Correlation of the Aryl Hydrocarbon Receptor with FSHR in Ovarian Cancer Patients

 ,
,  , and
, and
Abstract
1. Introduction
2. Results
2.1. Highest Cytoplasmic AhR Staining in Clear Cell Ovarian Cancer
2.2. AhR Expression Correlates with Clinical and Pathological Data
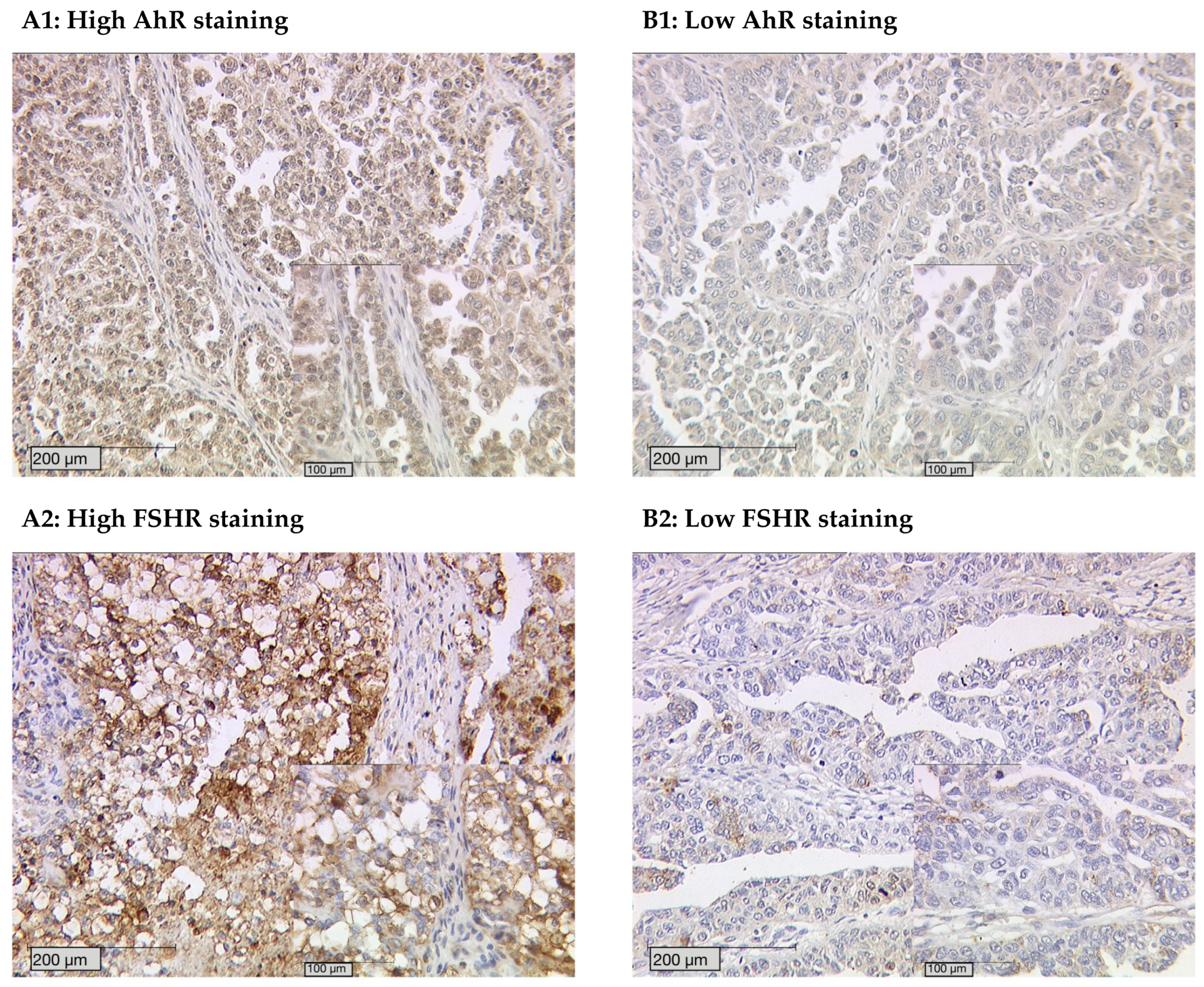
2.3. AhR Staining Intensity Correlates with FSHR Expression
2.4. Cytoplasmic AhR Expression Impairs Survival on its Own and Affects the Role of FSHR in Survival
2.5. Clinical and Pathological Parameters are Independent Prognostic Factors
3. Discussion
4. Materials and Methods
4.1. Patients and Specimens
4.2. Ethics Approval
4.3. Immunohistochemistry
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AhR | Aryl hydrocarbon receptor |
| FSH | Follicle-stimulating hormone |
| FSHR | Follicle-stimulating hormone receptor |
| IRS | Immunoreactive score |
| TCDD | 2,3,7,8-Tetrachlorodibenzo-p-dioxin |
References
- Oberaigner, W.; Minicozzi, P.; Bielska-Lasota, M.; Allemani, C.; de Angelis, R.; Mangone, L.; Sant, M.; Eurocare Working, G. Survival for ovarian cancer in europe: The across-country variation did not shrink in the past decade. Acta Oncol. 2012, 51, 441–453. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.; Naishadham, D.; Jemal, A. Cancer statistics, 2013. CA: Cancer J. Clin. 2013, 63, 11–30. [Google Scholar] [CrossRef] [PubMed]
- Aletti, G.D.; Gostout, B.S.; Podratz, K.C.; Cliby, W.A. Ovarian cancer surgical resectability: Relative impact of disease, patient status, and surgeon. Gynecol Oncol. 2006, 100, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Vergote, I.; De Brabanter, J.; Fyles, A.; Bertelsen, K.; Einhorn, N.; Sevelda, P.; Gore, M.E.; Kaern, J.; Verrelst, H.; Sjovall, K.; et al. Prognostic importance of degree of differentiation and cyst rupture in stage i invasive epithelial ovarian carcinoma. Lancet 2001, 357, 176–182. [Google Scholar] [CrossRef]
- Dembo, A.J.; Davy, M.; Stenwig, A.E.; Berle, E.J.; Bush, R.S.; Kjorstad, K. Prognostic factors in patients with stage i epithelial ovarian cancer. Obstet Gynecol. 1990, 75, 263–273. [Google Scholar] [PubMed]
- Yang, D.; Khan, S.; Sun, Y.; Hess, K.; Shmulevich, I.; Sood, A.K.; Zhang, W. Association of brca1 and brca2 mutations with survival, chemotherapy sensitivity, and gene mutator phenotype in patients with ovarian cancer. JAMA 2011, 306, 1557–1565. [Google Scholar] [CrossRef]
- Bolton, K.L.; Chenevix-Trench, G.; Goh, C.; Sadetzki, S.; Ramus, S.J.; Karlan, B.Y.; Lambrechts, D.; Despierre, E.; Barrowdale, D.; McGuffog, L.; et al. Association between brca1 and brca2 mutations and survival in women with invasive epithelial ovarian cancer. JAMA 2012, 307, 382–390. [Google Scholar] [CrossRef]
- Safe, S.; Lee, S.O.; Jin, U.H. Role of the aryl hydrocarbon receptor in carcinogenesis and potential as a drug target. Toxicol Sci. 2013, 135, 1–16. [Google Scholar] [CrossRef]
- Murray, I.A.; Patterson, A.D.; Perdew, G.H. Aryl hydrocarbon receptor ligands in cancer: Friend and foe. Nat. Rev. Cancer 2014, 14, 801–814. [Google Scholar] [CrossRef]
- Hernandez-Ochoa, I.; Karman, B.N.; Flaws, J.A. The role of the aryl hydrocarbon receptor in the female reproductive system. Biochem. Pharmacol. 2009, 77, 547–559. [Google Scholar] [CrossRef]
- Benedict, J.C.; Lin, T.M.; Loeffler, I.K.; Peterson, R.E.; Flaws, J.A. Physiological role of the aryl hydrocarbon receptor in mouse ovary development. Toxicol. Sci. 2000, 56, 382–388. [Google Scholar] [CrossRef] [PubMed]
- Benedict, J.C.; Miller, K.P.; Lin, T.M.; Greenfeld, C.; Babus, J.K.; Peterson, R.E.; Flaws, J.A. Aryl hydrocarbon receptor regulates growth, but not atresia, of mouse preantral and antral follicles. Biol. Reprod. 2003, 68, 1511–1517. [Google Scholar] [CrossRef] [PubMed]
- Barnett, K.R.; Tomic, D.; Gupta, R.K.; Babus, J.K.; Roby, K.F.; Terranova, P.F.; Flaws, J.A. The aryl hydrocarbon receptor is required for normal gonadotropin responsiveness in the mouse ovary. Toxicol. Appl. Pharmacol. 2007, 223, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Teino, I.; Kuuse, S.; Ingerpuu, S.; Maimets, T.; Tiido, T. The aryl hydrocarbon receptor regulates mouse FSHR promoter activity through an e-box binding site. Biol. Reprod. 2012, 86, 77. [Google Scholar] [CrossRef] [PubMed]
- Knerr, S.; Schrenk, D. Carcinogenicity of 2,3,7,8-tetrachlorodibenzo-p-dioxin in experimental models. Mol. Nutr. Food Res. 2006, 50, 897–907. [Google Scholar] [CrossRef] [PubMed]
- Andersson, P.; McGuire, J.; Rubio, C.; Gradin, K.; Whitelaw, M.L.; Pettersson, S.; Hanberg, A.; Poellinger, L. A constitutively active dioxin/aryl hydrocarbon receptor induces stomach tumors. Proc. Natl. Acad. Sci. USA 2002, 99, 9990–9995. [Google Scholar] [CrossRef] [PubMed]
- Moennikes, O.; Loeppen, S.; Buchmann, A.; Andersson, P.; Ittrich, C.; Poellinger, L.; Schwarz, M. A constitutively active dioxin/aryl hydrocarbon receptor promotes hepatocarcinogenesis in mice. Cancer Res. 2004, 64, 4707–4710. [Google Scholar] [CrossRef] [PubMed]
- Puga, A.; Xia, Y.; Elferink, C. Role of the aryl hydrocarbon receptor in cell cycle regulation. Chem. Biol. Interact. 2002, 141, 117–130. [Google Scholar] [CrossRef]
- DiNatale, B.C.; Schroeder, J.C.; Perdew, G.H. Ah receptor antagonism inhibits constitutive and cytokine inducible il6 production in head and neck tumor cell lines. Mol. Carcinog 2011, 50, 173–183. [Google Scholar] [CrossRef]
- Lin, P.; Chang, H.; Tsai, W.T.; Wu, M.H.; Liao, Y.S.; Chen, J.T.; Su, J.M. Overexpression of aryl hydrocarbon receptor in human lung carcinomas. Toxicol. Pathol. 2003, 31, 22–30. [Google Scholar] [CrossRef]
- Ishida, M.; Mikami, S.; Kikuchi, E.; Kosaka, T.; Miyajima, A.; Nakagawa, K.; Mukai, M.; Okada, Y.; Oya, M. Activation of the aryl hydrocarbon receptor pathway enhances cancer cell invasion by upregulating the mmp expression and is associated with poor prognosis in upper urinary tract urothelial cancer. Carcinogenesis 2010, 31, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Richmond, O.; Ghotbaddini, M.; Allen, C.; Walker, A.; Zahir, S.; Powell, J.B. The aryl hydrocarbon receptor is constitutively active in advanced prostate cancer cells. PLoS ONE 2014, 9, e95058. [Google Scholar] [CrossRef] [PubMed]
- Koliopanos, A.; Kleeff, J.; Xiao, Y.; Safe, S.; Zimmermann, A.; Buchler, M.W.; Friess, H. Increased arylhydrocarbon receptor expression offers a potential therapeutic target for pancreatic cancer. Oncogene 2002, 21, 6059–6070. [Google Scholar] [CrossRef] [PubMed]
- Gluschnaider, U.; Hidas, G.; Cojocaru, G.; Yutkin, V.; Ben-Neriah, Y.; Pikarsky, E. Beta-trcp inhibition reduces prostate cancer cell growth via upregulation of the aryl hydrocarbon receptor. PLoS ONE 2010, 5, e9060. [Google Scholar] [CrossRef] [PubMed]
- Portal-Nunez, S.; Shankavaram, U.T.; Rao, M.; Datrice, N.; Atay, S.; Aparicio, M.; Camphausen, K.A.; Fernandez-Salguero, P.M.; Chang, H.; Lin, P.; et al. Aryl hydrocarbon receptor-induced adrenomedullin mediates cigarette smoke carcinogenicity in humans and mice. Cancer Res. 2012, 72, 5790–5800. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zong, H.; Li, S.; Zhang, D.; Zhang, L.; Xia, Q. Activation of aryl hydrocarbon receptor suppresses invasion of esophageal squamous cell carcinoma cell lines. Tumori 2012, 98, 152–157. [Google Scholar] [CrossRef] [PubMed]
- Su, J.M.; Lin, P.; Chang, H. Prognostic value of nuclear translocation of aryl hydrocarbon receptor for non-small cell lung cancer. Anticancer Res. 2013, 33, 3953–3961. [Google Scholar]
- Saito, R.; Miki, Y.; Hata, S.; Takagi, K.; Iida, S.; Oba, Y.; Ono, K.; Ishida, T.; Suzuki, T.; Ohuchi, N.; et al. Aryl hydrocarbon receptor in breast cancer-a newly defined prognostic marker. Horm. Cancer 2014, 5, 11–21. [Google Scholar]
- Li, Y.; Wang, K.; Jiang, Y.Z.; Chang, X.W.; Dai, C.F.; Zheng, J. 2,3,7,8-tetrachlorodibenzo-p-dioxin (tcdd) inhibits human ovarian cancer cell proliferation. Cell Oncol. 2014, 37, 429–437. [Google Scholar] [CrossRef]
- Ouellet, V.; Guyot, M.C.; Le Page, C.; Filali-Mouhim, A.; Lussier, C.; Tonin, P.N.; Provencher, D.M.; Mes-Masson, A.M. Tissue array analysis of expression microarray candidates identifies markers associated with tumor grade and outcome in serous epithelial ovarian cancer. Int. J. Cancer 2006, 119, 599–607. [Google Scholar] [CrossRef]
- Hernandez-Ochoa, I.; Barnett-Ringgold, K.R.; Dehlinger, S.L.; Gupta, R.K.; Leslie, T.C.; Roby, K.F.; Flaws, J.A. The ability of the aryl hydrocarbon receptor to regulate ovarian follicle growth and estradiol biosynthesis in mice depends on stage of sexual maturity. Biol. Reprod. 2010, 83, 698–706. [Google Scholar] [CrossRef] [PubMed]
- Lenhard, M.; Lennerova, T.; Ditsch, N.; Kahlert, S.; Friese, K.; Mayr, D.; Jeschke, U. Opposed roles of follicle-stimulating hormone and luteinizing hormone receptors in ovarian cancer survival. Histopathology 2011, 58, 990–994. [Google Scholar] [CrossRef] [PubMed]
- Nakas, C.T.; Alonzo, T.A.; Yiannoutsos, C.T. Accuracy and cut-off point selection in three-class classification problems using a generalization of the youden index. Stat. Med. 2010, 29, 2946–2955. [Google Scholar] [CrossRef] [PubMed]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Fluss, R.; Faraggi, D.; Reiser, B. Estimation of the youden index and its associated cutoff point. Biom. J. 2005, 47, 458–472. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cytoplasmic AhR Expression | Nuclear AhR Expression | |||
|---|---|---|---|---|
| Variables | p | Correlation Coefficient | p | Correlation Coefficient |
| Histology | 0.000 | −0.296 | 0.002 | 0.274 |
| pT | 0.028 | 0.159 | 0.034 | −0.186 |
| pN | 0.101 | 0.136 | 0.147 | −0.162 |
| FIGO | 0.012 | 0.189 | 0.014 | 0.219 |
| Grading | ||||
| serous—low grading | 0.475 | −0.005 | 0.551 | 0.053 |
| serous—high grading | 0.004 | 0.216 | 0.052 | −0.170 |
| clear cell, endometrioid, and mucinous—G1 to G3 | 0.002 | −0.236 | 0.679 | 0.037 |
| Staining | AhR | High AhR Cytoplasm | FSHR |
|---|---|---|---|
| AhR | |||
| cc | 1.000 | 0.395 | 0.237 |
| p | . | 0.000 | 0.005 |
| n | 145 | 130 | 141 |
| high AhR cytoplasm | |||
| cc | 0.395 | 1.000 | 0.209 |
| p | 0.000 | . | 0.018 |
| n | 130 | 132 | 128 |
| FSHR | |||
| cc | 0.237 | 0.209 | 1.000 |
| p | 0.005 | 0.018 | . |
| n | 141 | 128 | 151 |
| Covariate | Coefficient (bi) | [HR Exp(bi)] | 95% CI | p-value | |
|---|---|---|---|---|---|
| Lower | Upper | ||||
| Histology serous clear cell endometrioid mucinous | −0.836 −0.441 −0.287 | 0.433 0.643 0.750 | 0.054 0.075 0.178 | 3.459 5.485 3.161 | 0.430 0.687 0.696 |
| FIGO (I, II vs. III, IV) | 1.097 | 2.994 | 1.420 | 6.315 | 0.004 |
| Grading serous low serous high clear cell, endometrioid and mucinous—G1 to G3 | −0.478 1.145 −0.002 | 0.630 3.141 0.998 | 0.146 0.889 0.422 | 2.631 11.101 2.363 | 0.517 0.076 0.997 |
| Patients’ age (≤60 vs. >60 years) | 0.580 | 1.786 | 1.095 | 2.914 | 0.020 |
| High AhR cytoplasmic | 0.074 | 1.077 | 0.653 | 1.776 | 0.771 |
| FSHR positive | −0.987 | 0.373 | 0.066 | 2.116 | 0.265 |
| AhR cytoplasmic and FSHR positive | 1.651 | 5.210 | 0.947 | 28.646 | 0.058 |
| Parameters | N | Percentage |
|---|---|---|
| Histology | ||
| serous | 110 | 70.5% |
| clear cell | 12 | 7.7% |
| endometrioid | 21 | 13.5% |
| mucinous | 13 | 8.3% |
| Lymph nodes | ||
| pNX pN0 | 61 43 | 39.1% 27.6% |
| pN1 | 52 | 33.3% |
| Distant Metastasis | ||
| pM0/X | 150 | 96.2% |
| pM1 | 6 | 3.8% |
| Grading serous | ||
| low | 24 | 23.0% |
| high endometrioid G1 G2 G3 mucinous G1 G2 G3 clear cell G3 | 80 6 5 8 6 6 0 9 | 77.0% 31.6% 26.3% 42.1% 50.0% 50.0% 0% 100% |
| FIGO | ||
| I II | 35 10 | 23.1% 6.6% |
| III IV | 103 3 | 68.2% 2.0% |
| Age | ||
| ≤60 years | 83 | 53.2% |
| >60 years | 73 | 46.8% |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deuster, E.; Mayr, D.; Hester, A.; Kolben, T.; Zeder-Göß, C.; Burges, A.; Mahner, S.; Jeschke, U.; Trillsch, F.; Czogalla, B. Correlation of the Aryl Hydrocarbon Receptor with FSHR in Ovarian Cancer Patients. Int. J. Mol. Sci. 2019, 20, 2862. https://doi.org/10.3390/ijms20122862
Deuster E, Mayr D, Hester A, Kolben T, Zeder-Göß C, Burges A, Mahner S, Jeschke U, Trillsch F, Czogalla B. Correlation of the Aryl Hydrocarbon Receptor with FSHR in Ovarian Cancer Patients. International Journal of Molecular Sciences. 2019; 20(12):2862. https://doi.org/10.3390/ijms20122862
Chicago/Turabian StyleDeuster, Eileen, Doris Mayr, Anna Hester, Thomas Kolben, Christine Zeder-Göß, Alexander Burges, Sven Mahner, Udo Jeschke, Fabian Trillsch, and Bastian Czogalla. 2019. "Correlation of the Aryl Hydrocarbon Receptor with FSHR in Ovarian Cancer Patients" International Journal of Molecular Sciences 20, no. 12: 2862. https://doi.org/10.3390/ijms20122862
APA StyleDeuster, E., Mayr, D., Hester, A., Kolben, T., Zeder-Göß, C., Burges, A., Mahner, S., Jeschke, U., Trillsch, F., & Czogalla, B. (2019). Correlation of the Aryl Hydrocarbon Receptor with FSHR in Ovarian Cancer Patients. International Journal of Molecular Sciences, 20(12), 2862. https://doi.org/10.3390/ijms20122862