Molecular and Clinical Issues about the Risk of Venous Thromboembolism in Older Patients: A Focus on Parkinson’s Disease and Parkinsonism

 and
and
Abstract
:1. Introduction
2. VTE in Older Patients: Results from Epidemiologic Studies
3. Etiology of VTE in Older Patients
4. Aging-Related Inflammation and Consequent Risk of Thrombosis: Molecular Mechanisms
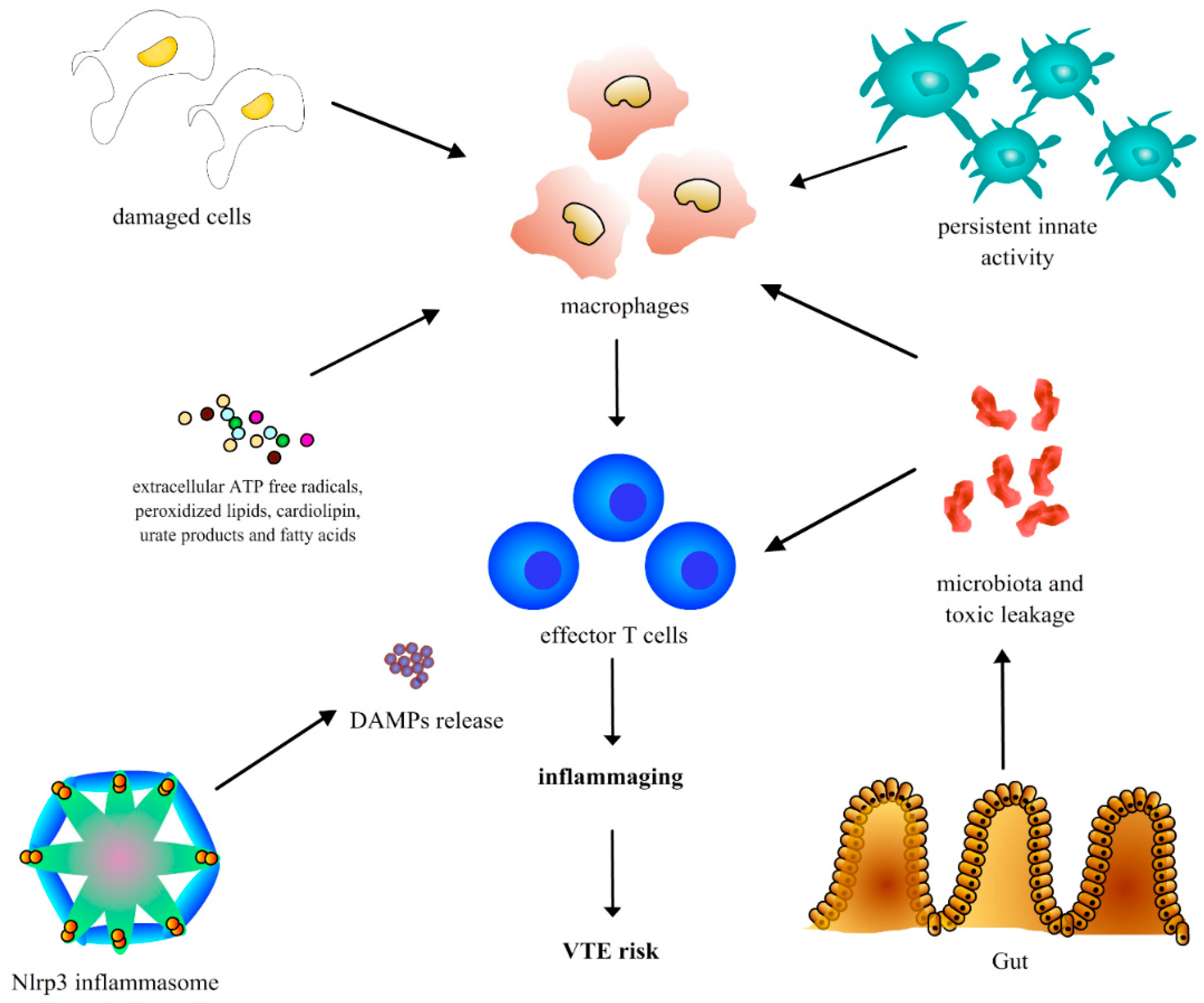
4.1. Chronic Inflammation in the Elderly (Inflammaging)
4.2. Chronic Inflammation, Oxidative Stress and Parkinson’s Disease
5. The Complex Molecular Interplay between the Three Components of the Virchow’s Triad and the Influence of Aging
5.1. Vascular Endothelial Dysfunction
5.2. Hypercoagulable Conditions
5.3. Functional Limitation, Muscle Strength Reduction and Blood Stasis
6. The Comprehensive Geriatric Assessment as a Useful Tool for VTE Risk Identification
7. Risk Prevention in the Elderly: Proposals for Anticoagulant Strategies
7.1. Risk-Benefit Ratio of Thromboprophylaxis in Older Patients
7.2. VTE Prevention in Older Patients
7.3. Tailored Approaches for the Treatment of VTE in the Elderly
7.4. Advantages and Limitations of Novel Oral Anticoagulants in the Elderly
8. VTE Prevention and the Pleiotropic Effects of Acetylsalicylic Acid and Other Antiplatelet Drugs
9. Conclusions
Acknowledgments
Conflicts of Interest
References
- Becattini, C.; Agnelli, G. Acute pulmonary embolism: Mortality prediction by the 2014 European Society of Cardiology risk stratification model. Eur. Respir. J. 2017, 49, 780–786. [Google Scholar] [CrossRef] [PubMed]
- Engbers, M.J.; van Hylckama Vlieg, A.; Rosendaal, F.R. Venous thrombosis in the elderly: Incidence, risk factors and risk groups. J. Thromb. Haemost. 2010, 8, 2105–2112. [Google Scholar] [CrossRef] [PubMed]
- Spencer, F.A.; Emery, C.; Lessard, D.; Anderson, F.; Emani, S.; Aragam, J.; Becker, R.C.; Goldberg, R.J. The Worcester Venous Thromboembolismstudy: A population-based study of the clinical epidemiology of venous thromboembolism. J. Gen. Intern. Med. 2006, 21, 722–727. [Google Scholar] [CrossRef] [PubMed]
- Spencer, F.A.; Emery, C.; Joffe, S.W.; Pacifico, L.; Lessard, D.; Reed, G.; Gore, J.M.; Goldberg, R.J. Incidence rates, clinical profile, and outcomes of patients with venous thromboembolism. The Worcester VTE study. J. Thromb. Thrombolysis 2009, 28, 401–409. [Google Scholar] [CrossRef] [PubMed]
- Spencer, F.A.; Gore, J.M.; Lessard, D.; Emery, C.; Pacifico, L.; Reed, G.; Gurwitz, J.H.; Goldberg, R.J. Venous thromboembolism in the elderly. A community-based perspective. Thromb. Haemost. 2008, 100, 780–788. [Google Scholar] [PubMed]
- Spencer, F.A.; Gurwitz, J.H.; Schulman, S.; Linkins, L.A.; Crowther, M.A.; Ginsberg, J.S.; Lee, A.Y.; Saczynski, J.S.; Anand, S.; Lessard, D.; et al. Venous thromboembolism in older adults: A community-based study. Am. J. Med. 2014, 127, 530–537. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.C.; Kao, C.C. Cardiovascular diseases and the risk of venous thromboembolism: A hospital-based case-control study. J. Chin. Med. Assoc. 2007, 70, 103–109. [Google Scholar] [CrossRef]
- Sobel, B.E.; Schneider, D.J. Platelet function, coagulopathy, and impaired fibrinolysis in diabetes. Cardiol. Clin. 2004, 22, 511–526. [Google Scholar] [CrossRef] [PubMed]
- Erelel, M.; Cuhadaroglu, C.; Ece, T.; Arseven, O. The frequency of deep venous thrombosis and pulmonary embolus in acute exacerbation of chronic obstructive pulmonary disease. Respir. Med. 2002, 96, 515–518. [Google Scholar] [CrossRef] [PubMed]
- Sellier, E.; Labarere, J.; Sevestre, M.A.; Belmin, J.; Thiel, H.; Couturier, P.; Bosson, J.L. Risk factors for deep vein thrombosis in older patients: A multicenter study with systematic compression ultrasonography in postacute care facilities in France. J. Am. Geriatr. Soc. 2008, 56, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Ginsberg, J.S. Management of venous thromboembolism. N. Engl. J. Med. 1996, 335, 1816–1828. [Google Scholar] [CrossRef] [PubMed]
- Franceschi, C.; Campisi, J. Chronic inflammation (inflammaging) and its potential contribution to age-associated diseases. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69 (Suppl. 1), S4–S9. [Google Scholar] [CrossRef] [PubMed]
- Ferrucci, L.; Corsi, A.; Lauretani, F.; Bandinelli, S.; Bartali, B.; Taub, D.D.; Guralnik, J.M.; Longo, D.L. The origins of age-related proinflammatory state. Blood 2005, 105, 2294–2299. [Google Scholar] [CrossRef] [PubMed]
- Franceschi, C. Inflammaging as a major characteristic of old people: Can it be prevented or cured? Nutr. Rev. 2007, 65 Pt 2, S173–S176. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Raoof, M.; Chen, Y.; Sumi, Y.; Sursal, T.; Junger, W.; Brohi, K.; Itagaki, K.; Hauser, C.J. Circulating mitochondrial DAMPs cause inflammatory responses to injury. Nature 2010, 464, 104–107. [Google Scholar] [CrossRef] [PubMed]
- Biagi, E.; Candela, M.; Franceschi, C.; Brigidi, P. The aging gut microbiota: New perspectives. Ageing Res. Rev. 2011, 10, 428–429. [Google Scholar] [CrossRef] [PubMed]
- Franceschi, C.; Bonafè, M.; Valensin, S. Human immunosenescence: The prevailing of innate immunity, the failing of clonotypic immunity, and the filling of immunological space. Vaccine 2000, 18, 1717–1720. [Google Scholar] [CrossRef]
- Aksu, K.; Donmez, A.; Keser, G. Inflammation-induced thrombosis: Mechanisms, disease associations and management. Curr. Pharm. Des. 2012, 18, 1478–1493. [Google Scholar] [PubMed]
- Martinez, B.; Peplow, P.V. MicroRNAs in Parkinson’s disease and emerging therapeutic targets. Neural. Regen. Res. 2017, 12, 1945–1959. [Google Scholar] [PubMed]
- Hirsch, E.C.; Vyas, S.; Hunot, S. Neuroinflammation in Parkinson’s disease. Parkinsonism Relat. Disord. 2012, 18 (Suppl. 1), S210–S212. [Google Scholar] [CrossRef]
- Rocha, N.P.; de Miranda, A.S.; Teixeira, A.L. Insights into Neuroinflammation in Parkinson’s Disease: From Biomarkers to Anti-Inflammatory Based Therapies. Biomed. Res. Int. 2015, 2015, 628192. [Google Scholar] [CrossRef] [PubMed]
- Tana, C.; Giamberardino, M.A.; Cipollone, F. microRNA profiling in atherosclerosis, diabetes, and migraine. Ann. Med. 2017, 49, 93–105. [Google Scholar] [CrossRef] [PubMed]
- Mazzoccoli, G.; Fontana, A.; Grilli, M.; Dagostino, M.P.; Copetti, M.; Pellegrini, F.; Vendemiale, G. Idiopathic deep venous thrombosis and arterial endothelial dysfunction in the elderly. Age 2012, 34, 751–760. [Google Scholar] [CrossRef] [PubMed]
- Prandoni, P.; Ghirarduzzi, A.; Prins, M.H.; Pengo, V.; Davidson, B.L.; Sørensen, H.; Pesavento, R.; Iotti, M.; Casiglia, E.; Iliceto, S.; et al. Venous thromboembolism and the risk of subsequent symptomatic atherosclerosis. J. Thromb. Haemost. 2006, 4, 1891–1896. [Google Scholar] [CrossRef] [PubMed]
- Jezovnik, M.K.; Poredos, P.; Lusa, L. Idiopathic venous thrombosis is associated with preclinical atherosclerosis. J. Atheroscler. Thromb. 2010, 17, 304–311. [Google Scholar] [CrossRef] [PubMed]
- Bilato, C.; Crow, M.T. Atherosclerosis and the vascular biology of aging. Aging Clin. Exp. Res. 1996, 8, 221–234. [Google Scholar]
- King, E.; Thomas, A. Systemic Inflammation in Lewy Body Diseases: A Systematic Review. Alzheimer Dis. Assoc. Disord. 2017, 31, 346–356. [Google Scholar] [CrossRef] [PubMed]
- Korkmaz, H.; Onalan, O. Evaluation of endothelial dysfunction: Flow-mediated dilation. Endothelium 2008, 15, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Lind, L.; Fors, N.; Hall, J.; Marttala, K.; Stenborg, A. A comparison of three different methods to evaluate endothelium-dependent vasodilation in the elderly: The Prospective Investigation of the Vasculature in Uppsala Seniors (PIVUS) study. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 2368–2375. [Google Scholar] [CrossRef] [PubMed]
- Mazzoccoli, G.; Grilli, M.; Ferrandino, F.; Copetti, M.; Fontana, A.; Pellegrini, F.; Dagostino, M.P.; De Cata, A.; Vendemiale, G. Arterial endothelial dysfunction and idiopathic deep venous thrombosis. J. Biol. Regul. Homeost. Agents 2011, 25, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Mazzoccoli, G.; Dagostino, M.P.; Fontana, A.; Copetti, M.; Pellegrini, F.; Grilli, M.; Greco, A. Concomitant evaluation of flow-mediated vasodilation and epicardial fat thickness in idiopathic deep venous thrombosis. J. Biol. Regul. Homeost. Agents 2012, 26, 81–88. [Google Scholar] [PubMed]
- Alvarado-Moreno, J.A.; Hernandez-Lopez, R.; Chavez-Gonzalez, A.; Yoder, M.C.; Rangel-Corona, R.; Isordia-Salas, I.; Hernandez-Juarez, J.; Cerbulo-Vazquez, A.; Gonzalez-Jimenez, M.A.; Majluf-Cruz, A. Endothelial colony-forming cells: Biological and functional abnormalities in patients with recurrent, unprovoked venous thromboembolic disease. Thromb. Res. 2016, 137, 157–168. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Lopez, R.; Chavez-Gonzalez, A.; Torres-Barrera, P.; Moreno-Lorenzana, D.; Lopez-DiazGuerrero, N.; Santiago-German, D.; Isordia-Salas, I.; Smadja, D.; Yoder, M.C.; Majluf-Cruz, A.; et al. Reduced proliferation of endothelial colony-forming cells in unprovoked venous thromboembolic disease as a consequence of endothelial dysfunction. PLoS ONE 2017, 12, e0183827. [Google Scholar] [CrossRef] [PubMed]
- Karasu, A.; Engbers, M.J.; Cushman, M.; Rosendaal, F.R.; van Hylckama Vlieg, A. Genetic risk factors for venous thrombosis in the elderly in a case-control study. J. Thromb. Haemost. 2016, 14, 1759–1764. [Google Scholar] [CrossRef] [PubMed]
- Tsai, A.W.; Cushman, M.; Rosamond, W.D.; Heckbert, S.R.; Tracy, R.P.; Aleksic, N.; Folsom, A.R. Coagulation factors, inflammation markers, and venous thromboembolism: The longitudinal investigation of thromboembolism etiology (LITE). Am. J. Med. 2002, 113, 636–642. [Google Scholar] [CrossRef]
- Okamura, D.; Starr, M.E.; Lee, E.Y.; Stromberg, A.J.; Evers, B.M.; Saito, H. Age-dependent vulnerability to experimental acute pancreatitis is associated with increased systemic inflammation and thrombosis. Aging Cell 2012, 11, 760–769. [Google Scholar] [CrossRef] [PubMed]
- Mohebali, D.; Kaplan, D.; Carlisle, M.; Supiano, M.A.; Rondina, M.T. Alterations in platelet function during aging: Clinical correlations with thromboinflammatory disease in older adults. J. Am. Geriatr. Soc. 2014, 62, 529–535. [Google Scholar] [CrossRef] [PubMed]
- Paul, R.; Borah, A. L-DOPA-induced hyperhomocysteinemia in Parkinson’s disease: Elephant in the room. Biochim. Biophys. Acta 2016, 1860, 1989–1997. [Google Scholar] [CrossRef] [PubMed]
- Ospina-Romero, M.; Cannegieter, S.C.; den Heijer, M.; Doggen, C.J.M.; Rosendaal, F.R.; Lijfering, W.M. Hyperhomocysteinemia and Risk of First Venous Thrombosis: The Influence of (Unmeasured) Confounding Factors. Am. J. Epidemiol. 2018. [Google Scholar] [CrossRef]
- Piette, J.C.; Cacoub, P. Antiphospholipid syndrome in the elderly: Caution. Circulation 1998, 97, 2195–2196. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, N.M. Venous thrombosis of the lower limbs with particular reference to bed-rest. Br. J. Surg. 1957, 45, 209–236. [Google Scholar] [CrossRef] [PubMed]
- Olsen, H.; Länne, T. Reduced venous compliance in lower limbs of aging humans and its importance for capacitance function. Am. J. Physiol. 1998, 275 Pt 2, H878–H886. [Google Scholar] [CrossRef] [PubMed]
- Ferrucci, L.; Penninx, B.W.; Volpato, S.; Harris, T.B.; Bandeen-Roche, K.; Balfour, J.; Leveille, S.G.; Fried, L.P.; Md, J.M. Change in muscle strength explains accelerated decline of physical function in older women with high interleukin-6 serum levels. J. Am. Geriatr. Soc. 2002, 50, 1947–1954. [Google Scholar] [CrossRef] [PubMed]
- Taaffe, D.R.; Harris, T.B.; Ferrucci, L.; Rowe, J.; Seeman, T.E. Cross-sectional and prospective relationships of interleukin-6 and C-reactive protein with physical performance in elderly persons: MacArthur studies of successful aging. J. Gerontol. A Biol. Sci. Med. Sci. 2000, 55, M709–M715. [Google Scholar] [CrossRef] [PubMed]
- Cervellati, C.; Trentini, A.; Bosi, C.; Valacchi, G.; Morieri, M.L.; Zurlo, A.; Brombo, G.; Passaro, A.; Zuliani, G. Low-grade systemic inflammation is associated with functional disability in elderly people affected by dementia. Geroscience 2018, 40, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Aiello, A.E.; Haan, M.N.; Pierce, C.M.; Simanek, A.M.; Liang, J. Persistent infection, inflammation, and functional impairment in older Latinos. J. Gerontol. A Biol. Sci. Med. Sci. 2008, 63, 610–618. [Google Scholar] [CrossRef] [PubMed]
- Brinkley, T.E.; Leng, X.; Miller, M.E.; Kitzman, D.W.; Pahor, M.; Berry, M.J.; Marsh, A.P.; Kritchevsky, S.B.; Nicklas, B.J. Chronic inflammation is associated with low physical function in older adults across multiple comorbidities. J. Gerontol. A Biol. Sci. Med. Sci. 2009, 64, 455–461. [Google Scholar] [CrossRef] [PubMed]
- Llovera, M.; Lopez-Soriano, F.J.; Argiles, J.M. Effects of tumor necrosis factor-alpha on muscle-protein turnover in female Wistar rats. J. Natl. Cancer Inst. 1993, 85, 1334–1339. [Google Scholar] [CrossRef] [PubMed]
- Haddad, F.; Zaldivar, F.; Cooper, D.M.; Adams, G.R. IL-6-induced skeletal muscle atrophy. J. Appl. Physiol. 2005, 98, 911–917. [Google Scholar] [CrossRef] [PubMed]
- Haren, M.T.; Malmstrom, T.K.; Miller, D.K.; Patrick, P.; Perry, H.M., 3rd; Herning, M.M.; Banks, W.A.; Morley, J.E. Higher C-reactive protein and soluble tumor necrosis factor receptor levels are associated with poor physical function and disability: A cross-sectional analysis of a cohort of late middle-aged African Americans. J. Gerontol. A Biol. Sci. Med. Sci. 2010, 65, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Pottier, P.; Hardouin, J.B.; Lejeune, S.; Jolliet, P.; Gillet, B.; Planchon, B. Immobilization and the risk of venous thromboembolism. A meta-analysis on epidemiological studies. Thromb. Res. 2009, 124, 468–476. [Google Scholar] [CrossRef] [PubMed]
- Weill-Engerer, S.; Meaume, S.; Lahlou, A.; Piette, F.; Saint-Jean, O.; Sachet, A.; Beinis, J.Y.; Gallinari, C.; Grancher, A.S.; Vincent, J.P.; et al. Risk factors for deep vein thrombosis in inpatients aged 65 and older: A case-control multicenter study. J. Am. Geriatr. Soc. 2004, 52, 1299–1304. [Google Scholar] [CrossRef] [PubMed]
- Engbers, M.J.; Blom, J.W.; Cushman, M.; Rosendaal, F.R.; van Hylckama Vlieg, A. The contribution of immobility risk factors to the incidence of venous thrombosis in an older population. J. Thromb. Haemost. 2014, 12, 290–296. [Google Scholar] [CrossRef] [PubMed]
- Lauretani, F.; Maggio, M.; Giordano, A.; Ceda, G.P.; Nardelli, A. The risk of venous thromboembolism in older patients with advanced stages of Parkinson’s disease. Aging Clin. Exp. Res. 2013, 25, 229–230. [Google Scholar] [CrossRef] [PubMed]
- Engbers, M.J.; Blom, J.W.; Cushman, M.; Rosendaal, F.R.; van Hylckama Vlieg, A. Functional Impairment and Risk of Venous Thrombosis in Older Adults. J. Am. Geriatr. Soc. 2017, 65, 2003–2008. [Google Scholar] [CrossRef] [PubMed]
- Engbers, M.J.; Karasu, A.; Blom, J.W.; Cushman, M.; Rosendaal, F.R.; van Hylckama Vlieg, A. Clinical features of venous insufficiency and the risk of venous thrombosis in older people. Br. J. Haematol. 2015, 171, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Guralnik, J.M.; Ferrucci, L.; Simonsick, E.M.; Salive, M.E.; Wallace, R.B. Lower-extremity function in persons over the age of 70 years as a predictor of subsequent disability. N. Engl. J. Med. 1995, 332, 556–561. [Google Scholar] [CrossRef] [PubMed]
- Juby, A.; Tench, S.; Baker, V. The value of clock drawing in identifying executive cognitive dysfunction in people with a normal Mini-Mental State Examination score. CMAJ 2002, 167, 859–864. [Google Scholar] [PubMed]
- Inzitari, M.; Pozzi, C.; Ferrucci, L.; Chiarantini, D.; Rinaldi, L.A.; Baccini, M.; Pini, R.; Masotti, G.; Marchionni, N.; Di Bari, M. Subtle neurological abnormalities as risk factors for cognitive and functional decline, cerebrovascular events, and mortality in older community-dwelling adults. Arch. Intern. Med. 2008, 168, 1270–1276. [Google Scholar] [CrossRef] [PubMed]
- Pavasini, R.; Guralnik, J.; Brown, J.C.; di Bari, M.; Cesari, M.; Landi, F.; Vaes, B.; Legrand, D.; Verghese, J.; Wang, C.; et al. Short Physical Performance Battery and all-cause mortality: Systematic review and meta-analysis. BMC Med. 2016, 14, 215. [Google Scholar] [CrossRef] [PubMed]
- Penninx, B.W.; Ferrucci, L.; Leveille, S.G.; Rantanen, T.; Pahor, M.; Guralnik, J.M. Lower extremity performance in nondisabled older persons as a predictor of subsequent hospitalization. J. Gerontol. A Biol. Sci. Med. Sci. 2000, 55, M691–M697. [Google Scholar] [CrossRef] [PubMed]
- Tanji, H.; Gruber-Baldini, A.L.; Anderson, K.E.; Pretzer-Aboff, I.; Reich, S.G.; Fishman, P.S.; Weiner, W.J.; Shulman, L.M. A comparative study of physical performance measures in Parkinson’s disease. Mov. Disord. 2008, 23, 1897–1905. [Google Scholar] [CrossRef] [PubMed]
- Lauretani, F.; Ceda, G.P.; Pelliccioni, P.; Ruffini, L.; Nardelli, A.; Cherubini, A.; Maggio, M. Approaching neurological diseases to reduce mobility limitations in older persons. Curr. Pharm. Des. 2014, 20, 3149–3164. [Google Scholar] [CrossRef] [PubMed]
- Lauretani, F.; Ceda, G.P.; Nardelli, A.; Maggio, M. Should post-mortem brain dissection be performed in Parkinson’s disease with atypical dementia? Aging Clin. Exp. Res. 2015, 27, 103–105. [Google Scholar] [CrossRef] [PubMed]
- Yamane, K.; Kimura, F.; Unoda, K.; Hosokawa, T.; Hirose, T.; Tani, H.; Doi, Y.; Ishida, S.; Nakajima, H.; Hanafusa, T. Postural abnormality as a risk marker for leg deep venous thrombosis in Parkinson’s disease. PLoS ONE 2013, 8, e66984. [Google Scholar] [CrossRef] [PubMed]
- Farinola, N.; Caughey, G.E.; Bell, J.S.; Johns, S.; Hauta-Aho, M.; Shakib, S. Influence of stroke and bleeding risk on prescribing of oral anticoagulants in older inpatients; has the availability of direct oral anticoagulants changed prescribing? Ther. Adv. Drug Saf. 2018, 9, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Kooistra, H.A.; Calf, A.H.; Piersma-Wichers, M.; Kluin-Nelemans, H.C.; Izaks, G.J.; Veeger, N.J.; Meijer, K. Risk of Bleeding and Thrombosis in Patients 70 Years or Older Using Vitamin K Antagonists. JAMA Intern. Med. 2016, 176, 1176–1183. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, T.; Yasaka, M.; Kida, M.; Imura, M. A survey of reasons for continuing warfarin therapy in the era of direct oral anticoagulants in Japanese patients with atrial fibrillation: The SELECT study. Patient Prefer. Adherence 2018, 12, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Malato, A.; Dentali, F.; Siragusa, S.; Fabbiano, F.; Kagoma, Y.; Boddi, M.; Gensini, G.F.; Peris, A.; Crowther, M.; Napolitano, M. The impact of deep vein thrombosis in critically ill patients: A meta-analysis of major clinical outcomes. Blood Transfus. 2015, 13, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Kahn, S.R.; Lim, W.; Dunn, A.S.; Cushman, M.; Dentali, F.; Akl, E.A.; Cook, D.J.; Balekian, A.A.; Klein, R.C.; Le, H.; et al. Prevention of VTE in nonsurgical patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012, 141 (Suppl. 2), e195S–e226S. [Google Scholar] [CrossRef] [PubMed]
- Saheb Sharif-Askari, F.; Syed Sulaiman, S.A.; Saheb Sharif-Askari, N.; Al Sayed Hussain, A.; Railey, M.J. Adverse outcomes of anticoagulant use among hospitalized patients with chronic kidney disease: A comparison of the rates of major bleeding events between unfractionated heparin and enoxaparin. PLoS ONE 2014, 9, e106517. [Google Scholar] [CrossRef] [PubMed]
- MacLean, S.; Mulla, S.; Akl, E.A.; Jankowski, M.; Vandvik, P.O.; Ebrahim, S.; McLeod, S.; Bhatnagar, N.; Guyatt, G.H. Patient values and preferences in decision making for antithrombotic therapy: A systematic review: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012, 141 (Suppl. 2), e1S–e23S. [Google Scholar] [CrossRef] [PubMed]
- Ticinesi, A.; Lauretani, F.; Milani, C.; Nouvenne, A.; Tana, C.; Del Rio, D.; Maggio, M.; Ventura, M.; Meschi, T. Aging Gut Microbiota at the Cross-Road between Nutrition, Physical Frailty, and Sarcopenia: Is There a Gut-Muscle Axis? Nutrients 2017, 9, 1303. [Google Scholar] [CrossRef] [PubMed]
- Bucci, M.; Tana, C.; Giamberardino, M.A.; Cipollone, F. Lp(a) and cardiovascular risk: Investigating the hidden side of the moon. Nutr. Metab. Cardiovasc. Dis. 2016, 26, 980–986. [Google Scholar] [CrossRef] [PubMed]
- Lauretani, F.; Meschi, T.; Ticinesi, A.; Maggio, M. “Brain-muscle loop” in the fragility of older persons: From pathophysiology to new organizing models. Aging Clin. Exp. Res. 2017, 29, 1305–1311. [Google Scholar] [CrossRef] [PubMed]
- Cederholm, T.; Nouvenne, A.; Ticinesi, A.; Maggio, M.; Lauretani, F.; Ceda, G.P.; Borghi, L.; Meschi, T. The role of malnutrition in older persons with mobility limitations. Curr. Pharm. Des. 2014, 20, 3173–3177. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.N.; Morel-Kopp, M.C.; Pepperell, D.; Cumming, R.G.; Hilmer, S.N.; Ward, C.M. The impact of frailty on coagulation and responses to warfarin in acute older hospitalised patients with atrial fibrillation: A pilot study. Aging Clin. Exp. Res. 2017, 29, 1129–1138. [Google Scholar] [CrossRef] [PubMed]
- Walston, J.D.; Bandeen-Roche, K. Frailty: A tale of two concepts. BMC Med. 2015, 13, 185. [Google Scholar] [CrossRef] [PubMed]
- Ruan, Q.; Yu, Z.; Chen, M.; Bao, Z.; Li, J.; He, W. Cognitive frailty, a novel target for the prevention of elderly dependency. Ageing Res. Rev. 2015, 20, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Giorgi-Pierfranceschi, M.; Di Micco, P.; Cattabiani, C.; Guida, A.; Pagán, B.; Morales Mdel, V.; Salgado, E.; Suriñach, J.M.; Tolosa, C.; Monreal, M.; et al. Platelet Count and Major Bleeding in Patients Receiving Vitamin K Antagonists for Acute Venous Thromboembolism, Findings from Real World Clinical Practice. Medicine 2015, 94, e1915. [Google Scholar] [CrossRef] [PubMed]
- Silverstein, R.L.; Bauer, K.A.; Cushman, M.; Esmon, C.T.; Ershler, W.B.; Tracy, R.P. Venous thrombosis in the elderly: More questions than answers. Blood 2007, 110, 3097–3101. [Google Scholar] [CrossRef] [PubMed]
- Tana, M.; Tana, C.; Amerio, P.; Vitullo, G.; di Giosia, P.; di Febbo, C.; Davì, G. Severe non-traumatic bleeding, the answer is not in the blood. Intern. Emerg. Med. 2015, 10, 461–464. [Google Scholar] [CrossRef] [PubMed]
- Shendre, A.; Parmar, G.M.; Dillon, C.; Beasley, T.M.; Limdi, N.A. Influence of age on warfarin dose, anticoagulation control, and risk of hemorrhage. Pharmacotherapy 2018. [Google Scholar] [CrossRef] [PubMed]
- Narayan, S.W.; Nishtala, P.S. Population-based study examining the utilization of preventive medicines by older people in the last year of life. Geriatr. Gerontol. Int. 2018. [Google Scholar] [CrossRef] [PubMed]
- Siebenhofer, A.; Rakovac, I.; Kleespies, C.; Piso, B.; Didjurgeit, U. Self-management of oral anticoagulation in the elderly: Rationale, design, baselines and oral anticoagulation control after one year of follow-up: A randomized controlled trial. Thromb. Haemost. 2007, 97, 408–416. [Google Scholar] [PubMed]
- Sconce, E.; Avery, P.; Wynne, H.; Kamali, F. Vitamin K supplementation can improve stability of anticoagulation for patients with unexplained variability in response to warfarin. Blood 2007, 109, 2419–2423. [Google Scholar] [CrossRef] [PubMed]
- Becattini, C.; Agnelli, G. Treatment of Venous Thromboembolism with New Anticoagulant Agents. J. Am. Coll. Cardiol. 2016, 67, 1941–1955. [Google Scholar] [CrossRef] [PubMed]
- Sardar, P.; Chatterjee, S.; Chaudhari, S.; Lip, G.Y. New oral anticoagulants in elderly adults: Evidence from a meta-analysis of randomized trials. J. Am. Geriatr. Soc. 2014, 62, 857–864. [Google Scholar] [CrossRef] [PubMed]
- Prins, M.H.; Lensing, A.W.; Bauersachs, R.; van Bellen, B.; Bounameaux, H.; Brighton, T.A.; Cohen, A.T.; Davidson, B.L.; Decousus, H.; Raskob, G.E.; et al. Oral rivaroxaban versus standard therapy for the treatment of symptomatic venous thromboembolism: A pooled analysis of the EINSTEIN-DVT and PE randomized studies. Thromb. J. 2013, 11, 21. [Google Scholar] [CrossRef] [PubMed]
- Sardar, P.; Chatterjee, S.; Herzog, E.; Pekler, G.; Mushiyev, S.; Pastori, L.J.; Visco, F.; Aronow, W.S. New oral anticoagulants in patients with cancer: Current state of evidence. Am. J. Ther. 2015, 22, 460–468. [Google Scholar] [CrossRef] [PubMed]
- Antiplatelet Trialists’ Collaboration. Collaborative overview of randomised trials of antiplatelet therapy—III: Reduction in venous thrombosis and pulmonary embolism by antiplatelet prophylaxis among surgical and medical patients. BMJ 1994, 308, 235–246. [Google Scholar]
- O’Brien, J.; Duncan, H.; Kirsh, G.; Allen, V.; King, P.; Hargraves, R.; Mendes, L.; Perera, T.; Catto, P.; Schofield, S.; et al. Prevention of pulmonary embolism and deep vein thrombosis with low dose aspirin: Pulmonary Embolism Prevention (PEP) trial. Lancet 2000, 355, 1295–1302. [Google Scholar]
- Joki, H.; Higashiyama, Y.; Nakae, Y.; Kugimoto, C.; Doi, H.; Kimura, K.; Kishida, H.; Ueda, N.; Nakano, T.; Takahashi, T.; et al. White matter hyperintensities on MRI in dementia with Lewy bodies, Parkinson's disease with dementia, and Alzheimer’s disease. J. Neurol. Sci. 2018, 385, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Manosalva, H.A.; Pio, F.; Jeerakathil, T.; Saqqur, M.; Camicioli, R.; Suchowersky, O. Vascular Parkinsonism in a Tertiary Care Stroke Prevention Clinic and the Development of a New Screening Strategy. J. Stroke Cerebrovasc. Dis. 2018, 27, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.P.; Chen, L.S.; Yen, M.F.; Fann, C.Y.; Chiu, Y.H.; Chen, H.H.; Pan, S.L. Parkinson’s disease is related to an increased risk of ischemic stroke-a population-based propensity score-matched follow-up study. PLoS ONE 2013, 8, e68314. [Google Scholar] [CrossRef] [PubMed]
- Ton, T.G.; Heckbert, S.R.; Longstreth, W.T., Jr.; Rossing, M.A.; Kukull, W.A.; Franklin, G.M.; Swanson, P.D.; Smith-Weller, T.; Checkoway, H. Nonsteroidal anti-inflammatory drugs and risk of Parkinson’s disease. Mov. Disord. 2006, 21, 964–969. [Google Scholar] [CrossRef] [PubMed]
- Gagne, J.J.; Power, M.C. Anti-inflammatory drugs and risk of Parkinson disease: A meta-analysis. Neurology 2010, 74, 995–1002. [Google Scholar] [CrossRef] [PubMed]
- Satizabal, C.L.; Beiser, A.S.; Chouraki, V.; Chêne, G.; Dufouil, C.; Seshadri, S. Incidence of Dementia over Three Decades in the Framingham Heart Study. N. Engl. J. Med. 2016, 374, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Amarenco, P. Learning from TARDIS: Time for more focused trials in stroke prevention. Lancet 2018. [Google Scholar] [CrossRef]
- Turner, G.M.; Calvert, M.; Feltham, M.G.; Ryan, R.; Finnikin, S.; Marshall, T. Clinical and Demographic Characteristics Associated with Suboptimal Primary Stroke and Transient Ischemic Attack Prevention: Retrospective Analysis. Stroke 2018. [Google Scholar] [CrossRef] [PubMed]
- Lindley, R. Stroke prevention in the very elderly. Stroke 2018. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Etiology | Molecular Mechanisms of Thrombotic Action | Prevalence (%) | Ref |
|---|---|---|---|
| Malignancy | Hypercoagulation, blood stasis | 10 | [6] |
| Immobilization | Blood stasis | 25 | [7] |
| CHF | Hypercoagulation, endothelial dysfunction, blood stasis (advanced stages) | 22 | [7] |
| DM | Hypercoagulation, endothelial dysfunction, blood stasis | 16 | [8] |
| COPD | Hypercoagulation, endothelial dysfunction | 11 | [9] |
| Genetic risk factors | Hypercoagulation | 7 | [2] |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tana, C.; Lauretani, F.; Ticinesi, A.; Prati, B.; Nouvenne, A.; Meschi, T. Molecular and Clinical Issues about the Risk of Venous Thromboembolism in Older Patients: A Focus on Parkinson’s Disease and Parkinsonism. Int. J. Mol. Sci. 2018, 19, 1299. https://doi.org/10.3390/ijms19051299
Tana C, Lauretani F, Ticinesi A, Prati B, Nouvenne A, Meschi T. Molecular and Clinical Issues about the Risk of Venous Thromboembolism in Older Patients: A Focus on Parkinson’s Disease and Parkinsonism. International Journal of Molecular Sciences. 2018; 19(5):1299. https://doi.org/10.3390/ijms19051299
Chicago/Turabian StyleTana, Claudio, Fulvio Lauretani, Andrea Ticinesi, Beatrice Prati, Antonio Nouvenne, and Tiziana Meschi. 2018. "Molecular and Clinical Issues about the Risk of Venous Thromboembolism in Older Patients: A Focus on Parkinson’s Disease and Parkinsonism" International Journal of Molecular Sciences 19, no. 5: 1299. https://doi.org/10.3390/ijms19051299