Additive Manufacturing for Guided Bone Regeneration: A Perspective for Alveolar Ridge Augmentation

 , ,
, ,
Abstract
:
1. Introduction
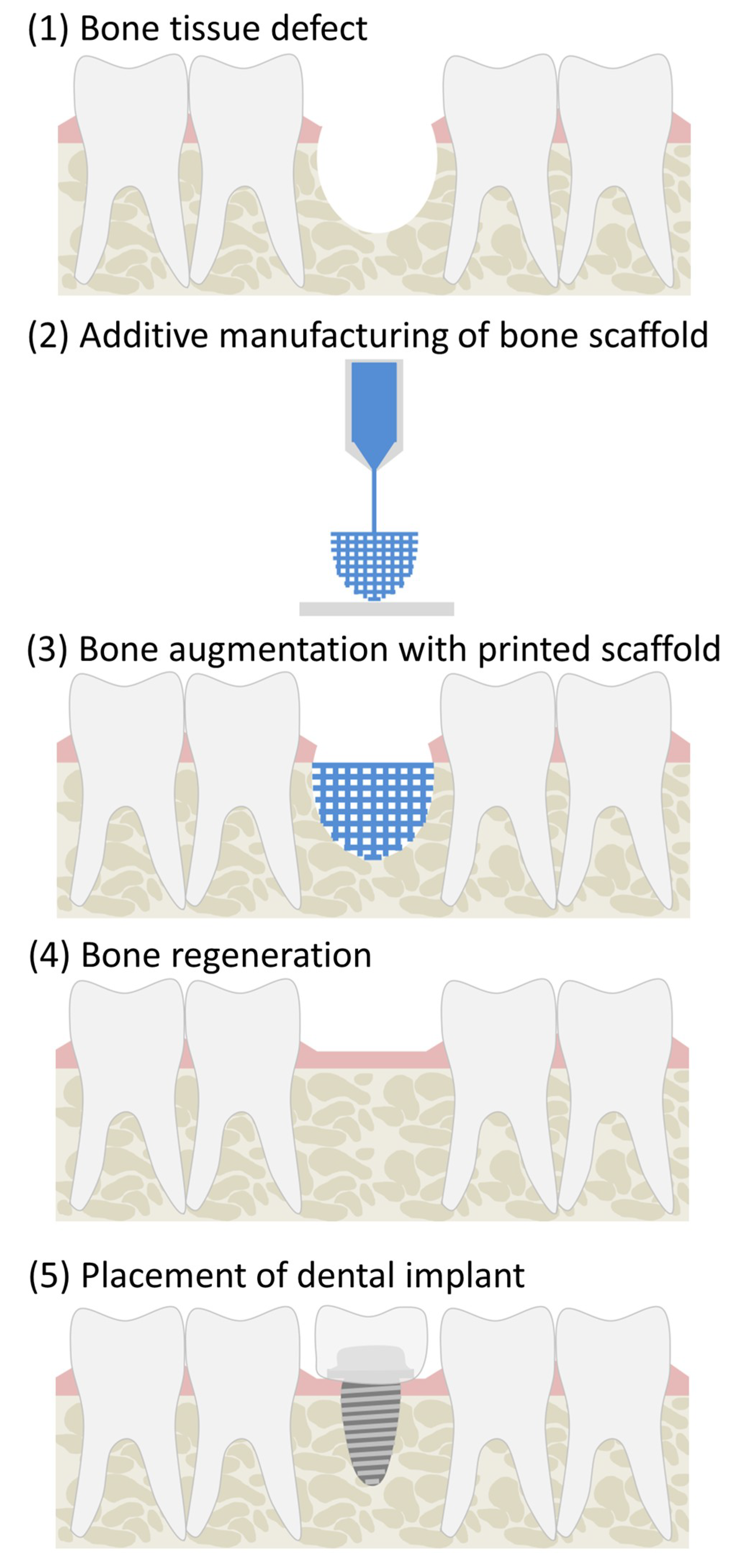
1.1. Alveolar Ridge Augmentation
1.2. Optimal Properties of Bone Tissue Scaffolds
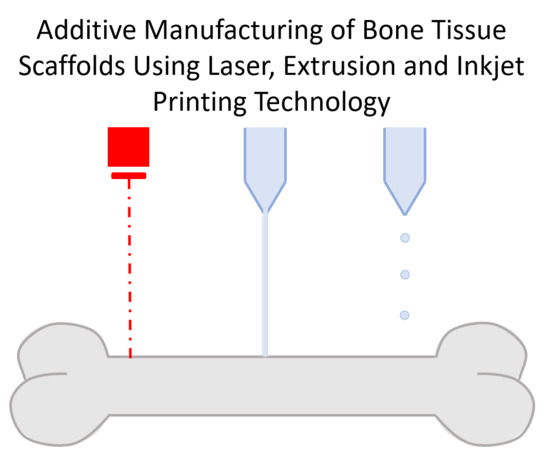
1.3. Additive Manufacturing Techniques (AM)
2. Stereolithography
2.1. Natural Polymers
2.1.1. Gelatin
2.1.2. Silk Fibroin
2.1.3. Chitosan
2.1.4. Alginate
2.2. Synthetic Polymers
2.2.1. Poly(Propylene Fumarate) (PPF)
2.2.2. Polycaprolactone (PCL)
2.2.3. Polylactic Acid (PLA)
2.2.4. Poly(trimethylene Carbonate) (PTMC)
2.2.5. Poly(ethylene Glycol) Divinyl Ether (PEG-DVE)
2.2.6. 2-Ethylhexyl Acrylates (EHA)/Isobornyl Acrylate (IBOA)
2.3. Bioceramics
Tricalcium Phosphate/Hydroxyapatite
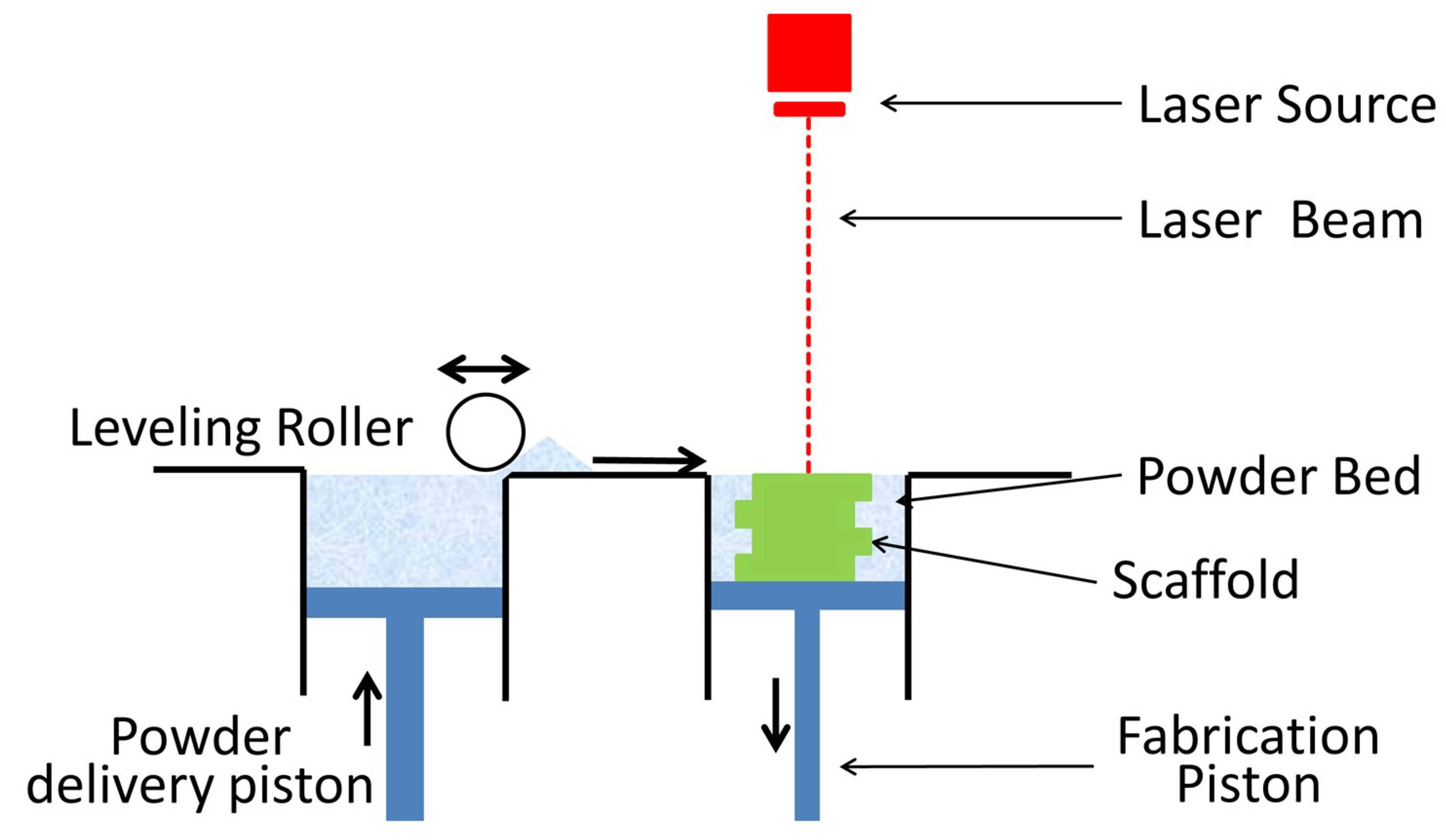
3. Selective Laser Sintering
3.1. Bioceramics
3.1.1. Magnesium Silicate
3.1.2. Tricalcium Phosphate (TCP)
3.1.3. Hydroxyapatite (HA)
3.2. Polymers
3.2.1. Polycaprolactone (PCL)
3.2.2. Poly(hydroxybutyrate) (PHB)
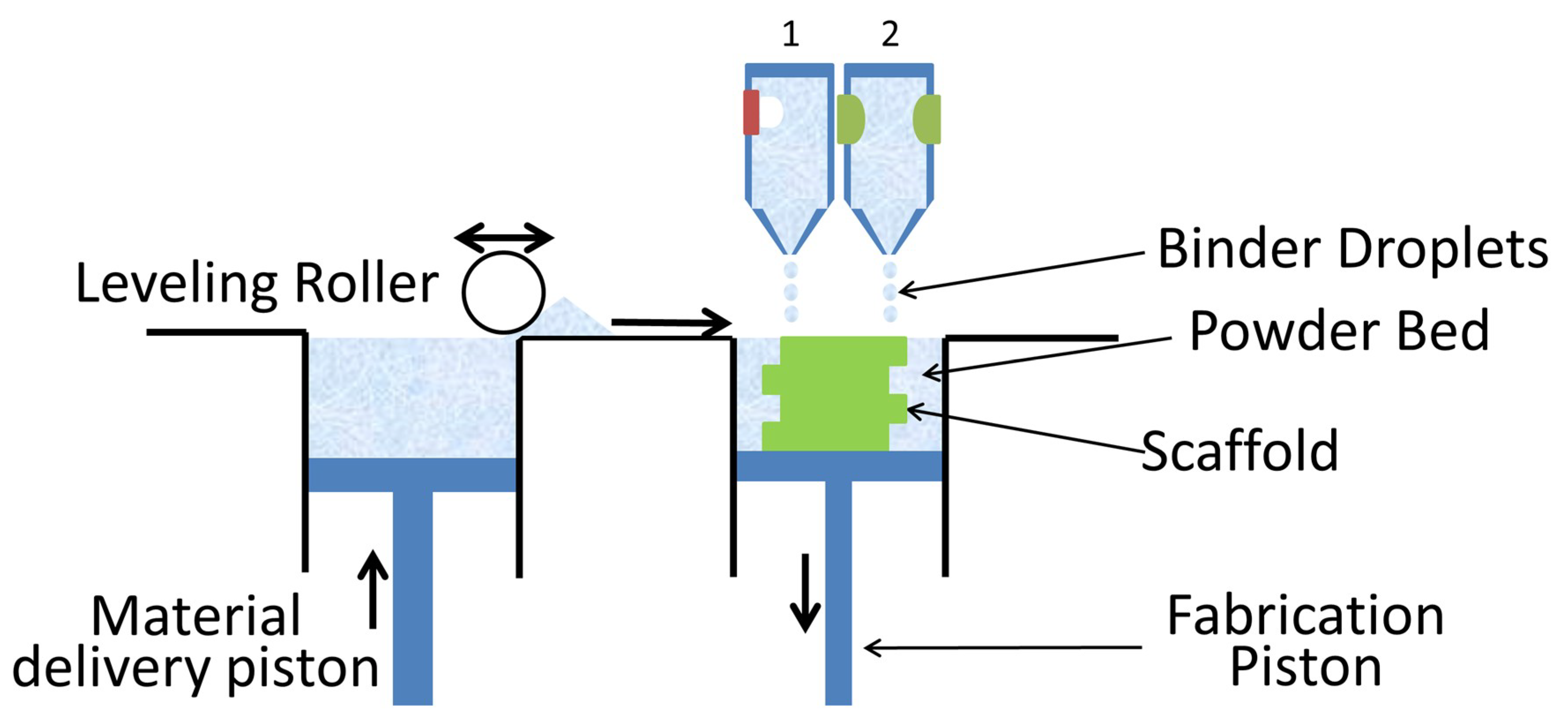
4. Powder Bed Inkjet Printing
4.1. Bioceramics
4.1.1. Hydroxyapatite
4.1.2. Tetracalcium Phosphate (TTCP)
4.1.3. Dicalcium Phosphate (DCP)
4.1.4. Tricalcium Phosphate (TCP)
4.1.5. Octacalcium Phosphate (OCP)
4.1.6. Calcium Polyphosphate (CPP)
4.1.7. Biphasic Calcium Phosphate (BCP)
4.1.8. Calcium Sulfate (CS)
4.1.9. Magnesium Ammonium Phosphate
4.2. Synthetic Polymers
4.2.1. Poly (dl-lactide-co-glycolide) (PLGA)
4.2.2. Poly(e-caprolactone) (PCL)
4.3. Clinical Study
5. Extrusion Printing
5.1. Bioceramics
5.1.1. Hydroxyapatite
5.1.2. Tricalcium Phosphate (TCP)
5.1.3. Strontium (Sr) Composites
5.2. Synthetic Polymers
5.2.1. Polylactic Acid (PLA)
5.2.2. Poly(dl-lactide-co-glycolide) (PLGA)
5.2.3. Poly(e-caprolactone) (PCL)
5.2.4. Poly(Propylene Fumarate) (PPF)
5.2.5. Pluronic® F-127 Hydrogel
6. Transfer to Alveolar Bone Augmentation
7. Conclusions
Conflicts of Interest
Abbreviations
| 2PP | Two-Photon Polymerization |
| AM | Additive Manufacture |
| AA | Alginic Acid |
| ALP | Alkaline Phosphatase |
| ASCs | Adipose-derived stem cells |
| BCP | Biphasic Calcium Phosphate |
| BG | Bioactive Glass S53P4 |
| BMSCs | Bone Marrow Mesenchymal Stem Cells |
| CHA | Carbonated Hydroxyapatite |
| CP | Calcium Phosphate |
| CNT | Carbon Nanotubes |
| CPP | Calcium Polyphosphate |
| CS | Calcium Sulfate |
| DCP | Dicalcium Phosphate |
| EHA | 2-ethylhexyl Acrylates |
| GBR | Guided Bone Regeneration |
| GelMA | Gelatin Methacrylate |
| GO | Graphene Oxide |
| HA | Hydroxyapatite |
| hFOB | Human Fetal Osteoblastic |
| HIPEs | High Internal Phase Emulsions |
| HUVEC | Human Umbilical Vein Endothelial Cells |
| IBOA | Isobornyl Acrylate |
| MWCNTs | Multiwalled Carbon Nanotubes |
| nHA | Nano-Hydroxyapatite |
| NVP | N-vinyl-2-pyrrolidone |
| OCP | Octacalcium Phosphate |
| pBMPC | Porcine Bone Marrow-Derived Progenitor Cells |
| PBT | Polybutylene terephthalate |
| PCL | Polycaprolactone |
| PDLLA | Poly(d,l-lactide) |
| PEGDA | Polyethylene Glycol Diacrylate |
| PEG-DVE | Poly(ethylene glycol) Divinyl Ether |
| PETMP | Pentaerythritol Tetrakis(3-mercaptopropionate) |
| PHB | Poly(hydroxybutyrate) |
| PHBV | Poly(hydroxybutyrate-co-hydroxyvalerate) |
| PLA | Polylactic Acid |
| PLGA | Poly(dl-lactide-co-glycolide) |
| PLLA | Poly(l-lactic acid) |
| PPF | Poly (propylene fumarate) |
| PTMC | Poly(trimethylene carbonate) |
| PVA | Poly Vinyl Alcohol |
| SDS | Sodium Dodecyl Sulfate |
| SF | Silk Fibroin |
| SilMA | Silk Methacrylate |
| SLA | Stereolithography |
| SLS | Selective Laser Sintering |
| Sr | Strontium |
| ß-TCP | Beta-Tricalcium Phosphate |
| TCP | Tricalcium Phosphate |
| TEGMA | Triethylene Glycol Dimethacrylate |
| TTCP | Tetracalcium Phosphate |
References
- Wang, W.; Duan, J.; Wang, Q.; Kuang, W. Complex reconstruction of facial deformity and function after severe gunshot injury: One case report. Int. J. Clin. Exp. Med. 2015, 8, 1427–1433. [Google Scholar] [PubMed]
- Park, Y.-H.; Choi, S.-H.; Cho, K.-S.; Lee, J.-S. Dimensional alterations following vertical ridge augmentation using collagen membrane and three types of bone grafting materials: A retrospective observational study. Clin. Implant Dent. Relat. Res. 2017, 19, 742–749. [Google Scholar] [CrossRef] [PubMed]
- Oryan, A.; Alidadi, S.; Moshiri, A.; Maffulli, N. Bone regenerative medicine: Classic options, novel strategies, and future directions. J. Orthop. Surg. Res. 2014, 9, 18. [Google Scholar] [CrossRef] [PubMed]
- Roseti, L.; Parisi, V.; Petretta, M.; Cavallo, C.; Desando, G.; Bartolotti, I.; Grigolo, B. Scaffolds for bone tissue engineering: State of the art and new perspectives. Mater. Sci. Eng. C 2017, 78, 1246–1262. [Google Scholar] [CrossRef] [PubMed]
- Polo-Corrales, L.; Latorre-Esteves, M.; Ramirez-Vick, J.E. Scaffold design for bone regeneration. J. Nanosci. Nanotechnol. 2014, 14, 15–56. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Johansson, C. Osteoinduction, osteoconduction and osseointegration. Eur. Spine J. 2001, 10, S96–S101. [Google Scholar] [CrossRef] [PubMed]
- Bouet, G.; Marchat, D.; Cruel, M.; Malaval, L.; Vico, L. In Vitro three-dimensional bone tissue models: From cells to controlled and dynamic environment. Tissue Eng. Part B Rev. 2015, 21, 133–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Luca, A.; Ostrowska, B.; Lorenzo-Moldero, I.; Lepedda, A.; Swieszkowski, W.; van Blitterswijk, C.; Moroni, L. Gradients in pore size enhance the osteogenic differentiation of human mesenchymal stromal cells in three-dimensional scaffolds. Sci. Rep. 2016, 6. [Google Scholar] [CrossRef] [PubMed]
- Kasten, P.; Beyen, I.; Niemeyer, P.; Luginbühl, R.; Bohner, M.; Richter, W. Porosity and pore size of β-tricalcium phosphate scaffold can influence protein production and osteogenic differentiation of human mesenchymal stem cells: An in vitro and in vivo study. Acta Biomater. 2008, 4, 1904–1915. [Google Scholar] [CrossRef] [PubMed]
- Mullen, C.A.; Vaughan, T.J.; Billiar, K.L.; McNamara, L.M. The effect of substrate stiffness, thickness, and cross-linking density on osteogenic cell behavior. Biophys. J. 2015, 108, 1604–1612. [Google Scholar] [CrossRef] [PubMed]
- Peterson, J.; Wang, Q.; Dechow, P.C. Material properties of the dentate maxilla. Anat. Rec. Part A Discov. Mol. Cell. Evol. Biol. 2006, 288, 962–972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Misch, C.E.; Qu, Z.; Bidez, M.W. Mechanical properties of trabecular bone in the human mandible: Implications for dental implant treatment planning and surgical placement. J. Oral Maxillofac. Surg. 1999, 57, 700–706. [Google Scholar] [CrossRef]
- Ruhé, P.Q.; Boerman, O.C.; Russel, F.G.M.; Mikos, A.G.; Spauwen, P.H.M.; Jansen, J.A. In vivo release of rhBMP-2 loaded porous calcium phosphate cement pretreated with albumin. J. Mater. Sci. Mater. Med. 2006, 17, 919–927. [Google Scholar] [CrossRef] [PubMed]
- Havaldar, R.; Pilli, S.; Putti, B. Insights into the effects of tensile and compressive loadings on human femur bone. Adv. Biomed. Res. 2014, 3, 101. [Google Scholar] [CrossRef] [PubMed]
- Sadrimanesh, R.; Siadat, H.; Sadr-Eshkevari, P.; Monzavi, A.; Maurer, P.; Rashad, A. Alveolar bone stress around implants with different abutment angulation: An FE-Analysis of anterior maxilla. Implant Dent. 2012, 21, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Karageorgiou, V.; Kaplan, D. Porosity of 3D biomaterial scaffolds and osteogenesis. Biomaterials 2005, 26, 5474–5491. [Google Scholar] [CrossRef] [PubMed]
- Tsuruga, E.; Takita, H.; Itoh, H.; Wakisaka, Y.; Kuboki, Y. Pore size of porous hydroxyapatite as the cell-substratum controls BMP-induced osteogenesis. J. Biochem. 1997, 121, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Chang, B.S.; Lee, C.K.; Hong, K.S.; Youn, H.J.; Ryu, H.S.; Chung, S.S.; Park, K.W. Osteoconduction at porous hydroxyapatite with various pore configurations. Biomaterials 2000, 21, 1291–1298. [Google Scholar] [CrossRef]
- Zioupos, P.; Cook, R.B.; Hutchinson, J.R. Some basic relationships between density values in cancellous and cortical bone. J. Biomech. 2008, 41, 1961–1968. [Google Scholar] [CrossRef] [PubMed]
- Ratner, B.D. Biomaterials Science: An Introduction to Materials in Medicine; Academic Press: Cambridge, MA, USA, 2013; ISBN 008087780X. [Google Scholar]
- Krane, S.M. Collagenases and Collagen Degradation. J. Investig. Dermatol. 1982, 79 (Suppl. 1), 83s–86s. [Google Scholar] [CrossRef] [PubMed]
- Goto, T.; Kojima, T.; Iijima, T.; Yokokura, S.; Kawano, H.; Yamamoto, A.; Matsuda, K. Resorption of synthetic porous hydroxyapatite and replacement by newly formed bone. J. Orthop. Sci. 2001, 6, 444–447. [Google Scholar] [CrossRef] [PubMed]
- Bose, S.; Vahabzadeh, S.; Bandyopadhyay, A. Bone tissue engineering using 3D printing. Mater. Today 2013, 16, 496–504. [Google Scholar] [CrossRef]
- Pati, F.; Jang, J.; Lee, J.W.; Cho, D.W. Extrusion Bioprinting; Academic Press: Cambridge, MA, USA, 2015; ISBN 9780128010150. [Google Scholar]
- Skoog, S.A.; Goering, P.L.; Narayan, R.J. Stereolithography in tissue engineering. J. Mater. Sci. Mater. Med. 2014, 25, 845–856. [Google Scholar] [CrossRef] [PubMed]
- Mondschein, R.J.; Kanitkar, A.; Williams, C.B.; Verbridge, S.S.; Long, T.E. Polymer structure-property requirements for stereolithographic 3D printing of soft tissue engineering scaffolds. Biomaterials 2017, 140, 170–188. [Google Scholar] [CrossRef] [PubMed]
- Shusteff, M.; Panas, R.M.; Henriksson, J.; Kelly, B.E.; Browar, A.E.M.; Fang, N.X.; Spadaccini, C.M.; Shusteff, M.; Panas, R.M.; Henriksson, J.; et al. Additive Fabrication of 3D Structures by Holographic Lithography. Annu. Int. Solid Free. Fabr. Symp. 2016, 1183–1192. [Google Scholar]
- Lin, H.; Tang, Y.; Lozito, T.P.; Oyster, N.; Kang, R.B.; Fritch, M.R.; Wang, B.; Tuan, R.S. Projection Stereolithographic Fabrication of BMP-2 Gene-activated Matrix for Bone Tissue Engineering. Sci. Rep. 2017, 7, 11327. [Google Scholar] [CrossRef] [PubMed]
- Nichol, J.W.; Koshy, S.T.; Bae, H.; Hwang, C.M.; Yamanlar, S.; Khademhosseini, A. Cell-laden microengineered gelatin methacrylate hydrogels. Biomaterials 2010, 31, 5536–5544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, W.; He, J.; Nichol, J.W.; Wang, L.; Hutson, C.B.; Wang, B.; Du, Y.; Fan, H.; Khademhosseini, A. Synthesis and characterization of photocrosslinkable gelatin and silk fibroin interpenetrating polymer network hydrogels. Acta Biomater. 2011, 7, 2384–2393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benton, J.A.; DeForest, C.A.; Vivekanandan, V.; Anseth, K.S. Photocrosslinking of Gelatin Macromers to Synthesize Porous Hydrogels That Promote Valvular Interstitial Cell Function. Tissue Eng. Part A 2009, 15, 3221–3230. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Yeon, Y.K.; Lee, J.M.; Chao, J.R.; Lee, Y.J.; Seo, Y.B.; Sultan, T.; Lee, O.J.; Lee, J.S. Precisely printable and biocompatible silk fibroin bioink for digital light processing 3D printing. Nat. Commun. 2018, 3. [Google Scholar] [CrossRef]
- Morris, V.B.; Nimbalkar, S.; Younesi, M.; McClellan, P.; Akkus, O. Mechanical Properties, Cytocompatibility and Manufacturability of Chitosan:PEGDA Hybrid-Gel Scaffolds by Stereolithography. Ann. Biomed. Eng. 2017, 45, 286–296. [Google Scholar] [CrossRef] [PubMed]
- Elomaa, L.; Kokkari, A.; Närhi, T.; Seppälä, J.V. Porous 3D modeled scaffolds of bioactive glass and photocrosslinkable poly(ε-caprolactone) by stereolithography. Compos. Sci. Technol. 2013, 74, 99–106. [Google Scholar] [CrossRef]
- Seol, Y.J.; Park, D.Y.; Park, J.Y.; Kim, S.W.; Park, S.J.; Cho, D.W. A new method of fabricating robust freeform 3D ceramic scaffolds for bone tissue regeneration. Biotechnol. Bioeng. 2013, 110, 1444–1455. [Google Scholar] [CrossRef] [PubMed]
- Chandler, E.M.; Berglund, C.M.; Lee, J.S.; Polacheck, W.J.; Gleghorn, J.P.; Kirby, B.J.; Fischbach, C. Stiffness of photocrosslinked RGD-alginate gels regulates adipose progenitor cell behavior. Biotechnol. Bioeng. 2011, 108, 1683–1692. [Google Scholar] [CrossRef] [PubMed]
- Elomaa, L.; Teixeira, S.; Hakala, R.; Korhonen, H.; Grijpma, D.W.; Seppälä, J.V. Preparation of poly(ε-caprolactone)-based tissue engineering scaffolds by stereolithography. Acta Biomater. 2011, 7, 3850–3856. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, A.; Leonards, H.; Tobies, N.; Pongratz, L.; Kreuels, K.; Kreimendahl, F.; Apel, C.; Wehner, M.; Nottrodt, N. New stereolithographic resin providing functional surfaces for biocompatible three-dimensional printing. J. Tissue Eng. 2017, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanodekaew, S.; Channasanon, S.; Uppanan, P. Preparation and degradation study of photocurable oligolactide-HA composite: A potential resin for stereolithography application. J. Biomed. Mater. Res. Part B Appl. Biomater. 2014, 102, 604–611. [Google Scholar] [CrossRef] [PubMed]
- Guillaume, O.; Geven, M.A.; Sprecher, C.M.; Stadelmann, V.A.; Grijpma, D.W.; Tang, T.T.; Qin, L.; Lai, Y.; Alini, M.; de Bruijn, J.D.; et al. Surface-enrichment with hydroxyapatite nanoparticles in stereolithography-fabricated composite polymer scaffolds promotes bone repair. Acta Biomater. 2017, 54, 386–398. [Google Scholar] [CrossRef] [PubMed]
- Rider, P.; Zhang, Y.; Tse, C.; Zhang, Y.; Jayawardane, D.; Stringer, J.; Callaghan, J.; Brook, I.M.; Miller, C.A.; Zhao, X.; et al. Biocompatible silk fibroin scaffold prepared by reactive inkjet printing. J. Mater. Sci. 2016, 51, 8625–8630. [Google Scholar] [CrossRef] [Green Version]
- Rider, P.; Brook, I.; Smith, P.; Miller, C. Reactive Inkjet Printing of Regenerated Silk Fibroin Films for Use as Dental Barrier Membranes. Micromachines 2018, 9, 46. [Google Scholar] [CrossRef]
- Zhu, J. Bioactive modification of poly(ethylene glycol) hydrogels for tissue engineering. Biomaterials 2010, 31, 4639–4656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.; Member, S.; Tian, Z.; Jin, X.; Holzman, J.F.; Menard, F.; Kim, K.; Preparation, A.H. Visible Light-based Stereolithography Bioprinting of Cell-adhesive Gelatin Hydrogels. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Seogwipo, Korea, 11–15 July 2017; pp. 1599–1602. [Google Scholar]
- Wang, Z.; Abdulla, R.; Parker, B.; Samanipour, R.; Ghosh, S.; Kim, K. A simple and high-resolution stereolithography-based 3D bioprinting system using visible light crosslinkable bioinks. Biofabrication 2015, 7, 45009. [Google Scholar] [CrossRef] [PubMed]
- Jeon, O.; Bouhadir, K.H.; Mansour, J.M.; Alsberg, E. Photocrosslinked alginate hydrogels with tunable biodegradation rates and mechanical properties. Biomaterials 2009, 30, 2724–2734. [Google Scholar] [CrossRef] [PubMed]
- Cooke, M.N.; Fisher, J.P.; Dean, D.; Rimnac, C.; Mikos, A.G. Use of Stereolithography to Manufacture Critical-Sized 3D Biodegradable Scaffolds for Bone Ingrowth. J. Biomed. Mater. Res. Part B Appl. Biomater. 2003, 64, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Lan, P.X.; Kim, B.; Lim, G.; Cho, D.W. 3D scaffold fabrication with PPF/DEF using micro-stereolithography. Microelectron. Eng. 2007, 84, 1702–1705. [Google Scholar] [CrossRef]
- Lee, J.W.; Kang, K.S.; Lee, S.H.; Kim, J.-Y.; Lee, B.-K.; Cho, D.-W. Bone regeneration using a microstereolithography-produced customized poly(propylene fumarate)/diethyl fumarate photopolymer 3D scaffold incorporating BMP-2 loaded PLGA microspheres. Biomaterials 2011, 32, 744–752. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.-W.; Wang, S.; Fox, B.C.; Ritman, E.L.; Yaszemski, M.J.; Lu, L. Poly(propylene fumarate) bone tissue engineering scaffold fabrication using stereolithography: Effects of resin formulations and laser parameters. Biomacromolecules 2007, 8, 1077–1084. [Google Scholar] [CrossRef] [PubMed]
- Melchels, F.P.W.; Feijen, J.; Grijpma, D.W. A poly(d,l-lactide) resin for the preparation of tissue engineering scaffolds by stereolithography. Biomaterials 2009, 30, 3801–3809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jansen, J.; Melchels, F.P.W.; Grijpma, D.W.; Feijen, J. Fumaric Acid Monoethyl Ester-Functionalized Poly (d,l-lactide)/N-vinyl-2-pyrrolidone Resins for the Preparation of Tissue Engineering Scaffolds by Stereolithography. Biomacromolecules 2009, 10, 214–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rydholm, A.E.; Reddy, S.K.; Anseth, K.S.; Bowman, C.N. Development and characterization of degradable thiol-allyl ether photopolymers. Polymer 2007, 48, 4589–4600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Machado, T.O.; Sayer, C.; Araujo, P.H.H. Thiol-ene polymerisation: A promising technique to obtain novel biomaterials. Eur. Polym. J. 2017, 86, 200–215. [Google Scholar] [CrossRef]
- Malayeri, A.; Sherborne, C.; Paterson, T.; Mittar, S.; Asencio, I.O.; Hatton, P.V.; Claeyssens, F. Osteosarcoma growth on trabecular bone mimicking structures manufactured via laser direct write. Int. J. Bioprint. 2016, 2, 67–77. [Google Scholar] [CrossRef]
- Silverstein, M.S. PolyHIPEs: Recent advances in emulsion-templated porous polymers. Prog. Polym. Sci. 2014, 39, 199–234. [Google Scholar] [CrossRef]
- Trombetta, R.; Inzana, J.A.; Schwarz, E.M.; Kates, S.L.; Awad, H.A. 3D Printing of Calcium Phosphate Ceramics for Bone Tissue Engineering and Drug Delivery. Ann. Biomed. Eng. 2017, 45, 23–44. [Google Scholar] [CrossRef] [PubMed]
- Kruth, J.P.; Wang, X.; Laoui, T.; Froyen, L. Lasers and materials in selective laser sintering. Assem. Autom. 2003, 23, 357–371. [Google Scholar] [CrossRef]
- Lorrison, J.C.; Dalgarno, K.W.; Wood, D.J. Processing of an apatite-mullite glass-ceramic and an hydroxyapatite/phosphate glass composite by selective laser sintering. J. Mater. Sci. Mater. Med. 2005, 16, 775–781. [Google Scholar] [CrossRef] [PubMed]
- Mazzoli, A. Selective laser sintering in biomedical engineering. Med. Biol. Eng. Comput. 2013, 51, 245–256. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; He, S.; Wu, P.; Gao, C.; Feng, P.; Xiao, T.; Deng, Y.; Shuai, C. A novel MgO-CaO-SiO2 system for fabricating bone scaffolds with improved overall performance. Materials 2016, 9, 287. [Google Scholar] [CrossRef] [PubMed]
- Feng, P.; Wei, P.; Shuai, C.; Peng, S. Characterization of mechanical and biological properties of 3-D scaffolds reinforced with zinc oxide for bone tissue engineering. PLoS ONE 2014, 9. [Google Scholar] [CrossRef] [PubMed]
- Shuai, C.; Li, P.; Liu, J.; Peng, S. Optimization of TCP/HAP ratio for better properties of calcium phosphate scaffold via selective laser sintering. Mater. Charact. 2013, 77, 23–31. [Google Scholar] [CrossRef]
- Smith, M.H.; Flanagan, C.L.; Kemppainen, J.M.; Sack, J.A.; Chung, H.; Das, S.; Hollister, S.J.; Feinberg, S.E. Computed tomography-based tissue-engineered scaffolds in craniomaxillofacial surgery. Int. J. Med. Robot. Comput. Assist. Surg. 2007, 3, 207–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lohfeld, S.; Cahill, S.; Barron, V.; McHugh, P.; Dürselen, L.; Kreja, L.; Bausewein, C.; Ignatius, A. Fabrication, mechanical and in vivo performance of polycaprolactone/tricalcium phosphate composite scaffolds. Acta Biomater. 2012, 8, 3446–3456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xia, Y.; Zhou, P.; Cheng, X.; Xie, Y.; Liang, C.; Li, C.; Xu, S. Selective laser sintering fabrication of nano-hydroxyapatite/poly-ε-caprolactone scaffolds for bone tissue engineering applications. Int. J. Nanomed. 2013, 8, 4197–4213. [Google Scholar] [CrossRef] [Green Version]
- Duan, B.; Wang, M.; You, W.; Lam, W.; Yang, Z.; Lu, W.W. Acta Biomaterialia Three-dimensional nanocomposite scaffolds fabricated via selective laser sintering for bone tissue engineering. Acta Biomater. 2010, 6, 4495–4505. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Hao, L.; Savalani, M.M.; Harris, R.A.; Di Silvio, L.; Tanner, K.E. In vitro biocompatibility of hydroxyapatite-reinforced polymeric composites manufactured by selective laser sintering. J. Biomed. Mater. Res. Part A 2009, 91, 1018–1027. [Google Scholar] [CrossRef] [PubMed]
- Shuai, C.; Zhuang, J.; Hu, H.; Peng, S.; Liu, D.; Liu, J. In vitro bioactivity and degradability of β-tricalcium phosphate porous scaffold fabricated via selective laser sintering. Biotechnol. Appl. Biochem. 2013, 60, 266–273. [Google Scholar] [CrossRef] [PubMed]
- Cameron, R.E.; Kamvari-Moghaddam, A. Synthetic bioresorbable polymers. Durab. Reliab. Med. Polym. 2012, 96–118. [Google Scholar] [CrossRef]
- Eshraghi, S.; Das, S. Mechanical and microstructural properties of polycaprolactone scaffolds with one-dimensional, two-dimensional, and three-dimensional orthogonally oriented porous architectures produced by selective laser sintering. Acta Biomater. 2010, 6, 2467–2476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiria, F.E.; Leong, K.F.; Chua, C.K.; Liu, Y. Poly-ε-caprolactone/hydroxyapatite for tissue engineering scaffold fabrication via selective laser sintering. Acta Biomater. 2007, 3, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Eosoly, S.; Brabazon, D.; Lohfeld, S.; Looney, L. Selective laser sintering of hydroxyapatite/poly-ε-caprolactone scaffolds. Acta Biomater. 2010, 6, 2511–2517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eosoly, S.; Vrana, N.E.; Lohfeld, S.; Hindie, M.; Looney, L. Interaction of cell culture with composition effects on the mechanical properties of polycaprolactone-hydroxyapatite scaffolds fabricated via selective laser sintering (SLS). Mater. Sci. Eng. C 2012, 32, 2250–2257. [Google Scholar] [CrossRef] [Green Version]
- Wang, M.; Duan, B. Nanocomposite Scaffolds for Bone Tissue Engineering: Design, Fabrication, Surface Modification and Sustained Release of Growth Factor. MRS Proc. Lib. Arch. 2011, 1301. [Google Scholar] [CrossRef]
- Shirazi, S.F.S.; Gharehkhani, S.; Mehrali, M.; Yarmand, H.; Metselaar, H.S.C.; Adib Kadri, N.; Osman, N.A.A. A review on powder-based additive manufacturing for tissue engineering: Selective laser sintering and inkjet 3D printing. Sci. Technol. Adv. Mater. 2015, 16, 033502. [Google Scholar] [CrossRef] [PubMed]
- Budding, A.; Vaneker, T.H.J.; Winnubst, A.J.A. Open source powder based rapid prototyping machine for ceramics. Procedia Soc. Behav. Sci. 2013, 6, 533–538. [Google Scholar] [CrossRef]
- Guo, Y.; Patanwala, H.S.; Bognet, B.; Ma, A.W.K. Inkjet and inkjet-based 3D printing: Connecting fluid properties and printing performance. Rapid Prototyp. J. 2017, 3, 562–576. [Google Scholar] [CrossRef]
- Jammalamadaka, U.; Tappa, K. Recent Advances in Biomaterials for 3D Printing and Tissue Engineering. J. Funct. Biomater. 2018, 9, 22. [Google Scholar] [CrossRef] [PubMed]
- Derby, B. Inkjet printing of functional and structural materials: Fluid property requirements, feature stability, and resolution. Annu. Rev. Mater. Res. 2010, 40, 395–414. [Google Scholar] [CrossRef]
- Saijo, H.; Igawa, K.; Kanno, Y.; Mori, Y.; Kondo, K.; Shimizu, K.; Suzuki, S.; Chikazu, D.; Iino, M.; Anzai, M.; et al. Maxillofacial reconstruction using custom-made artificial bones fabricated by inkjet printing technology. J. Artif. Organs 2009, 12, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Kanno, Y.; Nakatsuka, T.; Saijo, H.; Fujihara, Y.; Atsuhiko, H.; Chung, U.-I.; Takato, T.; Hoshi, K. Computed tomographic evaluation of novel custom-made artificial bones, “CT-bone”, applied for maxillofacial reconstruction. Regen. Ther. 2016, 5, 1–8. [Google Scholar] [CrossRef]
- Saijo, H.; Fujihara, Y.; Kanno, Y.; Hoshi, K.; Hikita, A.; Chung, U.-I.; Takato, T. Clinical experience of full custom-made artificial bones for the maxillofacial region. Regen. Ther. 2016, 5, 72–78. [Google Scholar] [CrossRef]
- Gbureck, U.; Hölzel, T.; Doillon, C.J.; Müller, F.A.; Barralet, J.E. Direct printing of bioceramic implants with spatially localized angiogenic factors. Adv. Mater. 2007, 19, 795–800. [Google Scholar] [CrossRef]
- Igawa, K.; Mochizuki, M.; Sugimori, O.; Shimizu, K.; Yamazawa, K.; Kawaguchi, H.; Nakamura, K.; Takato, T.; Nishimura, R.; Suzuki, S.; et al. Tailor-made tricalcium phosphate bone implant directly fabricated by a three-dimensional ink-jet printer. J. Artif. Organs 2006, 9, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Komlev, V.S.; Popov, V.K.; Mironov, A.V.; Fedotov, A.Y.; Teterina, A.Y.; Smirnov, I.V.; Bozo, I.Y.; Rybko, V.A.; Deev, R.V. 3D Printing of Octacalcium Phosphate Bone Substitutes. Front. Bioeng. Biotechnol. 2015, 3, 81. [Google Scholar] [CrossRef] [PubMed]
- Gbureck, U.; Hölzel, T.; Klammert, U.; Würzler, K.; Müller, F.A.; Barralet, J.E. Resorbable dicalcium phosphate bone substitutes prepared by 3D powder printing. Adv. Funct. Mater. 2007, 17, 3940–3945. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, K.; Li, X.; Wei, Q.; Chai, W.; Wang, S.; Che, Y.; Lu, T.; Zhang, B. 3D fabrication and characterization of phosphoric acid scaffold with a HA/β-TCP weight ratio of 60:40 for bone tissue engineering applications. PLoS ONE 2017, 12, e0174870. [Google Scholar] [CrossRef] [PubMed]
- Mandal, S.; Meininger, S.; Gbureck, U.; Basu, B. 3D powder printed tetracalcium phosphate scaffold with phytic acid binder: Fabrication, microstructure and in situ X-Ray tomography analysis of compressive failure. J. Mater. Sci. Mater. Med. 2018, 29. [Google Scholar] [CrossRef] [PubMed]
- Klammert, U.; Reuther, T.; Jahn, C.; Kraski, B.; Kübler, A.C.; Gbureck, U. Cytocompatibility of brushite and monetite cell culture scaffolds made by three-dimensional powder printing. Acta Biomater. 2009, 5, 727–734. [Google Scholar] [CrossRef] [PubMed]
- Tamimi, F.; Torres, J.; Gbureck, U.; Lopez-Cabarcos, E.; Bassett, D.C.; Alkhraisat, M.H.; Barralet, J.E. Craniofacial vertical bone augmentation: A comparison between 3D printed monolithic monetite blocks and autologous onlay grafts in the rabbit. Biomaterials 2009, 30, 6318–6326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asadi-Eydivand, M.; Solati-Hashjin, M.; Shafiei, S.S.; Mohammadi, S.; Hafezi, M.; Osman, N.A.A. Structure, properties, and in vitro behavior of heat-treated calcium sulfate scaffolds fabricated by 3D printing. PLoS ONE 2016, 11, e0151216. [Google Scholar] [CrossRef] [PubMed]
- Klammert, U.; Vorndran, E.; Reuther, T.; Müller, F.A.; Zorn, K.; Gbureck, U. Low temperature fabrication of magnesium phosphate cement scaffolds by 3D powder printing. J. Mater. Sci. Mater. Med. 2010, 21, 2947–2953. [Google Scholar] [CrossRef] [PubMed]
- Seitz, H.; Rieder, W.; Irsen, S.; Leukers, B.; Tille, C. Three-dimensional printing of porous ceramic scaffolds for bone tissue engineering. J. Biomed. Mater. Res. Part B Appl. Biomater. 2005, 74, 782–788. [Google Scholar] [CrossRef] [PubMed]
- Stevanovic, S.; Chavanne, P. Improvement of Mechanical Properties of 3D Printed Hydroxyapatite Scaffolds by Polymeric Infiltration. Bioceram. Dev. Appl. 2013, 3, 10–12. [Google Scholar] [CrossRef]
- Spath, S.; Drescher, P.; Seitz, H. Impact of particle size of ceramic granule blends on mechanical strength and porosity of 3D printed scaffolds. Materials 2015, 8, 4720–4732. [Google Scholar] [CrossRef] [PubMed]
- Warnke, P.H.; Seitz, H.; Warnke, F.; Becker, S.T.; Sivananthan, S.; Sherry, E.; Liu, Q.; Wiltfang, J.; Douglas, T. Ceramic scaffolds produced by computer-assisted 3D printing and sintering: Characterization and biocompatibility investigations. J. Biomed. Mater. Res. Part B Appl. Biomater. 2010, 93, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Bagher, Z.; Rajaei, F.; Shokrgozar, M. Comparative study of bone repair using porous hydroxyapatite/β-tricalcium phosphate and xenograft scaffold in rabbits with tibia defect. Iran. Biomed. J. 2012, 16, 18–24. [Google Scholar] [PubMed]
- Peri, Z.; Kavehei, F.; Houshmand, A.; Franke, J.; Smeets, R.; Rimashevskiy, D.; Wenisch, S.; Schnettler, R.; Jung, O.; Barbeck, M. Purification processes of xenogeneic bone substitutes and their impact on tissue reactions and regeneration. Int. J. Artif. Organs 2018. [Google Scholar] [CrossRef]
- Dutta Roy, T.; Simon, J.L.; Ricci, J.L.; Rekow, E.D.; Thompson, V.P.; Parsons, J.R. Performance of hydroxyapatite bone repair scaffolds created via three-dimensional fabrication techniques. J. Biomed. Mater. Res. 2003, 67, 1228–1237. [Google Scholar] [CrossRef] [PubMed]
- Klammert, U.; Gbureck, U.; Vorndran, E.; Rödiger, J.; Meyer-Marcotty, P.; Kübler, A.C. 3D powder printed calcium phosphate implants for reconstruction of cranial and maxillofacial defects. J. Cranio-Maxillofac. Surg. 2010, 38, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Tarafder, S.; Balla, V.K.; Davies, N.M.; Bandyopadhyay, A.; Bose, S. Microwave-sintered 3D printed tricalcium phosphate scaffolds for bone tissue engineering. J. Tissue Eng. Regen. Med. 2013, 7, 631–641. [Google Scholar] [CrossRef] [PubMed]
- Seidenstuecker, M.; Kerr, L.; Bernstein, A.; Mayr, H.O.; Suedkamp, N.P.; Gadow, R.; Krieg, P.; Latorre, S.H.; Thomann, R.; Syrowatka, F.; et al. 3D powder printed bioglass and β-tricalcium phosphate bone scaffolds. Materials 2017, 11, 13. [Google Scholar] [CrossRef] [PubMed]
- Tarafder, S.; Davies, N.M.; Bandyopadhyay, A.; Bose, S. 3D printed tricalcium phosphate scaffolds: Effect of SrO and MgO doping on in vivo osteogenesis in a rat distal femoral defect model. Biomater. Sci. 2013, 1, 1250–1259. [Google Scholar] [CrossRef] [PubMed]
- Fielding, G.A.; Bandyopadhyay, A.; Bose, S. Effects of silica and zinc oxide doping on mechanical and biological properties of 3D printed tricalcium phosphate tissue engineering scaffolds. Dent. Mater. 2012, 28, 113–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shanjani, Y.; Hu, Y.; Pilliar, R.M.; Toyserkani, E. Mechanical characteristics of solid-freeform-fabricated porous calcium polyphosphate structures with oriented stacked layers. Acta Biomater. 2011, 7, 1788–1796. [Google Scholar] [CrossRef] [PubMed]
- Shanjani, Y.; Hu, Y.; Toyserkani, E.; Grynpas, M.; Kandel, R.A.; Pilliar, R.M. Solid freeform fabrication of porous calcium polyphosphate structures for bone substitute applications: In vivo studies. J. Biomed. Mater. Res. Part B Appl. Biomater. 2013, 101B, 972–980. [Google Scholar] [CrossRef] [PubMed]
- Ghanaati, S.; Barbeck, M.; Detsch, R.; Deisinger, U.; Hilbig, U.; Rausch, V.; Sader, R.; Unger, R.E.; Ziegler, G.; Kirkpatrick, C.J. The chemical composition of synthetic bone substitutes influences tissue reactions in vivo: Histological and histomorphometrical analysis of the cellular inflammatory response to hydroxyapatite, beta-tricalcium phosphate and biphasic calcium phosphate ceramics. Biomed. Mater. 2012, 7, 015005. [Google Scholar] [CrossRef] [PubMed]
- Ge, Z.; Wang, L.; Heng, B.C.; Tian, X.-F.; Lu, K.; Tai Weng Fan, V.; Yeo, J.F.; Cao, T.; Tan, E. Proliferation and Differentiation of Human Osteoblasts within 3D printed Poly-Lactic-co-Glycolic Acid Scaffolds. J. Biomater. Appl. 2009, 23, 533–547. [Google Scholar] [CrossRef]
- Simon, J.L.; Roy, T.D.; Parsons, J.R.; Rekow, E.D.; Thompson, V.P.; Kemnitzer, J.; Ricci, J.L. Engineered cellular response to scaffold architecture in a rabbit trephine defect. J. Biomed. Mater. Res. 2003, 66, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Sharaf, B.; Faris, C.B.; Abukawa, H.; Susarla, S.M.; Vacanti, J.P.; Kaban, L.B.; Troulis, M.J. Three-dimensionally printed polycaprolactone and β-tricalcium phosphate scaffolds for bone tissue engineering: An in vitro study. J. Oral Maxillofac. Surg. 2012, 70, 647–656. [Google Scholar] [CrossRef] [PubMed]
- Ozbolat, I.T.; Hospodiuk, M. Current advances and future perspectives in extrusion-based bioprinting. Biomaterials 2016, 76, 321–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suntornnond, R.; Tan, E.Y.S.; An, J.; Chua, C.K. A Mathematical Model on the Resolution of Extrusion Bioprinting for the Development of New Bioinks. Materials 2016, 9, 756. [Google Scholar] [CrossRef] [PubMed]
- Sultana, N.; Hassan, M.I.; Lim, M.M. Composite Synthetic Scaffolds for Tissue Engineering and Regenerative Medicine; Springer: Cham, Switzerland, 2015; pp. 13–25. [Google Scholar]
- Feilden, E.; Ferraro, C.; Zhang, Q.; García-Tuñón, E.; D’Elia, E.; Giuliani, F.; Vandeperre, L.; Saiz, E. 3D Printing Bioinspired Ceramic Composites. Sci. Rep. 2017, 7, 13759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gregor, A.; Filová, E.; Novák, M.; Kronek, J.; Chlup, H.; Buzgo, M.; Blahnová, V.; Lukášová, V.; Bartoš, M.; Nečas, A.; et al. Designing of PLA scaffolds for bone tissue replacement fabricated by ordinary commercial 3D printer. J. Biol. Eng. 2017, 11, 31. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, B.N.; Aprile, P.; Kelly, D.J.; Thiré, R.M.S.M. Evaluation of BMSCs response to PLA Scaffolds produced by FDM and Coating with Dopamine and Collagen. In Proceedings of the 9° Congresso Latino-Americano de Orgãos Artificiais e Biomateriais, Foz do Iguaçu, Brazil, 24–27 August 2016. [Google Scholar] [CrossRef]
- Teixeira, B.; Maia-Pinto, M.O.C.; Calasans-Maia, M.D.; Kelly, D.J.; Thiré, R.M.S.M. Structural Evaluation of PLA Scaffolds Obtained by 3D Printing via Fused Deposition Modeling (FDM) Technique for Applications in Tissue Engineering. In Proceedings of the 5° Edição do Workshop de Biomateriais, Engenharia de Tecidos e Orgãos Artificiais, Maresias, SP, Brazil, 20–24 August 2017; pp. 3–6. [Google Scholar]
- Tellis, B.C.; Szivek, J.A.; Bliss, C.L.; Margolis, D.S.; Vaidyanathan, R.K.; Calvert, P. Trabecular scaffolds created using micro CT guided fused deposition modeling. Mater. Sci. Eng. C 2008, 28, 171–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.Y.; Cho, D.W. Blended PCL/PLGA scaffold fabrication using multi-head deposition system. Microelectron. Eng. 2009, 86, 1447–1450. [Google Scholar] [CrossRef]
- Hutmacher, D.W.; Schantz, T.; Zein, I.; Ng, K.W.; Teoh, S.H.; Tan, K.C. Mechanical properties and cell cultural response of polycaprolactone scaffolds designed and fabricated via fused deposition modeling. J. Biomed. Mater. Res. 2001, 55, 203–216. [Google Scholar] [CrossRef]
- Wang, F.; Shor, L.; Darling, A.; Khalil, S.; Sun, W.; Güçeri, S.; Lau, A. Precision extruding deposition and characterization of cellular poly-ε-caprolactone tissue scaffolds. Rapid Prototyp. J. 2004, 10, 42–49. [Google Scholar] [CrossRef]
- Gonçalves, E.M.; Oliveira, F.J.; Silva, R.F.; Neto, M.A.; Fernandes, M.H.; Amaral, M.; Vallet-Regí, M.; Vila, M. Three-dimensional printed PCL-hydroxyapatite scaffolds filled with CNTs for bone cell growth stimulation. J. Biomed. Mater. Res. Part B Appl. Biomater. 2016, 104, 1210–1219. [Google Scholar] [CrossRef] [PubMed]
- Boga, J.C.; Miguel, S.P.; de Melo-Diogo, D.; Mendonça, A.G.; Louro, R.O.; Correia, I.J. In vitro characterization of 3D printed scaffolds aimed at bone tissue regeneration. Colloids Surf. B Biointerfaces 2018, 165, 207–218. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Vázquez, F.J.; Perera, F.H.; Miranda, P.; Pajares, A.; Guiberteau, F. Improving the compressive strength of bioceramic robocast scaffolds by polymer infiltration. Acta Biomater. 2010, 6, 4361–4368. [Google Scholar] [CrossRef] [PubMed]
- Entezari, A.; Roohani-Esfahani, S.I.; Zhang, Z.; Zreiqat, H.; Dunstan, C.R.; Li, Q. Fracture behaviors of ceramic tissue scaffolds for load bearing applications. Sci. Rep. 2016, 6, 28816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhong, G.; Vaezi, M.; Liu, P.; Pan, L.; Yang, S. Characterization approach on the extrusion process of bioceramics for the 3D printing of bone tissue engineering scaffolds. Ceram. Int. 2017, 43, 13860–13868. [Google Scholar] [CrossRef]
- Mangano, C.; Barboni, B.; Valbonetti, L.; Berardinelli, P.; Martelli, A.; Muttini, A.; Bedini, R.; Tetè, S.; Piattelli, A.; Mattioli, M. In Vivo Behavior of a Custom-Made 3D Synthetic Bone Substitute in Sinus Augmentation Procedures in Sheep. J. Oral Implantol. 2015, 41, 240–250. [Google Scholar] [CrossRef] [PubMed]
- Belay, M.; Nagarale, R.K.; Verma, V. Preparation and characterization of graphene-agar and graphene oxide-agar composites. J. Appl. Polym. Sci. 2017, 134, 45085. [Google Scholar] [CrossRef]
- Lopez, C.D.; Diaz-Siso, J.R.; Witek, L.; Bekisz, J.M.; Cronstein, B.N.; Torroni, A.; Flores, R.L.; Rodriguez, E.D.; Coelho, P.G. Three dimensionally printed bioactive ceramic scaffold osseoconduction across critical-sized mandibular defects. J. Surg. Res. 2018, 223, 115–122. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, M.D.; Hill, R.G. Influence of strontium and the importance of glass chemistry and structure when designing bioactive glasses for bone regeneration. Acta Biomater. 2010, 6, 2382–2385. [Google Scholar] [CrossRef] [PubMed]
- Arora, M.; Arora, E. The Promise of Silicon: Bone regeneration and increased bone density. J. Arthrosc. Jt. Surg. 2017, 4, 103–105. [Google Scholar] [CrossRef]
- Glenske, K.; Donkiewicz, P.; Köwitsch, A.; Milosevic-Oljaca, N.; Rider, P.; Rofall, S.; Franke, J.; Jung, O.; Smeets, R.; Schnettler, R.; et al. Applications of Metals for Bone Regeneration. Int. J. Mol. Sci. 2018, 19, 826. [Google Scholar] [CrossRef] [PubMed]
- Deng, C.; Zhu, H.; Li, J.; Feng, C.; Yao, Q.; Wang, L.; Chang, J.; Wu, C. Bioactive scaffolds for regeneration of cartilage and subchondral bone interface. Theranostics 2018, 8, 1940–1955. [Google Scholar] [CrossRef] [PubMed]
- Roohani-Esfahani, S.-I.; Newman, P.; Zreiqat, H. Design and Fabrication of 3D printed Scaffolds with a Mechanical Strength Comparable to Cortical Bone to Repair Large Bone Defects. Sci. Rep. 2016, 6, 19468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grémare, A.; Guduric, V.; Bareille, R.; Heroguez, V.; Latour, S.; L’heureux, N.; Fricain, J.C.; Catros, S.; Le Nihouannen, D. Characterization of printed PLA scaffolds for bone tissue engineering. J. Biomed. Mater. Res. Part A 2018, 106, 887–894. [Google Scholar] [CrossRef] [PubMed]
- Vozzi, G.; Corallo, C.; Daraio, C. Pressure-activated microsyringe composite scaffold of poly(l-lactic acid) and carbon nanotubes for bone tissue engineering. J. Appl. Polym. Sci. 2013, 129, 528–536. [Google Scholar] [CrossRef]
- Lee, K.-G.; Lee, K.-S.; Kang, Y.-J.; Hwang, J.-H.; Lee, S.-H.; Park, S.-H.; Park, Y.; Cho, Y.-S.; Lee, B.-K. Rabbit Calvarial Defect Model for Customized 3D-Printed Bone Grafts. Tissue Eng. Part C Methods 2018. [Google Scholar] [CrossRef] [PubMed]
- Kawai, T.; Shanjani, Y.; Fazeli, S.; Behn, A.W.; Okuzu, Y.; Goodman, S.B.; Yang, Y.P. Customized, degradable, functionally graded scaffold for potential treatment of early stage osteonecrosis of the femoral head. J. Orthop. Res. 2018, 36, 1002–1011. [Google Scholar] [CrossRef] [PubMed]
- Nyberg, E.; Rindone, A.; Dorafshar, A.; Grayson, W.L. Comparison of 3D-Printed Poly-ε-Caprolactone Scaffolds Functionalized with Tricalcium Phosphate, Hydroxyapatite, Bio-Oss, or Decellularized Bone Matrix. Tissue Eng. Part A 2017, 23, 503–514. [Google Scholar] [CrossRef] [PubMed]
- Bacakova, L.; Grausova, L.; Vacik, J.; Fraczek, A.; Blazewicz, S.; Kromka, A.; Vanecek, M.; Svorcik, V. Improved adhesion and growth of human osteoblast-like MG 63 cells on biomaterials modified with carbon nanoparticles. Diam. Relat. Mater. 2007, 16, 2133–2140. [Google Scholar] [CrossRef]
- Lee, H.H.; Shin, U.S.; Jin, G.Z.; Kim, H.W. Highly homogeneous carbon nanotube-polycaprolactone composites with various and controllable concentrations of ionically-modified-MWCNTs. Bull. Korean Chem. Soc. 2011, 32, 157–161. [Google Scholar] [CrossRef]
- Rim, N.G.; Lee, J.H.; Jeong, S.I.; Lee, B.K.; Kim, C.H.; Shin, H. Modulation of Osteogenic Differentiation of Human Mesenchymal Stem Cells by Poly[(l-lactide)-co-(ε-caprolactone)]/Gelatin Nanofibers. Macromol. Biosci. 2009, 9, 795–804. [Google Scholar] [CrossRef] [PubMed]
- Arafat, M.T.; Lam, C.X.F.; Ekaputra, A.K.; Wong, S.Y.; Li, X.; Gibson, I. Biomimetic composite coating on rapid prototyped scaffolds for bone tissue engineering. Acta Biomater. 2011, 7, 809–820. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Hutmacher, D.W.; Varawan, S.-L.; Lim, T.M. In vitro bone engineering based on polycaprolactone and polycaprolactone–tricalcium phosphate composites. Polym. Int. 2007, 56, 333–342. [Google Scholar] [CrossRef]
- Kim, S.E.; Shim, K.M.; Jang, K.; Shim, J.H.; Kang, S.S. Three-dimensional printing-based reconstruction of a maxillary bone defect in a dog following tumor removal. In Vivo 2018, 32, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Shanjani, Y.; Pan, C.C.; Elomaa, L.; Yang, Y. A novel bioprinting method and system for forming hybrid tissue engineering constructs. Biofabrication 2015, 7, 045008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trachtenberg, J.E.; Placone, J.K.; Smith, B.T.; Fisher, J.P.; Mikos, A.G. Extrusion-based 3D printing of poly(propylene fumarate) scaffolds with hydroxyapatite gradients. J. Biomater. Sci. Polym. Ed. 2017, 28, 532–554. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Scaffold Mechanical Properties | Porosity (%) | Cell Viability | References |
|---|---|---|---|---|
| GelMA (Irgacure 2959) | 30 kPa * at the highest degree of methacrylation | Non-porous | Highest cell viability was reported in the lowest concentration of GelMA, 80–95% | [29] |
| SilMA (LAP) | 910 kPa ** at the highest percentage of Sil-MA | / | SilMA exhibited similar absorbance in a cck-8 assay as GelMA | [32] |
| GelMA:SF (Irgacure 2959) | Reached 75 kPa ** with the highest concentration of SF | 41.8 | Highest OD values was over 2.0, a little bit higher than the metabolic activity of pure GelMA | [30] |
| Chitosan:PEGDA (Irgacure 819) | ~1000 kPa * at the highest concentration of PEGDA | Non-porous | Ratios of 1:5 and 1:10 of Chitosan:PEGDA exhibited the highest cell viability percentages 93–97% | [33] |
| Methacry. PCL/BG (Lucirin TPO-L) | 3.4 MPa/dry * 2.5 MPa/wet * | 63 | Highest metabolic activity at highest BG concentration | [34] |
| CP CP/PCL | 2.04 ± 0.12 MPa ** 4.55 ± 0.21 MPa ** | / | CP:PCL had lower proliferation than pure CP but exhibited higher osteogenic markers expression | [35] |
| Methacrylated Alginate (VA-086) | 3.3–12.4 kPa ** depending on the photoinitiator content | Non-porous | 75% at moderate stiffness | [36] |
| Methacrylated PCL (Irgacure 2959, 369) | 2.02 ± 2.87 MPa ** | 70.5 ± 0.8 | Similar metabolic activity as in tissue culture polystyrene | [37] |
| PETMP:PEG-DVE | 6.9 ± 1.8 MPa * | Non-porous | 95% viability was exhibited in 120 h | [38] |
| Methacrylated PLA (camphorquinone) | 9.43 ± 3.2 MPa with intermediate content of HA and highest content of TEGDMA (flexural strength) | / | Samples with highest TEGDMA and HA content exhibited better cell viability. | [39] |
| PTMC/HA (Lucirin TPO-L) | / | 70 | Addition of HA and TEGDMA promoted better cell attachment and proliferation | [40] |
| Material | Scaffold Compressive Strength (MPa) | Porosity (%) | Biological Response | References |
|---|---|---|---|---|
| Magnesium silicate (Mg2SiO4) | 40.29 ± 1.32 MPa | / | / | [61] |
| β-TCP/ZnO | 17.89 MPa with 2.5 wt % ZnO | 56.8 | MG-63 cells indicated better attachment and proliferation with increased ZnO | [62] |
| HA/β-TCP | 18.35 MPa with 30 wt % β-TCP | ~61 | MG-63 cells exhibited better attachment and morphology on scaffolds with 30 wt % and 50 wt % | [63] |
| PCL | 2.3 MPa | 50 | Implanted in minipigs, exhibited full healing in 3 months | [64] |
| PCL/β-TCP | 6 MPa * with 10 wt % β-TCP | 68 | Pure β-TCP exhibited better ingrowth than polymer/ceramic composite | [65] |
| PCL/HA | 3.17 MPa with 15 wt % HA | 70.31 | PCL/HA scaffolds exhibited better bioactivity than pure PCL after 28 days | [66] |
| PHBV/CP | 0.55 MPa with 15 wt % CP | 62.6 ± 1.2 | The incorporation of CP nanoparticles significantly improved cell proliferation and alkaline phosphatase activity | [67] |
| PLLA/CHA | Over 0.6 MPa with 10 wt % CHA | 66.8 ± 2.5 | Cellular response similar to pure PLLA | [67] |
| Material | Binder | Porosity (%) | Compressive Strength (MPa) | Biological Response | References |
|---|---|---|---|---|---|
| HA | phosphoric acid 10% + 1 M NaH2PO4 | 60 59 * | 1.9 ± 0.2 5.8 ± 0.3 * | Implanted into mice, there was minimal tissue penetration. | [84] |
| α-TCP | Sodium chondroitin sulfate 5% + disodium succinate 12% | 61 | 18.6 | Implanted into beagle dogs, experienced bony bridging, bone formation and the presence of bone marrow. | [85] |
| β-TCP | Phosphoric acid 1 wt % | / | 2.5 7.5 * | Cranial plates implanted into mice, exhibited bone integration around edges and fibrous tissue in center. | [86] |
| β-TCP | Phosphoric acid 5 wt % Phosphoric acid 10 wt % Phosphoric acid 30 wt % | 53 50 41 | 0.9 ± 0.1 3.0 ± 0.3 8.7 ± 1.3 | When implanted, monetite and brushite degraded faster than the β-TCP | [87] |
| BCP (HA/β-TCP) | |||||
| 100:0 | PVA 0.6 wt % | 42 ± 2 | 1.54 ± 0.13 | Seeded with BMSCs, proliferation was highest for a HA/β-TCP ratio of 60:40 for both binder solutions. The scaffolds made with a PVA binder showed higher proliferation rates compared to the phosphoric acid samples. | |
| Phosphoric acid 8.75 wt % | 28 ± 2 | 2.81 ± 0.08 | |||
| 20:80 | PVA 0.6 wt % | 44 ± 2 | 1.21 ± 0.11 | ||
| Phosphoric acid 8.75 wt % | 49 ± 3 | 2.36 ± 0.18 | [88] | ||
| 40:60 | PVA 0.6 wt % | 43 ± 3 | 1.26 ± 0.09 | ||
| Phosphoric acid 8.75 wt % | 47 ± 2 | 2.57 ± 0.23 | |||
| 60:40 | PVA 0.6 wt % | 42 ± 1 | 1.35 ± 0.11 | ||
| Phosphoric acid 8.75 wt % | 49 ± 3 | 2.66 ± 0.20 | |||
| TTCP | Phytic acid 25 wt % | 39.4 ± 1.5 | 1.3 ± 0.2 4.0 ± 0.4 * | / | [89] |
| Brushite | Phosphoric acid 20 wt % | 38.8 | 23.4 ± 3.3 | Showed good biocompatibility when seeded with osteoblastic cells. | [90] |
| Phosphoric acid 20 wt % | 45 29 * | 5.3 ± 0.6 22.3 ± 1.5 * | When implanted, degraded slower than monetite samples, and over a 4-week period developed HA phases. | [87] | |
| Monetite | Phosphoric acid 20 wt % | 43.8 | 15.3 ± 1.1 | Showed good biocompatibility when seeded with osteoblastic cells. | [90] |
| Phosphoric acid 20 wt % | 44 | 15 * | After 8 weeks implanted into rabbits, had completely integrated/resorbed into native bone. | [91] | |
| Calcium Sulfate | 2-pyrrolidinone | 45.04 | 0.7 0.55 ** | Samples were non-cytotoxic when sintered above 1000 °C. | [92] |
| Struvite | Ammonium phosphate | / | 0.23 ± 1.37 7.01 ± 1.37 * | Osteoblastic cells showed good cell viability over 10 days. | [93] |
| Material | Porosity (%) | Compressive Strength (MPa) | Biological Response | References |
|---|---|---|---|---|
| Pluronic F-127 hydrogel | / | 50 MPa | / | [115] |
| PLA | 40% | 45.61 MPa | Metabolic activity and proliferation rate of osteosarcoma cells MG-63 did not have significant differences between each porosity. | [116] |
| PLA | 50–60% | 29.96 MPa | ||
| PLA | 60 ± 1.5% | 9.47 MPa | Better seeding and metabolic activity with collagen/dopamine coating | [117] |
| PLA | 55% | 13.25 ± 1.6 | Scaffolds with 66% porosity exhibited higher cell count | [118] |
| 60% | 9.47 ± 0.47 | |||
| 66% | 5.57 ± 0.27 | |||
| PBT | 62.11 ± 0.36% | 10.44 ± 2.09 MPa | / | [119] |
| PLGA/PCL | 69.6% | 12.9 MPa | Mesenchymal stem cells demonstrated good proliferation rates | [120] |
| PCL | 61 ± 1% | Dry 41.9 ± 3.5 MPa Wet 29.4 ± 4.0 MPa | Human fibroblasts and osteoprogenitor cells proliferated, differentiated and deposited ECM | [121] |
| PCL | 54.9% | / | Cardiomyoblasts attached to the structure, although a pore size of 250µm did not allow for cells to migrate. | [122] |
| PCL/HA/(0.2%) CNT PCL/HA | ~40% 57% | / | Higher concentrations of CNT enhanced cell adhesion and spreading of MG-63 cells | [123] |
| TCP/AA 60/40-GO TCP/AA, 60/40 | / / | / | Over a 21-day period, human osteoblasts had secreted mineral deposits | [124] |
| β-TCP PCL/β-TCP PLA/β-TCP | 49% | 20 ± 2 MPa 60 ± 10 MPa 130 ± 20 MPa | / | [125] |
| Sr-HT-Gahnite | 66.1% | 53 ± 9 MPA | / | [126] |
| 52.1% | 121 ± 12 MPa | |||
| 48.5% | 140 ± 15 MPa |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rider, P.; Kačarević, Ž.P.; Alkildani, S.; Retnasingh, S.; Schnettler, R.; Barbeck, M. Additive Manufacturing for Guided Bone Regeneration: A Perspective for Alveolar Ridge Augmentation. Int. J. Mol. Sci. 2018, 19, 3308. https://doi.org/10.3390/ijms19113308
Rider P, Kačarević ŽP, Alkildani S, Retnasingh S, Schnettler R, Barbeck M. Additive Manufacturing for Guided Bone Regeneration: A Perspective for Alveolar Ridge Augmentation. International Journal of Molecular Sciences. 2018; 19(11):3308. https://doi.org/10.3390/ijms19113308
Chicago/Turabian StyleRider, Patrick, Željka Perić Kačarević, Said Alkildani, Sujith Retnasingh, Reinhard Schnettler, and Mike Barbeck. 2018. "Additive Manufacturing for Guided Bone Regeneration: A Perspective for Alveolar Ridge Augmentation" International Journal of Molecular Sciences 19, no. 11: 3308. https://doi.org/10.3390/ijms19113308