IGF2BP2 Polymorphisms Are Associated with Clinical Characteristics and Development of Oral Cancer



Abstract
1. Introduction
2. Results
2.1. Characteristics of Study Participants and IGF2BP2 Polymorphism in Oral Cancer
2.2. Association between IGF2BP2 Polymorphic Genotypes and Clinical Features of Oral Cancer
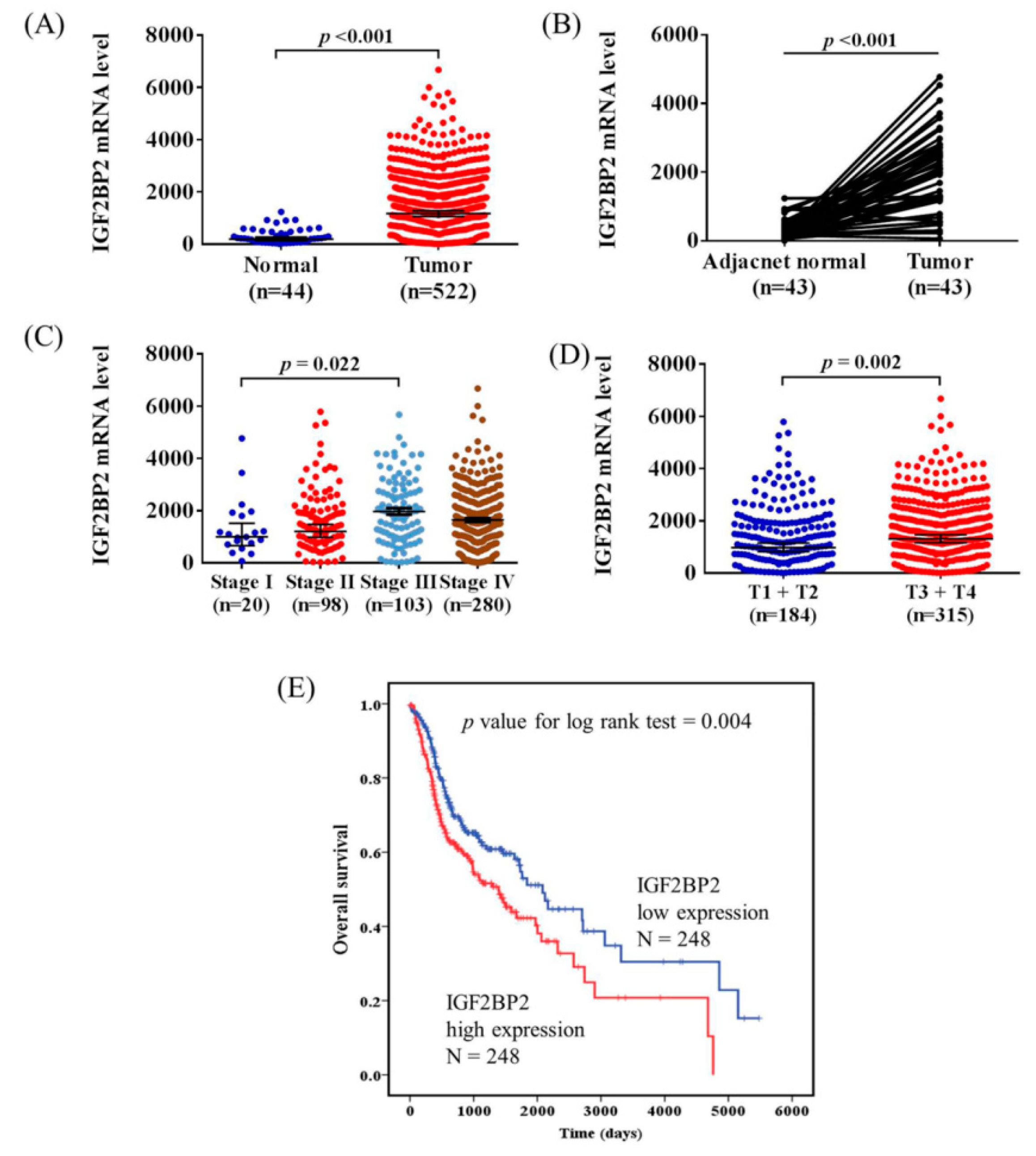
2.3. Association between IGFBP2 mRNA Expression and Clinical Characteristics of Head and Neck Squamous Cell Carcinoma (HNSCC) Tissues from The Cancer Genome Atlas (TCGA) Database
3. Discussion
4. Materials and Methods
4.1. Study Subjects
4.2. DNA Extraction and Genotyping
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Warnakulasuriya, S. Global epidemiology of oral and oropharyngeal cancer. Oral Oncol. 2009, 45, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Kao, S.Y.; Lim, E. An overview of detection and screening of oral cancer in taiwan. Chin. J. Dent. Res. 2015, 18, 7–12. [Google Scholar] [PubMed]
- Chaw, S.Y.; Abdul Majeed, A.; Dalley, A.J.; Chan, A.; Stein, S.; Farah, C.S. Epithelial to mesenchymal transition (emt) biomarkers–e-cadherin, beta-catenin, apc and vimentin--in oral squamous cell carcinogenesis and transformation. Oral Oncol. 2012, 48, 997–1006. [Google Scholar] [CrossRef] [PubMed]
- Mascitti, M.; Rubini, C.; De Michele, F.; Balercia, P.; Girotto, R.; Troiano, G.; Lo Muzio, L.; Santarelli, A. American joint committee on cancer staging system 7th edition versus 8th edition: Any improvement for patients with squamous cell carcinoma of the tongue? Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 126, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, J.; Christiansen, J.; Lykke-Andersen, J.; Johnsen, A.H.; Wewer, U.M.; Nielsen, F.C. A family of insulin-like growth factor ii mrna-binding proteins represses translation in late development. Mol. Cell Biol. 1999, 19, 1262–1270. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Wang, L.; He, J.; Bi, Y.; Li, M.; Wang, T.; Wang, L.; Jiang, Y.; Dai, M.; Lu, J.; et al. Prevalence and control of diabetes in chinese adults. JAMA 2013, 310, 948–959. [Google Scholar] [CrossRef]
- Christiansen, J.; Kolte, A.M.; Hansen, T.; Nielsen, F.C. Igf2 mrna-binding protein 2: Biological function and putative role in type 2 diabetes. J. Mol. Endocrinol. 2009, 43, 187–195. [Google Scholar] [CrossRef]
- Cao, J.; Mu, Q.; Huang, H. The roles of insulin-like growth factor 2 mrna-binding protein 2 in cancer and cancer stem cells. Stem Cells Int. 2018, 2018, 4217259. [Google Scholar] [CrossRef]
- Ruchat, S.M.; Elks, C.E.; Loos, R.J.; Vohl, M.C.; Weisnagel, S.J.; Rankinen, T.; Bouchard, C.; Perusse, L. Association between insulin secretion, insulin sensitivity and type 2 diabetes susceptibility variants identified in genome-wide association studies. Acta Diabetol. 2009, 46, 217–226. [Google Scholar] [CrossRef]
- Rao, P.; Wang, H.; Fang, H.; Gao, Q.; Zhang, J.; Song, M.; Zhou, Y.; Wang, Y.; Wang, W. Association between igf2bp2 polymorphisms and type 2 diabetes mellitus: A case-control study and meta-analysis. Int. J. Environ. Res. Public Health 2016, 13, 574. [Google Scholar] [CrossRef]
- Wu, H.H.; Liu, N.J.; Yang, Z.; Tao, X.M.; Du, Y.P.; Wang, X.C.; Lu, B.; Zhang, Z.Y.; Hu, R.M.; Wen, J. Igf2bp2 and obesity interaction analysis for type 2 diabetes mellitus in chinese han population. Eur. J. Med. Res. 2014, 19, 40. [Google Scholar] [CrossRef]
- Chistiakov, D.A.; Nikitin, A.G.; Smetanina, S.A.; Bel’chikova, L.N.; Suplotova, L.A.; Shestakova, M.V.; Nosikov, V.V. The rs11705701 g>a polymorphism of igf2bp2 is associated with igf2bp2 mrna and protein levels in the visceral adipose tissue − a link to type 2 diabetes susceptibility. Rev. Diabet Stud. 2012, 9, 112–122. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Qiu, H.; Liu, C.; Wang, Y.; Tang, W.; Kang, M. Relationship between igf2bp2 and igfbp3 polymorphisms and susceptibility to non-small-cell lung cancer: A case-control study in eastern chinese han population. Cancer Manag. Res. 2018, 10, 2965–2975. [Google Scholar] [CrossRef]
- Tang, W.; Chen, S.; Liu, J.; Liu, C.; Wang, Y.; Kang, M. Investigation of igf1, igf2bp2, and igfbp3 variants with lymph node status and esophagogastric junction adenocarcinoma risk. J. Cell Biochem. 2019, 120, 5510–5518. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.G.; Fisher, D.; Harris, R.; Maughan, T.S.; Phipps, A.I.; Richman, S.; Seymour, M.; Tomlinson, I.; Rosmarin, D.; Kerr, D.; et al. Analyses of 7,635 patients with colorectal cancer using independent training and validation cohorts show that rs9929218 in cdh1 is a prognostic marker of survival. Clin. Cancer Res. 2015, 21, 3453–3461. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.Y.; Zhou, S.J.; Deng, Y.L.; Zhang, Z.Y.; Zhang, E.L.; Wu, Z.B.; Huang, Z.Y.; Chen, X.P. Mir-216b is involved in pathogenesis and progression of hepatocellular carcinoma through hbx-mir-216b-igf2bp2 signaling pathway. Cell Death Dis. 2015, 6, e1670. [Google Scholar] [CrossRef]
- Barghash, A.; Helms, V.; Kessler, S.M. Overexpression of igf2 mrna-binding protein 2 (imp2/p62) as a feature of basal-like breast cancer correlates with short survival. Scand. J. Immunol. 2015, 82, 142–143. [Google Scholar] [CrossRef]
- Bigagli, E.; De Filippo, C.; Castagnini, C.; Toti, S.; Acquadro, F.; Giudici, F.; Fazi, M.; Dolara, P.; Messerini, L.; Tonelli, F.; et al. DNA copy number alterations, gene expression changes and disease-free survival in patients with colorectal cancer: A 10 year follow-up. Cell Oncol. (Dordr) 2016, 39, 545–558. [Google Scholar] [CrossRef]
- Davidson, B.; Rosenfeld, Y.B.; Holth, A.; Hellesylt, E.; Trope, C.G.; Reich, R.; Yisraeli, J.K. Vickz2 protein expression in ovarian serous carcinoma effusions is associated with poor survival. Hum. Pathol. 2014, 45, 1520–1528. [Google Scholar] [CrossRef]
- Kessler, S.M.; Pokorny, J.; Zimmer, V.; Laggai, S.; Lammert, F.; Bohle, R.M.; Kiemer, A.K. Igf2 mrna binding protein p62/imp2-2 in hepatocellular carcinoma: Antiapoptotic action is independent of igf2/pi3k signaling. Am. J. Physiol. Gastrointest Liver Physiol. 2013, 304, G328–G336. [Google Scholar] [CrossRef]
- Dai, N.; Ji, F.; Wright, J.; Minichiello, L.; Sadreyev, R.; Avruch, J. Igf2 mrna binding protein-2 is a tumor promoter that drives cancer proliferation through its client mrnas igf2 and hmga1. Elife 2017, 6. [Google Scholar] [CrossRef]
- Barghash, A.; Golob-Schwarzl, N.; Helms, V.; Haybaeck, J.; Kessler, S.M. Elevated expression of the igf2 mrna binding protein 2 (igf2bp2/imp2) is linked to short survival and metastasis in esophageal adenocarcinoma. Oncotarget 2016, 7, 49743–49750. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.; Zhu, T.; Cui, Y.; Liu, J.; Liu, J.; Zhao, Q.; Zhang, K.; Zhao, R. Correlation between igf2bp2 gene polymorphism and the risk of breast cancer in chinese han women. Biomed. Pharm. 2015, 69, 297–300. [Google Scholar] [CrossRef]
- Huang, Q.; Yin, J.Y.; Dai, X.P.; Pei, Q.; Dong, M.; Zhou, Z.G.; Huang, X.; Yu, M.; Zhou, H.H.; Liu, Z.Q. Igf2bp2 variations influence repaglinide response and risk of type 2 diabetes in chinese population. Acta Pharm. Sin. 2010, 31, 709–717. [Google Scholar] [CrossRef]
- Zhang, L.F.; Pei, Q.; Yang, G.P.; Zhao, Y.C.; Mu, Y.F.; Huang, Q.; Zhu, Y.L. The effect of igf2bp2 gene polymorphisms on pioglitazone response in chinese type 2 diabetes patients. Pharmacology 2014, 94, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Deng, N.; Zhou, H.; Fan, H.; Yuan, Y. Single nucleotide polymorphisms and cancer susceptibility. Oncotarget 2017, 8, 110635–110649. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Q.G.; Zhang, S.M.; Ding, X.X.; He, B.; Zhang, H.Q. Driver genes in non-small cell lung cancer: Characteristics, detection methods, and targeted therapies. Oncotarget 2017, 8, 57680–57692. [Google Scholar] [CrossRef]
- Yan, B.; Guan, D.; Wang, C.; Wang, J.; He, B.; Qin, J.; Boheler, K.R.; Lu, A.; Zhang, G.; Zhu, H. An integrative method to decode regulatory logics in gene transcription. Nat. Commun. 2017, 8, 1044. [Google Scholar] [CrossRef]
- He, B.; Lu, C.; Zheng, G.; He, X.; Wang, M.; Chen, G.; Zhang, G.; Lu, A. Combination therapeutics in complex diseases. J. Cell. Mol. Med. 2016, 20, 2231–2240. [Google Scholar] [CrossRef]
- He, X.; Li, W.; Liang, X.; Zhu, X.; Zhang, L.; Huang, Y.; Yu, T.; Li, S.; Chen, Z. Igf2bp2 overexpression indicates poor survival in patients with acute myelocytic leukemia. Cell Physiol. Biochem. 2018, 51, 1945–1956. [Google Scholar] [CrossRef]
- Edge, S.B.; Compton, C.C. The american joint committee on cancer: The 7th edition of the ajcc cancer staging manual and the future of tnm. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Controls (n = 1198) | Patients (n = 1349) | p Value |
|---|---|---|---|
| Age (yrs) | |||
| ≤55 | 608 (50.8%) | 683 (50.6%) | p = 0.935 |
| >55 | 590 (49.2%) | 666 (49.4%) | |
| Betel quid chewing | |||
| No | 1000 (83.5%) | 342 (25.4%) | |
| Yes | 198 (16.5%) | 1007 (74.6%) | p < 0.001 * |
| Cigarette smoking | |||
| No | 563 (47.0%) | 210 (15.6%) | |
| Yes | 635 (53.0%) | 1139 (84.4%) | p < 0.001 * |
| Alcohol drinking | |||
| No | 961 (80.2%) | 708 (52.5%) | |
| Yes | 237 (19.8%) | 641 (47.5%) | p < 0.001 * |
| Stage | |||
| I+II | 632 (46.9%) | ||
| III+IV | 717 (53.1%) | ||
| Tumor T status | |||
| T1+T2 | 679 (50.3%) | ||
| T3+T4 | 670 (49.7%) | ||
| Lymph node status | |||
| N0 | 890 (66.0%) | ||
| N1+N2+N3 | 459 (34.0%) | ||
| Metastasis | |||
| M0 | 1339 (99.3%) | ||
| M1 | 10 (0.7%) | ||
| Cell differentiation | |||
| Well differentiated | 189 (14.0%) | ||
| Moderately or poorly differentiated | 1160 (86.0%) |
| Variable | Controls (n = 1198) (%) | Patients (n = 1349) (%) | OR (95% CI) | AOR (95% CI) a |
|---|---|---|---|---|
| rs11705701 | ||||
| GG | 743 (62.0%) | 831 (61.6%) | 1.000 (reference) | 1.000 (reference) |
| GA | 390 (32.5%) | 466 (34.5%) | 1.068 (0.904–1.262) | 1.063 (0.864–1.308) |
| AA | 65 (5.5%) | 52 (3.9%) | 0.715 (0.490–1.044) | 0.778 (0.486–1.247) |
| GA+AA | 455 (38.0%) | 518 (38.4%) | 1.016 (0.865–1.192) | 1.024 (0.839–1.249) |
| rs4402960 | ||||
| GG | 710 (59.3%) | 799 (59.2%) | 1.000 (reference) | 1.000 (reference) |
| GT | 413 (34.5%) | 483 (35.8%) | 1.039 (0.880–1.227) | 1.123 (0.914–1.380) |
| TT | 75 (6.2%) | 67 (5.0%) | 0.793 (0.562–1.120) | 0.777 (0.505–1.194) |
| GT+TT | 488 (40.7%) | 550 (40.8%) | 0.999 (0.853–1.171) | 1.068 (0.877–1.300) |
| rs1470579 | ||||
| AA | 689 (57.5%) | 779 (57.7%) | 1.000 (reference) | 1.000 (reference) |
| AC | 428 (35.7%) | 499 (37.0%) | 1.031 (0.874–1.216) | 1.121 (0.913–1.376) |
| CC | 81 (6.8%) | 71 (5.3%) | 0.775 (0.554–1.083) | 0.768 (0.505–1.166) |
| AC+CC | 509 (42.5%) | 570 (42.3%) | 0.989 (0.845–1.157) | 1.063 (0.874–1.293) |
| Variable | AOR (95% CI) | p Value | ||
|---|---|---|---|---|
| Clinical Stage | ||||
| rs11705701 | Stage I+II | Stage III+IV | ||
| GG | 411 (65.0%) | 420 (58.6%) | 1.00 | |
| GA+AA | 221 (35.0%) | 297 (41.4%) | 1.322 (1.059–1.650) | p = 0.014 * |
| Tumor size | ||||
| rs11705701 | ≤T2 | >T2 | ||
| GG | 436 (64.2%) | 395 (59.0%) | 1.00 | |
| GA+AA | 243 (35.8%) | 275 (41.0%) | 1.253 (1.004–1.562) | p = 0.046 * |
| Lymph node metastasis | ||||
| rs11705701 | No | Yes | ||
| GG | 574 (64.5%) | 257 (56.0%) | 1.00 | |
| GA+AA | 316 (35.5%) | 202 (44.0%) | 1.440 (1.143–1.815) | p = 0.002 * |
| Metastasis | ||||
| rs11705701 | M0 | M1 | ||
| GG | 825 (61.6%) | 6 (60.0%) | 1.00 | |
| GA+AA | 514 (38.4%) | 4 (40.0%) | 1.078 (0.301–3.854) | p = 0.909 |
| Cell differentiated grade | ||||
| rs11705701 | ≤Grade I | >Grade I | ||
| GG | 120 (63.5%) | 711 (61.3%) | 1.00 | |
| GA+AA | 69 (36.5%) | 449 (38.7%) | 1.099 (0.798–1.514) | p = 0.562 |
| Variable | AOR (95% CI) | p Value | ||
|---|---|---|---|---|
| Clinical Stage | ||||
| rs4402960 | Stage I+II | Stage III+IV | ||
| GG | 392 (62.0%) | 407 (56.8%) | 1.00 | |
| GT+TT | 240 (38.0%) | 310 (43.2%) | 1.256 (1.009–1.563) | p = 0.042 * |
| Tumor size | ||||
| rs4402960 | ≤T2 | >T2 | ||
| GG | 427 (62.9%) | 372 (55.5%) | 1.00 | |
| GT+TT | 252 (37.1%) | 298 (44.5%) | 1.350 (1.085–1.680) | p = 0.007 * |
| Lymph node metastasis | ||||
| rs4402960 | No | Yes | ||
| GG | 549 (61.7%) | 250 (54.5%) | 1.00 | |
| GT+TT | 341 (38.3%) | 209 (45.5%) | 1.360 (1.081–1.711) | p = 0.009 * |
| Metastasis | ||||
| rs4402960 | M0 | M1 | ||
| GG | 794 (59.3%) | 5 (50.0%) | 1.00 | |
| GT+TT | 545 (40.7%) | 5 (50.0%) | 1.439 (0.413–5.013) | p = 0.568 |
| Cell differentiated grade | ||||
| rs4402960 | ≤Grade I | >Grade I | ||
| GG | 121 (64.0%) | 678 (58.5%) | 1.00 | |
| GT+TT | 68 (36.0%) | 482 (41.5%) | 1.260 (0.914–1.735) | p = 0.158 |
| Variable | AOR (95% CI) | p Value | ||
|---|---|---|---|---|
| Clinical Stage | ||||
| rs1470579 | Stage I+II | Stage III+IV | ||
| AA | 386 (61.1%) | 393 (54.8%) | 1.00 | |
| AC+CC | 246 (38.9%) | 324 (45.2%) | 1.306 (1.050–1.624) | p = 0.017 * |
| Tumor size | ||||
| rs1470579 | ≤T2 | >T2 | ||
| AA | 415 (61.1%) | 364 (54.3%) | 1.00 | |
| AC+CC | 264 (38.9%) | 306 (45.7%) | 1.317 (1.060–1.637) | p = 0.013 * |
| Lymph node metastasis | ||||
| rs1470579 | No | Yes | ||
| AA | 539 (60.6%) | 240 (52.3%) | 1.00 | |
| AC+CC | 351 (39.4%) | 219 (47.7%) | 1.416 (1.127–1.780) | p = 0.003 * |
| Metastasis | ||||
| rs1470579 | M0 | M1 | ||
| AA | 774 (57.8%) | 5 (50.0%) | 1.00 | |
| AC+CC | 565 (42.2%) | 5 (50.0%) | 1.348 (0.387–4.694) | p = 0.639 |
| Cell differentiated grade | ||||
| rs1470579 | ≤ Grade I | >Grade I | ||
| AA | 115 (60.9%) | 664 (57.2%) | 1.00 | |
| AC+CC | 74 (39.1%) | 496 (42.8%) | 1.158 (0.844–1.587) | p = 0.363 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chou, C.-H.; Chang, C.-Y.; Lu, H.-J.; Hsin, M.-C.; Chen, M.-K.; Huang, H.-C.; Yeh, C.-M.; Lin, C.-W.; Yang, S.-F. IGF2BP2 Polymorphisms Are Associated with Clinical Characteristics and Development of Oral Cancer. Int. J. Mol. Sci. 2020, 21, 5662. https://doi.org/10.3390/ijms21165662
Chou C-H, Chang C-Y, Lu H-J, Hsin M-C, Chen M-K, Huang H-C, Yeh C-M, Lin C-W, Yang S-F. IGF2BP2 Polymorphisms Are Associated with Clinical Characteristics and Development of Oral Cancer. International Journal of Molecular Sciences. 2020; 21(16):5662. https://doi.org/10.3390/ijms21165662
Chicago/Turabian StyleChou, Chia-Hsuan, Chien-Yuan Chang, Hsueh-Ju Lu, Min-Chien Hsin, Mu-Kuan Chen, Hsien-Cheng Huang, Chia-Ming Yeh, Chiao-Wen Lin, and Shun-Fa Yang. 2020. "IGF2BP2 Polymorphisms Are Associated with Clinical Characteristics and Development of Oral Cancer" International Journal of Molecular Sciences 21, no. 16: 5662. https://doi.org/10.3390/ijms21165662
APA StyleChou, C.-H., Chang, C.-Y., Lu, H.-J., Hsin, M.-C., Chen, M.-K., Huang, H.-C., Yeh, C.-M., Lin, C.-W., & Yang, S.-F. (2020). IGF2BP2 Polymorphisms Are Associated with Clinical Characteristics and Development of Oral Cancer. International Journal of Molecular Sciences, 21(16), 5662. https://doi.org/10.3390/ijms21165662