Upregulation of CD20 Positive B-Cells and B-Cell Aggregates in the Tumor Infiltration Zone is Associated with Better Survival of Patients with Pancreatic Ductal Adenocarcinoma

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
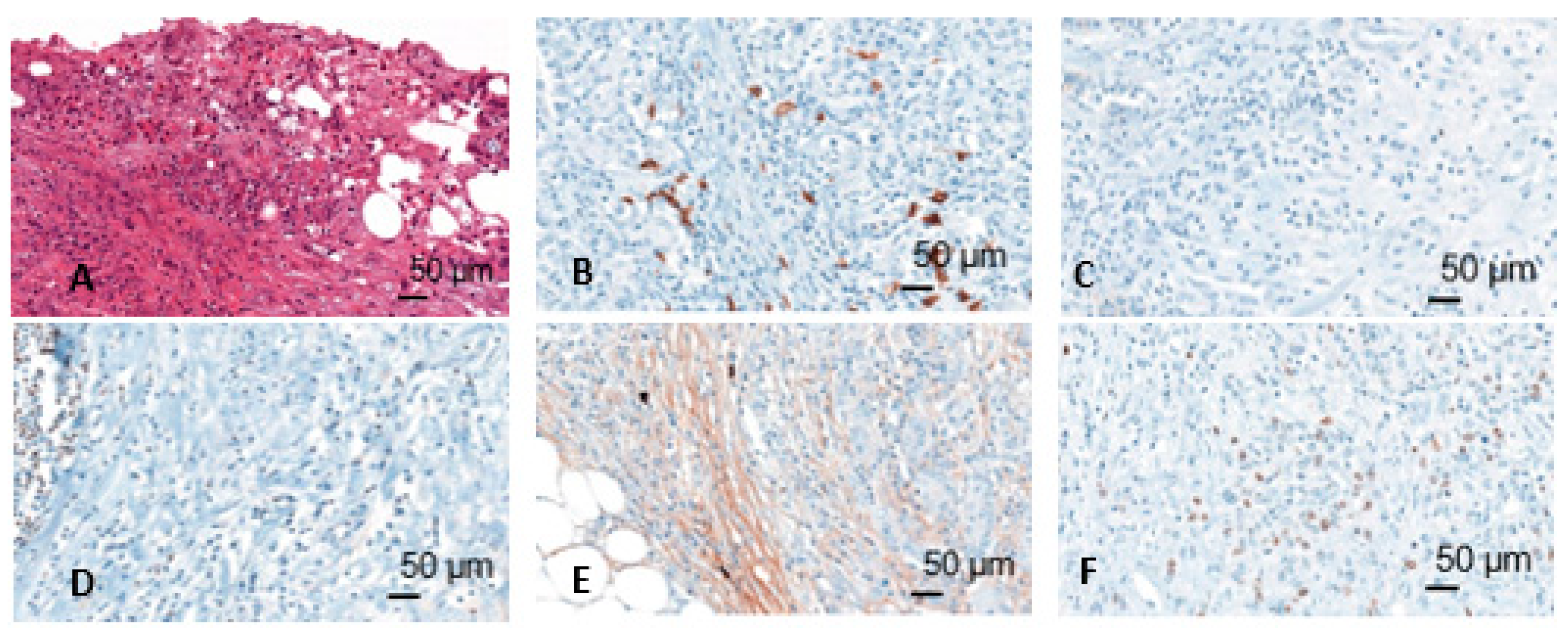
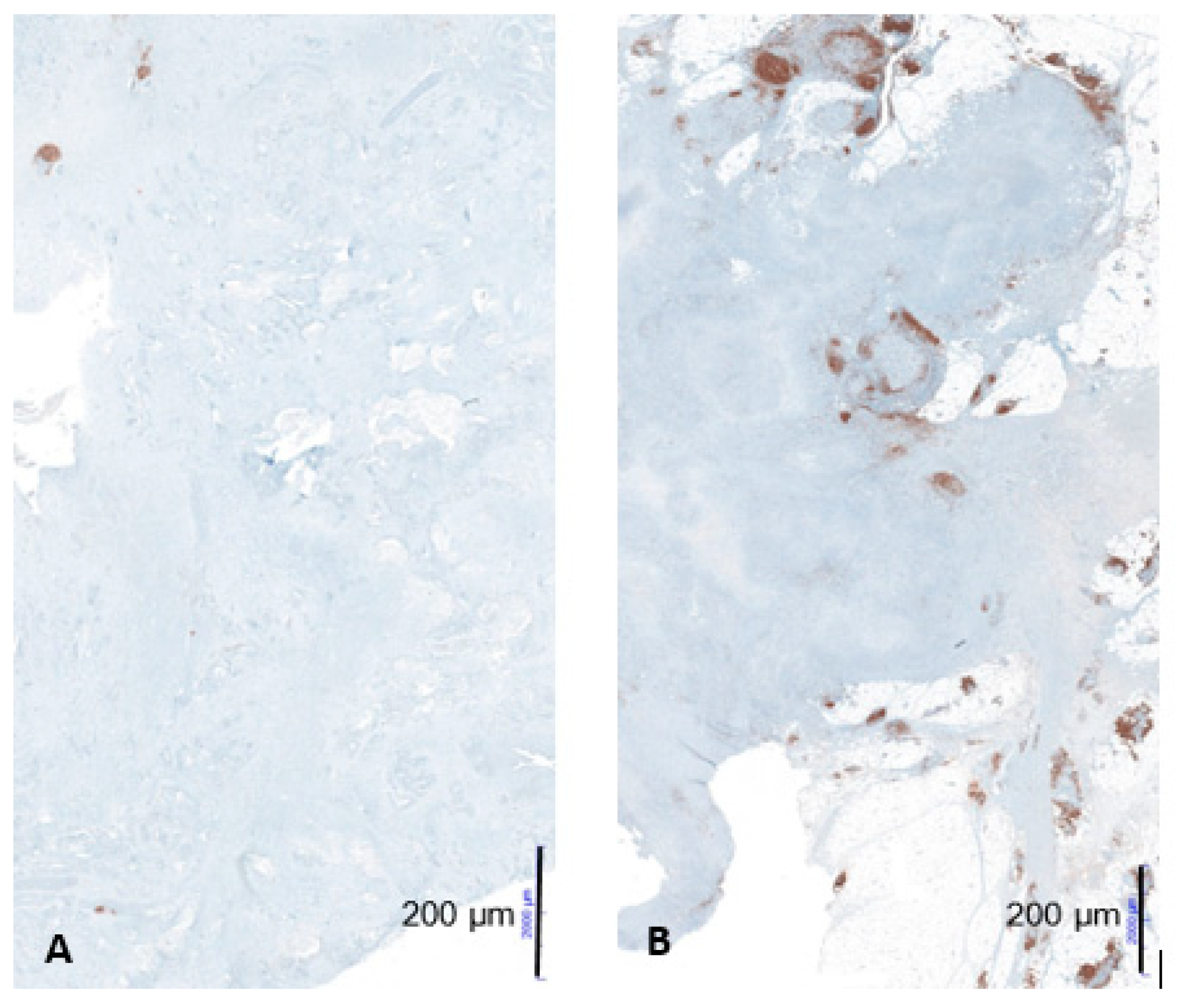
2.2. Immunohistochemical Staining and Scoring
2.3. Statistical Analysis
3. Results
3.1. Clinicopathological Characteristics
3.2. Immune Marker and Lymphoid Aggregates
3.3. Correlation of Immune Marker Expression with Clinicopathological Characteristics
3.4. Multivariate Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| PDAC | Pancreatic ductal adenocarcinoma |
| LTS | Long-term survivors |
| STS | Short-term survivors |
| OS | Overall survival |
| HR | Hazard ratio |
| CI | Confidence interval |
| TNM | Tumor-node-metastasis |
| CA19-9 | Carbohydrate antigen 19-9 |
| CEA | Carcinoembryonic antigen |
| TALs | Tumor-associated lymphocytes |
| kDa | Kilodalton |
| MHC | Major histocompatibility complex |
| LI | Lymphatic invasion |
| VI | Vascular invasion |
| PI | Perineural invasion |
| FU | Fluoruracil |
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2018. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Kaatsch, P.; Spix, C.; Katalinic, A.; Hentschel, S.; Luttmann, S.; Waldeyer-Sauerland, M.; Waldmann, A.; Christ, M.; Folkerts, J.; Hansmann, J.; et al. Gesellschaft der Epidemiologischen Krebsregister in Deutschland e.V.: Krebs in Deutschland 2015/16, 12th ed.; Robert-Koch-Institut: Berlin, Germany, 2019; Available online: http://www.gekid.de/Doc/krebs_in_deutschland_2019.pdf (accessed on 20 February 2020).
- Kamisawa, T.; Wood, L.D.; Itoi, T.; Takaori, K. Pancreatic cancer. Lancet 2016, 388, 73–85. [Google Scholar] [CrossRef]
- Kardosh, A.; Lichtensztajn, D.Y.; Gubens, M.A.; Kunz, P.L.; Fisher, G.A.; Clarke, C.A. Long-Term Survivors of Pancreatic Cancer: A California Population-Based Study. Pancreas 2018, 47, 958–966. [Google Scholar] [CrossRef]
- Stark, A.P.; Sacks, G.D.; Rochefort, M.M.; Donahue, T.R.; Reber, H.A.; Tomlinson, J.S.; Dawson, D.W.; Eibl, G.; Hines, O.J. Long-term survival in patients with pancreatic ductal adenocarcinoma. Surgery 2016, 159, 1520–1527. [Google Scholar] [CrossRef] [Green Version]
- Krautz, C.; Nimptsch, U.; Weber, G.F.; Mansky, T.; Grützmann, R. Effect of Hospital Volume on In-hospital Morbidity and Mortality Following Pancreatic Surgery in Germany. Ann. Surg. 2018, 267, 411–417. [Google Scholar] [CrossRef]
- Ino, Y.; Yamazaki-Itoh, R.; Shimada, K.; Iwasaki, M.; Kosuge, T.; Kanai, Y.; Hiraoka, N. Immune cell infiltration as an indicator of the immune microenvironment of pancreatic cancer. Br. J. Cancer 2013, 108, 914–923. [Google Scholar] [CrossRef]
- Wormann, S.M.; Diakopoulos, K.N.; Lesina, M.; Algul, H. The immune network in pancreatic cancer development and progression. Oncogene 2014, 33, 2956–2967. [Google Scholar] [CrossRef] [Green Version]
- Tewari, N.; Zaitoun, A.M.; Arora, A.; Madhusudan, S.; Ilyas, M.; Lobo, D.N. The presence of tumour-associated lymphocytes confers a good prognosis in pancreatic ductal adenocarcinoma: An immunohistochemical study of tissue microarrays. BMC Cancer 2013, 13, 436. [Google Scholar] [CrossRef]
- Diana, A.; Wang, L.M.; D’Costa, Z.; Azad, A.; Silva, M.A.; Soonawalla, Z.; Allen, P.; Liu, S.; McKenna, W.G.; Muschel, R.J.; et al. Prognostic role and correlation of CA9, CD31, CD68 and CD20 with the desmoplastic stroma in pancreatic ductal adenocarcinoma. Oncotarget 2016, 7, 72819–72832. [Google Scholar] [CrossRef]
- Golay, J.T.; Clark, E.A.; Beverley, P.C. The CD20 (Bp35) antigen is involved in activation of B cells from the G0 to the G1 phase of the cell cycle. J. Immunol. 1985, 135, 3795–3801. [Google Scholar] [PubMed]
- Juuti, A.; Nordling, S.; Lundin, J.; Louhimo, J.; Haglund, C. Syndecan-1 expression--a novel prognostic marker in pancreatic cancer. Oncology 2005, 68, 97–106. [Google Scholar] [CrossRef]
- Casali, P.; Schettino, E.W. Structure and function of natural antibodies. Curr. Top. Microbiol. Immunol. 1996, 210, 167–179. [Google Scholar] [PubMed]
- Kanteti, R.; Nallasura, V.; Loganathan, S.; Tretiakova, M.; Kroll, T.; Krishnaswamy, S.; Faoro, L.; Cagle, P.; Husain, A.N.; Vokes, E.E.; et al. PAX5 is expressed in small-cell lung cancer and positively regulates c-Met transcription. Lab. Investig. 2009, 89, 301–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerdes, J.; Schwab, U.; Lemke, H.; Stein, H. Production of a mouse monoclonal antibody reactive with a human nuclear antigen associated with cell proliferation. Int. J. Cancer 1983, 31, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Brierley, J.D.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumours, 8th ed.; Wiley-Blackwell: Oxford, UK, 2017. [Google Scholar]
- Droeser, R.; Zlobec, I.; Kilic, E.; Guth, U.; Heberer, M.; Spagnoli, G.; Oertli, D.; Tapia, C. Differential pattern and prognostic significance of CD4+, FOXP3+ and IL-17+ tumor infiltrating lymphocytes in ductal and lobular breast cancers. BMC Cancer 2012, 12, 134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, M.A.; Aleskandarany, M.A.; Rakha, E.A.; Moustafa, R.Z.; Benhasouna, A.; Nolan, C.; Green, A.R.; Ilyas, M.; Ellis, I.O. A CD44(−)/CD24(+) phenotype is a poor prognostic marker in early invasive breast cancer. Breast Cancer Res. Treat. 2011, 133, 979–995. [Google Scholar] [CrossRef]
- Ahmed, M.A.; Al-Attar, A.; Kim, J.; Watson, N.F.; Scholefield, J.H.; Durrant, L.G.; Ilyas, M. CD24 shows early upregulation and nuclear expression but is not a prognostic marker in colorectal cancer. J. Clin. Pathol. 2009, 62, 1117–1122. [Google Scholar] [CrossRef]
- Dieu-Nosjean, M.C.; Giraldo, N.A.; Kaplon, H.; Germain, C.; Fridman, W.H.; Sautès-Fridman, C. Tertiary lymphoid structures, drivers of the anti-tumor responses in human cancers. Immunol. Rev. 2016, 271, 260–275. [Google Scholar] [CrossRef]
- Hiraoka, N.; Ino, Y.; Yamazaki-Itoh, R.; Kanai, Y.; Kosuge, T.; Shimada, K. Intratumoral tertiary lymphoid organ is a favourable prognosticator in patients with pancreatic cancer. Br. J. Cancer 2015, 112, 1782–1790. [Google Scholar] [CrossRef] [Green Version]
- Petitprez, F.; de Reyniès, A.; Keung, E.Z.; Chen, T.W.; Sun, C.M.; Calderaro, J.; Jeng, Y.M.; Hsiao, L.P.; Lacroix, L.; Bougoüin, A.; et al. B cells are associated with survival and immunotherapy response in sarcoma. Nature 2020. [Google Scholar] [CrossRef]
- Helmink, B.A.; Reddy, S.M.; Gao, J.; Zhang, S.; Basar, R.; Thakur, R.; Yizhak, K.; Sade-Feldman, M.; Blando, J.; Han, G.; et al. B cells and tertiary lymphoid structures promote immunotherapy response. Nature 2020. [Google Scholar] [CrossRef] [PubMed]
- Gunderson, A.J.; Coussens, L.M. B cells and their mediators as targets for therapy in solid tumors. Exp. Cell Res. 2013, 319, 1644–1649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gunderson, A.J.; Kaneda, M.M.; Tsujikawa, T.; Nguyen, A.V.; Affara, N.I.; Ruffell, B.; Gorjestani, S.; Liudahl, S.M.; Truitt, M.; Olson, P.; et al. Bruton Tyrosine Kinase-Dependent Immune Cell Cross-talk Drives Pancreas Cancer. Cancer Discov. 2016, 6, 270–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K.E.; Spata, M.; Bayne, L.J.; Buza, E.L.; Durham, A.C.; Allman, D.; Vonderheide, R.H.; Simon, M.C. Hif1a Deletion Reveals Pro-Neoplastic Function of B Cells in Pancreatic Neoplasia. Cancer Discov. 2016, 6, 256–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pylayeva-Gupta, Y.; Das, S.; Handler, J.S.; Hajdu, C.H.; Coffre, M.; Koralov, S.B.; Bar-Sagi, D. IL35-Producing B Cells Promote the Development of Pancreatic Neoplasia. Cancer Discov. 2016, 6, 247–255. [Google Scholar] [CrossRef] [Green Version]
- Bondarenko, G.; Ugolkov, A.; Rohan, S.; Kulesza, P.; Dubrovskyi, O.; Gursel, D.; Mathews, J.; O’Halloran, T.V.; Wei, J.J.; Mazar, A.P. Patient-Derived Tumor Xenografts are Susceptible to Formation of Human Lymphocytic Tumors. Neoplasia 2015, 17, 735–741. [Google Scholar] [CrossRef] [Green Version]
- Castino, G.F.; Cortese, N.; Capretti, G.; Serio, S.; Di Caro, G.; Mineri, R.; Magrini, E.; Grizzi, F.; Cappello, P.; Novelli, F.; et al. Spatial distribution of B cells predicts prognosis in human pancreatic adenocarcinoma. Oncoimmunology 2016, 5, e1085147. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| STS | LTS | p-Value | ||
|---|---|---|---|---|
| Number | 16 | 16 | ||
| Mean Age (in years [range]) | 65 (47–78) | 64 (48–78) | 0.824 * | |
| Gender | Female | 11 (69) | 11 (69) | 1.000 * |
| Male | 5 (31) | 5 (31) | ||
| Tumor site | Head | 13 (81) | 13 (81) | 1.000 * |
| Head and tail | 2 (13) | 2 (13) | ||
| Tail | 1 (6) | 1 (6) | ||
| pN-category | pN0 | 7 (44) | 7 (44) | 1.000 * |
| pN + | 9 (56) | 9 (56) | ||
| Type of surgery | Whipples | 12 (75) | 12 (75) | 0.839 |
| Pylorus preserving | 1 (6) | 2 (13) | ||
| Left pancreatectomy | 3 (19) | 2 (13) | ||
| Grading | G2 | 6 (38) | 6 (38) | 1.000 |
| G3 | 10 (63) | 10 (63) | ||
| Lymphatic invasion | No | 9 (56) | 12 (75) | 0.458 |
| Yes | 7 (44) | 4 (25) | ||
| Vascular invasion | No | 15 (94) | 14 (88) | 1.000 |
| Yes | 1 (6) | 2 (13) | ||
| Perineural invasion | No | 4 (25) | 6 (38) | 0.704 |
| Yes | 12 (75) | 10 (63) | ||
| Adjuvant chemotherapy | Yes | 4 # (25) | 7 + (44) | 0.438 |
| No | 12 (75) | 9 (56) | ||
| CA19-9 | <40 IE/mL | 5 (31) | 5 (31) | 1.000 |
| ≥40 IE/mL | 5 (31) | 5 (31) | ||
| Unknown | 6 (38) | 6 (38) | ||
| CEA | <5 ng/L | 7 (44) | 9 (56) | 0.311 |
| ≥5 ng/L | 4 (25) | 1 (6) | ||
| Unknown | 1 (31) | 6 (38) |
| CD20 * | CD20-agg. TC | CD20-agg. IZ | CD138 * | IgM * | Pax5 * | Mib | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Low | High | p | Low | High | p | Low | High | p | Low | High | p | Low | High | p | Low | High | p | Low | High | p | |
| Age | |||||||||||||||||||||
| <65 years | 12 (80) | 5 (36) | 0.025 | 11 (58) | 7 (54) | 1.000 | 11 (69) | 7 (44) | 0.285 | 10 (63) | 8 (53) | 0.722 | 10 (63) | 8 (53) | 0.722 | 10 (67) | 7 (50) | 0.462 | 9 (56) | 9 (56) | 1000 |
| ≥65 years | 3 (20) | 9 (64) | 8 (42) | 6 (46) | 5 (31) | 9 (56) | 6 (38) | 7 (47) | 6 (38) | 7 (47) | 5 (33) | 7 (50) | 7 (44) | 7 (44) | |||||||
| Gender | |||||||||||||||||||||
| Female | 9 (60) | 12 (86) | 0.215 | 13 (68) | 9 (69) | 1.000 | 12 (75) | 10 (63) | 0.704 | 12 (75) | 10 (67) | 0.704 | 9 (56) | 13 (87) | 0.113 | 10 (67) | 11 (79) | 0.682 | 10 (63) | 12 (75) | 0.704 |
| Male | 6 (40) | 2 (14) | 6 (32) | 4 (31) | 4 (25) | 6 (38) | 4 (25) | 5 (33) | 7 (44) | 2 (13) | 5 (33) | 3 (21) | 6 (38) | 4 (25) | |||||||
| Tumor Site | |||||||||||||||||||||
| Head | 11 (73) | 13 (93) | 0.100 | 14 (74) | 12 (92) | 0.505 | 15 (94) | 11 (69) | 0.204 | 13 (81) | 12 (80) | 0.342 | 10 (63) | 15 (100) | 0.018 | 12 (80) | 12 (86) | 0.598 | 13 (81) | 13 (81) | 0.342 |
| Head and tail | 4 (27) | 0 (0) | 3 (16) | 1 (8) | 1 (6) | 3 (19) | 3 (19) | 1 (7) | 4 (25) | 0 (0) | 3 (20) | 1 (7) | 3 819) | 1 (6) | |||||||
| Tail | 0 (0) | 1 (7) | 2 (11) | 0 (0) | 0 (0) | 2 (13) | 0 (0) | 2 (13) | 2 (13) | 0 (0) | 0 (0) | 1 (7) | 0 (0) | 2 (13) | |||||||
| pN | |||||||||||||||||||||
| pN0 | 7 (47) | 6 (43) | 1.000 | 10 (52) | 4 (31) | 0.289 | 7 (44) | 7 (44) | 1.000 | 8 (50) | 5 (33) | 0.473 | 8 (50) | 5 (33) | 0.473 | 7 (47) | 6 (43) | 1.000 | 8 (50) | 6 (38) | 0.722 |
| pN+ | 8 (53) | 8 (57) | 9 (47) | 9 (69) | 9 (56) | 9 (56) | 8 (50) | 10 (67) | 8 (50) | 10 (67) | 8 (53) | 8 (57) | 8 (50) | 10 (63) | |||||||
| Type of Surgery | |||||||||||||||||||||
| Whipples | 11 (73) | 11 (79) | 0.686 | 14 (74) | 10 (77) | 0.497 | 14 (88) | 10 (63) | 0.356 | 13 (81) | 10 (67) | 0.595 | 9 (56) | 14 (93) | 0.040 | 11 (73) | 11 (79) | 0.686 | 13 (81) | 11 (69) | 0.730 |
| Pylorus preserving | 1 (7) | 2 (14) | 1 (5) | 2 (15) | 1 (6) | 2 (13) | 1 (6) | 2 (13) | 2 (13) | 1 (7) | 1 (7) | 2 (14) | 1 (6) | 2 (13) | |||||||
| Left pancreatectomy | 3 (20) | 1 (7) | 4 (21) | 1 (8) | 1 (6) | 4 (25) | 2 (13) | 3 (20) | 5 (31) | 0 (0) | 3 (20) | 1 (7) | 2 (13) | 3 (19) | |||||||
| Grading | |||||||||||||||||||||
| G2 | 5 (33) | 6 (43) | 0.710 | 7 (37) | 5 (39) | 1.000 | 6 (38) | 6 (38) | 1.000 | 5 (31) | 7 (47) | 0.473 | 5 (31) | 7 (47) | 0.473 | 5 (33) | 6 (43) | 0.710 | 6 (38) | 6 (38) | 1.000 |
| G3 | 10 (67) | 8 (57) | 12 (63) | 8 (62) | 10 (63) | 10 (63) | 11 (69) | 8 (53) | 11 (69) | 8 (53) | 10 (67) | 8 (57) | 10 (63) | 10 (63) | |||||||
| Lymphatic Invasion | |||||||||||||||||||||
| No | 11 (73) | 10 (71) | 1.000 | 13 (68) | 8 (62) | 0.721 | 11 (69) | 10 (63) | 1.000 | 11 (69) | 9 (60) | 0.716 | 10 (63) | 11 (73) | 0.704 | 10 (67) | 11 (79) | 0.682 | 11 (69) | 10 (63) | 1.000 |
| Yes | 4 (27) | 4 (29) | 6 (32) | 5 (39) | 5 (31) | 6 (38) | 5 (31) | 6 (40) | 6 (38) | 4 (27) | 5 (33) | 3 (21) | 5 (31) | 6 (38) | |||||||
| Vascular Invasion | |||||||||||||||||||||
| No | 13 (87) | 13 (93) | 1.000 | 17 (90) | 12 (92) | 1.000 | 15 (94) | 14 (88) | 1.000 | 14 (88) | 14 (93) | 1.000 | 15 (94) | 13 (87) | 0.600 | 13 (87) | 13 (93) | 1.000 | 14 (88) | 15 (94) | 1.000 |
| Yes | 2 (13) | 1 (7) | 2 (11) | 1 (8) | 1 (6) | 2 (13) | 2 (13) | 1 (7) | 1 (6) | 2 (13) | 2 (13) | 1 (7) | 2 (13) | 1 (6) | |||||||
| Perineural Invasion | |||||||||||||||||||||
| No | 5 (33) | 4 (29) | 1.000 | 6 (32) | 4 (31) | 1.000 | 4 (25) | 6 (38) | 0.704 | 4 (25) | 6 (40) | 0.458 | 5 (31) | 4 (27) | 1.000 | 4 (27) | 5 (36) | 0.700 | 3 (19) | 7 (44) | 0.252 |
| Yes | 10 (67) | 10 (71) | 13 (68) | 9 (69) | 12 (75) | 10 (63) | 12 (75) | 9 (60) | 11 (69) | 11 (73) | 11 (73) | 9 (64) | 13 (81) | 9 (56) | |||||||
| Adjuvant Chemotherapy | |||||||||||||||||||||
| Yes | 5 (33) | 6 (43) | 0.710 | 6 (32) | 5 (39) | 0.721 | 7 (44) | 4 (25) | 0.458 | 7 (44) | 4 (27) | 0.458 | 5 (31) | 6 (40) | 0.716 | 6 (40) | 5 (36) | 1.000 | 5 (31) | 6 (38) | 1.000 |
| No | 10 (67) | 8 (57) | 13 (68) | 8 (62) | 9 (56) | 12 (75) | 9 (56) | 11 (73) | 11 (69) | 9 (60) | 9 (60) | 9 (64) | 11 (69) | 10 (63) | |||||||
| CA19-9 ** | |||||||||||||||||||||
| <40 IE/mL | 5 (46) | 5 (63) | 0.650 | 7 (58) | 3 (38) | 0.650 | 7 (58) | 3 (38) | 0.650 | 8 (73) | 2 (25) | 0.070 | 4 (33) | 6 (75) | 0.170 | 6 (50) | 4 (57) | 1.000 | 7 (64) | 3 (33) | 0.370 |
| ≥40 IE/mL | 6 (55) | 3 (38) | 5 (42) | 5 (63) | 5 (42) | 5 (63) | 3 (27) | 6 (75) | 8 (67) | 2 (25) | 6 (50) | 3 (43) | 4 (36) | 6 (67) | |||||||
| CEA ** | |||||||||||||||||||||
| <5 ng/L | 9 (82) | 6 (67) | 0.617 | 10 (77) | 6 (75) | 1.000 | 7 (64) | 9 (90) | 0.311 | 7 (64) | 9 (90) | 0.311 | 9 (75) | 7 (78) | 1.000 | 10 (83) | 5 (63) | 0.603 | 9 (82) | 7 (70) | 0.635 |
| ≥5 ng/L | 2 (18) | 3 (33) | 3 (23) | 2 (25) | 4 (36) | 1 (10) | 4 (36) | 1 (10) | 3 (25) | 2 (22) | 2 (17) | 3 (38) | 2 (18) | 3 (30) | |||||||
| Univariate | Multivariate | |||
|---|---|---|---|---|
| HR | 95% CI | p-Value | ||
| CD20 * (Low vs. high) | 0.462 | - | - | 0.376 |
| CD20-aggregates in the tumor compartment (Low vs. high) | 0.473 | - | - | 0.337 |
| CD20-aggregates in the tumor infiltration zone (Low vs. high) | 0.016 | 9.2 | 1.6–51.4 | 0.012 |
| CD138 * (Low vs. high) | 0.724 | - | - | 0.337 |
| IgM * (Low vs. high) | 0.289 | - | - | 0.459 |
| Pax5 * (Low vs. high) | 0.462 | - | - | 0.648 |
| Mib (Low vs. high) | 0.724 | - | - | 0.189 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brunner, M.; Maier, K.; Rümmele, P.; Jacobsen, A.; Merkel, S.; Benard, A.; Krautz, C.; Kersting, S.; Grützmann, R.; Weber, G.F. Upregulation of CD20 Positive B-Cells and B-Cell Aggregates in the Tumor Infiltration Zone is Associated with Better Survival of Patients with Pancreatic Ductal Adenocarcinoma. Int. J. Mol. Sci. 2020, 21, 1779. https://doi.org/10.3390/ijms21051779
Brunner M, Maier K, Rümmele P, Jacobsen A, Merkel S, Benard A, Krautz C, Kersting S, Grützmann R, Weber GF. Upregulation of CD20 Positive B-Cells and B-Cell Aggregates in the Tumor Infiltration Zone is Associated with Better Survival of Patients with Pancreatic Ductal Adenocarcinoma. International Journal of Molecular Sciences. 2020; 21(5):1779. https://doi.org/10.3390/ijms21051779
Chicago/Turabian StyleBrunner, Maximilian, Katharina Maier, Petra Rümmele, Anne Jacobsen, Susanne Merkel, Alan Benard, Christian Krautz, Stephan Kersting, Robert Grützmann, and Georg F. Weber. 2020. "Upregulation of CD20 Positive B-Cells and B-Cell Aggregates in the Tumor Infiltration Zone is Associated with Better Survival of Patients with Pancreatic Ductal Adenocarcinoma" International Journal of Molecular Sciences 21, no. 5: 1779. https://doi.org/10.3390/ijms21051779