Abdominal Fat SIRT6 Expression and Its Relationship with Inflammatory and Metabolic Pathways in Pre-Diabetic Overweight Patients


 and
and 
Abstract
:1. Introduction
2. Results
2.1. Clinical Characteristics of the Study Population
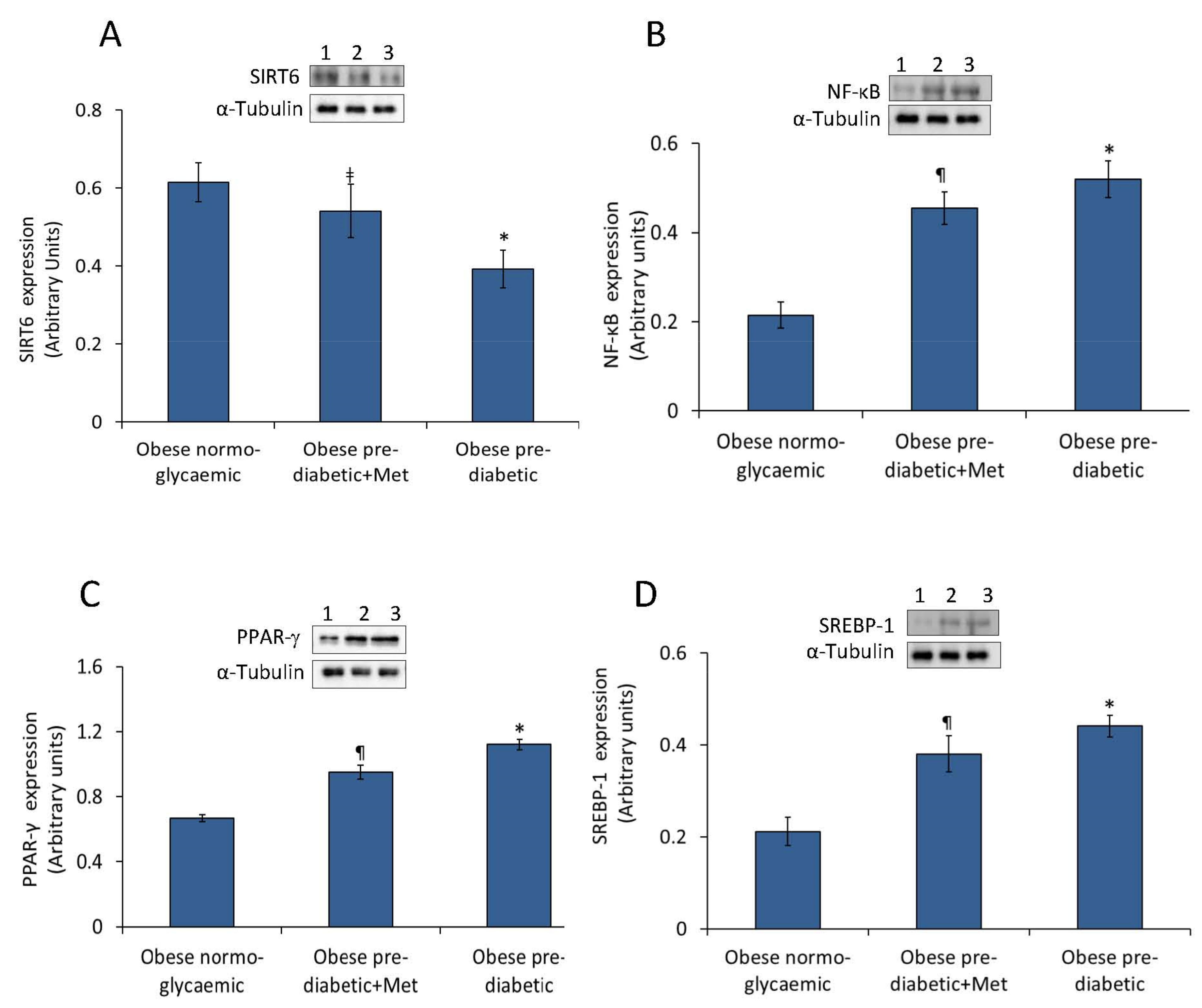
2.2. Abdominal Adipose Tissue Expression of SIRT6, NF-κB, PPAR-γ, and SREBP-1
3. Discussion
4. Materials and Methods
4.1. Research Design
4.2. Anthropometrics Parameters
4.3. Blood Sample Analyses
4.4. Abdominal Dermolipectomy
4.5. Analysis of Adipose Tissue
4.6. Western Blot Analysis
4.7. Statistical Analysis
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| CRP | C reactive protein |
| IL-6 | Interleukin 6 |
| LVEF | Left ventricle ejection fraction |
| MPI | Myocardial performance index |
| NF-κB | Nuclear factor kappa-light-chain-enhancer of activated B cells |
| NG | Normoglycemic |
| PPAR-γ | Peroxisome proliferator-activated receptor gamma |
| pre-DM | Pre-diabetic |
| SIRT1 | Sirtuin 1 |
| SIRT6 | Sirtuin 6 |
| SREBP-1 | Sterol regulatory element-binding transcription factor-1 |
| TNF-α | Tumor necrosis factor-α |
References
- Marfella, R.; Grella, R.; Barbieri, M.; Grella, R.; Ferraraccio, F.; Cacciapuoti, F.; Mazzarella, G.; Ferraro, N.; D’Andrea, F.; Paolisso, G.; et al. Role of subcutaneous abdominal on cardiac function and proinflammatory cytokines in premenopausal obese women. Ann. Plast. Surg. 2009, 63, 490–495. [Google Scholar] [CrossRef] [PubMed]
- Sardu, C.; Pieretti, G.; D’Onofrio, N.; Ciccarelli, F.; Paolisso, P.; Passavanti, M.B.; Marfella, R.; Cioffi, M.; Mone, P.; Dalise, A.M.; et al. Inflammatory cytokines and SIRT1 levels in subcutaneous abdominal fat. Relationship with cardiac performance in overweight pre-diabetics patients. Front. Physiol. 2018, 9, 1030. [Google Scholar] [CrossRef] [PubMed]
- Rappou, E.; Jukarainen, S.; Rinnankoski-Tuikka, R.; Kaye, S.; Heinonen, S.; Hakkarainen, A.; Lundbom, J.; Lundbom, N.; Saunavaara, V.; Rissanen, A.; et al. Weight loss is associated with increased NAD(+)/SIRT1 expression but reduced PARP activity in white adipose tissue. J. Clin. Endocrinol. Metab. 2016, 101, 1263–1273. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Cai, X.; Mai, W.; Li, M.; Hu, Y. Association between prediabetes and risk of cardiovascular disease and all cause mortality: Systematic review and meta-analysis. BMJ 2016, 355, i5953. [Google Scholar] [CrossRef] [PubMed]
- Kuang, J.; Chen, L.; Tang, Q.; Zhang, J.; Li, Y.; He, J. The Role of Sirt6 in Obesity and Diabetes. Front. Physiol. 2018, 27, 135. [Google Scholar] [CrossRef]
- D’Onofrio, N.; Servillo, L.; Balestrieri, M.L. SIRT1 and SIRT6 Signaling Pathways in Cardiovascular Disease Protection. Antioxid. Redox Signal. 2018, 28, 711–732. [Google Scholar] [CrossRef]
- Vachharajani, V.T.; Liu, T.; Wang, X.; Hoth, J.J.; Yoza, B.K.; McCall, C.E. Sirtuins Link Inflammation and Metabolism. J. Immunol. Res. 2016, 2016, 8167273. [Google Scholar] [CrossRef]
- Xiong, X.; Zhang, C.; Zhang, Y.; Fan, R.; Qian, X.; Dong, X.C. Fabp4-Cre-mediated Sirt6 deletion impairs adipose tissue function and metabolic homeostasis in mice. J. Endocrinol. 2017, 233, 307–314. [Google Scholar] [CrossRef]
- Kuang, J.; Zhang, Y.; Liu, Q.; Shen, J.; Pu, S.; Cheng, S.; Chen, L.; Li, H.; Wu, T.; Li, R.; et al. Fat-Specific Sirt6 Ablation Sensitizes Mice to High-Fat Diet-Induced Obesity and Insulin Resistance by Inhibiting Lipolysis. Diabetes 2017, 66, 1159–1171. [Google Scholar] [CrossRef]
- Lawrence, T. The Nuclear Factor NF-κB Pathway in Inflammation. Cold Spring Harb. Perspect. Biol. 2009, 1, a001651. [Google Scholar] [CrossRef]
- Picard, F.; Auwerx, J. PPARγ and glucose homeostasis. Annu. Rev. Nutr. 2002, 22, 167–197. [Google Scholar] [CrossRef] [PubMed]
- Eberlé, D.; Hegarty, B.; Bossard, P.; Ferré, P.; Foufelle, F. SREBP transcription factors: Master regulators of lipid homeostasis. Biochimie 2004, 86, 839–848. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Li, H.; Guo, Q.; Zhang, L.; Zhu, J.; Ji, J. Sirtuin6 inhibits c-triggered inflammation through TLR4 abrogation regulated by ROS and TRPV1/CGRP. J. Cell Biochem. 2018, 119, 9141–9153. [Google Scholar] [CrossRef] [PubMed]
- Xiao, C.; Wang, R.H.; Lahusen, T.J.; Park, O.; Bertola, A.; Maruyama, T.; Reynolds, D.; Chen, Q.; Xu, X.; Young, H.A.; et al. Progression of chronic liver inflammation and fibrosis driven by activation of c-JUN signaling in Sirt6 mutant mice. J. Biol. Chem. 2012, 287, 41903–41913. [Google Scholar] [CrossRef] [PubMed]
- Balestrieri, M.L.; Rizzo, M.R.; Barbieri, M.; Paolisso, P.; D’Onofrio, N.; Giovane, A.; Siniscalchi, M.; Minicucci, F.; Sardu, C.; D’Andrea, D.; et al. Sirtuin 6 expression and inflammatory activity in diabetic atherosclerotic plaques: Effects of incretin treatment. Diabetes 2015, 64, 1395–1406. [Google Scholar] [CrossRef] [PubMed]
- Hu, S.; Liu, H.; Ha, Y.; Luo, X.; Motamedi, M.; Gupta, M.P.; Ma, J.X.; Tilton, R.G.; Zhang, W. Posttranslational Modification of Sirt6 Activity by Peroxynitrite. Free Radic. Biol. Med. 2015, 79, 176–185. [Google Scholar] [CrossRef] [PubMed]
- Esteghamati, A.; Eskandari, D.; Mirmiranpour, H.; Noshad, S.; Mousavizadeh, M.; Hedayati, M.; Nakhjavani, M. Effects of metformin on markers of oxidative stress and antioxidant reserve in patients with newly diagnosed type 2 diabetes: A randomized clinical trial. Clin. Nutr. 2013, 32, 179–185. [Google Scholar] [CrossRef]
- Mostoslavsky, R.; Chua, K.F.; Lombard, D.B.; Pang, W.W.; Fischer, M.R.; Gellon, L.; Liu, P.; Mostoslavsky, G.; Franco, S.; Murphy, M.M.; et al. Genomic instability and aging-like phenotype in the absence of mammalian SIRT6. Cell 2006, 124, 315–329. [Google Scholar] [CrossRef]
- Zhong, L.; D’Urso, A.; Toiber, D.; Sebastian, C.; Henry, R.E.; Vadysirisack, D.D.; Guimaraes, A.; Marinelli, B.; Wikstrom, J.D.; Nir, T.; et al. The histone deacetylase Sirt6 regulates glucose homeostasis via Hif1alpha. Cell 2010, 140, 280–923. [Google Scholar] [CrossRef]
- Dominy, J.E., Jr.; Lee, Y.; Jedrychowski, M.P.; Chim, H.; Jurczak, M.J.; Camporez, J.P.; Ruan, H.B.; Feldman, J.; Pierce, K.; Mostoslavsky, R.; et al. The deacetylase Sirt6 activates the acetyltransferase GCN5 and suppresses hepatic gluconeogenesis. Mol. Cell 2012, 48, 900–913. [Google Scholar] [CrossRef]
- Puigserver, P.; Rhee, J.; Donovan, J.; Walkey, C.J.; Yoon, J.C.; Oriente, F.; Kitamura, Y.; Altomonte, J.; Dong, H.; Accili, D.; et al. Insulin-regulated hepatic gluconeogenesis through FOXO1-PGC-1alpha interaction. Nature 2003, 423, 550–555. [Google Scholar] [CrossRef] [PubMed]
- Xiong, X.; Tao, R.; DePinho, R.A.; Dong, X.C. Deletion of hepatic FoxO1/3/4 genes in mice significantly impacts on glucose metabolism through downregulation of gluconeogenesis and upregulation of glycolysis. PLoS ONE 2013, 8, e74340. [Google Scholar] [CrossRef] [PubMed]
- Song, M.Y.; Wang, J.; Ka, S.O.; Bae, E.J.; Park, B.H. Insulin secretion impairment in Sirt6 knockout pancreatic β cells is mediated by suppression of the FoxO1-Pdx1-Glut2 pathway. Sci. Rep. 2016, 6, 30321. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Xiao, C.; Wang, R.H.; Lahusen, T.; Xu, X.; Vassilopoulos, A.; Vazquez-Ortiz, G.; Jeong, W.I.; Park, O.; Ki, S.H.; et al. Hepatic-specific disruption of SIRT6 in mice results in fatty liver formation due to enhanced glycolysis and triglyceride synthesis. Cell Metab. 2010, 12, 224–236. [Google Scholar] [CrossRef] [PubMed]
- Tao, R.; Xiong, X.; Depinho, R.A.; Deng, C.X.; Dong, X.C. FoxO3 transcription factor and Sirt6 deacetylase regulate low density lipoprotein (LDL)-cholesterol homeostasis via control of the proprotein convertase Subtilisin/Kexin type 9 (Pcsk9) gene expression. J. Biol. Chem. 2013, 288, 29252–29259. [Google Scholar] [CrossRef] [PubMed]
- Tao, R.; Xiong, X.; Depinho, R.A.; Deng, C.X.; Dong, X.C. Hepatic SREBP-2 and and cholesterol biosynthesis are regulated by FoxO3 and Sirt6. J. Lipid Res. 2013, 54, 2745–2753. [Google Scholar] [CrossRef] [PubMed]
- Lambert, G.; Sjouke, B.; Choque, B.; Kastelein, J.J.; Hovingh, G.K. The PCSK9 decade. J. Lipid Res. 2012, 53, 2515–2524. [Google Scholar] [CrossRef]
- Elhanati, S.; Kanfi, Y.; Varvak, A.; Roichman, A.; Carmel-Gross, I.; Barth, S.; Gibor, G.; Cohen, H.Y. Multiple regulatory layers of SREBP1/2 by SIRT6. Cell Rep. 2013, 4, 905–912. [Google Scholar] [CrossRef]
- Kanfi, Y.; Peshti, V.; Gil, R.; Naiman, S.; Nahum, L.; Levin, E.; Kronfeld-Schor, N.; Cohen, H.Y. SIRT6 protects against pathological damage caused by diet-induced obesity. Aging Cell 2010, 9, 162–173. [Google Scholar] [CrossRef]
- Yang, S.J.; Choi, J.M.; Chae, S.W.; Kim, W.J.; Park, S.E.; Rhee, E.J.; Lee, W.Y.; Oh, K.W.; Park, S.W.; Kim, S.W.; et al. Activation of peroxisome proliferator-activated receptor gamma by rosiglitazone increases sirt6 expression and ameliorates hepatic steatosis in rats. PLoS ONE 2011, 6, e17057. [Google Scholar] [CrossRef]
- Martínez-Jiménez, V.; Cortez-Espinosa, N.; Rodríguez-Varela, E.; Vega-Cárdenas, M.; Briones-Espinoza, M.; Ruíz-Rodríguez, V.M.; López-López, N.; Briseño-Medina, A.; Turiján-Espinoza, E.; Portales-Pérez, D.P. Altered levels of sirtuin genes (SIRT1, SIRT2, SIRT3 and SIRT6) and their target genes in adipose tissue from individual with obesity. Diabetes Metab. Syndr. 2019, 13, 582–589. [Google Scholar] [CrossRef] [PubMed]
- Sozer, S.O.; Agullo, F.J.; Santillan, A.A.; Wolf, C. Decision making in abdominoplasty. Aesthet. Plast. Surg. 2007, 31, 117–127. [Google Scholar] [CrossRef] [PubMed]
- WHO. Obesity: Preventing and Managing the Global Epidemic—Report of a WHO Consultation; World Health Organization: Geneva, Switzerland, 2000; pp. 1–253. [Google Scholar]
- Standards of Medical Care in Diabetes 2017. Diabetes Care 2017, 40, S1–S2.


{kind=link}
| Study Variables | Obese NG (n = 18) | Obese Pre-DM + Metformin (n = 16) | Obese Pre-DM + Placebo (n = 16) | p Value |
|---|---|---|---|---|
| Baseline | ||||
| Clinical variables | ||||
| Age | 39.0 ± 8 | 40.5 ± 7 | 40.5 ± 6 | / |
| Male (%) | 5 (27.8) | 5 (25) | 6 (30) | / |
| BMI (kg/m2) | 33.7 ± 2.4 | 33.1 ± 2.7 | 33.5 ± 2.6 | / |
| Systolic arterial pressure (mmHg) | 126 ± 10.3 | 133 ± 11 | 129 ± 12 | / |
| Diastolic arterial pressure (mmHg) | 85 ± 2.1 | 82 ± 2.3 | 84 ± 2.1 | / |
| Heart rate (beats for minute) | 69 ± 8 | 72 ± 9 | 72 ± 10 | / |
| WHR | 0.91 ± 0.001 | 0.91 ± 0.006 | 0.91 ± 0.005 | / |
| HOMA-IR | 4.1 ± 0.28 | 4.7 ± 0.72 | 4.9 ± 0.68 | <0.05 *, <0.05 ** |
| Insulin (µU/mL) | 22.6 ± 1.9 | 20.9 ± 1.6 | 20.1 ± 1.8 | <0.05 *, <0.05 ** |
| Glucose (mmol/L) | 5.34 ± 0.57 | 5.81 ± 0.18 | 6.73 ± 0.24 | <0.05 *, <0.05 **, <0.05 *** |
| Cholesterol (mmol/L) | 4.66 ± 1.02 | 4.33 ± 0.86 | 4.51 ± 0.88 | / |
| HDL (mmol/L) | 1.78 ± 0.41 | 1.73 ± 0.44 | 1.83 ± 0.39 | / |
| LDL (mmol/L) | 3.17 ± 0.59 | 3.31 ± 0.61 | 3.33 ± 0.57 | / |
| Triglycerides (mmol/L) | 1.61 ± 0.31 | 1.89 ± 0.44 | 1.83 ± 0.54 | / |
| Creatinine (mmol/L) | 78.3 ± 2.6 | 98.6 ± 4.4 | 101.2 ± 3.5 | <0.05 *, <0.05 ** |
| Biohumoral inflammatory markers | ||||
| CRP (mmol/L) | 0.85 ± 0.38 | 0.97 ± 0.48 | 1.03 ± 0.43 | <0.05 *, <0.05 ** |
| IL-6 (pg/mL) | 3.53 ± 0.43 | 3.81 ± 0.45 | 4.10 ± 0.39 | <0.05 *, <0.05 ** |
| TNF-α (pg/mL) | 5.51 ± 1.09 | 6.19 ± 0.59 | 6.75 ± 0.53 | <0.05 *, <0.05 ** |
| Nitrotyrosine (nmol/L) | 1.211 ± 0.205 | 3.283 ± 0.712 | 5.309 ± 0.651 | <0.05 *, <0.05 **, <0.05 *** |
| Adipose tissue markers | ||||
| SIRT6 (arbitrary units) | 1.14 ± 0.18 | 1.05 ± 0.14 | 0.94 ± 0.12 | <0.05 *, <0.05 **, <0.05 *** |
| NF-κB (arbitrary units) | 0.91 ± 0.06 | 1.02 ± 0.12 | 1.10 ± 0.09 | <0.05 *, <0.05 **, <0.05 *** |
| PPAR-γ (arbitrary units) | 0.67 ± 0.03 | 0.99 ± 0.04 | 1.07 ± 0.03 | <0.05 *, <0.05 **, <0.05 *** |
| SREBP-1 (arbitrary units) | 0.21 ± 0.03 | 0.39 ± 0.04 | 0.44 ± 0.02 | <0.05 *, <0.05 **, <0.05 *** |
| Echocardiographic parameters | ||||
| Intima-media thickness | 0.85 ± 0.14 | 1.01 ± 0.15 | 1.03 ± 0.18 | <0.05 *, <0.05 ** |
| LVTDd (mm) | 54 ± 4.6 | 56 ± 3.8 | 55 ± 4.1 | / |
| LVTSd (mm) | 31 ± 6.7 | 34 ± 4.4 | 32 ± 4.8 | / |
| LVEF (%) | 53 ± 6 | 54 ± 6 | 54 ± 7 | / |
| LAD (mm) | 42 ± 2 | 45 ± 6 | 43 ± 6 | / |
| Septum (mm) | 13.5 ± 2.6 | 14 ± 2.5 | 14 ± 2.2 | / |
| Posterior wall (mm) | 11 ± 1 | 11 ± 1.5 | 11 ± 1 | / |
| MPI | 0.57 ± 0.03 | 0.58 ± 0.03 | 0.57 ± 0.03 | / |
| LV mass (g) | 203.7 ± 48.4 | 192.5 ± 49.5 | 191.7 ± 49.7 | / |
| LV mass/BSA (g/m2) | 90.13 ± 21.42 | 84.06 ± 21.62 | 82.62 ± 21.42 | / |
| LV mass/h (m2) | 72.23 ± 17.16 | 69 ± 17.75 | 67.03 ± 17.38 | / |
| Drug therapy | ||||
| ACE inhibitors (%) | 9 (50) | 8 (50) | 9 (56.2) | / |
| ARS blockers (%) | 5 (28) | 5 (31.2) | 5 (31.2) | / |
| Calcium channels blockers (%) | 2 (11.1) | 2 (12.5) | 2 (12.5) | / |
| Loop diuretics (%) | 2 (11.1) | 2 (12.5) | 2 (12.5) | / |
| Metformin (%) | 0 | 16 (100%) | 0 | |
| Statin (%) | 7 (39) | 8 (50) | 9 (56.2) | / |
| Thiazides (%) | 5 (27.8) | 5 (31.2) | 6 (37.5) | / |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Onofrio, N.; Pieretti, G.; Ciccarelli, F.; Gambardella, A.; Passariello, N.; Rizzo, M.R.; Barbieri, M.; Marfella, R.; Nicoletti, G.; Balestrieri, M.L.; et al. Abdominal Fat SIRT6 Expression and Its Relationship with Inflammatory and Metabolic Pathways in Pre-Diabetic Overweight Patients. Int. J. Mol. Sci. 2019, 20, 1153. https://doi.org/10.3390/ijms20051153
D’Onofrio N, Pieretti G, Ciccarelli F, Gambardella A, Passariello N, Rizzo MR, Barbieri M, Marfella R, Nicoletti G, Balestrieri ML, et al. Abdominal Fat SIRT6 Expression and Its Relationship with Inflammatory and Metabolic Pathways in Pre-Diabetic Overweight Patients. International Journal of Molecular Sciences. 2019; 20(5):1153. https://doi.org/10.3390/ijms20051153
Chicago/Turabian StyleD’Onofrio, Nunzia, Gorizio Pieretti, Feliciano Ciccarelli, Antonio Gambardella, Nicola Passariello, Maria Rosaria Rizzo, Michelangela Barbieri, Raffaele Marfella, Gianfranco Nicoletti, Maria Luisa Balestrieri, and et al. 2019. "Abdominal Fat SIRT6 Expression and Its Relationship with Inflammatory and Metabolic Pathways in Pre-Diabetic Overweight Patients" International Journal of Molecular Sciences 20, no. 5: 1153. https://doi.org/10.3390/ijms20051153