44.9) |
| Grading | |
| 1–2 | 25 (59.5) |
| 3 | 17 (40.5) |
| Missing | 10 (19.0) |
| CT Regimen | |
| FOLFOX4 | 27 (51.9) |
| FOLFIRI | 25 (48.1) |
| Prior Cancer Therapy | |
| Surgery | 40 (76.9) |
| Radiotherapy | 4 (7.7) |
| Adjuvant CT | 9 (17.3) |
| RAS Status | |
| Wild type | 27 (51.9) |
| Mutated | 25 (48.1) |
| BRAF Status | |
| Wild type | 46 (88.5) |
| Mutated | 6 (11.5) |
| miRNA | Left-Sided | Right-Sided | p |
|---|---|---|---|
| Median Value (Range) | |||
| hsa-miR-199a-5p | 3188 (0.5–149,395) | 1960.5 (0.47–48,761) | 0.034 |
| hsa-miR-335-5p | 6574.5 (1493–1,332,286) | 3214 (2.14–40,038) | 0.006 |
| hsa-miR-520d-3p | 5087 (3.09–2,831,724) | 1505 (0.49–48,452) | 0.008 |
| miRNA | KRAS | p | NRAS | p | ||
|---|---|---|---|---|---|---|
| Median Value (Range) | Median Value (Range) | |||||
| Wild Type | Mutated | Wild Type | Mutated | |||
| hsa-miR-21-5p | 1424 (0.57–4627) | 1.71 (0.53–3594) | 0.019 | 1558 (0.57–4627) | 1011 (0.53–3594) | 0.008 |
| hsa-miR-221-3p | 1163 (0.03–5499) | 1878 (0.58–34,375) | 0.050 | 1122 (0.03–5499) | 1866 (0.58–34,375) | 0.010 |
| Baseline | PFS | OS | ||
|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | |
| has-miR-20b-5p | 0.922 (0.847–0.989) | 0.035 | 0.930 (0.850–0.995) | 0.046 |
| has-miR-29b-3p | 0.854 (0.728–0.997) | 0.045 | 0.872 (0.753–0.991) | 0.039 |
| has-miR-424-5p | 0.968 (0.877–1.069) | 0.517 | 0.936 (0.838–1.046) | 0.242 |
| has-miR-155-5p | 0.927 (0.863–0.997) | 0.040 | 0.917 (0.850–0.990) | 0.026 |
| ECOG PS (1–2 vs. 0) | 1.206 (0.424–3.433) | 0.725 | 1.838 (0.667–5.060) | 0.239 |
| BRAF (mutated vs. wild type) | 3.574 (1.075–11.882) | 0.038 | 3.628 (1.063–12.378) | 0.040 |
| Age, years (≥65 vs. <65) | 2.207 (0.987–4.935) | 0.054 | 1.478 (0.650–3.364) | 0.351 |
| PFS | No. Patients | No. Events | Median PFS (Months) (95% CI) | p | HR (95% CI) | p |
| hsa-miR-20b-5p | ||||||
| <1293 | 26 | 24 | 8.1 (5.0–12.5) | 1.00 | ||
| ≥1293 | 26 | 20 | 14.0 (9.4–21.3) | 0.008 | 0.44 (0.24–0.82) | 0.010 |
| hsa-miR-29b-3p | ||||||
| <3138 | 25 | 23 | 8.2 (5.0–12.4) | 1.00 | ||
| ≥3138 | 27 | 21 | 14.9 (9.1–21.3) | 0.021 | 0.50 (0.27–0.91) | 0.024 |
| hsa-miR-155-5p | ||||||
| <0.73 | 32 | 30 | 8.3 (6.1–9.7) | 1.00 | ||
| ≥0.73 | 20 | 14 | 16.0 (10.2–23.0) | 0.007 | 0.42 (0.22–0.81) | 0.009 |
| OS | No. Patients | No. Events | Median OS (Months) (95% CI) | p | HR (95% CI) | p |
| hsa-miR-20b-5p | ||||||
| <1293 | 26 | 23 | 11.6 (8.2–23.4) | 1.00 | ||
| ≥1293 | 26 | 17 | 28.8 (19.3–42.9) | 0.004 | 0.40 (0.21–0.77) | 0.005 |
| hsa-miR-29b-3p | ||||||
| <3138 | 25 | 22 | 15.5 (6.8–24.8) | 1.00 | ||
| ≥3138 | 27 | 18 | 31.7 (13.9–47.1) | 0.005 | 0.40 (0.21–0.78) | 0.007 |
| hsa-miR-155-5p | ||||||
| <0.73 | 32 | 27 | 13.5 (8.2–23.4) | 1.00 | ||
| ≥0.73 | 20 | 13 | 31.6 (21.8–42.9) | 0.024 | 0.47 (0.24–0.92) | 0.028 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ulivi, P.; Canale, M.; Passardi, A.; Marisi, G.; Valgiusti, M.; Frassineti, G.L.; Calistri, D.; Amadori, D.; Scarpi, E. Circulating Plasma Levels of miR-20b, miR-29b and miR-155 as Predictors of Bevacizumab Efficacy in Patients with Metastatic Colorectal Cancer. Int. J. Mol. Sci. 2018, 19, 307. https://doi.org/10.3390/ijms19010307
Ulivi P, Canale M, Passardi A, Marisi G, Valgiusti M, Frassineti GL, Calistri D, Amadori D, Scarpi E. Circulating Plasma Levels of miR-20b, miR-29b and miR-155 as Predictors of Bevacizumab Efficacy in Patients with Metastatic Colorectal Cancer. International Journal of Molecular Sciences. 2018; 19(1):307. https://doi.org/10.3390/ijms19010307
Chicago/Turabian StyleUlivi, Paola, Matteo Canale, Alessandro Passardi, Giorgia Marisi, Martina Valgiusti, Giovanni Luca Frassineti, Daniele Calistri, Dino Amadori, and Emanuela Scarpi. 2018. "Circulating Plasma Levels of miR-20b, miR-29b and miR-155 as Predictors of Bevacizumab Efficacy in Patients with Metastatic Colorectal Cancer" International Journal of Molecular Sciences 19, no. 1: 307. https://doi.org/10.3390/ijms19010307
APA StyleUlivi, P., Canale, M., Passardi, A., Marisi, G., Valgiusti, M., Frassineti, G. L., Calistri, D., Amadori, D., & Scarpi, E. (2018). Circulating Plasma Levels of miR-20b, miR-29b and miR-155 as Predictors of Bevacizumab Efficacy in Patients with Metastatic Colorectal Cancer. International Journal of Molecular Sciences, 19(1), 307. https://doi.org/10.3390/ijms19010307