Vascular Adhesion Protein-1 (VAP-1) as Predictor of Radiographic Severity in Symptomatic Knee Osteoarthritis in the New York University Cohort


Abstract
:1. Introduction
2. Results
2.1. Baseline Characteristics of the Subjects in the New York University (NYU) Cohort
2.2. Elevated SSAO/sVAP-1 Levels in Synovial Fluid of OA Patients
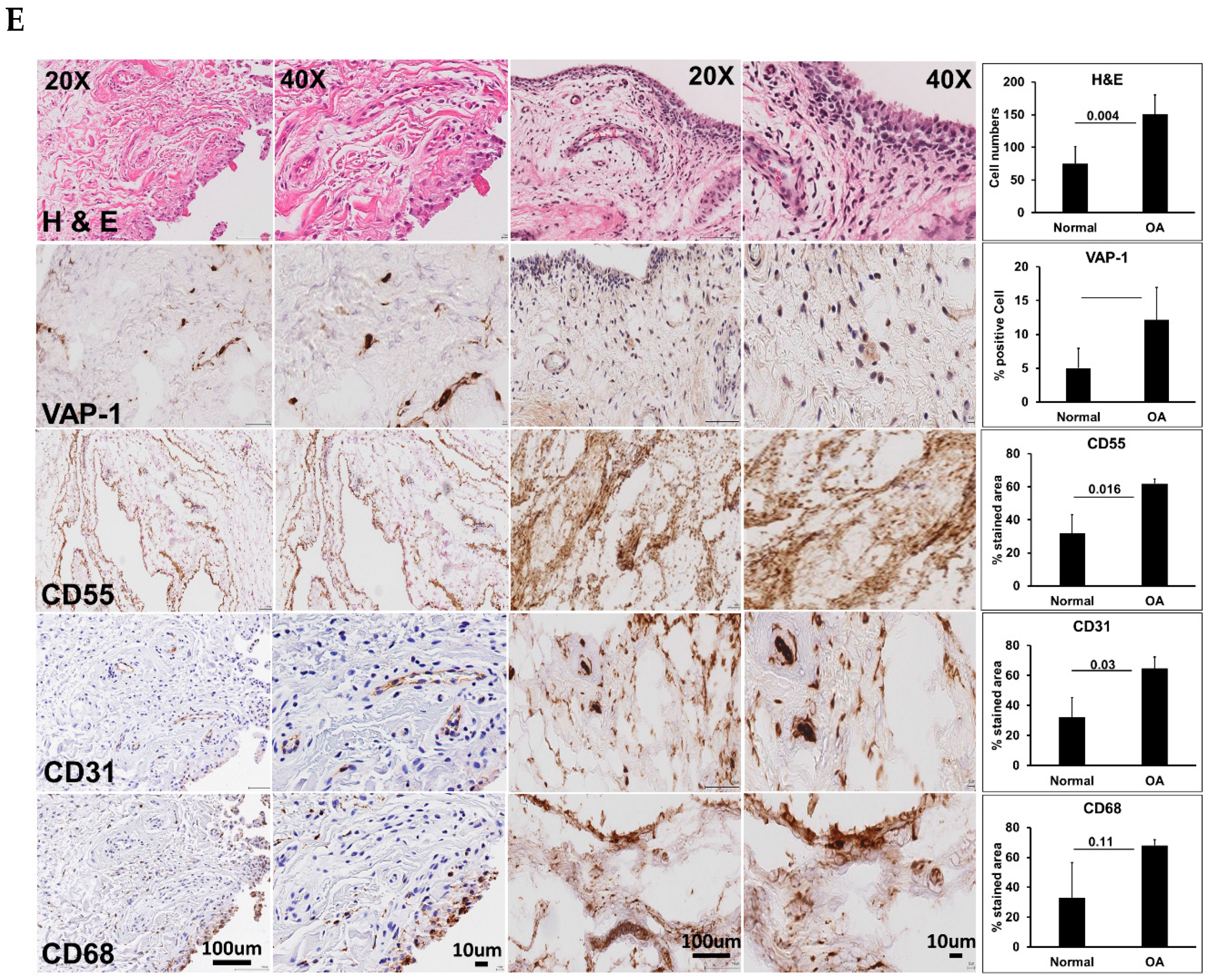
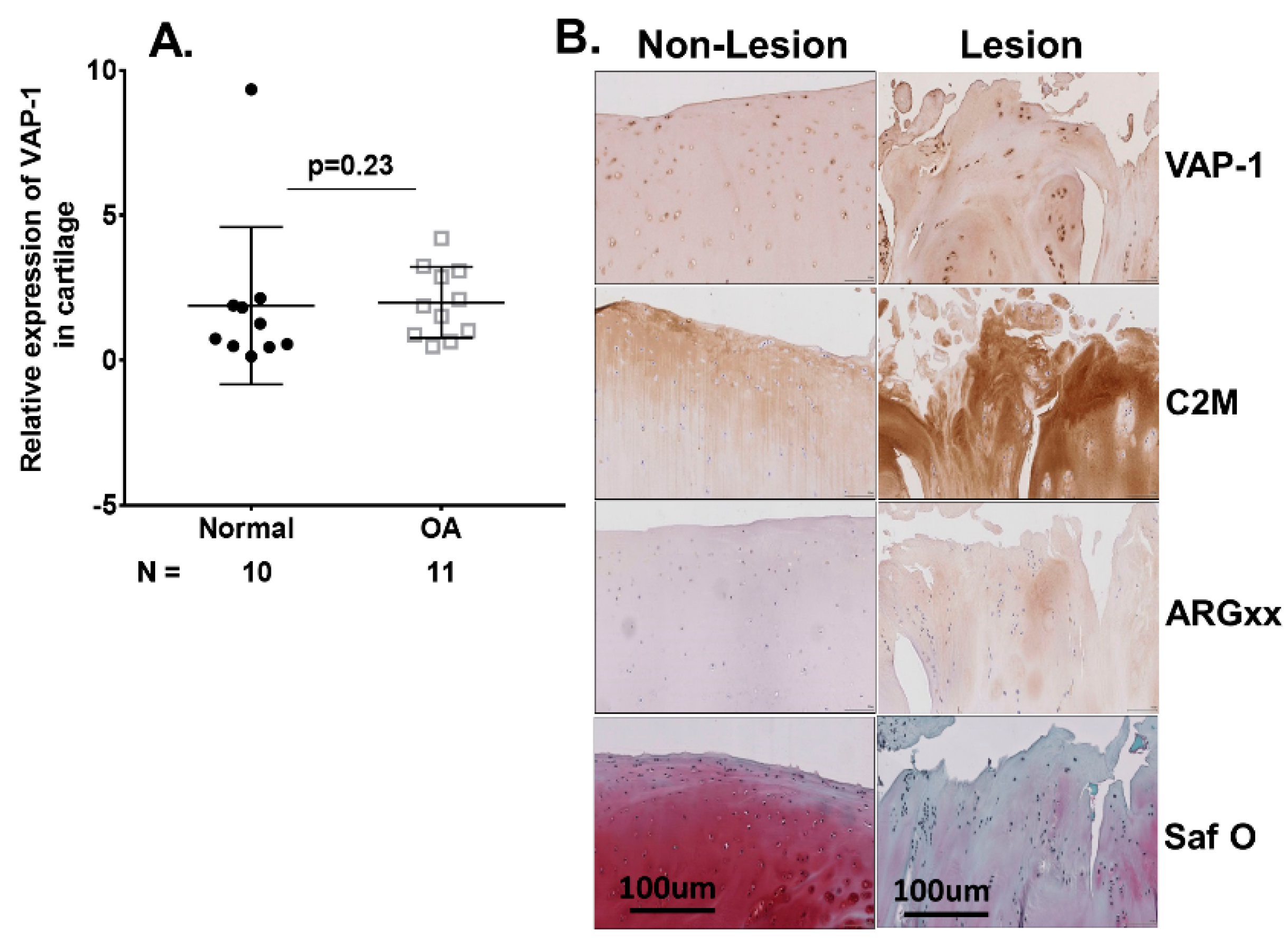
2.3. VAP-1 Locally Overexpressed in the Synovium and Not Cartilage of End-Stage Knee OA Patients
2.4. Serum sVAP-1 Levels Correlated with Pain
2.5. Correlation of Baseline Serum sVAP-1 Levels with Other Biomarkers
3. Discussion
4. Materials and Methods
4.1. Symptomatic Knee OA (SKOA), New York University (NYU) Patient Cohort
4.2. Synovial Fluid, Synovium, and Cartilage from Non-OA Subjects and OA Patients
4.3. Microarray Gene Expression Analysis
4.4. Cytokine and sVAP-1 Measurement
4.5. Real-Time Quantitative Polymerase Chain Reaction (qRT-PCR)
4.6. Histological and Immunohistochemical Analysis of Human Synovial Tissue and Cartilage
4.7. Statistical Analysis
4.8. Ethics Approval
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Vina, E.R.; Kwoh, C.K. Epidemiology of osteoarthritis: literature update. Curr. Opin. Rheumatol. 2018, 30, 160–167. [Google Scholar] [CrossRef]
- Abramson, S.B.; Attur, M.; Yazici, Y. Prospects for disease modification in osteoarthritis. Nat. Clin. Pract. Rheumatol. 2006, 2, 304–312. [Google Scholar]
- Berenbaum, F. Osteoarthritis as an inflammatory disease (osteoarthritis is not osteoarthrosis!). Osteoarthr. Cartil. 2013, 21, 16–21. [Google Scholar] [CrossRef] [Green Version]
- Wisniewski, H.G.; Colón, E.; Liublinska, V.; Karia, R.J.; Stabler, T.V.; Attur, M.; Abramson, S.B.; Band, P.A.; Kraus, V.B. TSG-6 activity as a novel biomarker of progression in knee osteoarthritis. Osteoarthr. Cartil. 2014, 22, 235–241. [Google Scholar] [CrossRef] [Green Version]
- Pelletier, J.P.; Martel-Pelletier, J.; Abramson, S.B. Osteoarthritis, an inflammatory disease: Potential implication for the selection of new therapeutic targets. Arthritis Rheumatol. 2001, 44, 1237–1247. [Google Scholar] [CrossRef]
- Sohn, D.H.; Sokolove, J.; Sharpe, O.; Erhart, J.C.; Chandra, P.E.; Lahey, L.J.; Lindstrom, T.M.; Hwang, I.; Boyer, K.A.; Andriacchi, T.P.; et al. Plasma proteins present in osteoarthritic synovial fluid can stimulate cytokine production via Toll-like receptor 4. Arthritis Res. Ther. 2012, 14, R7. [Google Scholar] [CrossRef]
- Attur, M.; Belitskaya-Lévy, I.; Oh, C.; Krasnokutsky, S.; Greenberg, J.; Samuels, J.; Smiles, S.; Lee, S.; Patel, J.; Al-Mussawir, H.; et al. Increased interleukin-1β gene expression in peripheral blood leukocytes is associated with increased pain and predicts risk for progression of symptomatic knee osteoarthritis. Arthritis Rheumatol. 2011, 63, 1908–1917. [Google Scholar] [CrossRef]
- Attur, M.; Statnikov, A.; Samuels, J.; Li, Z.; Alekseyenko, A.V.; Greenberg, J.D.; Krasnokutsky, S.; Rybak, L.; Lu, Q.A.; Todd, J.; et al. Plasma levels of interleukin-1 receptor antagonist (IL1Ra) predict radiographic progression of symptomatic knee osteoarthritis. Osteoarthr. Cartil. 2015, 23, 1915–1924. [Google Scholar] [CrossRef] [Green Version]
- Salmi, M.; Jalkanen, S. A 90-kilodalton endothelial cell molecule mediating lymphocyte binding in humans. Science 1992, 257, 1407–1409. [Google Scholar] [CrossRef]
- Smith, D.J.; Salmi, M.; Bono, P.; Hellman, J.; Leu, T.; Jalkanen, S. Cloning of vascular adhesion protein 1 reveals a novel multifunctional adhesion molecule. J. Exp. Med. 1998, 188, 17–27. [Google Scholar] [CrossRef]
- Airas, L.; Salmi, M.; Jalkanen, S. Lymphocyte-vascular adhesion protein-2 is a novel 70-kDa molecule involved in lymphocyte adhesion to vascular endothelium. J. Immunol. 1993, 151, 4228–4238. [Google Scholar] [PubMed]
- Salmi, M.; Kalimo, K.; Jalkanen, S. Induction and function of vascular adhesion protein-1 at sites of inflammation. J. Exp. Med. 1993, 178, 2255–2260. [Google Scholar] [CrossRef]
- Jaakkola, K.; Nikula, T.; Holopainen, R.; Vähäsilta, T.; Matikainen, M.T.; Laukkanen, M.L.; Huupponen, R.; Halkola, L.; Nieminen, L.; Hiltunen, J.; et al. In vivo detection of vascular adhesion protein-1 in experimental inflammation. Am. J. Pathol. 2000, 157, 463–471. [Google Scholar] [CrossRef]
- Koskinen, K.; Nevalainen, S.; Karikoski, M.; Hänninen, A.; Jalkanen, S.; Salmi, M. VAP-1-deficient mice display defects in mucosal immunity and antimicrobial responses: Implications for antiadhesive applications. J. Immunol. 2007, 179, 6160–6168. [Google Scholar] [CrossRef] [PubMed]
- Salmi, M.; Jalkanen, S. Ectoenzymes in leukocyte migration and their therapeutic potential. Semin. Immunopathol. 2014, 36, 163–176. [Google Scholar] [CrossRef] [PubMed]
- Marttila-Ichihara, F.; Smith, D.J.; Stolen, C.; Yegutkin, G.G.; Elima, K.; Mercier, N.; Kiviranta, R.; Pihlavisto, M.; Alaranta, S.; Pentikäinen, U.; et al. Vascular amine oxidases are needed for leukocyte extravasation into inflamed joints in vivo. Arthritis Rheumatol. 2006, 54, 2852–2862. [Google Scholar] [CrossRef]
- Horváth, Á.; Tékus, V.; Bencze, N.; Szentes, N.; Scheich, B.; Bölcskei, K.; Szőke, É.; Mócsai, A.; Tóth-Sarudy, É.; Mátyus, P.; et al. Analgesic effects of the novel semicarbazide-sensitive amine oxidase inhibitor SZV 1287 in mouse pain models with neuropathic mechanisms: Involvement of transient receptor potential vanilloid 1 and ankyrin 1 receptors. Pharmacol. Res. 2018, 131, 231–243. [Google Scholar] [CrossRef]
- Akin, E.; Aversa, J.; Steere, A.C. Expression of adhesion molecules in synovia of patients with treatment-resistant lyme arthritis. Infect. Immun. 2001, 69, 1774–1780. [Google Scholar] [CrossRef]
- Filip, A.; Pinzano, A.; Bianchi, A.; Fève, B.; Jalkanen, S.; Gillet, P.; Mainard, D.; Lacolley, P.; Magdalou, J.; Mercier, N. Expression of the semicarbazide-sensitive amine oxidase in articular cartilage: Its role in terminal differentiation of chondrocytes in rat and human. Osteoarthr. Cartil. 2016, 24, 1223–1234. [Google Scholar] [CrossRef]
- Ling, S.M.; Patel, D.D.; Garnero, P.; Zhan, M.; Vaduganathan, M.; Muller, D.; Taub, D.; Bathon, J.M.; Hochberg, M.; Abernethy, D.R.; et al. Serum protein signatures detect early radiographic osteoarthritis. Osteoarthr. Cartil. 2009, 17, 43–48. [Google Scholar] [CrossRef] [Green Version]
- Bellamy, N.; Buchanan, W.W.; Goldsmith, C.H.; Campbell, J.; Stitt, L.W. Validation study of WOMAC: A health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J. Rheumatol. 1988, 15, 1833–1840. [Google Scholar]
- Srikanth, V.K.; Fryer, J.L.; Zhai, G.; Winzenberg, T.M.; Hosmer, D.; Jones, G. A meta-analysis of sex differences prevalence, incidence and severity of osteoarthritis. Osteoarthr. Cartil. 2005, 13, 769–781. [Google Scholar] [CrossRef] [Green Version]
- Shane Anderson, A.; Loeser, R.F. Why is osteoarthritis an age-related disease? Best Pract Res. Clin. Rheumatol. 2010, 24, 15–26. [Google Scholar] [CrossRef] [Green Version]
- Bedson, J.; Croft, P.R. The discordance between clinical and radiographic knee osteoarthritis: a systematic search and summary of the literature. BMC Musculoskelet. Disord. 2008, 9, 116. [Google Scholar] [CrossRef]
- Hannan, M.T.; Felson, D.T.; Pincus, T. Analysis of the discordance between radiographic changes and knee pain in osteoarthritis of the knee. J. Rheumatol. 2000, 27, 1513–1517. [Google Scholar]
- Deveza, L.A.; Loeser, R.F. Is osteoarthritis one disease or a collection of many? Rheumatology 2018, 57 (Suppl. 4), iv34–iv42. [Google Scholar] [CrossRef]
- Liu-Bryan, R.; Terkeltaub, R. Emerging regulators of the inflammatory process in osteoarthritis. Nat. Rev. Rheumatol. 2015, 11, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Robinson, W.H.; Lepus, C.M.; Wang, Q.; Raghu, H.; Mao, R.; Lindstrom, T.M.; Sokolove, J. Low-grade inflammation as a key mediator of the pathogenesis of osteoarthritis. Nat. Rev. Rheumatol. 2016, 12, 580–592. [Google Scholar] [CrossRef]
- Attur, M.; Krasnokutsky-Samuels, S.; Samuels, J.; Abramson, S.B. Prognostic biomarkers in osteoarthritis. Curr. Opin. Rheumatol. 2013, 25, 136–144. [Google Scholar] [CrossRef] [Green Version]
- Attur, M.; Krasnokutsky, S.; Statnikov, A.; Samuels, J.; Li, Z.; Friese, O.; Hellio Le Graverand-Gastineau, M.P.; Rybak, L.; Kraus, V.B.; Jordan, J.M.; et al. Low-grade inflammation in symptomatic knee osteoarthritis: Prognostic value of inflammatory plasma lipids and peripheral blood leukocyte biomarkers. Arthritis Rheumatol. 2015, 67, 2905–2915. [Google Scholar] [CrossRef] [PubMed]
- Kuo, C.H.; Wei, J.N.; Yang, C.Y.; Ou, H.Y.; Wu, H.T.; Fan, K.C.; Wang, S.H.; Hua, C.H.; Hsiao, C.H.; Lee, M.K.; et al. Serum vascular adhesion protein-1 is up-regulated in hyperglycemia and is associated with incident diabetes negatively. Int. J. Obes. 2019, 43, 512–522. [Google Scholar] [CrossRef] [PubMed]
- Attur, M.; Yang, Q.; Shimada, K.; Tachida, Y.; Nagase, H.; Mignatti, P.; Statman, L.; Palmer, G.; Kirsch, T.; Beier, F.; et al. Elevated expression of periostin in human osteoarthritic cartilage and its potential role in matrix degradation via matrix metalloproteinase-13. FASEB J. 2015, 29, 4107–4121. [Google Scholar] [CrossRef]
- Mix, K.S.; McMahon, K.; McMorrow, J.P.; Walkenhorst, D.E.; Smyth, A.M.; Petrella, B.L.; Gogarty, M.; Fearon, U.; Veale, D.; Attur, M.G.; et al. Orphan nuclear receptor NR4A2 induces synoviocyte proliferation, invasion, and matrix metalloproteinase 13 transcription. Arthritis Rheumatol. 2012, 64, 2126–2136. [Google Scholar] [CrossRef] [PubMed]
- Livak, K.J.; Schmittgen, T.D. Analysis of relative gene expression data using real-time quantitative PCR and the 2−∆∆Ct Method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Normal (N = 24) | SKOA (N = 372) | p Values | Adjusted for AGB p Values |
|---|---|---|---|---|
| Age (years) | 54.63 (9.37), [40.00–75.00] | 61.21 (10.51), [37.00–88.00] | 0.003 | |
| Gender (%) | ||||
| Male | 50% | 36.93% | ||
| Female | 50% | 63.07% | ||
| BMI (kg/m2) | 26.30 (3.92), [20.00–32.40] | 26.35 (3.50), [15.40–32.60] | 0.943 | 0.943 |
| VAS (0–100) | 0 | 46.97 (26.47), [0.00–100.00] | NA | NA |
| WOMAC (0–100) | 0 | 30.97 (24.73), [0.00–98.60] | NA | NA |
| JSW (mm) | NA | 3.39 (1.34), [0.00–7.30] | NA | NA |
| KL Grades | ||||
| KL0 | 63.64% | 5.41% | ||
| KL1 | 36.36% | 15.68% | ||
| KL2 | 0.00% | 32.70% | ||
| KL3 | 0.00% | 31.35% | ||
| KL4 | 0.00% | 14.86% | ||
| IL-1Ra (pg/mL) | 354.53 (172.28), [91.40–726.43] | 350.04 (156.37), [97.97–999.98] | 0.901 | 0.943 |
| MMP-1 (pg/mL) | 2388.24 (1140.35), [1137.52–4679.16] | 3151.94 (2383.33), [401.28–17,537.19] | 0.146 | 0.351 |
| MMP-3 (pg/mL) | 16,525.13 (8777.40), [6684.15–33,139.95] | 17,517.27 (16,424.86), [3768.51–244,674.57] | 0.784 | 0.943 |
| MMP-9 (ng/mL) | 49,197.66 (56,813.60), [9256.92–257,706.04] | 38,409.48 (29,838.25), [9426.51–197,065.54] | 0.135 | 0.351 |
| IL-15 (pg/mL) | 1.18 (0.30), [0.70–1.90] | 1.15 (0.32), [0.6–3.29] | 0.714 | 0.943 |
| hsCRP (mg/L) | 4.06 (4.85), [0.14–19.85] | 2.73 (3.68), [0.00–37.00] | 0.117 | 0.351 |
| CD163 (ng/mL) | 679.84 (317.42), [291.74–1852.40] | 656.09 (236.68), [164.69–1501.75] | 0.692 | 0.943 |
| HA (ng/mL) | 29.59 (18.07), [1.91–72.72] | 30.20 (29.75), [0.76–193.22] | 0.929 | 0.943 |
| sRAGE (ng/mL) | 1303.70 (542.76), [435.92–2463.60] | 1106.13 (571.74), [239.11–4657.23] | 0.182 | 0.363 |
| sVAP-1 (ng/mL) | 569.90 (178.01), [276.32–1105.39] | 430.00 (115.50), [136.16–851.32] | <0.002 | <0.0001 |
| Variable | Normal (N = 14) | SKOA (N = 301) ≥51 Years | p Values | Adjusted for AGB p Values |
|---|---|---|---|---|
| Age (years) | 60.79 (6.94), [51.00–75.00] | 64.69 (8.34), [51.00–88.00] | 0.086 | 0.305 |
| Gender (%) | ||||
| Male | 64.29% | 35.55% | ||
| Female | 35.71% | 64.45% | ||
| BMI (kg/m2) | 26.62 (4.08), [20.00–31.90] | 26.35 (3.52), [15.40–32.60] | 0.779 | 0.934 |
| VAS (0–100) | 0 | 46.12 (25.83), [0.00–100.00] | NA | NA |
| WOMAC (0–100) | 0 | 30.66 (23.25), [0.00–91.60] | NA | NA |
| JSW (mm) | NA | 3.28 (1.37), [0.00–7.30] | NA | NA |
| KL Grades | ||||
| KL0 | 46.2% | 4.3% | ||
| KL1 | 53.8% | 12.6% | ||
| KL2 | 0.0% | 30.6% | ||
| Kl3 | 0.0% | 34.6% | ||
| KL4 | 0.0% | 17.9% | ||
| IL-1Ra (pg/mL) | 362.21 (163.82), [91.40–702.70] | 363.47 (154.69), [97.97–999.98] | 0.977 | 0.977 |
| MMP-1 (pg/mL) | 2511.82 (1290.26), [1137.52–4679.16] | 3230.39 (2430.58), [401.28–17,537.19] | 0.274 | 0.657 |
| MMP-3 (pg/mL) | 15,704.52 (7796.96), [6684.15–33,139.95] | 17,546.72 (17,564.45), [4685.58–244,674.57] | 0.697 | 0.934 |
| MMP-9 (ng/mL) | 41,278.95 (36,076.83), [9256.92–150,916.05] | 38,662.00 (28,912.33), [9426.51–184,835.39] | 0.745 | 0.934 |
| IL-15 (pg/mL) | 1.28 (0.28), [0.70–1.90] | 1.14 (0.30), [0.63–3.29] | 0.102 | 0.305 |
| hsCRP (mg/L) | 4.80 (5.59), [0.14–19.85] | 2.91 (3.96), [0.00–37.00] | 0.090 | 0.305 |
| CD163 (ng/mL) | 749.40 (348.24), [483.96–1852.40] | 687.27 (235.73), [223.48–1501.75] | 0.396 | 0.680 |
| HA (ng/mL) | 34.51 (17.67), [13.25–72.72] | 33.78 (31.59), [0.76–193.22] | 0.933 | 0.977 |
| sRAGE (pg/mL) | 1342.65 (492.87), [802.28–1927.11] | 1142.09 (615.22), [293.75–4657.23] | 0.396 | 0.680 |
| sVAP-1 (ng/mL) | 577.93 (192.95), [332.83–1105.39] | 437.86 (111.13), [161.94–851.32] | <0.0001 | <0.0001 |
| Variable | Normal (N = 20) | OA (N = 45) | p Values | Adjusted for AGB p Values |
|---|---|---|---|---|
| Age (years) | 75.00 (10.72), [51.00–90.00] | 62.15 (11.47), [43.00–87.00] | <0.00001 | |
| Gender (%) | ||||
| Male | 66.67% | 45.83% | ||
| Female | 33.33% | 54.17% | ||
| BMI | NA | 28.74 (5.08), [20.00–44.09] | NA | NA |
| KL Grades | ||||
| KL1 | NA | 17% | ||
| KL2 | NA | 26% | ||
| KL3 | NA | 33% | ||
| KL4 | NA | 20% | ||
| KL not known | 4% | |||
| IL-8 (pg/mL) | 22.38 (39.90), [3.21–134.79] | 24.68 (42.13), [1.04–249.18] | 0.839 | 0.979 |
| HSIL-6 (pg/mL) | 122.62 (193.02), [0.3–496.45] | 122.22 (140.02), [5.26–630.25] | 0.993 | 0.993 |
| CCL2 (pg/mL) | 682.53 (631.01), [0.10–2125.20] | 357.34 (179.17), [36.73–953.08] | 0.002 | 0.004 |
| CCL4 (pg/mL) | 1.12 (4.43), [0.10–19.39] | 25.49 (38.31), [0.10–154.01] | 0.008 | 0.013 |
| HSIL-10 (pg/mL) | 1.41 (2.84), [0.14–12.17] | 1.03 (2.40), [0.05–16.27] | 0.597 | 0.835 |
| sRAGE (pg/mL) | 146.8 (89.63), [13.38–327.40] | 232.22 (163.7), [10.8–970.00] | 0.041 | 0.046 |
| SF-sVAP-1 (ng/mL) | 38.12 (22.98), [6.20–88.35] | 107.94 (41.42), [7.38–05.47] | <0.0001 | <0.0001 |
| sVAP-1 (ng/mL)—serum | Not available | 482.5 (132.5), [180.6–695.6] |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bournazou, E.; Samuels, J.; Zhou, H.; Krasnokutsky, S.; Patel, J.; Han, T.; Bencardino, J.; Rybak, L.; Abramson, S.B.; Junker, U.; et al. Vascular Adhesion Protein-1 (VAP-1) as Predictor of Radiographic Severity in Symptomatic Knee Osteoarthritis in the New York University Cohort. Int. J. Mol. Sci. 2019, 20, 2642. https://doi.org/10.3390/ijms20112642
Bournazou E, Samuels J, Zhou H, Krasnokutsky S, Patel J, Han T, Bencardino J, Rybak L, Abramson SB, Junker U, et al. Vascular Adhesion Protein-1 (VAP-1) as Predictor of Radiographic Severity in Symptomatic Knee Osteoarthritis in the New York University Cohort. International Journal of Molecular Sciences. 2019; 20(11):2642. https://doi.org/10.3390/ijms20112642
Chicago/Turabian StyleBournazou, Eirini, Jonathan Samuels, Hua Zhou, Svetlana Krasnokutsky, Jyoti Patel, Tianzhen Han, Jenny Bencardino, Leon Rybak, Steven B. Abramson, Uwe Junker, and et al. 2019. "Vascular Adhesion Protein-1 (VAP-1) as Predictor of Radiographic Severity in Symptomatic Knee Osteoarthritis in the New York University Cohort" International Journal of Molecular Sciences 20, no. 11: 2642. https://doi.org/10.3390/ijms20112642