Effect of Ischemic Preconditioning and Postconditioning on Exosome-Rich Fraction microRNA Levels, in Relation with Electrophysiological Parameters and Ventricular Arrhythmia in Experimental Closed-Chest Reperfused Myocardial Infarction

 , , , , ,
, , , , ,  and
and
Abstract
:1. Introduction
2. Results
2.1. Ischemia-Related ECG Parameters
2.2. Conduction-Related ECG Parameters
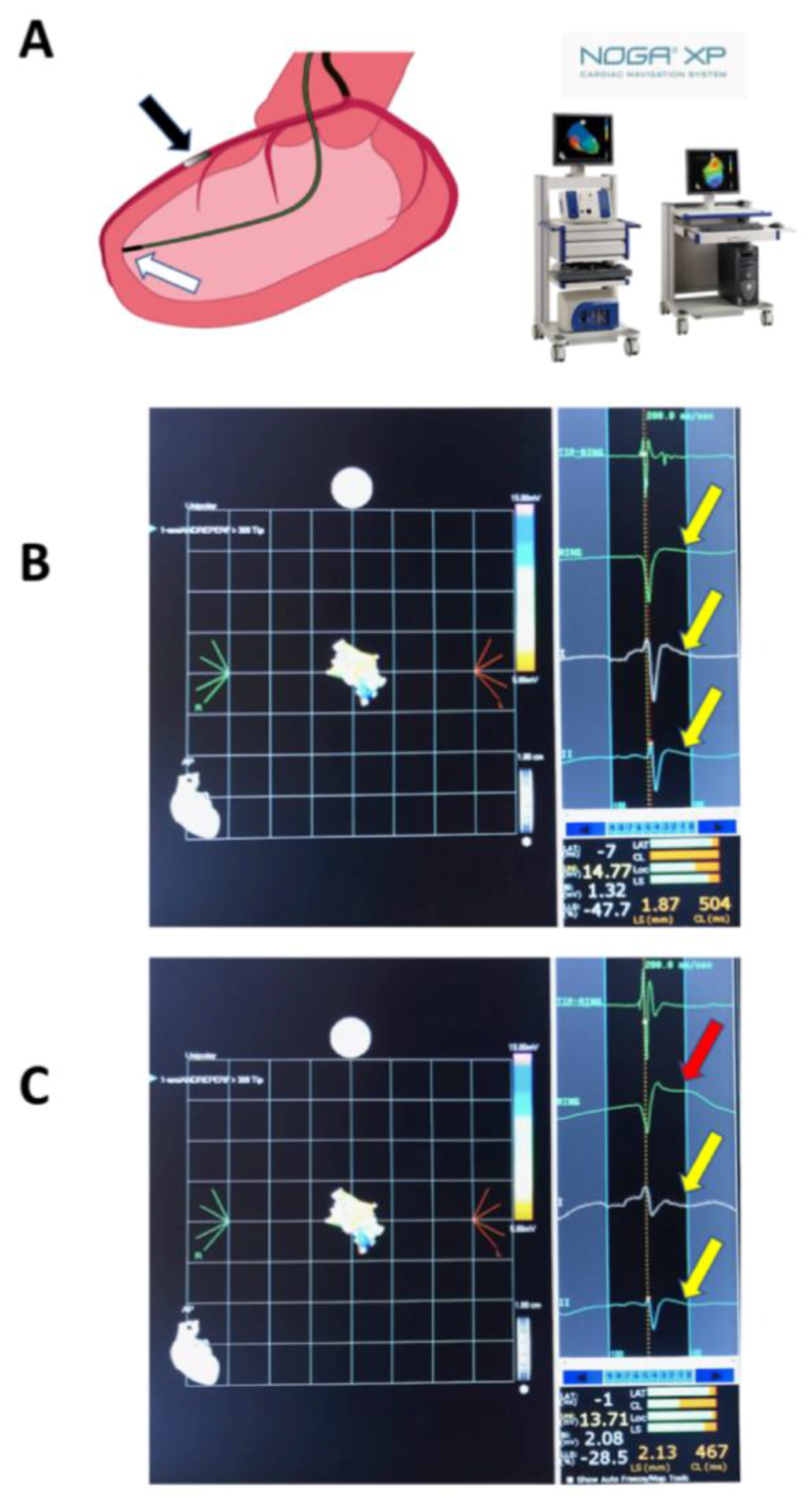
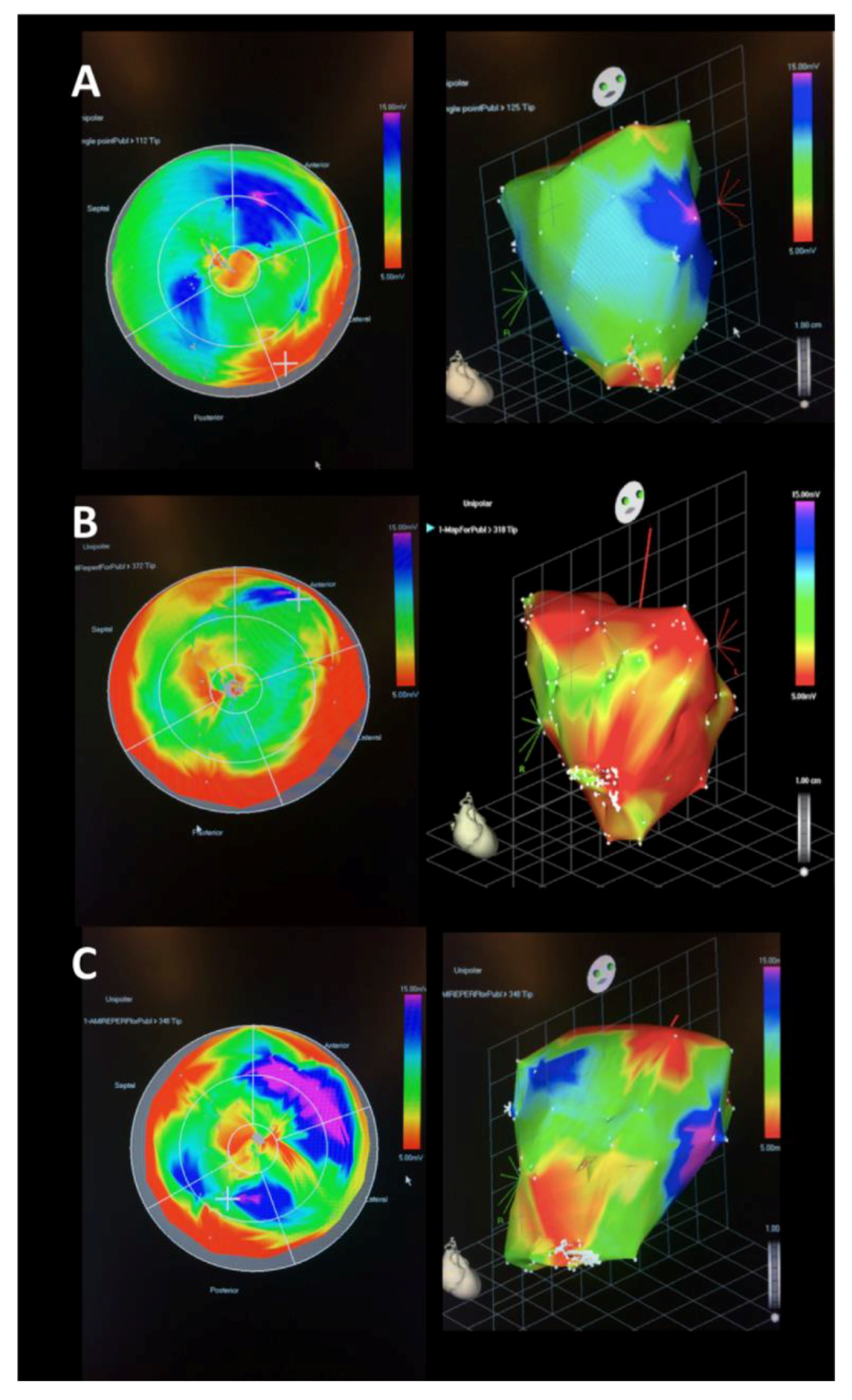
2.3. NOGA Electroanatomical Mapping
2.4. Arrhythmia Scores
2.5. Plasma TnI and Creatine Kinase (CK) Values
2.6. qPCR Results
2.7. cMRI Results
3. Discussion
Limitations
4. Materials and Methods
4.1. Study Design
4.2. Animal Preparation
4.3. Intracardiac ECG
4.4. Scoring of Ventricular Arrhythmias
4.5. Cardiac cMRI with Late Enhancement
4.6. Measurements of Ischemia Biomarkers Troponin I and Creatine Kinase
4.7. Isolation of Exosome-Rich Fraction
4.8. miR Isolation and qPCR
4.9. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Yellon, D.M.; Hausenloy, D.J. Myocardial reperfusion injury. N. Engl. J. Med. 2007, 357, 1121–1135. [Google Scholar] [CrossRef]
- Ferrari, R.; Balla, C.; Malagu, M.; Guardigli, G.; Morciano, G.; Bertini, M.; Biscaglia, S.; Campo, G. Reperfusion Damage—A Story of Success, Failure, and Hope. Circ. J. 2017, 81, 131–141. [Google Scholar] [CrossRef]
- Hausenloy, D.J.; Garcia-Dorado, D.; Botker, H.E.; Davidson, S.M.; Downey, J.; Engel, F.B.; Jennings, R.; Lecour, S.; Leor, J.; Madonna, R.; et al. Novel targets and future strategies for acute cardioprotection: Position Paper of the European Society of Cardiology Working Group on Cellular Biology of the Heart. Cardiovasc. Res. 2017, 113, 564–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manning, A.S.; Hearse, D.J. Reperfusion-induced arrhythmias: Mechanisms and prevention. J. Mol. Cell. Cardiol. 1984, 16, 497–518. [Google Scholar] [CrossRef]
- Lekli, I.; Haines, D.D.; Balla, G.; Tosaki, A. Autophagy: An adaptive physiological countermeasure to cellular senescence and ischaemia/reperfusion-associated cardiac arrhythmias. J. Cell. Mol. Med. 2017, 21, 1058–1072. [Google Scholar] [CrossRef]
- Chen, Z.; Luo, H.; Zhuang, M.; Cai, L.; Su, C.; Lei, Y.; Zou, J. Effects of ischemic preconditioning on ischemia/reperfusion-induced arrhythmias by upregulatation of connexin 43 expression. J. Cardiothorac. Surg. 2011, 6, 80. [Google Scholar] [CrossRef] [PubMed]
- Okishige, K.; Yamashita, K.; Yoshinaga, H.; Azegami, K.; Satoh, T.; Goseki, Y.; Fujii, S.; Ohira, H.; Satake, S. Electrophysiologic effects of ischemic preconditioning on QT dispersion during coronary angioplasty. J. Am. Coll. Cardiol. 1996, 28, 70–73. [Google Scholar] [CrossRef] [Green Version]
- Kolettis, T.M.; Vilaeti, A.D.; Tsalikakis, D.G.; Zoga, A.; Valenti, M.; Tzallas, A.T.; Papalois, A.; Iliodromitis, E.K. Effects of pre- and postconditioning on arrhythmogenesis in the in vivo rat model. J. Cardiovasc. Pharmacol. Ther. 2013, 18, 376–385. [Google Scholar] [CrossRef] [PubMed]
- Araszkiewicz, A.; Grygier, M.; Pyda, M.; Rajewska, J.; Lesiak, M.; Grajek, S. Postconditioning attenuates early ventricular arrhythmias in patients with high-risk ST-segment elevation myocardial infarction. J. Cardiol. 2015, 65, 459–465. [Google Scholar] [CrossRef] [Green Version]
- Favaretto, E.; Roffi, M.; Frigo, A.C.; Lee, M.S.; Marra, M.P.; Napodano, M.; Tarantini, G. Meta-Analysis of Randomized Trials of Postconditioning in ST-Elevation Myocardial Infarction. Am. J. Cardiol. 2014, 114, 946–952. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.R.; Binabdulhak, A.A.; Alastal, Y.; Khan, S.; Faricy-Beredo, B.M.; Luni, F.K.; Lee, W.M.; Khuder, S.; Tinkel, J. Cardioprotective role of ischemic postconditioning in acute myocardial infarction: A systematic review and meta-analysis. Am. Heart J. 2014, 168, 512–521.e4. [Google Scholar] [CrossRef]
- Tarantini, G.; Favaretto, E.; Marra, M.P.; Frigo, A.C.; Napodano, M.; Cacciavillani, L.; Giovagnoni, A.; Renda, P.; De Biasio, V.; Plebani, M.; et al. Postconditioning during coronary angioplasty in acute myocardial infarction: The POST-AMI trial. Int. J. Cardiol. 2012, 162, 33–38. [Google Scholar] [CrossRef]
- Touboul, C.; Angoulvant, D.; Mewton, N.; Ivanes, F.; Muntean, D.; Prunier, F.; Ovize, M.; Bejan-Angoulvant, T. Ischaemic postconditioning reduces infarct size: Systematic review and meta-analysis of randomized controlled trials. Arch. Cardiovasc. Dis. 2015, 108, 39–49. [Google Scholar] [CrossRef] [Green Version]
- Yang, X.M.; Liu, Y.; Liu, Y.; Tandon, N.; Kambayashi, J.; Downey, J.M.; Cohen, M.V. Attenuation of infarction in cynomolgus monkeys: Preconditioning and postconditioning. Basic Res. Cardiol. 2010, 105, 119–128. [Google Scholar] [CrossRef]
- Hansen, P.R.; Thibault, H.; Abdulla, J. Postconditioning during primary percutaneous coronary intervention: A review and meta-analysis. Int. J. Cardiol. 2010, 144, 22–25. [Google Scholar] [CrossRef]
- Freixa, X.; Bellera, N.; Ortiz-Perez, J.T.; Jimenez, M.; Pare, C.; Bosch, X.; De Caralt, T.M.; Betriu, A.; Masotti, M. Ischaemic postconditioning revisited: Lack of effects on infarct size following primary percutaneous coronary intervention. Eur. Heart J. 2012, 33, 103–112. [Google Scholar] [CrossRef]
- Ferdinandy, P.; Hausenloy, D.J.; Heusch, G.; Baxter, G.F.; Schulz, R. Interaction of risk factors, comorbidities, and comedications with ischemia/reperfusion injury and cardioprotection by preconditioning, postconditioning, and remote conditioning. Pharmacol. Rev. 2014, 66, 1142–1174. [Google Scholar] [CrossRef]
- Baranyai, T.; Giricz, Z.; Varga, Z.V.; Koncsos, G.; Lukovic, D.; Makkos, A.; Sárközy, M.; Pávó, N.; Jakab, A.; Czimbalmos, C.; et al. In vivo MRI and ex vivo histological assessment of the cardioprotection induced by ischemic preconditioning, postconditioning and remote conditioning in a closed-chest porcine model of reperfused acute myocardial infarction: Importance of microvasculature. J. Transl. Med. 2017, 15, 67. [Google Scholar] [CrossRef]
- Kloner, R.A.; Dow, J.; Bhandari, A. Postconditioning markedly attenuates ventricular arrhythmias after ischemia-reperfusion. J. Cardiovasc. Pharmacol. Ther. 2006, 11, 55–63. [Google Scholar] [CrossRef]
- Dow, J.; Bhandari, A.; Kloner, R.A. Ischemic postconditioning’s benefit on reperfusion ventricular arrhythmias is maintained in the senescent heart. J. Cardiovasc. Pharmacol. Ther. 2008, 13, 141–148. [Google Scholar] [CrossRef]
- Sasaki, H.; Shimizu, M.; Ogawa, K.; Okazaki, F.; Taniguchi, M.; Taniguchi, I.; Mochizuki, S. Brief ischemia-reperfusion performed after prolonged ischemia (ischemic postconditioning) can terminate reperfusion arrhythmias with no reduction of cardiac function in rats. Int. Heart J. 2007, 48, 205–213. [Google Scholar] [CrossRef]
- Okishige, K.; Kanda, S.; Shimura, T.; Kurabayashi, M.; Ueshima, D.; Miwa, N.; Sugiyama, K.; Aoyagi, H.; Yoshimura, K.; Yanagi, H.; et al. Clinical study of the electrophysiological effects of ischemic post-conditioning in patients with acute myocardial infarctions. J. Cardiol. 2011, 58, 137–142. [Google Scholar] [CrossRef] [Green Version]
- Galagudza, M.; Kurapeev, D.; Minasian, S.; Valen, G.; Vaage, J. Ischemic postconditioning: Brief ischemia during reperfusion converts persistent ventricular fibrillation into regular rhythm. Eur. J. Cardio-Thoracic Surg. 2004, 25, 1006–1010. [Google Scholar] [CrossRef]
- Yamaguchi, T.; Izumi, Y.; Nakamura, Y.; Yamazaki, T.; Shiota, M.; Sano, S.; Tanaka, M.; Osada-Oka, M.; Shimada, K.; Miura, K.; et al. Repeated remote ischemic conditioning attenuates left ventricular remodeling via exosome-mediated intercellular communication on chronic heart failure after myocardial infarction. Int. J. Cardiol. 2015, 178, 239–246. [Google Scholar] [CrossRef]
- Bostjancic, E.; Zidar, N.; Stajer, D.; Glavac, D. MicroRNAs miR-1, miR-133a, miR-133b and miR-208 are dysregulated in human myocardial infarction. Cardiology 2010, 115, 163–169. [Google Scholar] [CrossRef]
- Corsten, M.F.; Dennert, R.; Jochems, S.; Kuznetsova, T.; Devaux, Y.; Hofstra, L.; Wagner, D.R.; Staessen, J.A.; Heymans, S.; Schroen, B. Circulating MicroRNA-208b and MicroRNA-499 reflect myocardial damage in cardiovascular disease. Circ. Cardiovasc. Genetics 2010, 3, 499–506. [Google Scholar] [CrossRef]
- Lu, Y.; Zhang, Y.; Wang, N.; Pan, Z.; Gao, X.; Zhang, F.; Zhang, Y.; Shan, H.; Luo, X.; Bai, Y.; et al. MicroRNA-328 contributes to adverse electrical remodeling in atrial fibrillation. Circulation 2010, 122, 2378–2387. [Google Scholar] [CrossRef]
- Barana, A.; Matamoros, M.; Dolz-Gaitón, P.; Pérez-Hernández, M.; Amorós, I.; Núñez, M.; Sacristán, S.; Pedraz, Á.; Pinto, Á.; Fernández-Avilés, F.; et al. Chronic Atrial Fibrillation Increases MicroRNA-21 in Human Atrial Myocytes Decreasing L-Type Calcium Current. Circulation 2014, 7, 861–868. [Google Scholar] [CrossRef] [Green Version]
- Song, M.A.; Paradis, A.N.; Gay, M.S.; Shin, J.; Zhang, L. Differential expression of microRNAs in ischemic heart disease. Drug Discov. Today 2015, 20, 223–235. [Google Scholar] [CrossRef] [Green Version]
- Wu, Z.K.; Iivainen, T.; Pehkonen, E.; Laurikka, J.; Tarkka, M.R. Arrhythmias in off-pump coronary artery bypass grafting and the antiarrhythmic effect of regional ischemic preconditioning. J. Cardiothorac. Vasc. Anesth. 2003, 17, 459–464. [Google Scholar] [CrossRef]
- Wu, Z.K.; Iivainen, T.; Pehkonen, E.; Laurikka, J.; Tarkka, M.R. Ischemic preconditioning suppresses ventricular tachyarrhythmias after myocardial revascularization. Circulation 2002, 106, 3091–3096. [Google Scholar] [CrossRef]
- Wu, Z.K.; Iivainen, T.; Pehkonen, E.; Laurikka, J.; Tarkka, M.R. Perioperative and postoperative arrhythmia in three-vessel coronary artery disease patients and antiarrhythmic effects of ischemic preconditioning. Eur. J. Cardio-Thoracic Surg. 2003, 23, 578–584. [Google Scholar] [CrossRef] [Green Version]
- Papadopoulos, C.E.; Karvounis, H.I.; Parharidis, G.E.; Louridas, G.E. Preconditioning reduces QTc value in patients with first non-ST-segment elevation myocardial infarction (NSTEMI). Ann. Noninvasive Electrocardiol. 2003, 8, 275–283. [Google Scholar] [CrossRef]
- Pasceri, V.; Lanza, G.A.; Patti, G.; Pedrotti, P.; Crea, F.; Maseri, A. Preconditioning by transient myocardial ischemia confers protection against ischemia-induced ventricular arrhythmias in variant angina. Circulation 1996, 94, 1850–1856. [Google Scholar] [CrossRef]
- Meijs, L.P.B.; Galeotti, L.; Pueyo, E.P.; Romero, D.; Jennings, R.B.; Ringborn, M.; Warren, S.G.; Wagner, G.S.; Strauss, D.G. An electrocardiographic sign of ischemic preconditioning. Am. J. Physiol. 2014, 307, H80–H87. [Google Scholar] [CrossRef] [Green Version]
- Pavo, N.; Emmert, M.Y.; Giricz, Z.; Varga, Z.V.; Ankersmit, H.J.; Maurer, G.; Hoerstrup, S.P.; Ferdinandy, P.; Wu, J.C.; Gyongyosi, M. On-line visualization of ischemic burden during repetitive ischemia/reperfusion. JACC. Cardiovasc. Imag. 2014, 7, 956–958. [Google Scholar] [CrossRef]
- Birnbaum, G.D.; Birnbaum, I.; Birnbaum, Y. Twenty years of ECG grading of the severity of ischemia. J. Electrocardiol. 2014, 47, 546–555. [Google Scholar] [CrossRef]
- Wagner, G.S.; Johanson, P.; Weston, P.; Floyd, J.; Jennings, R. The supplementary effect of QRS changes on the inverse relationship between ST changes and salvage: Testing the Sclarovsky/Birnbaum clinical method in the basic Jennings/Reimer model. J. Electrocardiol. 2003, 36, 13–16. [Google Scholar] [CrossRef]
- Weston, P.; Johanson, P.; Schwartz, L.M.; Maynard, C.; Jennings, R.B.; Wagner, G.S. The value of both ST-segment and QRS complex changes during acute coronary occlusion for prediction of reperfusion-induced myocardial salvage in a canine model. J. Electrocardiol. 2007, 40, 18–25. [Google Scholar] [CrossRef]
- Cohen, M.V.; Yang, X.M.; Downey, J.M. Attenuation of S-T segment elevation during repetitive coronary occlusions truly reflects the protection of ischemic preconditioning and is not an epiphenomenon. Basic Res. Cardiol. 1997, 92, 426–434. [Google Scholar] [CrossRef]
- Taggart, P.; Yellon, D.M. Preconditioning and arrhythmias. Circulation 2002, 106, 2999–3001. [Google Scholar] [CrossRef]
- Floyd, J.S.; Maynard, C.; Weston, P.; Johanson, P.; Jennings, R.B.; Wagner, G.S. Effects of ischemic preconditioning and arterial collateral flow on ST-segment elevation and QRS complex prolongation in a canine model of acute coronary occlusion. J. Electrocardiol. 2009, 42, 19–26. [Google Scholar] [CrossRef]
- Billman, G.E. Role of ATP sensitive potassium channel in extracellular potassium accumulation and cardiac arrhythmias during myocardial ischaemia. Cardiovasc. Res. 1994, 28, 762–769. [Google Scholar] [CrossRef]
- Moss, A.J.; Kass, R.S. Long QT syndrome: From channels to cardiac arrhythmias. J. Clin. Invest. 2005, 115, 2018–2024. [Google Scholar] [CrossRef]
- Miller, L.E.; Hosick, P.A.; Wrieden, J.; Hoyt, E.; Quindry, J.C. Evaluation of arrhythmia scoring systems and exercise-induced cardioprotection. Med. Sci. Sports Exerc. 2012, 44, 435–441. [Google Scholar] [CrossRef]
- Curtis, M.J.; Walker, M.J. Quantification of arrhythmias using scoring systems: An examination of seven scores in an in vivo model of regional myocardial ischaemia. Cardiovasc. Res. 1988, 22, 656–665. [Google Scholar] [CrossRef]
- Kim, G.H. MicroRNA regulation of cardiac conduction and arrhythmias. Transl. Res. 2013, 161, 381–392. [Google Scholar] [CrossRef]
- Harada, M.; Luo, X.; Murohara, T.; Yang, B.; Dobrev, D.; Nattel, S. MicroRNA Regulation and Cardiac Calcium Signaling. Circ. Res. 2014, 114, 689–705. [Google Scholar] [CrossRef]
- Limana, F.; Marenzi, G.; Rubino, M.; De Simone, M.; Carena, M.C.; Devanna, P.; D’Alessandra, Y.; Pompilio, G.; Di Carlo, A.; Martelli, F.; et al. Circulating microRNAs are new and sensitive biomarkers of myocardial infarction. Eur. Heart J. 2010, 31, 2765–2773. [Google Scholar] [CrossRef] [Green Version]
- Sluijter, J.P.G.; Davidson, S.M.; Boulanger, C.M.; Buzas, E.I.; de Kleijn, D.P.V.; Engel, F.B.; Giricz, Z.; Hausenloy, D.J.; Kishore, R.; Lecour, S.; et al. Extracellular vesicles in diagnostics and therapy of the ischaemic heart: Position Paper from the Working Group on Cellular Biology of the Heart of the European Society of Cardiology. Cardiovasc. Res. 2018, 114, 19–34. [Google Scholar] [CrossRef]
- Agg, B.; Baranyai, T.; Makkos, A.; Veto, B.; Farago, N.; Zvara, A.; Giricz, Z. MicroRNA interactome analysis predicts post-transcriptional regulation of ADRB2 and PPP3R1 in the hypercholesterolemic myocardium. Sci. Rep. 2018, 8, 10134. [Google Scholar] [CrossRef]
- Bencsik, P.; Kiss, K.; Ágg, B.; Baán, J.A.; Ágoston, G.; Varga, A.; Gömöri, K.; Mendler, L.; Faragó, N.; Zvara, Á.; et al. Sensory Neuropathy Affects Cardiac miRNA Expression Network Targeting IGF-1, SLC2a-12, EIF-4e, and ULK-2 mRNAs. Int. J. Mol. Sci. 2019, 20, 991. [Google Scholar] [CrossRef]
- Pavo, N.; Lukovic, D.; Zlabinger, K.; Zimba, A.; Lorant, D.; Goliasch, G.; Winkler, J.; Pils, D.; Auer, K.; Jan Ankersmit, H.; et al. Sequential activation of different pathway networks in ischemia-affected and non-affected myocardium, inducing intrinsic remote conditioning to prevent left ventricular remodeling. Sci. Rep. 2017, 7, 43958. [Google Scholar] [CrossRef] [Green Version]
- Gyongyosi, M.; Dib, N. Diagnostic and prognostic value of 3D NOGA mapping in ischemic heart disease. Nat. Rev. Cardiol. 2011, 8, 393–404. [Google Scholar] [CrossRef]
- Pavo, N.; Zimmermann, M.; Pils, D.; Mildner, M.; Petrasi, Z.; Petnehazy, O.; Fuzik, J.; Jakab, A.; Gabriel, C.; Sipos, W.; et al. Long-acting beneficial effect of percutaneously intramyocardially delivered secretome of apoptotic peripheral blood cells on porcine chronic ischemic left ventricular dysfunction. Biomaterials 2014, 35, 3541–3550. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| R-Amplitude (mV) | |||||
| Time | IPC-AMI (n = 9) | AMI-PostC (n = 5) | AMI (n = 7) | p-Value | |
| Baseline | 1.26 ± 0.54 | 1.22 ± 0.47 | 1.27 ± 0.22 | n.s. | |
| IPC | Occlusion 3 × 5min. (pooled) | 1.01 ± 0.58 | |||
| Reperfusion 3 × 5min. (pooled) | 1.27 ± 0.83 | ||||
| Occlusion | 1–10 min | 1.07 ± 0.50 | 1.05 ± 0.43 | 1.02 ± 0.88 | n.s. |
| 10–20 min | 1.04 ± 0.54 * | 0.86 ± 0.36 * | 0.83 ± 0.33 | 0.007 | |
| 20–30 min | 1.06 ± 0.50 * | 0.83 ± 0.52 * | 0.72 ± 0.23 † | <0.001 | |
| 30–60min | 1.19 ± 0.80 *,† | 0.66 ± 0.34 *,° | 0.48 ± 0.25 †,° | <0.001 | |
| 60–90 min | 1.03 ± 0.65 *,† | 0.57 ± 0.23 * | 0.44 ± 0.37 † | <0.001 | |
| PostC | Reperfusion 6 × 30sec (pooled) | 0.92 ± 0.42 | |||
| Occlusion 6 × 30sec (pooled) | 0.98 ± 0.42 | ||||
| Reperfusion | 1–10 min. rep | 1.11 ± 0.45 † | 1.10 ± 0.43 ° | 0.47 ± 0.28 †,° | <0.001 |
| 10–20 min. rep | 1.09 ± 0.57 † | 1.12 ± 0.35 ° | 0.68 ± 0.46 †,° | <0.001 | |
| 20–30 min. rep | 1.01 ± 0.68 † | 1.06 ± 0.34 ° | 0.75 ± 0.53 †,° | 0.013 | |
| 30–60 min. rep | 0.98 ± 0.61 † | 1.06 ± 0.37 ° | 0.61 ± 0.36,° | <0.001 | |
| Maximal ST-Segment Elevation (mV) | |||||
| Time | IPC-AMI (n = 9) | AMI-PostC (n = 5) | AMI (n = 7) | p-Value | |
| Baseline | 0.66 ± 0.38 | 0.50 ± 0.33 | 0.50 ± 0.18 | n.s. | |
| IPC | Occlusion 3 × 5min. (pooled) | 3.47 ± 1.41 | |||
| Reperfusion 3 × 5min. (pooled) | 2.71 ± 1.10 | ||||
| Occlusion | 1–10 min | 4.19 ± 1.66 * | 4.82 ± 2.19 * | 5.53 ± 2.09 | <0.001 |
| 10–20 min | 4.59 ± 1.35 *,† | 5.78 ± 1.32 * | 6.24 ± 1.33 † | <0.001 | |
| 20–30 min | 4.19 ± 1.32 *,† | 5.13 ± 1.46 * | 5.67 ± 1.73 † | <0.001 | |
| 30–60min | 3.71 ± 1.62 *,† | 2.98 ± 1.05 * | 3.21 ± 1.33 † | <0.001 | |
| 60–90 min | 2.42 ± 1.10 *,† | 2.06 ± 0.70 * | 2.20 ± 0.76 † | 0.003 | |
| PostC | Reperfusion 6x30sec (pooled) | 1.42 ± 0.41 | |||
| Occlusion 6x30sec (pooled) | 1.37 ± 0.41 | ||||
| Reperfusion | 1–10 min. rep | 2.21 ± 1.09 * | 1.15 ± 0.42 *,° | 2.03 ± 0.51 ° | <0.001 |
| 10–20 min. rep | 1.93 ± 0.71 * | 0.92 ± 0.54 *,° | 1.78 ± 0.67 ° | <0.001 | |
| 20–30 min. rep | 1.59 ± 0.70 * | 0.87 ± 0.22 *,° | 1.42 ± 0.60 ° | <0.001 | |
| 30–60 min. rep | 1.19 ± 0.79 | 0.88 ± 0.26 | 1.12 ± 0.42 | n.s. | |
| QTc (ms) | |||||
| Time | IPC-AMI (n = 9) | AMI-PostC (n = 5) | AMI (n = 7) | p-Value | |
| Baseline | 309 ± 85 | 309 ± 31 | 311 ± 18 | n.s. | |
| IPC | Occlusion 3 × 5min. (pooled) | 319 ± 92 | |||
| Reperfusion 3 × 5min. (pooled) | 318 ± 101 | ||||
| Occlusion | 1–10 min | 327 ± 91 | 316 ± 33 | 312 ± 23 | n.s. |
| 10–20 min | 333 ± 97 | 320 ± 46 | 322 ± 41 | n.s. | |
| 20–30 min | 330 ± 104 | 325 ± 34 | 331 ± 66 | n.s. | |
| 30–60min | 320 ± 97 | 320 ± 38 | 323 ± 60 | n.s. | |
| 60–90 min | 324 ± 96 | 318 ± 47 | 325 ± 54 | n.s. | |
| PostC | Reperfusion 6 × 30sec (pooled) | 310 ± 84 | |||
| Occlusion 6 × 30sec (pooled) | 309 ± 84 | ||||
| Reperfusion | 1–10 min. rep | 320 ± 96 * | 305 ± 91 *,° | 326 ± 37 ° | 0.037 |
| 10–20 min. rep | 321 ± 97 | 305 ± 82 | 325 ± 50 | n.s. | |
| 20–30 min. rep | 320 ± 113 | 308 ± 67 | 325 ± 78 | n.s. | |
| 30–60 min. rep | 319 ± 102 | 305 ± 73 | 326 ± 52 | n.s. | |
| Heart rate (bpm) | |||||
| Time | IPC-AMI (n = 9) | AMI-PostC (n = 5) | AMI (n = 7) | p-value | |
| Baseline | 87 ± 21 | 80 ± 34 | 85 ± 20.08 | n.s. | |
| IPC | Occlusion 3 × 5min. (pooled) | 96 ± 33 | |||
| Reperfusion 3 × 5min. (pooled) | 91 ± 24 | ||||
| Occlusion | 1–10 min | 98 ± 32 | 103 ± 27 | 104 ± 23 | n.s. |
| 10–20 min | 103 ± 44 *,† | 117 ± 6 * | 115 ± 25 † | 0.019 | |
| 20–30 min | 96 ± 69 *,† | 119 ± 7 * | 115 ± 19 † | 0.015 | |
| 30–60min | 89 ± 27 *,† | 127 ± 7 * | 121 ± 21 † | <0.001 | |
| 60–90 min | 84 ± 23 *,† | 127 ± 12 * | 124 ± 25 † | <0.001 | |
| PostC | Reperfusion 6 × 30sec (pooled) | 125 ± 13 | |||
| Occlusion 6 × 30sec (pooled) | 124 ± 12 | ||||
| Reperfusion | 1–10 min. rep | 92 ± 20 *,† | 119 ± 10 * | 125 ± 23 † | <0.001 |
| 10–20 min. rep | 84 ± 24 *,† | 119 ± 10 * | 126 ± 25 † | <0.001 | |
| 20–30 min. rep | 84 ± 18 *,† | 120 ± 7 * | 131 ± 32 † | <0.001 | |
| 30–60 min. rep | 78 ± 18 | 114 ± 7 | 125 ± 22 | <0.001 | |
| Arrhythmia Score E | Score (0–6) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | 5 | 6 | IVR | ||
| Ischemia | IPC-AMI | 3 | 3 | 2 | 1 | ||||
| AMI | 1 | 3 | 1 | 1 | 1 | ||||
| AMI-PostC | 4 | 1 | |||||||
| Reperfusion | IPC-AMI | 3 | 6 | 5 | |||||
| AMI | 4 | 1 | 1 | 1 | 3 | ||||
| AMI-PostC | 3 | 2 | 2 | ||||||
| Variable | IPC-AMI (n = 8)+ | AMI-PostC (n = 4)+ | AMI (n = 6)+ | p-Value |
|---|---|---|---|---|
| Infarct size of LV (%) | 17.0 ± 7.1 * | 24.5 ± 3.8 | 25.2 ± 5.1 | 0.047 |
| LVEF (%) | 40.9 ± 4.2 | 37.2 ± 5.5 | 35.2 ± 4.6 | n.s. |
| LVEDVI (mL) | 66.3 ± 6.0 | 70.3 ± 12.4 | 64.5 ± 7.8 | n.s. |
| LVESVI (mL) | 39.2 ± 4.8 | 44.1 ± 9.1 | 41.7 ± 4.4 | n.s. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spannbauer, A.; Traxler, D.; Lukovic, D.; Zlabinger, K.; Winkler, J.; Gugerell, A.; Ferdinandy, P.; Hausenloy, D.J.; Pavo, N.; Emmert, M.Y.; et al. Effect of Ischemic Preconditioning and Postconditioning on Exosome-Rich Fraction microRNA Levels, in Relation with Electrophysiological Parameters and Ventricular Arrhythmia in Experimental Closed-Chest Reperfused Myocardial Infarction. Int. J. Mol. Sci. 2019, 20, 2140. https://doi.org/10.3390/ijms20092140
Spannbauer A, Traxler D, Lukovic D, Zlabinger K, Winkler J, Gugerell A, Ferdinandy P, Hausenloy DJ, Pavo N, Emmert MY, et al. Effect of Ischemic Preconditioning and Postconditioning on Exosome-Rich Fraction microRNA Levels, in Relation with Electrophysiological Parameters and Ventricular Arrhythmia in Experimental Closed-Chest Reperfused Myocardial Infarction. International Journal of Molecular Sciences. 2019; 20(9):2140. https://doi.org/10.3390/ijms20092140
Chicago/Turabian StyleSpannbauer, Andreas, Denise Traxler, Dominika Lukovic, Katrin Zlabinger, Johannes Winkler, Alfred Gugerell, Péter Ferdinandy, Derek J. Hausenloy, Noemi Pavo, Maximilian Y. Emmert, and et al. 2019. "Effect of Ischemic Preconditioning and Postconditioning on Exosome-Rich Fraction microRNA Levels, in Relation with Electrophysiological Parameters and Ventricular Arrhythmia in Experimental Closed-Chest Reperfused Myocardial Infarction" International Journal of Molecular Sciences 20, no. 9: 2140. https://doi.org/10.3390/ijms20092140