Serum Levels of Interleukin-6 and Titers of Antibodies against Porphyromonas gingivalis Could Be Potential Biomarkers for the Diagnosis of Oral Squamous Cell Carcinoma


 and
and
Abstract
:1. Introduction
2. Results
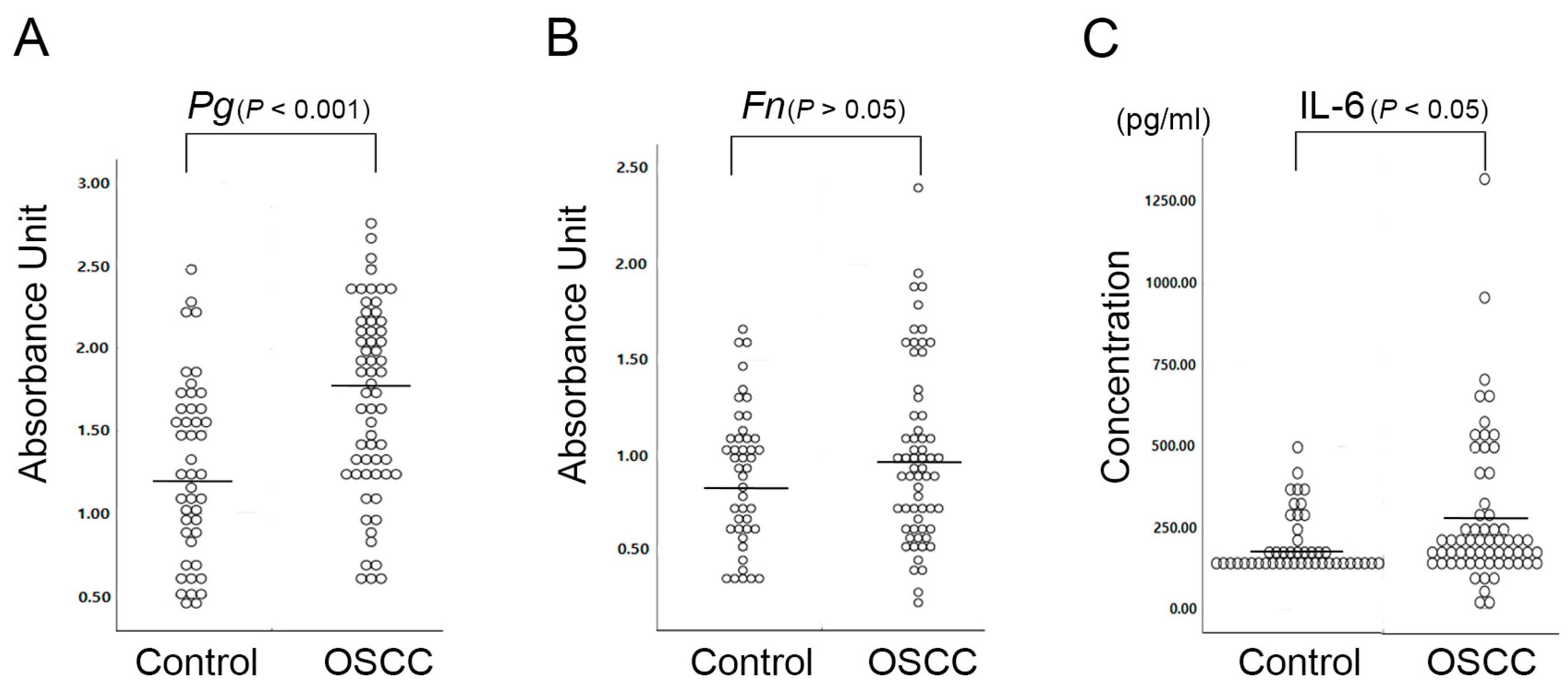
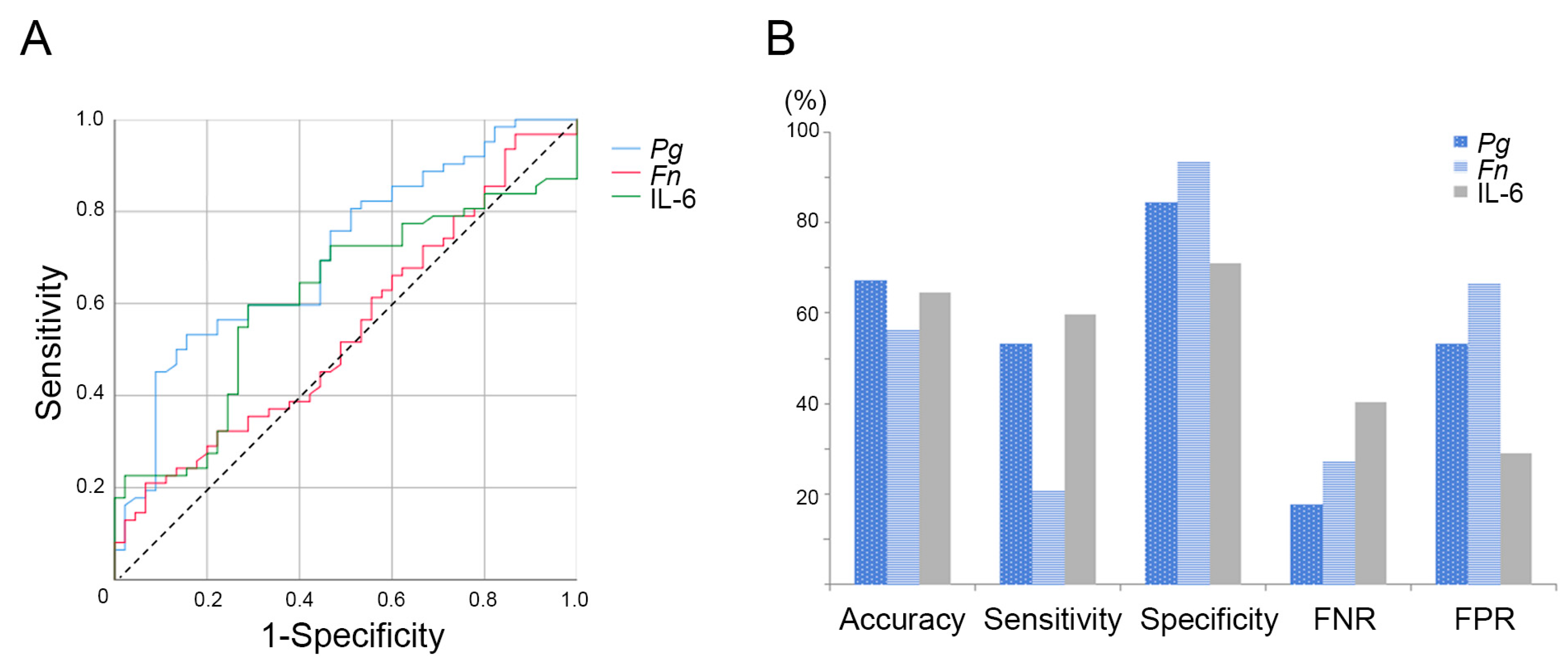
2.1. P. gingivalis Is More Closely Associated with OSCC than F. nucleatum
2.2. Serum Interleukin-6 Is Associated with the 5-Year Survival Rate in OSCC Patients
3. Discussion
4. Materials and Methods
4.1. Study Subjects
4.2. Enzyme-Linked Immunosorbent Assay
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| OSCC | Oral Squamous Cell Carcinoma |
| ESCC | Esophageal Squamous Cell Carcinoma |
| IL-6 | Interleukin-6 |
| ROC | Receiver Operating Characteristic |
| AUC | Area Under the ROC Curve |
References
- Devine, J.C.; Rogers, S.N.; McNally, D.; Brown, J.S.; Vaughan, E.D. A comparison of aesthetic, functional and patient subjective outcomes following lip-split mandibulotomy and mandibular lingual releasing access procedures. Int. J. Oral Maxillofac. Surg. 2001, 30, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Wei, F.C.; Yazar, S.; Lin, C.H.; Cheng, M.H.; Tsao, C.K.; Chiang, Y.C. Double free flaps in head and neck reconstruction. Clin. Plast. Surg. 2005, 32, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Arruebo, M.; Vilaboa, N.; Saez-Gutierrez, B.; Lambea, J.; Tres, A.; Valladares, M.; Gonzalez-Fernandez, A. Assessment of the evolution of cancer treatment therapies. Cancers (Basel) 2011, 3, 3279–3330. [Google Scholar] [CrossRef] [PubMed]
- Goldman, J.M.; Melo, J.V. Chronic myeloid leukemia--advances in biology and new approaches to treatment. N. Engl. J. Med. 2003, 349, 1451–1464. [Google Scholar] [CrossRef] [PubMed]
- Kolokythas, A. Long-Term Surgical Complications in the Oral Cancer Patient: A Comprehensive Review. Part II. J. Oral Maxillofac Res. 2010, 1, e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolokythas, A. Long-term surgical complications in the oral cancer patient: A comprehensive review. Part I. J. Oral Maxillofac Res. 2010, 1, e1. [Google Scholar] [CrossRef]
- Nathan, M.R.; Schmid, P. The emerging world of breast cancer immunotherapy. Breast 2018, 37, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Silva, T.D.; Ferreira, C.B.; Leite, G.B.; de Menezes Pontes, J.R.; Antunes, H.S. Oral manifestations of lymphoma: A systematic review. Ecancermedicalscience 2016, 10, 665. [Google Scholar] [CrossRef] [PubMed]
- Skoetz, N.; Trelle, S.; Rancea, M.; Haverkamp, H.; Diehl, V.; Engert, A.; Borchmann, P. Effect of initial treatment strategy on survival of patients with advanced-stage Hodgkin’s lymphoma: A systematic review and network meta-analysis. Lancet Oncol. 2013, 14, 943–952. [Google Scholar] [CrossRef]
- Bulsara, V.M.; Worthington, H.V.; Glenny, A.M.; Clarkson, J.E.; Conway, D.I.; Macluskey, M. Interventions for the treatment of oral and oropharyngeal cancers: Surgical treatment. Cochrane Database Syst. Rev. 2018, 12, CD006205. [Google Scholar] [CrossRef]
- Rivera, C.; Venegas, B. Histological and molecular aspects of oral squamous cell carcinoma (Review). Oncol. Lett. 2014, 8, 7–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Axley, P.; Ahmed, Z.; Ravi, S.; Singal, A.K. Hepatitis C Virus and Hepatocellular Carcinoma: A Narrative Review. J. Clin Transl Hepatol 2018, 6, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Jess, T.; Rungoe, C.; Peyrin-Biroulet, L. Risk of colorectal cancer in patients with ulcerative colitis: A meta-analysis of population-based cohort studies. Clin. Gastroenterol. Hepatol. 2012, 10, 639–645. [Google Scholar] [CrossRef] [PubMed]
- Van Der Kraak, L.; Gros, P.; Beauchemin, N. Colitis-associated colon cancer: Is it in your genes? World J. Gastroenterol. 2015, 21, 11688–11699. [Google Scholar] [CrossRef] [PubMed]
- Snider, A.J.; Bialkowska, A.B.; Ghaleb, A.M.; Yang, V.W.; Obeid, L.M.; Hannun, Y.A. Murine Model for Colitis-Associated Cancer of the Colon. Methods Mol. Biol. 2016, 1438, 245–254. [Google Scholar] [PubMed] [Green Version]
- Huang, P.; Liu, M.; Zang, F.; Yao, Y.; Yue, M.; Wang, J.; Fan, H.; Zhuo, L.; Wu, J.; Xia, X.; et al. The development of hepatocellular carcinoma in HCV-infected patients treated with DAA: A comprehensive analysis. Carcinogenesis 2018, 39, 1497–1505. [Google Scholar] [CrossRef]
- Yamashita, T.; Honda, M.; Kaneko, S. Molecular mechanisms of hepatocarcinogenesis in chronic hepatitis C virus infection. J. Gastroenterol. Hepatol. 2011, 26, 960–964. [Google Scholar] [CrossRef] [Green Version]
- Heikkila, P.; But, A.; Sorsa, T.; Haukka, J. Periodontitis and cancer mortality: Register-based cohort study of 68,273 adults in 10-year follow-up. Int. J. Cancer 2018, 142, 2244–2253. [Google Scholar] [CrossRef] [Green Version]
- Sfreddo, C.S.; Maier, J.; De David, S.C.; Susin, C.; Moreira, C.H.C. Periodontitis and breast cancer: A case-control study. Community Dent. Oral Epidemiol. 2017, 45, 545–551. [Google Scholar] [CrossRef]
- Chung, S.D.; Tsai, M.C.; Huang, C.C.; Kao, L.T.; Chen, C.H. A population-based study on the associations between chronic periodontitis and the risk of cancer. Int. J. Clin. Oncol. 2016, 21, 219–223. [Google Scholar] [CrossRef]
- Tezal, M.; Sullivan, M.A.; Hyland, A.; Marshall, J.R.; Stoler, D.; Reid, M.E.; Loree, T.R.; Rigual, N.R.; Merzianu, M.; Hauck, L.; et al. Chronic periodontitis and the incidence of head and neck squamous cell carcinoma. Cancer Epidemiol. Biomarkers Prev. 2009, 18, 2406–2412. [Google Scholar] [CrossRef] [PubMed]
- Ha, N.H.; Woo, B.H.; Kim, D.J.; Ha, E.S.; Choi, J.I.; Kim, S.J.; Park, B.S.; Lee, J.H.; Park, H.R. Prolonged and repetitive exposure to Porphyromonas gingivalis increases aggressiveness of oral cancer cells by promoting acquisition of cancer stem cell properties. Tumour Biol. 2015, 36, 9947–9960. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Roberts, J.S.; Atanasova, K.R.; Chowdhury, N.; Han, K.; Yilmaz, O. Human Primary Epithelial Cells Acquire an Epithelial-Mesenchymal-Transition Phenotype during Long-Term Infection by the Oral Opportunistic Pathogen, Porphyromonas gingivalis. Front. Cell Infect. Microbiol. 2017, 7, 493. [Google Scholar] [CrossRef]
- Kim, H.J.; Cha, G.S.; Kim, H.J.; Kwon, E.Y.; Lee, J.Y.; Choi, J.; Joo, J.Y. Porphyromonas gingivalis accelerates atherosclerosis through oxidation of high-density lipoprotein. J. Periodontal Implan. 2018, 48, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Liang, S.; Ren, H.; Guo, H.; Xing, W.; Liu, C.; Ji, Y.; Jiang, H.; Zhang, P.; Du, M. Periodontal infection with Porphyromonas gingivalis induces preterm birth and lower birth weight in rats. Mol. Oral Microbiol. 2018, 33, 312–321. [Google Scholar] [CrossRef]
- Geng, F.X.; Liu, J.C.; Guo, Y.; Li, C.; Wang, H.Y.; Wang, H.Y.; Zhao, H.J.; Pan, Y.P. Persistent Exposure to Porphyromonas gingivalis Promotes Proliferative and Invasion Capabilities, and Tumorigenic Properties of Human Immortalized Oral Epithelial Cells. Front. Cell Infect. Microbiol. 2017, 7. [Google Scholar] [CrossRef]
- Woo, B.H.; Kim, D.J.; Choi, J.I.; Kim, S.J.; Park, B.S.; Song, J.M.; Lee, J.H.; Park, H.R. Oral cancer cells sustainedly infected with Porphyromonas gingivalis exhibit resistance to Taxol and have higher metastatic potential. Oncotarget 2017, 8, 46981–46992. [Google Scholar] [CrossRef]
- Bradshaw, D.J.; Marsh, P.D.; Watson, G.K.; Allison, C. Role of Fusobacterium nucleatum and coaggregation in anaerobe survival in planktonic and biofilm oral microbial communities during aeration. Infect. Immun. 1998, 66, 4729–4732. [Google Scholar]
- Schiegnitz, E.; Kammerer, P.W.; Schon, H.; Blatt, S.; Berres, M.; Sagheb, K.; Al-Nawas, B. Proinflammatory cytokines as serum biomarker in oral carcinoma-A prospective multi-biomarker approach. J. Oral Pathol. Med. 2018, 47, 268–274. [Google Scholar] [CrossRef]
- Zanotti, L.; Paderno, A.; Piazza, C.; Pagan, E.; Bignotti, E.; Romani, C.; Bandiera, E.; Calza, S.; Del Bon, F.; Nicolai, P.; et al. Epidermal growth factor receptor detection in serum and saliva as a diagnostic and prognostic tool in oral cancer. Laryngoscope 2017, 127, E408–E414. [Google Scholar] [CrossRef]
- Rajkumar, K.; Ramya, R.; Nandhini, G.; Rajashree, P.; Ramesh Kumar, A.; Nirmala Anandan, S. Salivary and serum level of CYFRA 21-1 in oral precancer and oral squamous cell carcinoma. Oral Dis. 2015, 21, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Ha, N.H.; Park, D.G.; Woo, B.H.; Kim, D.J.; Choi, J.I.; Park, B.S.; Kim, Y.D.; Lee, J.H.; Park, H.R. Porphyromonas gingivalis increases the invasiveness of oral cancer cells by upregulating IL-8 and MMPs. Cytokine 2016, 86, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Inaba, H.; Sugita, H.; Kuboniwa, M.; Iwai, S.; Hamada, M.; Noda, T.; Morisaki, I.; Lamont, R.J.; Amano, A. Porphyromonas gingivalis promotes invasion of oral squamous cell carcinoma through induction of proMMP9 and its activation. Cell Microbiol. 2014, 16, 131–145. [Google Scholar] [CrossRef] [PubMed]
- Michaud, D.S.; Izard, J.; Wilhelm-Benartzi, C.S.; You, D.H.; Grote, V.A.; Tjonneland, A.; Dahm, C.C.; Overvad, K.; Jenab, M.; Fedirko, V.; et al. Plasma antibodies to oral bacteria and risk of pancreatic cancer in a large European prospective cohort study. Gut 2013, 62, 1764–1770. [Google Scholar] [CrossRef] [PubMed]
- Gao, S.G.; Yang, J.Q.; Ma, Z.K.; Yuan, X.; Zhao, C.; Wang, G.C.; Wei, H.; Feng, X.S.; Qi, Y.J. Preoperative serum immunoglobulin G and A antibodies to Porphyromonas gingivalis are potential serum biomarkers for the diagnosis and prognosis of esophageal squamous cell carcinoma. BMC Cancer 2018, 18, 17. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.; Segers, S.; Hayes, R.B. Periodontal disease, Porphyromonas gingivalis serum antibody levels and orodigestive cancer mortality. Carcinogenesis 2012, 33, 1055–1058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taniguchi, K.; Karin, M. IL-6 and related cytokines as the critical lynchpins between inflammation and cancer. Semin. Immunol. 2014, 26, 54–74. [Google Scholar] [CrossRef]
- Brailo, V.; Vucicevic-Boras, V.; Lukac, J.; Biocina-Lukenda, D.; Zilic-Alajbeg, I.; Milenovic, A.; Balija, M. Salivary and serum interleukin 1 beta, interleukin 6 and tumor necrosis factor alpha in patients with leukoplakia and oral cancer. Med. Oral Patol. Oral Cir. Bucal. 2012, 17, e10. [Google Scholar] [CrossRef]
- Vinocha, A.; Grover, R.K.; Deepak, R. Clinical significance of interleukin-6 in diagnosis of lung, oral, esophageal, and gall bladder carcinomas. J. Cancer Res. Ther. 2018, 14, S758–S760. [Google Scholar] [CrossRef]
- Mantovani, A.; Allavena, P.; Sica, A.; Balkwill, F. Cancer-related inflammation. Nature 2008, 454, 436–444. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | lgG Titer (Mean ± SD) | p | |
|---|---|---|---|
| Age | ≤60 (24 (38.7%)) | 1.61 ± 0.51 | 0.34 |
| >60 (38 (61.3%)) | 1.74 ± 0.60 | ||
| Gender | males (45 (72.6%)) | 1.70 ± 0.54 | 0.77 |
| Females (17 (27.4%)) | 1.65 ± 0.64 | ||
| Tobacco Use | No (39 (65.0%)) | 1.67 ± 0.58 | 0.74 |
| Yes (21 (35.0%)) | 1.73 ± 0.59 | ||
| Alcohol Use | No (37 (59.7%)) | 1.70 ± 0.61 | 0.70 |
| Yes (25 (40.3%)) | 1.68 ± 0.52 | ||
| Histopathologic Grade | I (21 (35.6%)) | 1.78 ± 0.44 | 0.16 |
| II (26 (44.1%)) | 1.53 ± 0.59 | ||
| III (6 (10.2%)) | 1.55 ± 0.73 | ||
| IV (6 (10.2%)) | 2.03 ± 0.39 | ||
| Lymph Node Metastasis | No (33 (59.7%)) | 1.63 ± 0.63 | 0.38 |
| Yes (29 (40.3%)) | 1.76 ± 0.49 | ||
| Tumor Size | T1 (25 (42.4%)) | 1.62 ± 0.58 | 0.74 |
| T2 (16 (27.1%)) | 1.61 ± 0.44 | ||
| T3 (5 (8.5%)) | 1.89 ± 0.67 | ||
| T4 (13 (22.0)) | 1.74 ± 0.68 | ||
| TNM Stage | I (19 (30.6%)) | 1.59 ± 0.63 | 0.53 |
| II (9 (14.5%)) | 1.54 ± 0.52 | ||
| III (11 (17.2%)) | 1.74 ± 0.45 | ||
| IV (23 (37.1%)) | 1.81 ± 0.59 | ||
| Variables | lgG Titer (Mean ± SD) | p | |
|---|---|---|---|
| Age | ≤60 (24 (38.7%)) | 1.00 ± 0.52 | 0.78 |
| >60 (38 (61.3%)) | 0.99 ± 0.43 | ||
| Gender | males (45 (72.6%)) | 1.00 ± 0.42 | 0.45 |
| Females (17 (27.4%)) | 0.99 ± 0.58 | ||
| Tobacco Use | No (39 (65.0%)) | 1.03 ± 0.49 | 0.76 |
| Yes (21 (35.0%)) | 0.96 ± 0.44 | ||
| Alcohol Use | No (37 (59.7%)) | 0.96 ± 0.45 | 0.33 |
| Yes (25 (40.3%)) | 1.05 ± 0.49 | ||
| Histopathologic Grade | I (21 (35.6%)) | 1.04 ± 0.50 | 0.64 |
| II (26 (44.1%)) | 0.91 ± 0.43 | ||
| III (6 (10.2%)) | 1.05 ± 0.52 | ||
| IV (6 (10.2%)) | 1.11 ± 0.45 | ||
| Lymph Node Metastasis | No (33 (59.7%)) | 1.02 ± 0.49 | 0.99 |
| Yes (29 (40.3%)) | 0.98 ± 0.45 | ||
| Tumor Size | T1 (25 (42.4%)) | 1.04 ± 0.50 | 0.69 |
| T2 (16 (27.1%)) | 0.92 ± 0.48 | ||
| T3 (5 (8.5%)) | 0.98 ± 0.58 | ||
| T4 (13 (22.0)) | 1.06 ± 0.42 | ||
| TNM Stage | I (19 (30.6%)) | 1.08 ± 0.54 | 0.12 |
| II (9 (14.5%)) | 0.87 ± 0.46 | ||
| III (11 (17.2%)) | 0.77 ± 0.35 | ||
| IV (23 (37.1%)) | 1.09 ± 0.43 | ||
| Variables | IL-6 (pg/mL) (Mean ± SD) | p | |
|---|---|---|---|
| Age | ≤60 (24 (38.7%)) | 303.9 ± 230.9 | 0.30 |
| >60 (38 (61.3%)) | 256.6 ± 228.2 | ||
| Gender | males (45 (72.6%)) | 260.2 ± 170.3 | 0.94 |
| Females (17 (27.4%)) | 314.0 ± 342.3 | ||
| Tobacco Use | No (39 (65.0%)) | 297.4 ± 262.5 | 0.38 |
| Yes (21 (35.0%)) | 229.7 ± 147.2 | ||
| Alcohol Use | No (37 (59.7%)) | 304.9 ± 265.3 | 0.23 |
| Yes (25 (40.3%)) | 230.6 ± 154.1 | ||
| Histopathologic Grade | I (21 (35.6%)) | 277.5 ± 288.3 | 0.59 |
| II (26 (44.1%)) | 266.4 ± 200.5 | ||
| III (6 (10.2%)) | 315.5 ± 189.8 | ||
| IV (6 (10.2%)) | 317.3 ± 236.4 | ||
| Lymph Node Metastasis | No (33 (59.7%)) | 291.1 ± 273.7 | 0.92 |
| Yes (29 (40.3%)) | 256.5 ± 165.9 | ||
| Tumor Size | T1 (25 (42.4%)) | 237.9 ± 144.4 | 0.85 |
| T2 (16 (27.1%)) | 338.3 ± 330.2 | ||
| T3 (5 (8.5%)) | 226.0 ± 145.1 | ||
| T4 (13 (22.0)) | 293.1 ± 258.5 | ||
| TNM Stage | I (19 (30.6%)) | 232.9 ± 150.7 | 0.82 |
| II (9 (14.5%)) | 396.8 ± 404.9 | ||
| III (11 (17.2%)) | 239.1 ± 180.5 | ||
| IV (23 (37.1%)) | 279.1 ± 208.8 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, D.-G.; Woo, B.H.; Lee, B.-J.; Yoon, S.; Cho, Y.; Kim, Y.-D.; Park, H.R.; Song, J.M. Serum Levels of Interleukin-6 and Titers of Antibodies against Porphyromonas gingivalis Could Be Potential Biomarkers for the Diagnosis of Oral Squamous Cell Carcinoma. Int. J. Mol. Sci. 2019, 20, 2749. https://doi.org/10.3390/ijms20112749
Park D-G, Woo BH, Lee B-J, Yoon S, Cho Y, Kim Y-D, Park HR, Song JM. Serum Levels of Interleukin-6 and Titers of Antibodies against Porphyromonas gingivalis Could Be Potential Biomarkers for the Diagnosis of Oral Squamous Cell Carcinoma. International Journal of Molecular Sciences. 2019; 20(11):2749. https://doi.org/10.3390/ijms20112749
Chicago/Turabian StylePark, Dae-Gun, Bok Hee Woo, Byung-Joo Lee, Sanggyeong Yoon, Youngseuk Cho, Yong-Deok Kim, Hae Ryoun Park, and Jae Min Song. 2019. "Serum Levels of Interleukin-6 and Titers of Antibodies against Porphyromonas gingivalis Could Be Potential Biomarkers for the Diagnosis of Oral Squamous Cell Carcinoma" International Journal of Molecular Sciences 20, no. 11: 2749. https://doi.org/10.3390/ijms20112749